M
AŁGORZATAK
OTULSKAElectrochemotherapy in Cancer Treatment
Elektrochemioterapia w leczeniu nowotworów
Institute of Biomedical Engineering and Instrumentation, Wroclaw University of Technology, Poland Adv Clin Exp Med 2007, 16, 5, 601–607
ISSN 1230−025X
EDITORIAL
© Copyright by Silesian Piasts University of Medicine in Wrocław
Abstract
An electric field of high intensity changes the organization of lipids in the cell membrane, creating transient hydrophilic pores through which ions can freely permeate. This phenomenon, called electroporation (EP), greatly facilitates molecular transport across the membrane and permits enhanced delivery of biologically active mole− cules, such as drugs and nucleic acids, into the cell. Currently, EP is commonly used for in vitrocell transfection as the cleanest method available. It can also be applied in genetic therapy or immunotherapy in vivo. The most recent application of EP, becoming increasingly popular in the EU, the USA, and Australia, is electrochemothera− py (ECT), in which electroporation significantly increases the intracellular concentration of a cytotoxic agent. ECT applied with a drug that can hardly permeate through the plasma membrane without EP, such as bleomycin, allows localized treatment of a tumor, thereby reducing the side effects of systemic chemotherapy. In some cases, ECT eliminates the necessity of surgery (Adv Clin Exp Med 2007, 16, 5, 601–607).
Key words: electroporation, electrochemotherapy, drug internalization, cancer.
Streszczenie
Pod wpływem silnego pola elektrycznego cząsteczki lipidów w błonie komórkowej zmieniają swoją organizację, tworząc przejściowe hydrofilowe pory, które umożliwiają swobodny transport jonów poprzez membranę. Zjawi− sko takie, nazywane elektroporacją (EP), pozwala na pokonanie bariery błony komórkowej i ułatwione wprowa− dzanie do wnętrza komórek substancji biologicznie czynnych, takich jak leki lub kwasy nukleinowe. Obecnie EP jest standardowo wykorzystywana w hodowlach komórkowych in vitro, jako najczystsza dostępna metoda trans− fekcji genów. EP można też stosować w genoterapii oraz immunogenoterapii in vivo. Najnowszym zastosowaniem EP, które staje się coraz bardziej powszechne w krajach europejskich, a także w USA i Australii, jest elektroche− mioterapia (ECT), w której elektroporacja istotnie podnosi wewnątrzkomórkowe stężenie substancji cytotoksycz− nej. Zastosowanie w ECT leku, który samoistnie jest bardzo słabo transportowany do wnętrza komórki, jak np. ble− omycyny, umożliwia miejscowe leczenie nowotworu, ograniczając skutki uboczne chemioterapii ogólnoustrojo− wej. W niektórych przypadkach ECT eliminuje konieczność interwencji chirurgicznej (Adv Clin Exp Med 2007, 16, 5, 601–607).
Słowa kluczowe:elektroporacja, elektrochemioterapia, rak.
Cell membranes are sensitive to physicochemi− cal conditions such as the biochemical environ− ment, temperature, mechanical stress, and electro− magnetic field. It was discovered that under certain conditions the plasma membrane of a cell loses its continuity. This has been observed mainly under an electric field of high intensity (Fig. 1) and is called electroporation (EP) (reviewed in [4, 13, 30, 39]). The mechanism of electroporation is still not suffi− ciently explored and not fully understood. Due to their small size, combined with their very high
Pores significantly increase membrane con− ductance and open a transport pathway for mole− cules. Opening a new pathway through the plasma membrane has severe consequences for the cell, which is no longer separated from its environment. Various molecules normally kept outside the cell can get into the cytoplasm, avoiding the usual strict control. Although this is undesirable under the physiological conditions, it can be useful in therapy. Typically, molecules are transported into cells by channels or pumps located in the plasma membrane. Lipophilic molecules, which are solu− ble in the lipid bilayer, can diffuse across the plas− ma membrane directly. Molecules that are neither lipophilic nor transported by channels and pumps cannot be easily delivered into the cell. In genetic therapy, all targets are inside the cell. Therefore, a very important application of electroporation is gene therapy or gene vaccination, where it has become a standard method for delivering DNA or RNA into cells since the 1980s. Similarly, almost all the cytotoxic drugs in cancer therapy become biologically effective inside the cell. If the drug is not lipophilic, its internalization is difficult. Electroporation is currently used in the elec− trochemotherapy (ECT) of cancer [29], gene ther− apy, and DNA vaccination (reviewed in [11]). Tests show that it can be applied in intraocular therapy [32], and the application of EP in photo− dynamic therapy is also considered [24]. In current applications, the electropermeabilization of the tis− sue enhances the internalization of extracellular molecules under 30 kDa. Results from chronoam− perometry after current clamp (CACC) electro− poration [22], the authors’ novel combinatory method using electropores with the edge gradually stabilized, show that creating large pores with a controllable diameter and lifetime is possible. Such electropores may facilitate the delivery of large molecules, e.g. plasmid DNA, into cells. It was recently shown that ultra−short nanosecond
pulses alone are capable of eradicating melanoma cells with no use of cytostatic drugs. The studies indicate the induction of apoptosis in tumor cells subjected to nanosecond pulses [1].
Electrochemotherapy
in Cancer Treatment
Electrochemotherapy (ECT) is a novel thera− peutic approach enabling the delivery of nonper− meant drugs directly into the cell. The first study of ECT in vivo on an animal tumor model was reported in 1987 [31]. The effectiveness of elec− trochemotherapy was first tested on animal models and then on humans in preclinical and clinical tri− als. ECT is a very promising treatment method in the case of localized tumors. It may increase treat− ment effectiveness for various cancers treated by chemotherapy, increasing the permeability of the cell membrane for the cytotoxic agent. ECT was envisaged as a very promising method in tumors resistant to conventional cancer therapies, such as melanoma, where the typical response rate is low, with partial response (PR) of 20–45% and com− plete response (CR) of less than 5% [2, 10]. The ECT tests included cutaneous and subcutaneous tumors, treated mainly by means of the non− lipophilic cytotoxic drug bleomycin. Preclinical trials with bleomycin, especially efficient in the treatment of head and neck cancer, showed that cytotoxicity increased 300 to 700−fold if ECT was applied [7]. Patients with tumors located in the facial/cervical region, oral cavity, pharynx, larynx, and sinus showed 73% objective response (CR+PR) when treated with bleomycin by ECT [5]. No response was obtained with similar doses of bleomycin or electroporation alone. Tests have also been conducted using cisplatin, where a 2− to 8−fold enhancement of citotoxicity was reported [7], and actinomycin D, with a 3 to 5−fold cyto− toxicity increase [32]. ECT does not increase the cytotoxicity of amphi− and lipophilic drugs, such as danorubicin, doxorubicin, etoposide, and pacli− taxel [7, 12].
An important feature of electroporation in vivo
is its influence on blood flow, demonstrated by decreased blood circulation [28]. This phenome− non is called a vascular lock. The vascular system reacts to an electric field by constriction (1–2 min), which is enhanced by an increase in the interstitial pressure (30 min) related to the release of fluids from the electroporated cells into the extracellular space [9]. Therefore, for a few min− utes following the application of electrical pulses the cells under treatment are not accessible for molecules in the blood. Vascular constriction is
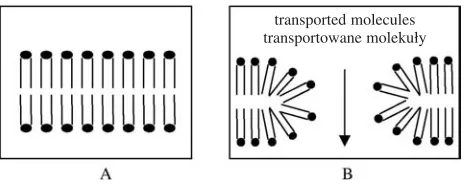
Fig. 1. A continuous lipid membrane (A) develops a conducting hydrophilic electropore when the mem− brane is exposed to a sufficiently high electric field (B)
Ryc. 1.W ciągłej strukturze błony lipidowej (A) pod wpływem silnego pola elektrycznego powstaje hydro− filowy elektropor (B)
most conspicuous in tumor tissue due to its irregu− lar microvasculature and lack of a well−defined boundary separating the vascular system from the interstitial fluid. In tumor tissues the vascular lock lasts up to one hour. This effect is very favorable in terms of chemotherapy, where it prevents wash− ing out of the drug from the cancerous tissue. The drug should be provided before the application of the electric field so that it can enter the cells before the lock appears.
On the other hand, the tumor hypoxia associ− ated with the vascular lock may result in resistance to radiotherapy, opposing the radiosensitizing effect of bleomycin and cysplastin used in ECT. It was proved [23], however, that ECT−induced hypoxia of the tumor does not counteract the favorable effect of bleomycin. Therefore, the ECT− enhanced uptake of bleomycin and cisplatin into cancerous cells results in significantly higher sen− sitivity of the tumor to radiotherapy. Moreover, the temporal decrease in tissue oxygenation may be utilized in the therapy with hypoxic cytotoxins, such as tirapazamine. Animal model studies showed an up to six−fold increase in tumor growth delay when ECT with tirapazamine was combined with radiotherapy compared with tirapazamine with radiation alone [3, 25].
The combination of electrochemotherapy with immunotherapy increasing the host’s immune response by the administration of biologically active modifiers might be an attractive modifica− tion of standard ECT [26]. Preclinical trials with interleukin−2 have been performed on a non− metastasizing murine tumor model [27], a metas− tasizing murine tumor model [33], and a carcino− ma model transplanted into rabbit liver [35]. The studies showed improvement in the local effects combined with the systemic antitumor effect.
Principles of
Electropermeabilization
in ECT
Several tests on animal models have been con− ducted in search of the optimal parameters for the ECT procedure, such as the field frequency, ampli− tude, and the electrode layout. It was estimated that the intensity of the electric field used in ECT should fall between 900–1500 V/cm [10], with the optimum in cancer therapy being 1300 V/cm. Typically, the electric field is delivered by four to eight square pulses, each 100 µs in width, admin− istered at one−second intervals. Rectangular sig− nals are more effective than the initially used exponential pulses since their duration can be con−
trolled independently of the pulse intensity; there− by, less intense fields can be applied. It was shown that rotating the electrodes by 90° after the first four pulses enhances the result by better coverage of the tumor tissue [37]. One sequence of electric pulses is sufficient for small tumors. For large tumors the therapy is repeated at a different posi− tion of the electrodes so that the tumor surface can be better covered. The most unpleasant side effect of the pulse wave protocol is a painful muscle con− traction appearing with each train of pulses and caused by the high amplitude of the pulses. Since the amplitude cannot be reduced, it was proposed to increase the frequency of the pulse repetition, which would diminish the number of painful individual muscle contractions. As results showed that an increase in the repetition frequency even to 8.3 kHz does not affect drug uptake [34], it was proposed that the repetition frequency may be set above the frequency of tetanic contraction (100 Hz).
The effective electric field in the cells depends on the voltage amplitude and the configuration of the electrodes. Several different electrode layouts have been analyzed: parallel−plate electrodes and needle electrodes located in linear, circular, and hexagonal arrays [8]. It was found that needle electrodes are more efficient for subcutaneous tumors. A study published by Gehl and colleagues [6] recommends linear eight−needle electrodes in which the needles are placed in two rows 4 mm apart. Such electrodes distribute the electric field more homogeneously, which permits applying lower voltages than in a circular arrangement. Other authors recommend six electrodes arranged hexagonally, with changing polarity [5]. Although plate electrodes are noninvasive, the electric field cannot be applied deeply. They can be successive− ly used for cutaneous cancers. Application of plate electrodes may lead to the occurrence of superfi− cial burns on the patient’s skin.
Bleomycin: the Most
Typical Drug in ECT
test” [36] to recognize the genetic instability char− acteristic of cancerous cells. Bleomycin does not cause myelotoxicity, cardiotoxicity, diarrhea, vo− miting, or nausea; only very high cumulative doses can lead to lung fibrosis. Importantly, bleo− mycin does not restrict the cellular immune response. However, the low permeability of bleo− mycin into the cell, leading to its low effective− ness, hampered its use and it could not be admin− istered alone. In electrochemotherapy, this feature can be regarded as an asset. A high intracellular concentration of the drug can be limited to only the regions undergoing treatment.
At therapeutic doses, which can be signifi− cantly decreased if ECT is used, bleomycin kills cells by generating free radicals which cleave DNA and RNA. There is no agreement on whether the cell death is due to apoptosis or necrosis. In necrotic death, the damaged ion pumps and chan− nels of the cell do not perform their selective trans− port, which leads to swelling of the cell and its organelles, leakage of the material into the extra− cellular space, and an inflammatory response. In apoptosis, which is a genetically programmed cell death, the gradual dismantling of cell function is very orderly. Mir et al. support the idea of non− apoptotic cell death caused by bleomycin [28]. They claim that bleomycin triggers a slow death process of the cell which resembles mitotic cell death. Therefore, a favorable inflammatory immu− ne response is present. Nonetheless, other authors who observed chromatin condensation and nuclear fragmentation, which is typical for apoptosis, claim that the cell disintegrates in an apoptotic way with some elements of necrosis [5]. Bleomycin is known to release or induce the pro− duction of cytokines such as interleukin−2, interleukin−6, and tumor necrosis factor, which additionally contributes to the healing process [5]. The half−life of bleomycin in the blood of patients with good renal function is 2–4 hours. The drug is eliminated mainly by renal excretion. Cells with increased repair mechanisms may be less sensitive to bleomycin. No rapid induction of resistant cells has been observed [9]. Similarly, bleomycin is not subject to multidrug resistance (MDR), which is a common problem with other cytotoxic agents. The MDR gene increases the activity of P−glyco− protein, which transports many anti−neoplastic drugs but it does not transport bleomycin [9]. Bleomycin can be degraded by bleomycin hydro− lase present in the cytosol of all cells as a part of the cells’ protesome disintegrating many cellular proteins. Bleomycin hydrolase has a lower con− centration in the lungs and skin, which probably explains the higher cytotoxicity of bleomycin in these tissues. Also, bleomycin can be disabled by
bleomycin resistance proteins (BRP), which are found in microorganisms producing bleomycin or bleomycin derivatives.
The low transport rate of the bleomycin mole− cules into the cell is the main problem of an effec− tive treatment. Typically, when no electroperme− abilization is induced, bleomycin is bound by spe− cific membrane proteins located on the cell surface and transported into the cell by endocytosis. Autoradiography with C14−labeled bleomycin
demonstrated that only 0.1% of the bleomycin added to the medium was associated with cells after a few hours. When cellular electropermeabi− lization is applied, the drug’s internalization is massively increased. Moreover, bleomycin in electropermeabilized cells produces DNA breaks very rapidly, usually in less than 30 sec. The con− centration of bleomycin in the electropermeabi− lized cell is proportional to its external concentra− tion in a well−defined manner. On average, an external concentration of 10 nM relates to 3000 bleomycin molecules inside the cell. This helps to predict the precise dose and cellular reaction.
Most favorably, bleomycin in ECT can be administered intravenously or intratumorally ([9] and references therein) as a bolus or infusion [10]. The optimal intravenous doses related to the pa− tient’s approximate body surface area were estimat− ed to be 5.6–15 mg/m2(10–27 U/m2; one unit (U) of
antimicrobial activity contains 0.56–0.66 mg of bleomycin [9] and corresponds to 1000 interna− tional units (IU)). The optimal infusion time at this dose is 30–45 s. The doses for intravenous treat− ment are similar to the doses used in conventional chemotherapy, i.e. 18–27 U/m2[9]; the injection is
applied only once. Intratumoral treatment is sug− gested in the case of a small number of distinct subcutaneous tumors, especially when the tumors are poorly vascularized. The doses depend on the tumor volume V, calculated as:
V= ab2 π/6
The optimal concentration of delivered drug was estimated at 0.25 ml (0.25 U)/cm3for tumors
larger than 1 cm3, 0.5 ml (0.5 U)/cm3for tumors of
medium size, i.e. 0.5 cm3< V< 1 cm3, and 1 ml
(1 U)/cm3 for tumors smaller than 0.5 cm3. The
drug concentration decreases since larger tumors absorb larger quantities of the solute. The drug concentration is usually insignificantly in excess because the distribution of the injected fluid can be heterogeneous. Unlike typical chemotherapy, ECT is a once−only treatment, which significantly decreases the cumulative dose that may cause lung fibrosis if a dose of 300 mg/m2 is reached [9].
bleomycin, such as erythema, induration, hyperk− eratosis, and peeling of the skin, are avoided due to the low cumulative doses applied in ECT.
Effectiveness and Clinical
Use of EP Therapies
Studies of the ECT effectiveness have been provided for a wide variety of cancers; a thorough review of recent clinical results is presented in a supplement to the European Journal of Cancer entirely devoted to electrochemotherapy [29]. The review includes mostly melanoma cases, where results are the most conspicuous, hepatocellular carcinoma, breast carcinoma, fibrosarcoma and glioma, head and neck squamous cell carcinoma, Kaposi’s sarcoma, basal cell carcinoma, and ade− nocarcinoma. In general, very significant increas− es in objective response (72–100%) and complete responses (85%) following ECT application hve been reported in many cases. In some situations, ECT treatment proves effective where other, con− ventional methods fail (e.g. refractory breast cancer [40]). In other situations it permits avoiding surgery, particularly when it may improve the patient’s com− fort by saving an organ or its significant part from removal (e.g. the eye lid, rectum [38]).
Among many electroporators available on the market, two are designed specifically for the clin− ical use of ECT on humans. The European device was constructed following the EU−funded ESOPE (European Standard Operating Procedure for Electrochemotherapy) project. As a result of this
project, a biomedical company, IGEA, introduced the Cliniporator (Fig. 2). The Cliniporator com− plies with directive 93/42/EEC for medical devices and is officially permitted for clinical use in all EU countries. Although the standard condi− tions for ECT with the Cliniporator are eight square−wave pulses each 100 µs wide, the operator can choose the number of pulses from a range of 1–20. The amplitude of the pulses ranges between 100–1000 V. The electrodes optimal for the treat− ment of subcutaneous tumors are either hexagonal or linear needle arrays; two plates are available for cutaneous tumors. The possibility of extending the Cliniporator with an ECG synchronizer, which would minimize the risk of heart defibrillation, is under study. Compared with the prices of advanced devices for radiotherapy, the apparatus is quite cost effective. Moreover, treatment can be performed on an outpatient basis, additionally reducing the costs of treatment and increasing the patient’s comfort. In the USA, BTX released a clinical electroporator, the MedPulser, in 2004. The MedPulser is supplied with hexagonal elec− trodes that apply six pulses of an intensity of 1130 V within 10 seconds. However, until now the apparatus can be applied for clinical use only out− side EU countries.
In Europe, ECT treatment of skin, head, and neck cancers have successfully gone through the stage of clinical tests and have received the CE mark. The clinical use of ECT among EU coun− tries has been reported in France, Denmark, Slovenia, Ireland, Italy, and Spain. ECT is also successfully used in the USA and Australia.
Fig. 2.The Cliniporator by IGEA and a set of electrodes for subcuta− neous (upper) and cutaneous tumors (bottom). Reprinted with permis− sion from IGEA
Ryc. 2. Kliniporator (IGEA) i zestaw elektrod do nowotworów nie− operacyjnych (góra) i operacyjnych (dół). Przedruk za zgodą IGEA
hexagonal and linear needle array for treatment of subcutaneous tumours heksagonalna i liniowa macierz igłowa do leczenia guzów nieoperacyjnych
Perspectives
of the Electroporation
Therapy
In a few years’ time, ECT may become an important alternative therapy to the surgical resec− tion of recurrent melanoma tumors. It could be very useful in metastatic diseases in sites where defects remaining after surgery are difficult to close, especially when nodal excision or irradia−
tion were previously administered [20]. The next stage of research into electrochemotherapy will concern the possibility of ECT treatment of prima− ry tumors in internal organs. Genetic vaccines, which will become increasingly popular in treat− ment and prophylactics, will tend to use safer physicochemical methods based on non−viral vec− tors, such as electroporation. The main challenge concerning EP therapies will be the development of safe and efficient methods for electropermeabi− lization of tissue in internal organs.
Acknowledgements
The author would like to thank Dr. Lluis M. Mir from CNRS, France, and Dr. Maja Cemazar from Institute of Oncology in Ljubljana, Slovenia, for very stimulating discussions concerning electrochemotherapy.
References
[1] Beebe SJ, Fox PM, Rec LJ, Lauren E, Willis K, Schoenbach H:Nanosecond, high intensity pulsed electric fields induce apoptosis in human cells. FASEB 2003, 17, 1493–1495.
[2] Byrne CM, Thompson JF:Role of electrochemotherapy in the treatment of metastatic melanoma and other metastatic and primary skin tumors. Expert Rev Anticancer Ther 2006, 6, 671–678.
[3] Cemazar M, Parkins CS, Holder AL, Kranjc S, Chaplin DJ, Sersa G:Cytotoxicity of bioreductive drug tira− pazamine is increased by application of electric pulses in SA−1 tumours in mice. Anticancer Res 2001, 21, 1151–1156.
[4] Chang DC, Chassy BM, Saunders JA, Sowers AE (Eds.): Guide to Electroporation and Electrofusion. Academic Press, San Diego 1992.
[5] Dev SB, Rabussay DP, Widera G, Hofmann GA:Medical applications of electroporation. IEEE Transactions on Plasma Sci 2000, 28, 206–223.
[6] Gehl J, Sorensen TH, Nielsen K, Raskmark P, Nielsen SL, Skovsgaard T, Mir LM: In vivoelectroporation of skeletal muscle: threshold, efficacy and relation to electric field distribution. Biochim Biophys Acta 1999, 1428, 233–240.
[7] Gehl J, Skovsgaard T, Mir LM:Enhancement of cytotoxicity by electropermeabilization: an improved method for screening drugs. Anticancer Drugs 1998, 9, 319–325.
[8] Gilbert RA, Jaroszeski MJ, Heller R:Novel electrode designs for electrochemotherapy. Biochim Biophys Acta 1997, 1334, 9–14.
[9] Gothelf A, Mir LM, Gehl J: Electrochemotherapy: results of cancer treatment using enhanced delivery of bleomycin by electroporation. Cancer Treat Rev 2003, 29, 371–387.
[10] Heller R, Gilbert R, Jaroszeski MJ:Clinical applications of electrochemothrapy. Adv Drug Deliv Rev 1999, 35, 119–129.
[11] Heller LC, Heller R:In vivoelectroporation for gene therapy. Hum Gene Ther 2006, 17, 890–897.
[12] Jaroszeski MJ, Dang V, Pottinger C, Hickey J, Gilbert R, Heller R:Toxicity of anticancer agents mediated by electroporation in vitro. Anticancer Drugs 2000, 11, 201–208.
[13] Kalinowski S:Elektrochemia membran lipidowych. Wyd. Uniwersytetu Warmińsko−Mazurskiego 2004.
[14] Kalinowski S, Koronkiewicz S, Kotulska M, Kubica K:Simulation of electroporated cell by chronopotentiom− etry. Bioelectrochemistry 2007, 70, 83–90.
[15] Koronkiewicz S, Kalinowski S, Bryl K:Programmable chronopotentiometry as a tool for the study of electro− poration and resealing of pores in bilayer lipid membranes. Biochim Biophys Acta 2002, 1561, 222–229.
[16] Kotulska M, Koronkiewicz S, Kalinowski S:Cholesterol induced changes in the characteristics of the time series from planar lipid bilayer membrane during electroporation. Acta Phys Pol B 2002, 33, 1115–1124.
[17] Kotulska M, Koronkiewicz S, Kalinowski S: Self−similar processes and flicker noise from a fluctuating nanopore in a lipid membrane. Phys Rev E 2004, 69, 031920–031930.
[18] Kotulska M:1/f noise in nanopores and its potential application in biosensors. Elektronika 2004, 8–9, 130–134.
[19] Kotulska M, Kubica K:Structural and energetical effects of ionic strength in modeling lipid membranes. Acta Phys Pol B 2005, 36, 1641–1651.
[20] Kotulska M, Kubica K:Structural and energetic model of the mechanisms for reduced self−diffusion in a lipid bilayer with increasing ionic strength. Phys Rev E 2005, 72, 061903–061909.
[21] Kotulska M, Kubica K, Koronkiewicz S, Kalinowski S:Modeling the induction of lipid membrane electroper− meabilization. Bioelectrochemistry 2007, 70, 64–70.
[23] Kranjc S, Cemazar M, Grosel A, Sentjurc M, Sersa G:Radiosensitising effect of electrochemotherapy with bleomycin in LPB sarcoma cells and tumors in mice. BMC Cancer 2005, 5, 115–124.
[24] Labanauskiene J, Gehl J, Didziapetriene J:Evaluation of cytotoxic effect of photodynamic therapy in combi− nation with electroporation in vitro. Bioelectrochemistry 2007, 70, 78–82.
[25] Maxim PG, Carson JJ, Ning S, Knox SJ, Boyer AL, Hsu CP, Benaron DA, Walleczek J: Enhanced effec− tiveness of radiochemotherapy with tirapazamine by local application of electric pulses to tumors. Radiat Res 2004, 162, 185–193.
[26] Mir LM, Orlowski S, Poddevin B, Belehradek J Jr:Electrochemotherapy tumor treatment is improved by inter− leukin−2 stimulation of the host’s defenses. Eur Cytokine Netw 1992, 3, 331–334.
[27] Mir LM, Roth C, Orlowski S, Quintin−Colonna F, Fradelizi D, Belehradek J Jr, Kourilsky P:Systemic anti− tumor effects of electrochemotherapy combined with histoincompatible cells secreting interleukin−2. J Immunother Emphasis Tumor Immunol 1995, 17, 30–38.
[28] Mir LM, Orlowski S:Mechanisms of electrochemotherapy. Adv Drug Deliv Rev 1999, 35, 107–118.
[29] Mir LM, Ed.:Eur J Cancer – Supplements 2006, 4, 1–51.
[30] Neumann E, Kakorin S, Toensing K: Fundamentals of electroporative delivery of drugs and genes. Bioelectrochem Bioenerg 1999, 48, 3–16.
[31] Okino M, Mohri H: Effects of a high−voltage electrical impulse and an anticancer drug on in vivo growing tumors. Jpn J Cancer Res 1987, 78, 1319–1321.
[32] Orlowski S, Belehradek J Jr, Paoletti C, Mir LM:Transient electropermeabilization of cells in culture. Increase of the cytotoxicity of anticancer drugs. Biochem Pharmacol 1988, 37, 4727–4733.
[33] Orlowski S, An D, Belehradek J Jr, Mir LM:Antimetastatic effects of electrochemotherapy and of histoin− compatible interleukin−2−secreting cells in the murine Lewis lung tumor. Anticancer Drugs 1998, 9, 551–556.
[34] Pucihar G, Mir LM, Miklavcic D:The effect of pulse repetition frequency on the uptake into electropermeabi− lized cells in vitrowith possible applications in electrochemotherapy. Bioelectrochemistry2002, 57, 167–172.
[35] Ramirez LH, Orlowski S, An D, Bindoula G, Dzodic R, Ardouin P, Bognel C, Belehradek J Jr, Munck JN, Mir LM: Electrochemotherapy on liver tumours in rabbits. Br J Cancer 1998, 77, 2104–2111.
[36] Schantz SP, Hsu TC, Ainslie N, Moser RP:Young adults with head and neck cancer express increased suscep− tibility to mutagen−induced chromosome damage. JAMA 1989, 262, 3313–3315.
[37] Sersa G, Cemazar M, Miklavcic D: Antitumor effectiveness of electrochemotherapy with cis−diammine− dichloroplatinum(II) in mice. Cancer Res 1995, 55, 3450–3455.
[38] Snoj M, Rudolf Z, Cemazar M, Jancar B, Sersa G:Successful sphincter−saving treatment of anorectal malig− nant melanoma with electrochemotherapy, local excision and adjuvant brachytherapy. Anticancer Drugs 2005, 16, 345–348.
[39] Weaver JC, Chizmadzhev YA: Theory of electroporation: a review. Bioelectrochem Bioenerg 1996, 41, 135–160.
[40] Whelan MC, Larkin JO, Collins CG, Cashman J, Breathnach O, Soden DM, O’Sullivan GC:Effective treat− ment of an extensive recurrent breast cancer which was refractory to multimodal therapy by multiple applications of electrochemotherapy. Eur J Cancer Supplements 2006, 4, 32–34.
Address for correspondence:
Institute of Biomedical Engineering and Instrumentation Wroclaw University of Technology
Wybrzeze Wyspianskiego 27 50−370 Wroclaw
Poland
Tel.: +48 71 320 39 74
E−mail: [email protected]
Conflict of interest: None declared