Katarzyna Raftowicz-Wójcik
1, Teresa Matthews-Brzozowska
2, Beata Kawala
1,
Joanna Antoszewska
1The Effects of Breast Feeding on Occlusion
in Primary Dentition
Wpływ karmienia piersią na zgryz w uzębieniu mlecznym
1 Department of Orthodontics and Dentofacial Orthopedics, Wroclaw Medical University, Poland 2 Department of Orthodontics, Poznań University of Medical Sciences, Poland
Abstract
Background. It has long been suggested that different types of infant feeding can have different effects on the for-mation of dental occlusion, but previous results on the influence of breast feeding and bottle feeding on orofacial development are inconclusive.
Objectives. To examine the effects of breast-feeding patterns on occlusion in deciduous dentition.
Material and Methods. The study group comprised 245 children aged 3–5 years with deciduous dentition. The study was based on clinical examinations and questionnaires. The sample was categorized according to the dura-tion of breast feeding and the types of malocclusions.
Results. There were no statistically significant correlations between the duration of breast feeding and the preva-lence of altered and normal occlusion. However, the authors found significant correlations between the duration of infant feeding and certain types of malocclusions: open bite, increased overbite and mesial bite.
Conclusions. Breast feeding for 6–12 months seems to have a preventive effect against open bite in the primary dentition, and exclusive bottle feeding seems to be a risk factor for mesial bite, but future longitudinal studies with a larger sample size are required (Adv Clin Exp Med 2011, 20, 3, 371–375).
Key words: breast feeding, malocclusion, primary dentition.
Streszczenie
Wprowadzenie. Od dawna sugerowano w piśmiennictwie, że różne rodzaje karmienia w okresie niemowlęcym mogą wpływać na rozwój zgryzu, ale rezultaty wcześniejszych badań odnośnie do wpływu karmienia piersią i butel-ką na tworzenie struktur ustno-twarzowych nie dały jednoznacznych wniosków.
Cel pracy. Zbadanie wpływu wzorców karmienia piersią na postać zgryzu w uzębieniu mlecznym.
Materiał i metody. Materiał badawczy obejmował 245 dzieci w wieku 3–5 lat z uzębieniem mlecznym. Metody były oparte na badaniu klinicznym i ankietowym. W badanej próbie wprowadzono podział uwzględniający okres karmienia piersią oraz rodzaj wady zgryzu.
Wyniki. Nie stwierdzono różnic istotnych statystycznie między okresem karmienia naturalnego a występowaniem zaburzonej lub prawidłowej okluzji. Znaleziono jednak statystycznie istotne różnice między różnymi okresami karmienia a niektórymi postaciami wad zgryzu: zgryzem otwartym, powiększonym nagryzem pionowym i przodo-zgryzem.
Wnioski. Wydaje się, że karmienie piersią przez 6–12 miesięcy ma profilaktyczny wpływ na występowanie zgryzu otwartego w uzębieniu mlecznym, a wyłączne karmienie butelką jest czynnikiem ryzyka powstania przodozgryzu, ale konieczne są dalsze długookresowe badania większej populacji dzieci (Adv Clin Exp Med 2011, 20, 3, 371–375).
Słowa kluczowe: karmienie piersią, wada zgryzu, uzębienie mleczne.
Adv Clin Exp Med 2011, 20, 3, 371–375 ISSN 1230-025X
ORIgINAl PAPERS
© Copyright by Wroclaw Medical University
Breast feeding is the most natural way to feed a small child, and it provides a range of nutrition-al, immunologicnutrition-al, socioeconomic and emotional benefits [1]. The World Health Organization
nu-trients that human milk supplies is unique, and its anti-infectious, anti-inflammatory and immuno-modulatory properties help prevent many diseas-es, reducing the incidence of hospital admissions [3]. Breast feeding also contributes also to proper motoric oral development, reducing the risk of speech-language disorders[1, 4].It has long been suggested in the literature that different types of nutrition and non-nutritive oral habits can have different effects on the formation of dental occlu-sion, but reports on the influence of breast and bottle feeding on orofacial development have been inconclusive [5–8].
This study was aimed at examining the effects of breast feeding patterns on occlusion in decidu-ous dentition.
Material and Methods
The study group was comprised of 245 pre-school children aged 3–5 years with deciduous dentition who already participated in a study deal-ing with malocclusions and speech disorders [9]. All the parents provided written informed con-sent, and the study design was approved by both the Bioethical Committee of Wroclaw Medical University (KB–232/2004) and the Department of Education of the Wroclaw Municipal Office (WE/ DPAN/07181/184/2004).
Dividing the study population according to the duration of breast feeding, four groups of children were obtained: (1) no breast feeding (= exclusively bottle-fed), (2) 0–6 months, (3) 6–12 months, and (4) more than 12 months. Subsequently, each group underwent orthodontic diagnosis to identify the following malocclusions of the primary dentition: 1) open bite – no vertical contact between the upper and lower teeth; 2) crossbite – constriction of the maxilla and/or overgrowth of the mandible; 3) in-creased overjet – horizontalincisoroverlapgreater than 3 mm; 4) increased overbite – vertical incisor overlap covering more than 75% of the lower inci-sor; 5) mesial occlusion – a mesial position of the lower teeth in relation to the upper ones.
All the malocclusions in every individual were recorded. Two children’s data were incomplete, so the statistical analysis included only 243 individu-als. Pearson`s χ2 test was used, and statistical
sig-nificance established as p < 0.05.
Results
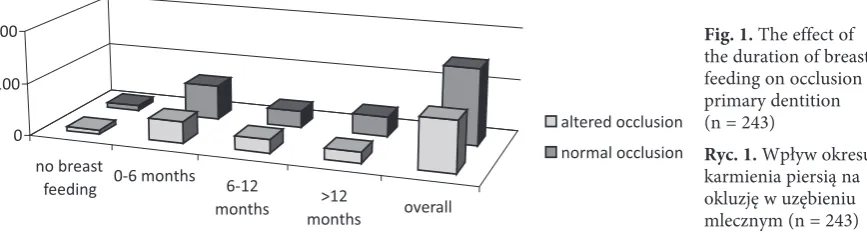
The duration of breast feeding did not signifi-cantly influence the development of malocclusion in general (p > 0.05; Fig. 1). Altered occlusion (A) was detected in 97 children and normal occlu-sion (N) in 146: (1) no breast feeding: 8 A, 10 N; (2) 0–6 months: 42 A, 66 N; 6–12 months: 26 A, 32 N; > 12 months: 21 A, 38 N.
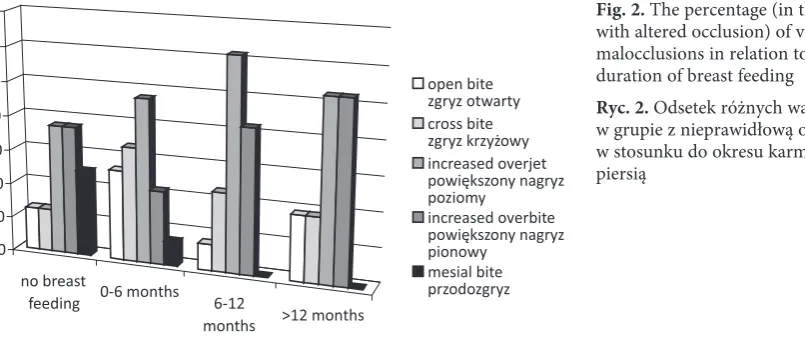
However, statistically significant correlations were found between the duration of breast feed-ing and certain types of malocclusions (Fig. 2, Ta-ble 1). The prevalence of an open bite in the group who were breast feed for 6–12 months was 7.7%; the frequency was significantly higher in the group breast-fed for 0–6 months (26.2%; p = 0.0001); in the group breast-fed for more than 12 months (19%; p = 0.0003); and among the children who were exclusively bottle-fed (12.5%; p = 0.0025). In-creased overbite was noted significantly more of-ten in the group that was breast-fed for more than 12 months (52.4%; p = 0.0156) than in the group breast-fed for 0–6 months (21.4%). The frequency of mesial occlusion was higher in the group that was exclusively bottle-fed (25%) in comparison to the other groups: in the group breast-fed for 0–6 months the frequency was 7.1% (p = 0.0156); and mesial occlusion was not detected in the group breast-fed for 6–12 months (p = 0.0131) or in the group breast-fed for more than 12 months (p = 0.0249).
Discussion
According to some clinicians breast feeding plays a particular role in preventing the develop-ment of posterior crossbite in primary dentition
Fig. 1. The effect of the duration of breast feeding on occlusion in primary dentition (n = 243)
Ryc. 1. Wpływ okresu karmienia piersią na okluzję w uzębieniu mlecznym (n = 243)
no breast
feeding 0-6 months 6-12
months months>12 overall 0
100 200
[10–13]. Karjalainen et al. [10] examined 148 3-year-old Finnish children and detected poste-rior crossbite in 13% of the group. The authors reported that the exclusive and total breast feed-ing periods in the children with posterior crossbite were significantly shorter (3.6 ± 3.8 and 4.7 ± 3.6 months, respectively) than the average (5.8 ± 3.6 and 7.3 ± 3.8 months, respectively). They conclud-ed that early weaning seems to be associatconclud-ed with an increased risk of posterior crossbite.
In a retrospective study of 1130 preschool chil-dren, Viggiano et al. [11] showed that bottle-fed children had more than double the risk of posterior crossbite. This type of malocclusion was recorded in 13% of the bottle-fed children with non-nutritive sucking activity and in 5% of the breast-fed children with non-nutritive sucking activity. However, based on the results of the study, Viggiano et al. stated that it is non-nutritive sucking rather than the method of feeding in the first months of life that is the main risk factor promoting the development of malocclu-sions in the primary dentition.
Those results are in accordance with the find-ings reported by Vázquez-Nava et al. [12], who – in a longitudinal study of 1160 children aged 4–5 years – found that bottle feeding alone, especially in children with allergic rhinitis, had an effect on posterior crossbite; however, a lack of nutritive sucking combined with allergic rhinitis turned out to be the most important factors contributing to the development of this type of malocclusion.
Peres et al. [13] carried out a cross-sectional study in Pelotas, Brazil. They examined a sample of 359 6-year-old children and observed that breast feeding lasting less than 9 months and regular use of a pacifier in children aged from 12 months to 4 years were risk factors for the development of posterior crossbite.
However, Øgaard et al., who examined 445 3-year-old children from Sweden and Norway, found that the type of infant feeding did not influ-ence the development of posterior crossbite [14]. Similarly, Warren and Bishara, in their longitudi-nal study involving 372 breast-fed children with
Fig. 2. The percentage (in the group with altered occlusion) of various malocclusions in relation to the duration of breast feeding
Ryc. 2. Odsetek różnych wad zgryzu w grupie z nieprawidłową okluzją w stosunku do okresu karmienia piersią
no breast
feeding 0-6 months 6-12
months >12 months 0
10 20 30 40 50 60 70
open bite zgryz otwarty cross bite zgryz krzyżowy increased overjet powiększony nagryz poziomy
increased overbite powiększony nagryz pionowy
mesial bite przodozgryz
Table 1. The percentage (in the group with altered occlusion) of various malocclusions in relation to the duration of breast feeding
Tabela 1. Odsetek różnych wad zgryzu w grupie z nieprawidłową okluzją w stosunku do okresu karmienia piersią
Open bite (Zgryz otwarty) %
Crossbite (Zgryz krzyżowy) %
Increased overjet (Powiększony nagryz poziomy) %
Increased overbite (Powiększony nagryz pionowy) %
Mesial bite (Przodozgryz) %
No breast feeding
(Brak karmienia piersią) 12.5* 12.5 37.5 37.5 25*
0–6 months
(0–6 miesięcy) 26.2* 33.3 47.6 21.4* 7.1*
6–12 months
(6–12 miesięcy) 7.7* 23 61.5 42 0*
> 12 months
(> 12 miesięcy) 19* 19 52.4 52.4* 0*
impaired sucking habits, whom they examined in their first year and again when they were 4–5 years old,did not find any correlation between the dura-tion of breast feeding and the dental arch param-eters or occlusal characteristics evaluated on the basis of diagnostic models [15].
Meyers and Hertzberg conducted a survey based on questionnaires sent to the parents of 737 patients aged 10–12 years. The questions in-cluded the type of infant feeding, the use of paci-fiers, sucking activity, the history of orthodontic treatment and parental orthodontic history. They found a trend of only marginal significance associ-ating a need for orthodontic treatment with bottle feeding, but they stated that these data should be interpreted with caution [16].
Charchut et al.investigated the effects of dif-ferent methods of infant feeding on the develop-ment of occlusion in deciduous dentition in 126 preschool children. They found that “predominant bottle-feeding between 0 and 6 months of age was associated with the development of a pacifier hab-it” and with greater probability of “[developing] an overbite > 75%, although just shy of nominal statistical significance” [17].
On the other hand, after examining 748 chil-dren aged 4–6 years and living in a rural area, Adamiak found a negative relationship between the duration of breast feeding and the prevalence of malocclusions [18].
Such results indicate that the evidence that breast feeding influences the development of mal-occlusion is ambiguous.
The findings of the current study indicate that the overall effects of breast feeding and bottle feed-ing on occlusion in deciduous dentition seem to be comparable. However relationships between different types of infant feeding and particular malocclusions were detected: open bite, increased overbite and mesial bite. Breast feeding for 6–12 months seems to have a preventive effect on open bite, while exclusive bottle feeding seems to be a risk factor for mesial bite. Future longitudinal studies comprising a larger group of individuals may provide more conclusive evidence clarifying the nature of any mutual relationships between the mode of nutrition and the development of maloc-clusion.
References
Neiva FCF, Cattoni DM, Ramos JLA, Issler H:
[1] Early weaning: implications to oral motor development. J Pediatr 2003, 79, 7–12.
[2] www.who.int/topics/breastfeeding/en/
do Nascimento MB, Issler H:
[3] Breastfeeding: making the difference in the development, health and nutrition of term and preterm newborns. Rev Hosp Clin Fac Med S Paulo 2003, 58, 49–60.
Raftowicz-Wójcik K, Matthews-Brzozowska T, Kawala B:
[4] Breast feeding in the prophylaxis of malocclusions and articulation disorders. Pediatr Pol 2007, 82, 143–146.
Fabac E, Legouvić M, Župan M:
[5] The linkage between breast feeding and the growth of the orofacial area. Fortschr Kieferorthop 1992, 53, 187–191.
Turgeon-O`Brien H, Lachapelle D, Gagnon P F, Larocque I, Maheu-Robert L-F:
[6] Nutritive and nonnutritive
sucking habits: A review. J Dent Child 1996, 321–327.
Larsson E.:
[7] Sucking, chewing, and feeding habits and the development of crossbite: a longitudinal study of girls from birth to 3 years of age. Angle Orthod 2001, 71, 116–119.
Ganesh M, Tandon S, Sajida B:
[8] Prolonged feeding practice and its effects on developing dentition. J Indian Soc Pedod Prev Dent 2005, 23, 141–145.
Raftowicz-Wójcik K, Matthews-Brzozowska T:
[9] Wady zgryzu u dzieci w wieku przedszkolnym z/bez wad wymowy. Czas Stomatol 2006, 5, 361–367.
Karjalainen S, Ronning O, Lapinleimu H, Simmell O:
[10] Association between early weaning, non-nutritive sucking habits and occlusal anomalies in 3-year old Finnish children. Int J Paediatr Dent 1999, 9, 169–173.
Viggiano D, Fasano D, Monaco G, Strohmenger L:
[11] Breast feeding, bottle feeding, and non-nutritive sucking; effects on occlusion in deciduous dentition. Arch Dis Child 2004, 89, 1121–1123.
Vázquez-Nava F, Quezada-Castillo JA, Oviedo-Treviño S, Saldivar-Gonzales AH, Sanchez-Nuncio HR, Beltran-[12]
Guzman FJ, Vázquez-Rodriguez E M, Vázquez-Rodriguez CF: Association between allergic rhinitis, bottle feeding, non-nutritive sucking habits, and malocclusion in the primary dentition. Arch Dis Child 2006, 91, 836–840.
Peres KG, Barros AJD, Peres MA, Victora CG:
[13] Effects of breastfeeding and sucking habits on malocclusion in a birth cohort study. Rev Saúde Pública 2007, 41, 343–350.
Øgaard B, Larsson E, Lindsten R:
[14] The effect of sucking habits, cohort, sex, intercanine arch widths, and breast or bottle feeding on posterior crossbite in Norwegian and Swedish 3-year-old-children. Am J Orthod Dentofac Orthop 1994, 106, 161–166.
Warren JJ, Bishara SE:
[15] Duration of nutritive and nonnutritive sucking behaviors and their effects on the dental arches in the primary dentition. Am J Orthod Dentofac Orthop 2002, 121, 347–356.
Meyers A, Hertzberg J:
Charchut SW, Allred EN, Needleman HL:
[17] The effects of infant feeding patterns on the occlusion of the primary dentition. J Dent Child (Chic) 2003, 70, 197–203.
Adamiak E:
[18] Occlusion anomalies in preschool children in rural areas in relation to certain individual features. Czas Stomatol 1981, 34, 551–555.
Address for correspondence:
Joanna Antoszewska
Department of Orthodontics and Dentofacial Orthopedics Wroclaw Medical University
Krakowska 26 50-425 Wrocław Poland
Tel./fax: +48 71 784 02 99 E-mail: [email protected]
Conflict of interest: None declared