Ohio Statewide Quality-Improvement Collaborative to
Reduce Late-Onset Sepsis in Preterm Infants
WHAT’S KNOWN ON THIS SUBJECT: Late-onset infections cause significant morbidity and mortality in preterm infants. Quality-improvement interventions focused on catheter care have reduced nosocomial infections in adult and pediatric patients but have yet to be proven effective in preterm neonates.
WHAT THIS STUDY ADDS: This study extended previous work, and the results showed that increased application of evidence-based catheter care as part of a state-evidence-based quality-improvement collaborative can reduce infections in preterm neonates. It also highlights the important role of reliability principles in evidence implementation.
abstract
OBJECTIVE:We aimed to reduce late-onset bacterial infections in in-fants born at 22 to 29 weeks’ gestation by using collaborative quality-improvement methods to implement evidence-based catheter care. We hypothesized that these methods would result in a 50% reduction in nosocomial infection.
PATIENTS AND METHODS:We conducted an interrupted time-series study among 24 Ohio NICUs. The intervention began in September 2008 and continued through December 2009. Sites used the Institute for Healthcare Improvement Breakthrough Series quality-improvement model to facilitate implementation of evidence-based catheter care. Data were collected monthly for all catheter insertions and for at least 10 observations of indwelling catheter care. NICUs also submitted monthly data on catheter-days, patient-days, and episodes of infection. Data were analyzed by using statistical process control methods.
RESULTS:During the intervention, NICUs submitted information on 1916 infants. Of the 242 infections reported, 69% were catheter asso-ciated. Compliance with catheter-insertion components was⬎90% by April 2009. Compliance with components of evidence-based indwelling catheter care reached 80.4% by December 2009. There was a signifi-cant reduction in the proportion of infants with at least 1 late-onset infection from a baseline of 18.2% to 14.3%.
CONCLUSIONS:There was a 20% reduction in the incidence of late-onset infection after the intervention, but the magnitude was less than hypothesized, perhaps because compliance with components of evidence-based care of indwelling catheters remained⬍90%. Because nearly one-third of infections were not catheter associated, improve-ment may require attention to other aspects of care such as skin integrity and nutrition.Pediatrics2011;127:427–435
AUTHORS:Heather C. Kaplan, MD, MSCE,a,bCarole
Lannon, MD, MPH,bMichele C. Walsh, MD, MSE,cand
Edward F. Donovan, MD,bfor the Ohio Perinatal Quality
Collaborative
aPerinatal Institute andbJames M. Anderson Center for Health
Systems Excellence, Cincinnati Children’s Hospital Medical Center, Cincinnati, Ohio; andcDivision of Neonatology, Case
Western Reserve University, Cleveland, Ohio
KEY WORDS
infection, catheters, indwelling, infant, premature, quality improvement
ABBREVIATIONS QI—quality improvement IRB—institutional review board
OPQC—Ohio Perinatal Quality Collaborative VON—Vermont Oxford Network
CDC—Centers for Disease Control and Prevention CSF—cerebrospinal fluid
CONS—coagulase-negativeStaphylococcus
SPC—statistical process control
Preliminary results of this study were presented as a platform at the Pediatric Academic Societies meeting; May 3, 2010; Vancouver, British Columbia, Canada.
www.pediatrics.org/cgi/doi/10.1542/peds.2010-2141
doi:10.1542/peds.2010-2141
Accepted for publication Nov 19, 2010
Address correspondence to Heather C. Kaplan, MD, MSCE, Cincinnati Children’s Hospital Medical Center, 3333 Burnet Ave, MLC 7009, Cincinnati, OH 45229. E-mail: heather.kaplan@cchmc. org.
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2011 by the American Academy of Pediatrics
Late-onset (⬎72 hours of life) bacte-rial bloodstream infections occur in 15% to 30% of preterm infants and are a significant source of morbidity, mor-tality, and added health care costs.1,2A
majority of these infections are be-lieved to be associated with the use of indwelling vascular catheters.3,4
Quality-improvement (QI) interven-tions focused on catheter care have re-duced nosocomial infection rates in adult and PICUs. Among 108 adult ICUs participating in a QI intervention, at-tention to evidence-based catheter care resulted in a 66% reduction in catheter-associated bloodstream in-fections.5 Similarly, use of
evidence-based catheter care practices resulted in a 43% reduction in catheter-associated bloodstream in-fections among a group of PICUs.6
Strategies that result in decreased in-fection rates in adults and older chil-dren may have similar effects in pre-term infants. However, preterm infants present special challenges re-lated to relative immunologic immatu-rity, compromised skin integimmatu-rity, long lengths of hospital stay, and long dura-tion of catheter use.
Our objective was to reduce the inci-dence of late-onset infections in in-fants born at 22 to 29 weeks’ gestation in 24 NICUs in Ohio by using collabora-tive QI methods designed to increase the use of evidence-based central cath-eter care. We hypothesized that reli-able, simultaneous implementation of multiple aspects of catheter care (⬎90% of opportunities) would result in an aggregate 50% reduction in the incidence of nosocomial infections.
METHODS
Study Design
We conducted a multisite, interrupted time-series study. Historical compari-son (baseline) data were obtained for the period from April 2006 through Au-gust 2008. The intervention began
Sep-tember 2008 and continued for 15 con-secutive months. The study was approved by the institutional review board (IRB) of the Cincinnati Children’s Hospital Medical Center. All participat-ing NICUs received either IRB approval or were classified as exempt from IRB review. Templates used by teams to prepare their IRB submission and to execute agreements for data sharing are available on the Ohio Perinatal Quality Collaborative (OPQC) Web site (www.opqc.net/toolkit).
Ohio Perinatal Quality Collaborative
The OPQC is a state-based network of Ohio perinatal care clinicians, hospi-tals, professional organizations, and state agencies with a mission to re-duce preterm births and improve out-comes of preterm infants. Participat-ing hospitals and clinicians are supported by a central staff with QI ex-pertise and an administrative and data management infrastructure.7
NICU Participants and Patient Population
All Ohio NICUs that were members of the Vermont Oxford Network (VON) very low birth weight registry were el-igible to participate (n⫽26). Senior administrators at hospitals with eligi-ble NICUs were required to approve participation. The 24 NICUs that elected to participate include all Ohio NICUs designated by the Ohio Department of Health as level 3 neonatal programs.
Infants were included if they were born between 22 and 29 weeks’ gestational age inclusive and were admitted to a participating NICU before 28 days after birth.
Interventions: Catheter Care
On the basis of local unpublished data, we determined that ⬎75% of late-onset infections were associated with catheters. Therefore, the OPQC chose
to focus on catheter care during inser-tion and thereafter (maintenance) un-til the catheter was removed. On the basis of suggestions from the Centers for Disease Control and Prevention (CDC)8and existing toolkits,6,92
compi-lations of recommendations for stan-dardized catheter care (bundles) were developed, 1 for care during catheter insertion and 1 for ongoing care (maintenance) (Table 1).
Interventions: QI
The OPQC used standardized collabo-rative QI methods based on the Break-through Series Collaborative Model of the Institute for Healthcare Improve-ment.10 Participating NICUs identified
multidisciplinary teams that partici-pated in 3, day-long, face-to-face learn-ing sessions (September 2008, Janu-ary 2009, and October 2009). NICUs were asked to create a team that con-sisted of a physician, a nurse, a data manager, and as many as 3 additional members. Between learning sessions, teams participated in monthly Web-based seminars, which were used to share aggregate and site-specific re-sults and strategies for change.
Data were analyzed by OPQC staff and provided to teams in a monthly progress report that included their in-dividual site results, aggregate collab-orative results, and deidentified com-parison results for other participating NICUs.
During the 15-month intervention pe-riod, each team was counseled to use the “plan-do-study-act” method11to
im-plement components of the catheter bundles.
Data Source and Measures
registry that was transmitted monthly for analysis. VON data were available for 13 sites for the entire baseline pe-riod. Two sites had baseline data for 20 months before the intervention. The re-maining 9 sites reported baseline data for 6 to 8 months before the interven-tion. After a 1-month run-in period, teams submitted data monthly on bun-dle compliance for all catheter inser-tions and for at least 10 observainser-tions of indwelling-catheter care. NICU teams also submitted data monthly on total days of catheter use, NICU patient-days, and selected character-istics of each infection. These data were collected by NICU teams by using forms that were pilot tested and re-fined on the basis of feedback from
several sites and were entered into the OPQC Internet-based data-entry tem. The Internet-based data-entry sys-tem was designed with specific
valida-tion rules to improve data quality. In addition, data were reviewed monthly for potential errors (eg, catheter-days equal to patient-catheter-days, increases in reported values for a given month compared with previous months,
etc). Teams were contacted and asked to resolve any data concerns. External audits of source data were not conducted.
Process measures included
compli-ance with the specified care bundles. Use of each bundle component was an-alyzed separately. An all-or-none
mea-sure of the percentage of observations during which all bundle components were used was also calculated.12
Because it was the only measure for which baseline data were available, the primary outcome, obtained from the VON registry, was the proportion of eligible infants with at least 1 late-onset nosocomial infection. Nosoco-mial infection was defined according to the VON manual of operations to in-clude: (1) a positive bacterial culture of blood or cerebrospinal fluid (CSF) obtained 72 hours or more after birth, or (2) a positive blood or CSF culture for coagulase-negative Staphylococ-cus(CONS) obtained 72 hours or more after birth and associated with gener-alized symptoms of illness and for which the infant received antibiotics for ⱖ5 days.13 For monthly graphic
evaluation of the primary outcome, in-fants were plotted according to their month of discharge, which means that improvements noted on the control charts may reflect changes in care in-stituted in earlier months. An infection was labeled as catheter-associated if there was a catheter in place or the catheter was removed⬍48 hours be-fore the positive blood culture results were obtained.
Analyses
In the primary analyses we examined whether there were changes in aggre-gate results summed over the 24 par-ticipating NICUs. Statistical process control (SPC) was the primary method used to detect changes in processes and outcomes.14For the primary
out-come, baseline mean and control lim-its were calculated and displayed for the period from April 2006 through Au-gust 2008. The upper and lower control limits reflected the inherent variation in the data and were calculated at⫾3 SEs of the mean (based on the bino-mial distribution). The baseline mean was carried forward and displayed
TABLE 1 Bundles for Safe Catheter Insertion and Maintenance
Safe catheter insertion
Assessment of need for catheter insertion Use of maximal sterile barriers
Patient covered in full-body (head-to-toe) drape Inserter wears mask, hat, sterile gown/gloves Assistants wear mask, hat, sterile gown/gloves Face mask worn by those within 3 ft of sterile field
Excellent hand hygiene: inserter performs hand hygiene before gloving Supplies available: all supplies required available at bedside before insertion
Appropriate site preparation: skin preparation agent completely dry at time of first skin puncture Ability to stop the line: if problems encountered maintaining sterile field, observers stopped the
procedure Safe catheter maintenance
Daily assessment
Assessment of whether the catheter should be retained or removed occurs daily Dressing integrity and site cleanliness assessed daily (at minimum)
Site care
If dressing change performed
Site cleansed with an appropriate solution (povodone-iodine, CHG, or alcohol) Cleansing solution allowed to air dry completely
Use of a closed system: closed system maintained for infusion, blood draws, and medication administration; closed system is one in which entries are made through needle less connectors or hubs that have been disinfected before use
Catheter access
For all catheter entries/access
Scrub needle less connector or hub using friction with alcohol or CHG forⱖ15 s Allow surface of connector or hub to dry before entry
Staff wear clean gloves when accessing or entering catheter (if not using closed system) Staff perform hand-hygiene before and after access or entry
Tubing care For tubing changes
Staff wear clean gloves (at minimum)
Staff use sterile or clean barrier for tubing assembly
Prefilled flush: use prefilled flush containing syringes for all catheter flushes; prefilled means that syringes were filled with flush solution either by the manufacturer or in pharmacy using sterile technique
throughout the intervention period. Data values were added monthly and monitored for evidence of significant change by using standard SPC rules, including the presence of (1) 1 point outside the upper or lower control lim-its, (2) 2 of 3 successive points in the outer third of the control limit, (3) 8 successive points above or below the center line, or (4) 6 consecutive points increasing or decreasing.14We
deter-mined a priori that if 1 of these criteria were met, we would conclude that a significant change occurred.
On the basis of the results of the PICU collaborative,6 we posited
that maintenance-bundle compliance would be directly related to reduction in infection. Therefore, we planned a subgroup analysis to determine if there was an association between maintenance-bundle compliance and infection incidence. Infection rates among NICUs that failed to achieve an average of 90% compliance with the maintenance bundle for the last 3 months of the intervention period were compared with NICUs that achievedⱖ90% compliance. Because baseline comparison data were not available, process-of-care measures were plotted monthly without mean or control limits, so that we could ob-serve general patterns.
RESULTS
Twenty-four NICUs participated in the study. Of these, 20 were maternity hos-pitals and 4 were freestanding chil-dren’s hospitals. All hospitals were lo-cated in urban areas. Sixteen (66.6%) of the participating NICUs trained res-idents and 13 (54.2%) trained fellows. According to birth certificate data, these hospitals care for⬎90% of Ohio infants born at 22 to 29 weeks’ gesta-tion. During the intervention period, 1916 eligible infants were discharged from OPQC NICUs. The range among hospitals was 209 infants in the largest
hospital and 10 infants in the smallest hospital. The average baseline preva-lence of late-onset nosocomial infec-tion in infants 22 to 29 weeks’ gesta-tion among the 24 NICUs (in aggregate) was 18.2%. During the intervention pe-riod, NICUs submitted information on 125 150 days of patient care including 42 612 days (34%) with indwelling catheters. There were 242 infections of which 69% were catheter associated and 121 (50%) were caused by bacte-ria other than CONS, most frequently
Staphylococcus aureus (26%), Kleb-siella species (14%), Escherichia coli
(14%), and Enterococcus species (12%).
Improvements in Processes of Care and Outcomes
Aggregate compliance with all
catheter-insertion components was
⬎90% by April 2009 (Fig 1A). For the last 3 months of the intervention pe-riod, among sites that submitted at least 30 maintenance-bundle
observa-tions (n ⫽ 17), maintenance-bundle compliance among NICUs ranged from 8% to 100%. Nine sites (53%) achieved maintenance-bundle compliance of
ⱖ90% by the end of the intervention period. Aggregate compliance with all components of the maintenance bun-dle reached 80.4% by the end of the FIGURE 1
intervention period (Fig 1B). Daily doc-umentation of assessment of catheter necessity, use of prefilled flush sy-ringes, and use of a closed system were the slowest bundle components to improve (Fig 1C).
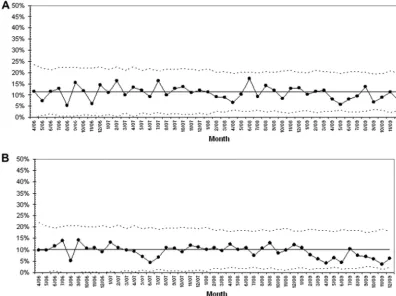
In the postintervention period, there was a reduction in the proportion of infants with infection (Fig 2A). In the 3-month period from April through June 2009,
the proportion of infants with
infec-tions was consistently low, in the outer third of the control limits, which indi-cated a significant change based on a priori SPC rules. On the basis of these findings and the concurrent improve-ments in our processes of care, we
ad-justed the baseline mean and control limits for the period from April 2006 through December 2008 (average
in-fection rate of 18.2%) and from Janu-ary 2009 through December 2009 (av-erage infection rate of 14.0%). In the period immediately before significant improvement was documented (April 2009), January 2009 was the first month during which the infection rate was con-sistently below the historical baseline.
Significant change (8 points below the mean) was seen in the 9 sites with high FIGURE 2
maintenance-bundle compliance (Fig 2B). There was also improvement in the sites with lower maintenance-bundle compliance (Fig 2C), although this improvement occurred later in the intervention period and was of a smaller magnitude. When we exam-ined the reduction in the proportion of infants with infections related to bac-terial pathogens other than CONS ver-sus infections related to CONS, it seems that there were greater reduc-tions in CONS infecreduc-tions (Fig 3).
DISCUSSION
The OPQC has extended the findings of other investigators by showing that a state-based, improvement collabora-tive that includes all Ohio level 3 NICUs can be used to reduce NICU-associated infections. This finding confirms con-clusions drawn from similar efforts in adult and PICUs.5,6It is also consistent
with findings from improvement
ef-forts that focused on the application of evidence-based catheter-care princi-ples and infection reduction in pre-term infants.9,15–17 Thirteen California
NICUs collaboratively demonstrated a 25% reduction in catheter-associated infection rates from 4.3 to 3.2 per 1000
line days.9Similarly, 6 VON NICUs
col-laboratively reduced the proportion of infants with nosocomial infections from 26.3% to 20.9% and the rate of CONS infections from 22% to 16.6%.17
The OPQC achieved a similar 20%
re-duction in the overall incidence of in-fection, likely driven by reductions in infections caused by CONS.
The OPQC effort provides support for
the important role of reliability princi-ples in improving the application of ev-idence in practice.18The initial theory
driving OPQC interventions was that
to reduce infections, evidence-based
catheter care would need to be applied consistently in⬎90% of care opportu-nities. Although a cutoff of 90% still means that there is a 1 in 10 chance
that suboptimal care will be provided, the achievement of 90% reliability indi-cates that a specific common process exists for the application of evidence in practice.18Subgroup analysis in which
sites with compliance of ⱖ90% with the maintenance bundle components were compared to those with compli-ance of⬍90% supports this theory in that it shows greater improvement
among the NICUs with higher compli-ance. NICUs that achieved high
reliabil-ity moved beyond educational
strate-gies and focused on changes such as
the institution of specific protocols to
standardize the timing of catheter re-moval and the addition of questions FIGURE 3
about catheter necessity to templates in the medical record.
Another unique contribution was the attention paid to the reduction of both catheter-associated and non– catheter-associated infections. Al-though the intervention focused ini-tially on the implementation of evidence-based catheter care, the par-ticipating NICUs had a high degree of belief that a comprehensive approach to infection was necessary. The adop-tion of the proporadop-tion of infants with at least 1 bacterial infection (catheter as-sociated or non– catheter asas-sociated) as the primary outcome measure, al-though perhaps a less sensitive mea-sure of catheter-associated infection, allows the OPQC to continue to test subsequent interventions related to other portals of entry for invasive in-fections, including the skin, respira-tory tract, and gastrointestinal tract. A similar approach may be useful to other QI collaborative groups that have successfully reduced catheter-associated infections and are now poised to tackle other key processes unrelated to catheter care.
Our study design did not include a con-temporaneous control group. Thus al-ternative explanations for the change in infection rates cannot be excluded. At the start of the OPQC intervention, participating NICUs had an aggregate nosocomial infection rate lower than that reported for the entire VON net-work. This lower baseline rate may indicate that many of the OPQC NICUs were already actively working on in-fection reduction. However, addi-tional reductions were seen during the OPQC intervention. Infections among comparable infants dis-charged from hospitals participating in the VON network have declined minimally over a similar time period. Unpublished data from the VON Nightingale Web site indicates that the incidence of late-onset
nosoco-mial infection decreased from 27.3% to 24.7% from 2006 to 2008.
We chose to use the VON measure of late-onset nosocomial infection as the primary outcome measure because participating NICUs had processes in place to collect these data and consid-erable baseline data were available. Some collaborative groups have used measures defined by the CDC National Health Care Safety Network to monitor changes in infection rates.6,9The OPQC/
VON definition focuses on bloodstream and CSF infections regardless of the source, whereas the CDC definition al-lows for exclusion of infections in which the organism may have been re-lated to infection at another site and therefore tends to identify infections that can be more directly attributed to the presence of an indwelling catheter. In addition, the CDC definition requires isolation of bacteria from 2 blood cul-tures along with generalized signs of illness to classify an infection as being related to organisms that are gener-ally considered skin contaminants. Ac-cording to the OPQC/VON definition, an infection is related to a skin contami-nant when it is associated with a single positive culture, generalized symp-toms of illness, and treatment with an-tibiotics forⱖ5 days. We believe that the CDC definition captures a subset of all NICU-associated infections; how-ever, direct comparisons of results ob-tained by use of these 2 definitions have not been performed. Among transferred infants, before January 2009, VON data did not differentiate be-tween infections that occurred at the transferring hospital and those that occurred subsequent to admission at the accepting hospital. Although this lack of differentiation may have had a significant impact on the rates of infec-tion calculated for individual hospitals, particularly for those hospitals with mainly outborn infants, in aggregate this effect was unlikely to have led to
variation in results calculated for the baseline and intervention periods. OPQC used various methods to pro-mote data quality including using es-tablished data sources (eg, VON regis-try data) and building data quality checks into the Internet-based data collection system. Although we did not conduct site audits, we believe our other data quality processes and ef-forts to create a culture where sharing results (even negative ones) and learn-ing from data were the norm, serve to reduce the likelihood that sites were systematically under-reporting infections.
The magnitude of the reduction experi-enced by the OPQC was less than the hypothesized reduction. We believed that evidence-based catheter care must be applied inⱖ90% of instances to achieve significant improvements in outcomes. However, by the end of the intervention period, maintenance-bundle compliance had reached only 80%. It is possible that NICUs must achieve higher reliability before more significant reductions in infection can be seen. In addition, because NICUs that participated in the OPQC started with a lower infection rate than that seen in previous collaborative group efforts17, and only 69% of infections
were reported to be catheter associ-ated, the magnitude of the effect attributable to improved catheter care may have been smaller than initially hypothesized.
CONCLUSIONS
other care practices unrelated to cath-eters may be needed to effect larger decreases in infections. Future re-search should explore the impact of evidence-based nutrition (eg, human milk) and skin care practices applied to further reduce the incidence of infection.
ACKNOWLEDGMENTS
This work was supported in part by grant 1U0CMS030227/01 from the Cen-ter for Medicare and Medicaid Ser-vices administered by the Ohio Depart-ment of Job and Family Services.
OPQC participating hospitals and key improvement team members included Akron Children’s Hospital, Akron: Kim Firestone, Anand Kantak, and Judy Ohlinger; St Elizabeth Health Center, Youngstown: Linda Beilstein, Carrie Cannon, Patricia Hray, Diane L. Pitts, and Elena Rossi; Aultman Hospital, Canton: Corena Albert, Brenda Doug-lass, Fran Kessler, and Jamie Mosnot; Cincinnati Children’s Hospital Medical Center, Cincinnati: Pattie Bondurant, Claire Burkhart, Cathy Grisby, Beth Haberman, and Debbie Hershberger; Cleveland Clinic, Cleveland: John Baker, Carol Bennett, Marita DiNetto, Rita Eakins, Greg Gagliano, and Amy Toth; Dayton Children’s Medical Cen-ter, Dayton: Karen Beekman, Lisa Jasin, Alicia Link, Jennifer Morris, and Jerod Rone; Fairview Hospital, Cleveland: Laura Bobek, Louana Dickey, Patricia Kaser, Jeffrey Pietz, and Denise Speer; Good Samaritan Hospital, Cincinnati: Juanita Dudley, Laura Harris, Amy Nathan, Cheri Potts, Kurt Schibler, and Janet Sherrod; Hillcrest Hospital,
May-field: Sue Levar, Jeffrey Schwersenski, Susan Shirey, and Christine Walton; MetroHealth Medical Center, Cleve-land: Marc Collin, Monica Fundzak, and Maroun Mhanna; Miami Valley Hospi-tal, Dayton: Marc Belcastro, Sue Mackey, and Tracy Morrison; Mount Carmel East Hospital, Columbus: Ehab Ahmed, Marcia Garrett, Debbie LaJeu-nesse, Theresa Lombardo, Jennifer Notestine, and Kathy Sturges; Mount Carmel St Ann’s Hospital, Westerville: Jill Beverly, Sandy Conte, Martha Mey-ers, Randy Miller, Ann Peeples, and Gary Snyder; Mount Carmel West Hos-pital, Columbus: Marcia Garrett, Barry Halpern, Mickey Johnson, and Laura Shade; Nationwide Children’s Hospital, Columbus: Gail Bagwell, Al Gest, John Hitchner, Tami Kelly, Jodi Lowe, Renee Miller, Joanna Sutton, and Rick Taylor; Doctor’s Hospital, Columbus: Dan Mall-eske and Stephanie Stafford; Grant Hospital, Columbus: Margaret Holston, Brandon Kuehne, and Apurwa Naik; Riverside Hospital, Columbus: Carol Jaeger, Kari Kennedy, and Pat Wall; St Vincent Mercy Medical Center, Toledo: Moustafa M. Aouthmany, Jennifer Roe, Paula Samples, and Joan Zolla Bold; Summa Health Systems, Akron: Theresa Flohr, Karen Frantz, Jennifer Grow, and Debbie Seiber; Ohio State University Medical Center, Columbus: Shelly Biggs, Leandro Cordero, Cynthia Jenkins, Michael Popa, Michele Sweet, and David Taylor; Toledo Children’s Hospital, Toledo: Barbara Chappell, Debbie Fritz, Vicky Gall, Judy Gresky, Mary Moore, Joan Ruff, and Howard Stein; University Hospital, Cincinnati: Linda Croop, Vivek Narendran, and
Emily Rosenberg; University Hospital Case Medical Center and Rainbow Ba-bies & Children, Cleveland: Beverly Capper, Kathleen Deakins, Jonathan Fanaroff, Kathleen Haas, Elie Abu Jaw-deh, Tina Lewis, Ann Reitenbach, Amy Seekely, and Michele Walsh; OPQC Exec-utive Committee: Mary Applegate, Gail Bagwell, Jennifer Bailit, Marc Belcas-tro, Jo Bouchard, Barbara Chappell, Ronda Christopher, Lori Deacon, Ed Donovan, Kelly Friar, Al Gest, Pat Hein-rich, Karen Hughes, Jay Iams, Anand Kantak, Heather Kaplan, Karen Keller, Carole Lannon, Michael Marcotte, Rick McClead, Dave McKenna, Brian Mercer, Barbara Rose, Craig Strafford, Mary Ann Swank, and Michele Walsh; for the Ohio Department of Health: Jo Bou-chard, Lori Deacon, Kelly Friar, Karen Hughes, Mark Kassouf, John Paulson, and Bev Wargo; for the Ohio Depart-ment of Job and Family Services: Mary Applegate, Karen Keller, Debbie Clem-ent Saxe, and Michael Wiggins; for the VON: Joseph Carpenter, Nancy Cloutier, Jeffrey Horbar, Ted Krieder, Kathy Leahy, A. Lynn Stillman, and Pete Warner; project directors and staff, Ohio Department of Health Regional Perinatal Center Program Grants, Re-gion I, Cincinnati: Kathy Hill; ReRe-gion II, Dayton: Mary Ann Swank; Region III, To-ledo: Debbie Fritz; Region IV, Columbus: Corey F. Ferguson; Region V, Cleveland: Marilyn Benjamin; Region VI, Akron: Judy Orosz and Connie Teal; OPQC Cen-tral Administration: Harry Atherton, John Besl, Ronda Christopher, Diana McClendon, Barbara Rose, Tim Sal-vage, Sang Sam, Kenneth Matthew Short, and Mariea Taylor.
REFERENCES
1. Makhoul IR, Sujov P, Smolkin T, Lusky A, Reichman B. Epidemiological, clinical, and microbiological characteristics of late-onset sepsis among very low birth weight infants in Israel: a national survey. Pediat-rics. 2002;109(1):34 –39
2. Stoll BJ, Hansen N, Fanaroff AA, Wright LL, Carlo WA, Ehrenkranz RA, et al. Late-onset
sep-sis in very low birth weight neonates: the ex-perience of the NICHD Neonatal Research Net-work.Pediatrics. 2002;110(2 pt 1):285–291 3. Chien LY, Macnab Y, Aziz K, Andrews W,
McMil-lan DD, Lee SK. Variations in central venous catheter-related infection risks among Cana-dian neonatal intensive care units.Pediatr In-fect Dis J. 2002;21(6):505–511
4. Perlman SE, Saiman L, Larson EL. Risk fac-tors for late-onset health care-associated bloodstream infections in patients in neo-natal intensive care units.Am J Infect Con-trol. 2007;35(3):177–182
blood-stream infections in the ICU.N Engl J Med. 2006;355(26):2725–2732
6. Miller MR, Griswold M, Harris JM 2nd, et al. Decreasing PICU catheter-associated bloodstream infections: NACHRI’s quality transformation efforts. Pediatrics. 2010; 125(2):206 –213
7. Ohio Perinatal Quality Collaborative Writing Committee. Collaborative improvement of population perinatal health in Ohio: study de-sign, methods, and provider site participa-tion. Available at: www.opqc.net/sites/ bmidrupalpopqc.chmcres.cchmc.org/files/ docs/articles/EdManuscript.pdf. Accessed July 7, 2010
8. National Nosocomial Infections Surveil-lance (NNIS) System Report, data summary from January 1992 through June 2004, is-sued October 2004. Am J Infect Control.
2004;32(8):470 – 485
9. Wirtschafter DD, Pettit J, Kurtin P, et al. A statewide quality improvement collabora-tive to reduce neonatal central
line-associated blood stream infections.J Peri-natol. 2010;30(3):170 –181
10. Institute for Healthcare Improvement.The Breakthrough Series: IHI’s Collaborative Model for Achieving Breakthrough Improve-ment. Boston, MA: Institute for Health Care Improvement; 2003. IHI Innovation Series white paper. Available at: www.IHI.org. Ac-cessed December 10, 2010
11. Langley GL, Nolan KM, Nolan TW, Norman CL, Provost LP.The Improvement Guide: A Practi-cal Approach to Enhancing Organizational Performance. San Francisco, CA: Jossey-Bass; 1996
12. Nolan T, Berwick DM. All-or-none measure-ment raises the bar on performance.JAMA. 2006;295(10):1168 –1170
13. Vermont Oxford Network. Manual of opera-tions for infants born in 2008. Release 12.1, Updated February 2008. Available at: www.vtoxford.org/tools/2008Manualof Operationswithindex12_1.pdf. Accessed De-cember 10, 2010
14. Benneyan JC, Lloyd RC, Plsek PE. Statistical process control as a tool for research and healthcare improvement. Qual Saf Health Care. 2003;12(6):458 – 464
15. Powers RJ, Wirtschafter DW. Decreasing central line associated bloodstream infec-tion in neonatal intensive care.Clin Perina-tol. 2010;37(1):247–272
16. Schulman J, Stricof RL, Stevens TP, et al. Development of a statewide collaborative to decrease NICU central line-associated bloodstream infections. J Perinatol. 2009; 29(9):591–599
17. Horbar JD, Rogowski J, Plsek PE, et al. Collaborative quality improvement for neonatal intensive care. NIC/Q Project In-vestigators of the Vermont Oxford Net-work.Pediatrics. 2001;107(1):14 –22 18. Luria JW, Muething SE, Schoettker PJ,
Kota-gal UR. Reliability science and patient safety.Pediatr Clin North Am. 2006;53(6): 1121–1133
LIVING LONGER:The other night, we had my parents over for dinner. After they left, a friend of mine remarked, “Your parents don’t make getting old look easy.” My father, whose mind is razor sharp, has had a heart attack and because of joint problems and being overweight, can sometimes hardly walk. He has, how-ever, lived longer than any other member of his family. My mother, whose cognitive function is not as sharp, carries with her at all times a remarkably large pill box for her various chronic medical conditions and can hardly use her hands because of arthritis. A day that does not involve a physician or therapist visit for one of them is considered a great day and seen as a rare event. As reported inThe New York Times(December 27, 2010: Health) Americans, like my parents, are indeed living longer than ever, but the added years are more likely to include living with conditions such as heart disease, stroke, cancer, diabetes and significant physical disability. According to the article, researchers comb-ing published US morbidity and mortality data from the last decade and a half concluded that people live longer not because they are less likely to get sick, but because they survive longer with disease. Their data suggest that 20-year-old men today can expect to live about a year longer than men who were 20-years-old in 1998. However, today’s 20-year-20-years-old men will spend approximately one more year with disease and two years without full mobility. While I am thrilled that I still get to see my parents, and hope I can continue to have dinners with them for many more years to come, I can’t help but be reminded a tiny bit of Tithonus, the lover of Eos, whom Zeus granted immortality but not eternal youth. So, when I have dinner with my own 20-year-old son, I counsel him that asking for immortality has always been a bad request. Putting practices that improve and ensure better long term health into place at an early age seems to be the way to go.
DOI: 10.1542/peds.2010-2141 originally published online February 21, 2011;
2011;127;427
Pediatrics
the Ohio Perinatal Quality Collaborative
Heather C. Kaplan, Carole Lannon, Michele C. Walsh, Edward F. Donovan and for
in Preterm Infants
Ohio Statewide Quality-Improvement Collaborative to Reduce Late-Onset Sepsis
Services
Updated Information &
http://pediatrics.aappublications.org/content/127/3/427
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/127/3/427#BIBL
This article cites 14 articles, 5 of which you can access for free at:
Subspecialty Collections
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_ Fetus/Newborn Infant
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2010-2141 originally published online February 21, 2011;
2011;127;427
Pediatrics
the Ohio Perinatal Quality Collaborative
Heather C. Kaplan, Carole Lannon, Michele C. Walsh, Edward F. Donovan and for
http://pediatrics.aappublications.org/content/127/3/427
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.