Vol. 46, No. 3, pp. 331 - 340, 2005
The purpose of this study was to develop and test a struc-tural model explaining medication compliance of schiz-ophrenia. From a review of the literature, a hypothetical model was developed based on the conceptual framework of the Health Belief Model with medication knowledge, symptom severity and social support as the exogenous variables, and perceived benefits, perceived barriers, substance use and medication compliance as the endogenous variables. Data was collected at various mental health facilities, including psychi-atric outpatient clinics of general hospitals and community mental health centers, between March and May, 2001. A structured questionnaire was used by one- on- one interviews to collect data on 208 schizophrenic patients. Well established measurement instruments, with confirmed reliability, were used to assess each method variable. As a result of covariance structural analysis, the hypothetical model was found not to fit the empirical data well, so a parsimonious model was adopted after modifying the model. The final model was able to explain the 33% medication compliance. Medication knowledge, social support and perceived benefits had significant effects on medication compliance. The findings of this study address the importance of medication education and social support to promote medication compliance. It is also suggested that various education programs and support groups are needed to enhance medication compliance.
Key Words: Medication compliance, schizophrenia
INTRODUCTION
Medication compliance is essential in managing
the psychotic symptoms of schizophrenic patients. However, it has been reported that 65.8% of mentally ill patients had experiences of taking their medication at different times and with dif-ferent dosages from those prescribed by their doctor.1 Medication noncompliance leads to a
lapse of symptoms and rehospitalization. A re-lapse rate of 16% over one year was reported when schizophrenic patients took their medication as their doctors ordered, but this was 74% when the prescribed regimen was not followed.2
Many variables influencing medication compli-ance in the mentally ill have been identified from prior studies. Medication knowledge,3-5 symptom
severity,6-8social support,9-11 perceived benefits12-14
and barriers,15-17 and substance abuse18-19 have all been well identified as variables influencing medication noncompliance. When patients had no knowledge of their medication, their psychiatric symptoms were serious, but when social support was received from their family, friends and health care providers, medication noncompliance was higher. Alcohol and drug use also interfere with medication compliance.
Even though these variables are well known, prior studies have only revealed the direct effects of these variables on medication compliance; thus, which variables are most influential and impor-tant remain unknown. Therefore, the factors influ-encing medication compliance, and to what degree, either direct or indirect, needs to be examined.
Thus, the development of a comprehensive model explaining chronic schizophrenic patients' medication compliance is required. The more variables included in the model, the higher the explanation power. However, to develop a precise
Development of a Structural Model Explaining Medication
Compliance of Persons with Schizophrenia
Mi-A Seo1 and Sung-Kil Min2
1Department of Social Welfare, Seoul Cyber University, Seoul, Korea;
2Department of Psychiatry, Yonsei University College of Medicine, Seoul, Korea.
Received July 16, 2004 Accepted December 20, 2004
Reprint address: requests to Dr. Mi-A Seo, Department of Social Welfare, Seoul Cyber University, 193 Mia 3-dong, Gangbuk-gu, Seoul 142-711, Korea. Tel: 82-2-944-5014, Fax: 82-2-980-7200, E-mail: [email protected]
and concise model, it is necessary to involve the most influential variables.
The purpose of this study was to develop a comprehensive and parsimonious model expla-ining a schizophrenic patients' medication compli-ance. The model should have a theoretical basis, so that it will be possible to enhance intervention for increased medication compliance.
CONCEPTUAL FRAMEWORK AND A HYPO-THETICAL MODEL
Conceptual framework
The conceptual framework of this study con-sisted of variables identified through a review of the literature as major factors directly or indirectly influencing medication compliance. The concept of Becker's (1974) health belief model,20 in which
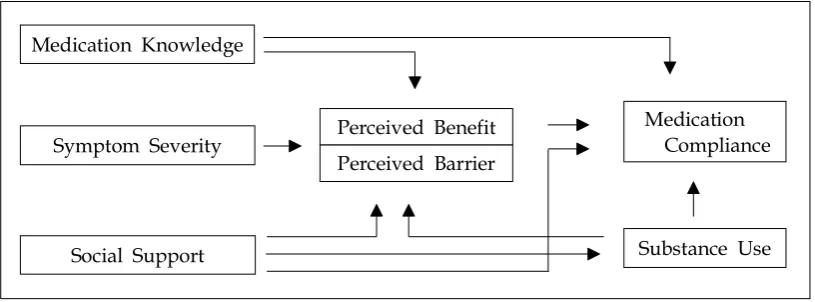
medication compliance is seen as a behavior for improving one's health, was used (Fig. 1). This model has two assumptions: First, that one has a need to avoid or recover from illness; second, one performs a specific behavior to prevent an illness. The Health Belief Model is applicable and useful for psychiatric patients as they perform specific behaviors, such as taking their medication to get over their mental illness.
Hypothetical model
The hypothetical model consisted of three ex-ogenous variables (medication knowledge, symp-tom severity, and social support) and four
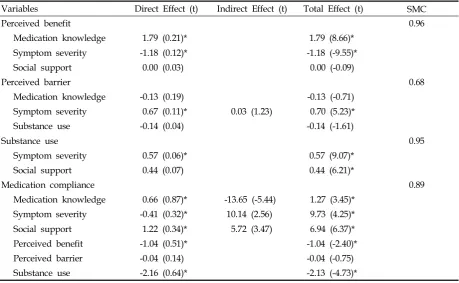
endo-genous variables (perceived benefit, perceived barrier, substance use, and medication compli-ance). The exogenous variables were independent variables influencing the endogenous variables either directly or indirectly. A total of 14 hypo-thetical paths were established (Fig. 2).
MATERIALS AND METHODS
Subjects
The criteria for the study subjects were as follows: 1) Adult schizophrenic patients between the age of 18 and 65 years, diagnosed with a schizophrenia for at least 6 months.
2) A total score on the MMSE (Mini Mental State Examination) over 25 in order to under-stand the questions and correctly answer the questionnaire.
3) Patients currently receiving psychiatric treat-ment and taking medication.
4) Those currently residing in the community. Hospitalized patients were not involved in the sample as hospitalization affects medi-cation compliance.
5) Patients had to verbally agreed to participate in the study
Data collection
[image:2.595.93.501.575.726.2]A pilot study was undertaken to ascertain if all of the questions were understandable, then the questionnaire was administered, on a on-to-one basis, to 34 patients meeting the sample selection
Fig. 1. Conceptual framework.
Medication Knowledge
Perceived Benefit Perceived Barrier
Medication Compliance
Substance Use Symptom Severity
criteria before further study was conducted. Par-ticipants were asked which questions they found difficult or did not understand, with feedback on those items used to modify the questions of easier understanding.
Data were collected between March and May, 2001 through one-on-one interviews. To decrease the sample error, eight provinces were used for data, which was carried out in three general hos-pital out patients' clinics, five community mental health centers in different provinces, one com-munity public health center, one day care center, one doctor's clinic, and in patients' homes. Before going to the mental health care facilities for data collection, the purpose and method of the study was explained to representatives of each facility by letter and phone, and permission received for collecting the data. The purpose of the study was explained to each participant, and those agreeing to participate were interviewed by the researcher. A total of 244 patients meeting the subject selec-tion criteria were interviewed and completed the questionnaire. However, 36 participants' family members were unable to be reached by phone to measure medication compliance; thus, a total of 208 participant's questionnaires were used for the analysis. A one-on-one interview for the
question-naire was undertaken by the researcher, which took 30-40 minutes to complete.
Instruments
Medication knowledge
A total of 14 questions were asked relating to medication knowledge, which was initially pre-sented by Harbor et al. (1996).21 Each question
was answered either 'yes', 'no', or 'don't know', with total scores ranging from 0 to 14; the higher the score, the greater the stress.
Symptom severity
Symptom severity was measured on the BPRS (Brief Psychiatric Rating Scale) developed by Overall et al. (1962).22 This questionnaire consisted
of 18 questions, divided into two parts. One part measured the subjective symptoms, such as degree of anxiety and depression, which consisted of 9 questions. The second part also consisted of 9 questions, and measured the researchers' obser-vations relating to slow movement and non cooperation, etc. The score range of each question was from 1 to 7, with the total scores ranging from 18 to 126; the higher the score, the greater the severity of the symptom. The Cronbach's X1: Taking medicine X4: Medication characteristics X7: Family support Y1: Perceived benefit Y4: Alcohol
X2: Medication effects X5: Subjective symptom X8: Friend support Y2: Cost and stigma Y5: Smoking X3: Cautions X6: Objective symptom X9: Health professional support Y3: Side effects Y6: Substance use
0.66 X1
X2 X3 X4
X5 X6
X7 X8 X9
ξ1 Medication Knowledge
ξ2 Symptom
Severity
ξ3 Social Support
η1 Perceived
Benefit
η2 Perceived
Barrier
Y1
Y2 Y3
Y6
Y4 Y5 0.41
0.57 0.48
0.44 0.00
0.67 -1.18 -0.13
1.79
-1.04
-0.04
-0.14
η4 Medication Compliance
η3 Substance
[image:3.595.104.523.97.334.2]Use -2.16
alpha was 0.95 in this study.
Social support
Sarason's (1983) social support questionnaire23
was used to measure family, friend and health care provider support. A total of 8 questions were asked, including the degree of satisfaction about people they can trust, with each question having a 6-point Likert style answer, from 'very unsat-isfied' to 'very satunsat-isfied'. The total scores ranged from 8 to 48; the higher the score, the greater the degree of social support. The Cronbach's alpha in the study was 0.92.
Perceived benefit
The perceived benefit refers to the good things that can be attained by medication compliance, which was measured using a modified Korean version of Moon's (1990) health belief question-naire24 for Korean adults; 6 questions were
in-cluded in this questionnaire: symptom improve-ment, decreasing the chance for relapse and improvement of interpersonal relationship, etc. having a 5-point Likert scale. The total scores ranged from 6 to 30; the higher the score, the greater the perceived benefits. The Cronbach's alpha in this study was 0.84.
Perceived barrier
The perceived barriers refer to the difficulties experienced by a person, which were addressed by five items: medication side effects, price, avoiding people's eye, visiting the hospital regularly and trying to follow medication times. This was measured using a modified Korean ver-sion of Moon's (1990) health belief questionnaire24 for Korean adults. Each question had a 5-point Likert scale; with the answers ranging from 'very likely' to 'unlikely'. The total scores ranged from 5 to 25; the higher the score, the greater the perceived barriers. The Cronbach's alpha in this study was 0.65.
Substance use
Substance refers to the psychoactive chemical agents. The substance use questionnaire, devel-oped by the Ministry of Culture and Athletics (1996), was used.25 The amount of alcohol and cigarette uses per day and per month were
mea-sured, with the degree of alcohol use converted to alcohol content; the higher the score, the greater the participant's use of alcohol and cigarettes.
Medication compliance
Medication compliance refers to the behavior of taking the correct medication and dose at the correct time, as prescribed the participant's doc-tors. This was measured in two ways, by self-reporting and from family member's report. The question, 'what age percent have you taken your medication in the past one month? Answer 100% if you took all medication as your doctor pre-scribed', was asked to the patient. The question, 'what age percent has your ill family member taken his/her medication in the past month? Answer 100% if they took the medication as their doctor prescribed', was asked to the participant's family. When it was not possible to contact the participant's family, a data collection phone in-terview of the participant's family member was carried out, with the patients' consent. The mean of the two scores (patient and family) was the par-ticipant's final medication compliance score; the higher the score, the greater the medication com-pliance.
Data analysis
The SPSS PC 11.0 Program was used for de-scriptive statistics, and LISREL 8.12 for covariance analysis for coincidence testing of the hypothetical and modified models.
RESULTS
Demographic characters
There were 126 males (60.8%) and 82 females (39.2%), with a mean age of 38.89 years and a mean age at the onset of schizophrenia of 24.47 years. The mean illness and medication periods were 11.4 and 9.4 years, respectively.
The effects and squared multiple correlation of the hypothetical model
per-ceived benefit and substance use had significant direct effects on medication compliance, with an explanation power of 89%; however, the indices of the hypothetical model did not fit well. Therefore, the model was modified (Table 1).
Testing hypothesis
The hypotheses including perceived benefits as endogenous variables were:
Hypothesis 1 : 'The greater the medication knowledge, the greater the perceived benefit' was supported as a direct effect (r=0.10, t=3.18); signi-ficant.
Hypothesis 2 : 'The more severe the symptoms, the greater the perceived benefit' was not sup-ported as a direct effect (r=0.03, t=0.29) ; not signi-ficant.
Hypothesis 3 : 'The greater the social support, the greater the perceived benefits' was supported as a direct effect (r=0.54, t=8.08) ; significant.
The hypotheses including perceived barriers as endogenous variables were:
Hypothesis 4 : 'The greater the medication
knowledge, the lower the perceived barriers' was not supported as a direct effect (r=-0.07, t=-1.95); significant.
Hypothesis 5 : 'The more severe the symptoms, the greater the perceived barriers' was supported as a direct effect (r=0.90, t=13.76); significant.
Hypothesis 6 : 'The greater the substance use, the greater the perceived barriers' was not supported, as this path was removed.
The hypotheses including substance use as an endogenous variable were:
Hypothesis 7 : 'The more severe the symptoms, the greater the substance use' was supported as a direct effect (r=0.71, t=11.41); significant.
Hypothesis 8 : 'The greater the social support, the lower the substance use' was not supported (r=0.30, t=5.45) ; even though the statistical value was effective, the direction of the effect coefficient did not coincide.
The hypotheses including medication compli-ance as an endogenous variable were:
[image:5.595.67.527.446.729.2]Hypothesis 9 : 'The greater the medication knowledge, the greater the medication compli-ance' was supported as a direct effect (r=0.15,
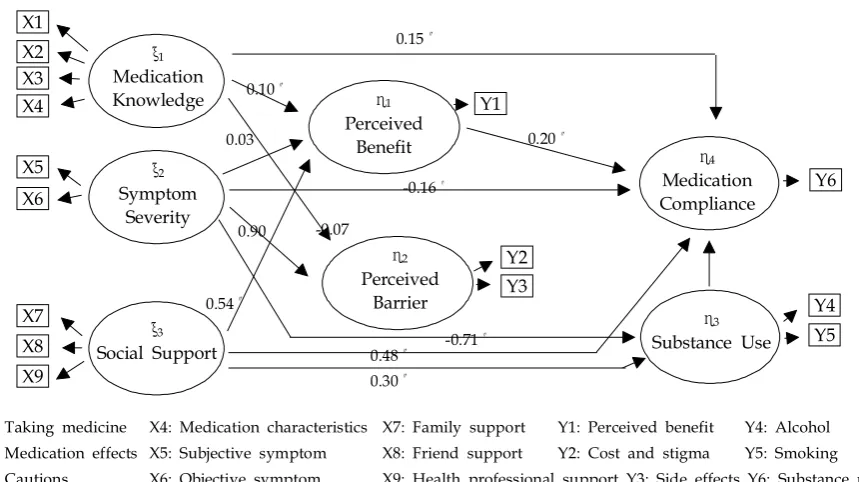
Table 1. Effects of Endogenous Variables for the Hypothetical Model
Variables Direct Effect (t) Indirect Effect (t) Total Effect (t) SMC
Perceived benefit 0.96
Medication knowledge 1.79 (0.21)* 1.79 (8.66)*
Symptom severity -1.18 (0.12)* -1.18 (-9.55)*
Social support 0.00 (0.03) 0.00 (-0.09)
Perceived barrier 0.68
Medication knowledge -0.13 (0.19) -0.13 (-0.71)
Symptom severity 0.67 (0.11)* 0.03 (1.23) 0.70 (5.23)*
Substance use -0.14 (0.04) -0.14 (-1.61)
Substance use 0.95
Symptom severity 0.57 (0.06)* 0.57 (9.07)*
Social support 0.44 (0.07) 0.44 (6.21)*
Medication compliance 0.89
Medication knowledge 0.66 (0.87)* -13.65 (-5.44) 1.27 (3.45)*
Symptom severity -0.41 (0.32)* 10.14 (2.56) 9.73 (4.25)*
Social support 1.22 (0.34)* 5.72 (3.47) 6.94 (6.37)*
Perceived benefit -1.04 (0.51)* -1.04 (-2.40)*
Perceived barrier -0.04 (0.14) -0.04 (-0.75)
Substance use -2.16 (0.64)* -2.13 (-4.73)*
t=3.63); significant.
Hypothesis 10 : 'The more severe the symptoms, the greater the medication compliance' was not supported as a direct effect (r=-0.16, t=-1.80); not significant.
Hypothesis 11 : 'The greater the social support, the greater the medication compliance' was sup-ported as a direct effect (r=0.48, t=7.72); signi-ficant.
Hypothesis 12 : 'The greater the perceived ben-efit, the greater the medication compliance' was supported as a direct effect (r=0.20, t=2.14); signi-ficant.
Hypothesis 13 : 'The lower the perceived bar-riers, the greater the medication compliance' was not supported, as this path was removed.
Hypothesis 14 : 'The greater the substance use, the greater the medication compliance' was not supported as a direct effect (r=0.07, t=1.87); not significant.
Modifying the hypothetical model
The modifying process or the model considered the conciseness, suitability, statistical significance and theoretical meaning. The variables with a correlation above 0.45 were used in the final
[image:6.595.82.512.98.339.2]an-alysis, which was the case with most of the variables in this study. Two paths were removed as their effects were weak and insignificant, and were found to decrease the suitability. These were 'how substance use affected perceived barriers' and 'how perceived barriers affected medication' (Fig. 3).
Fitness of the modified model
The chi-square value of the hypothetical model was too high (842.92), and the other indices also necessitated model modification. After modifica-tion, all indices indicating suitability and concise-ness fitted to the model well, with all ×2 (37.08, df=18,p=0.005), GFI (0.98), AGFI (0.93), RMR (0.05), NNFI (0.97) and CN (283.55) values (Table 2).
The effects and squared multiple correlation of the modified model
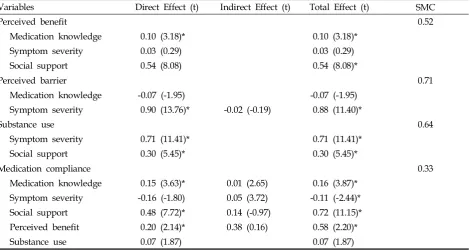
Among the medication knowledge, symptom severity and social support variables, which pre-dict perceived benefits, medication knowledge and social support had significant direct effects, with an explanation power of 52%. Among the medication knowledge, symptom severity and Fig. 3. Path coefficient of the modified model.
X1 X2 X3 X4
X5 X6
X7 X8 X9
ξ1 Medication Knowledge
ξ2 Symptom
Severity
ξ3 Social Support
η1 Perceived
Benefit
η2 Perceived
Barrier
η4 Medication Compliance
η3 Substance Use Y1
Y2 Y3
Y6
Y4 Y5 0.10
0.15
0.20
-0.16
0.48 0.30
-0.71 0.54
0.90 0.03
-0.07
substance use variables, which predict the per-ceived barriers, only symptom severity had a significant direct effect, with an explanation power of 71%. Both symptom severity and social support had significant direct effects on substance use, and both variables listed substance use as 64%. The endogenous variables, which predict medication compliance, were medication knowl-edge, symptom severity, social support, perceived benefits and substance use. Three variables of medication knowledge, social support, and per-ceived benefits had significant direct effects on medication compliance, with an explanation power of 33%; social support had the strongest direct effect among these variables (Table 3).
DISCUSSION
The model developed by structural equation
analysis has to reflect reality and have theoretical validity.26 The aim of this study was to develop
a concise, well fitted model to predict factors and explain their direct and indirect effects on medica-tion compliance. Many variables influencing me-dication compliance in the mentally ill were identified through an extensive literature review. Among the variables identified, six were found to have the most influence on medication compli-ance. The endogenous variables were medication knowledge, symptom severity and social support, with perceived benefits, perceived barriers and substance use as mediating variables. Medication compliance of chronic schizophrenic patients was directly affected by medication knowledge, social support and perceived benefits, with an explana-tion power for these variables of 33%.
[image:7.595.61.539.118.163.2]Prior study results have not been consistent with regards to medication knowledge directly affecting medication compliance. One research
Table 2. Fitness of Indices
κ2 df κ2/df GFI AGFI RMR NNFI NFI CN
Hypothetical model 842.92 (p=0.00) 19 44.36 0.70 0.13 0.84 0.81 0.25 13.92
Modified model 37.08 (p=0.005) 18 2.06 0.98 0.93 0.05 0.97 0.98 283.55
Table 3. Effects of Endogenous Variables for the Modified Model
Variables Direct Effect (t) Indirect Effect (t) Total Effect (t) SMC
Perceived benefit 0.52
Medication knowledge 0.10 (3.18)* 0.10 (3.18)*
Symptom severity 0.03 (0.29) 0.03 (0.29)
Social support 0.54 (8.08) 0.54 (8.08)*
Perceived barrier 0.71
Medication knowledge -0.07 (-1.95) -0.07 (-1.95)
Symptom severity 0.90 (13.76)* -0.02 (-0.19) 0.88 (11.40)*
Substance use 0.64
Symptom severity 0.71 (11.41)* 0.71 (11.41)*
Social support 0.30 (5.45)* 0.30 (5.45)*
Medication compliance 0.33
Medication knowledge 0.15 (3.63)* 0.01 (2.65) 0.16 (3.87)*
Symptom severity -0.16 (-1.80) 0.05 (3.72) -0.11 (-2.44)*
Social support 0.48 (7.72)* 0.14 (-0.97) 0.72 (11.15)*
Perceived benefit 0.20 (2.14)* 0.38 (0.16) 0.58 (2.20)*
Substance use 0.07 (1.87) 0.07 (1.87)
[image:7.595.64.535.199.449.2]report suggested that medication knowledge in-creased after a medication education program, which led to an increase in medication compli-ance.5 However, another study reported that
me-dication education to schizophrenic patients did not change medication compliance, even though their medication knowledge had increased.27
Medication compliance was found to be directly affected by medication knowledge in this study. It is thought that most participants attended an outpatient treatment care center, where they were repeatedly educated about the effects and side effects of the medication and the importance of taking medication for preventing a relapse; thus, they knew about their medication and it increased compliance.
Social support has consistently been identified as a reinforcement factor for medication compli-ance through prior studies.28,29 However, the
ex-tent to which social support predicts medication compliance has not been identified. The finding of this study, that social support was the most powerful predictor of influences on medication compliance in chronic schizophrenic patients, is new. Thus, strengthen social support is suggested, for which various strategies need to be developed that involve families, friends and health care pro-fessionals.
Perceived benefits come from the therapeutic effects of the antipsychotic agents, improvement in the symptoms, and relapse and rehospitaliza-tion prevenrehospitaliza-tion, and are determining factors of health behaviors. They can also be heightened by medication education, and complying patients have higher perceived benefits than noncompliant patients.30From the findings in this study, it was clear that the perceived benefits are the second strongest variables for predicting medication com-pliance. Thus, it is also suggested that the medi-cation's positive rather than negative effects, such as side effects, have to be reinforced.
Unlike other diseases, schizophrenic patients do not take their medication, as they lose their insight into illness and treatment. It was reported that the degree of insight was consistently related to the degree of medication compliance,31 so is
suggested a variable that should be included in further study.
Also, severe psychotic symptoms lead to
in-creases in medication dose and frequency, which impede medication compliance.32 Thus, symptom
severity was an important factor that could de-crease medication compliance in schizophrenia. However, this variable did not significantly pre-dict medication compliance in this study. The mean BPRS score in this study was 27.45, which was very low in comparison to the original median BPRS score of 72.0, suggesting the symp-toms were not that severe in most of the par-ticipants. The reason the BPRS was low was due to all the study participants residing in the com-munity, not a hospital, so their symptoms were manageable and less severe. Thus, a very low BPRS did not have a significant effect on medica-tion compliance in this study.
Substance use has been identified in prior studies as a major factor leading to medication noncompliance and most patients in psychiatric hospitals have a substance abuse history.33,34 With
alcohol abuse, 62% of patients discontinued their medication, which increased the medication non-compliance eight fold.35 The study participants'
amount of substance use was very low, so did not significantly affect medication compliance in this study. A small number of participants drank al-cohol at a social drinking level. Cigarette smoking was not that significant either. Because most patients were involved in treatment settings, such as community mental health centers, outpatient clinics and public health centers, they knew it was harmful to use substances while on medication therapy.
Perceived barriers, such as health care cost, fear, side effects and accessibility,36 need to be
over-come before beginning healthy behavior. Per-ceived barriers lead patients to believe that their medication is not helpful and has no benefits.37
enough to decrease medication compliance. In this study, medication knowledge, social support and perceived benefits predicted both direct and indirect medication compliance. Thus, to strengthen medication compliance of chronic schizophrenic patients residing in the community, continuous education needs to be enhanced to increase medication knowledge and social support from families, health care persons, and friends.
The significance of this study lies in the devel-opment of a basis for theory for schizophrenic patients' medication compliance. However, our results are limited, and do not apply to hospita-lized schizophrenics or those not involved in a treatment setting. Also, those patients that stay at home, without the involvement of a treatment setting, were not included in the study sample. Thus, the model developed in the study can only be applied to schizophrenic patients involved in a treatment setting. It is suggested that these patients should be included in a future study and a model developed that can be applied to all schizophrenic patients, irrespective of their envir-onment. Developing various programs to enhance patients' medication compliance, and many inter-vention programs to heighten social support, have been suggested.
REFERENCES
1. Ruscher SM, Wit R, Mazmanian D. Psychiatric patients' attitudes about medication and factors affecting non-compliance. Psychiatr Serv 1997;48:82-5.
2. Kissling W. Ideal and reality of neuroleptic relapse pre-vention. Br J Psychiatry 1992;161:133-9.
3. Bond WS, Hussar DA. Detection methods and strate-gies for improving medication compliance. Am J Hosp Pharm 1991;48:1978-88.
4. Oh HJ. The burden and professional help for the family of the mental illness. J Korean Acad Nurs 2000;30:202-12.
5. Harvey NS, Peet M. Lithium maintenance: Effects of personality and attitude on health information acqui-sition and compliance. Br J Psychiatr 1991;158:200-4. 6. Drain J, Solomon P. Explaining attitudes toward
medi-cation compliance among a seriously mentally ill popu-lation. J Nerv Ment Dis 1994;182:50-4.
7. Schwartz RC, Skaggs JL, Peterson S. Critique of recent empirical research on insight and symptomology in schizophrenia. Psychol Rep 2000;86:471-4.
8. Gao X, Nau DP, Rosenbluth VS, Woodward C. The
relationship of disease severity, health beliefs and medication adherence among HIV patients. AIDS Care 2000;12:387-98.
9. Scott CS, Lore C, Owen RG. Increasing medication compliance and peer support among psychiatrically diagnosed students. J Sch Health 1992;62:478-80. 10. Buchanan A. A two-year prospective study of
treat-ment compliance in patients with schizophrenia. Psychol Med 1992;22:787-97.
11. Razali MS, Yahya H. Compliance with treatment in schizophrenia: A drug intervention program in a devel-oping program. Acta Psychiatr Scand 1995;91:331-5. 12. Shon KH. A comparative study on relationship of
social support, life events, and depression between psychiatric patients and normal subjects. Nurs Science 1997;9:59-86.
13. Adams J, Scott J. Predicting medication adherence in severe mental disorders. Acta Psychiatr Scand 2000; 101:119-24.
14. Budd RJ, Hughes I, Smith JA. Health beliefs and com-pliance with antipsychotic medication. Br J Clin Psychol 1996;35:393-7.
15. Janz NK, Becker MH. The Health belief model: A decade later. Health Educ Q 1984;11:1-47.
16. Fenton WS, Blyler CR, Heinssen RK. Determinants of medication compliance in schizophrenia: Empirical and clinical findings. Schizophr Bull 1997;23:637-51. 17. Richardson MA, Simons-Morton B, Annegers JF. Effect
of perceived barriers on compliance with antihyperten-sive medication. Health Edu Q 1993;20:489-503. 18. Reiger DA, Farmer ME, Rae DS. Comorbidity of mental
disorders with alcohol and other drug abuse. J Am Med Association 1990;264:2511-8.
19. Lee CS, Han ES, Hwang TY. Public mental health and community: psychosocial rehabilitation program for mentally ill. Kyoungido: Yongin psychiatric hospital 1996.
20. Becker MH. The health belief model and personal health behavior. Health Educ Mono 1974;2:324-473. 21. Harber J, Krainovich-Miller B, McMahon LA,
Price-Hoskins P. Comprehensive Psychiatric Nursing 5th ed. St. Louis: Mosby; 1996.
22. Overall JE, Gorham DR. The brief psychiatric rating scale. Psychol Rep 1962;10:799-812.
23. Sarason IG. The social support questionnaire. In Measuring health: A guide to rating scales and ques-tionnaires. New York: Oxford Univ. Press; 1983. p.867-9. 24. Moon JS. A study of instrument development for health belief of Korean adults[dissertation]. Seoul: Yonsei Univ.: 1990.
25. Korean Ministry of Culture and Athlete. Current status of adolescent drug misuse and prevention strategies. Ministry of culture and athlete press 1996.
26. Cho SB. LISREL structural equation model. Seoul: Young-Ji Press; 1996.
Univ.: 1998.
28. Collins-Colon T. Do it yourself: Medication manage-ment for community based clients. J Psychosoc Nurs 1990;28:25-9.
29. Ku MO, Lee EO. Health belief model and Korean chronic patients' sick role. J Korean Academy 1990;29: 49-63.
30. Shon KH, Park SS. Medication and symptom manage-ment education program for the rehabilitation of psychiatric patients in Korea: the effects of promoting schedule on self-efficacy theory. Yonsei Med J 2002;43: 579-89.
31. Kim BY, Lee CW, Park CW. The relationship among insight, psychopathology and drug compliance in the schizophrenic patient. J Korean Neuropsychiatric Asso-ciation 1993;32:373-80,
32. Perkins DO. Adherence to antipsychotic medications. J Clin Psychiatry 1999;60:25-30.
33. Owen RR, Fischer EP, Booth BM, Cuffel BJ. Medication noncompliance and substance abuse among patients with schizophrenia. Psychiatr Serv 1996;47:853-8. 34. Olfson M, Mechanic D, Hansell S, Boyer AC, Walkup
J, Weiden PJ. Predicting medication noncompliance after hospital discharge among patients with schizo-phrenia. Psychiatr Serv 2000;51:216-22.
35. Pristach CA, Smith CM. Medication compliance and substance abuse among schizophrenia patients. Hosp Community Psychiatry 1990;41:1345-8.
36. Rosenstock IM, Strecher VJ, Becker MH. Social learning theory and the health belief model. Health Educ Q 1988;15:175-83.