Total
Hip
Replacement
FRANK E. STINCHFIELD,* M.D., ERIc S. WmTE,** M.D.
From the New York Orthopaedic Hospital, Columbia-Presbyterian Medical Center,
New York City
OURclinical experience with total hip re-placement is based upon the work of
Charnley.2'
6 In 1958, he departed from the anatomic approach to arthroplasty of the hip and designed a mechanical hip joint based uponbiomechanical and engineering principles.The essential features ofthe low friction arthroplasty are: (1) A metal-to-plastic rather than metal-to-metal joint surface is used with a small diameter femoral head. The surface friction between metal and plastic is considerably less than metal-to-metal and the small diameterhead reduces the contact area between the articulating surfaces.3 (2) Atthe time of operation, the acetabulum is deepened in order to medi-allydisplace the center of rotation and the weight-bearing axis. This reduces the moment of force onthe
prosthetic
compon-ents. In addition, the hip abductor muscles are transplanted laterally and distally toallow them to work at a more effective lever arm. (3) A self-curing cement,
methylmethacrylate,
is used to bond both the acetabular and femoral components toendosteal bone.
Methymethacrylate
has noadhesive properties, but acts as a filler or
mechanical bond which allows a more
uni--'orm distribution of stress over a
large
surface area. These three features are de-signed to minimize wear and to prevent loosening of the
prosthesis (Fig.
1).
*161 Fort Washington Avenue, New York,
NewYork 10032.
**622 West 168th Street, New York, New
York 10032.
Presentedat theAnnualMeeting of the
Ameri-canSurgicalAssociation, March 24-26, 1971, Boca Raton, Florida.
Methylmethacrylate
The unanswered question about the use of cement, which has led to conservatism in the United
States,
is thelong-term tissue tolerance of this material in the human body.Charnley's
monograph, Acrylic Ce-ment inOrthopaedicSurgery, discussesthis question indepth.4
Laboratory investigation has shown that the initial host response to methylmethacrylate in bone is a narrow margin ofcell
death, presumably causedby
the heat of polymerization followed by a fibroblasticresponse with interspersedgiantcells.
After the passage of time, normal re-modeling and bone marrow function take place adjacentto cementseparated only by a thin layer of fibroustissue."'5'
21 At The New York Orthopaedic Hospital, we have done in vivo studies utilizing the canine femur to try and separate the various fac-tors which elicit the histological changes towardmethylmethacrylate.13
Under condi-tions of a minimum shearing-load, histo-logic sections 6 months after implant show normal bone function directly adjacent, to cementwithno residual fibrous lining. Fur-ther studies are being performed to study the relationship between increased shear-ing-loads, i.e., motion, and the amount of fibrous tissue lining between bone and cement.Operative Technic
A shortdescription of the operative tech-nic would seem indicated. A lateral ap-proach to the hip joint is used. Osteotomy of the greater trochanter is recommended to minimize muscle dissection to allow easier dislocation andto facilitate adequate acetabular exposure. This also permits
656
STINCHFIELD AND WHITEFIG. 1. Low Friction Arthroplasty of Charnley.
Barium sulfate is added to the cement to make it
radiopaque. A wire outlines the outer surface of
the plastic socket. Fixation holes are drilled into the acetabulum to produce maximum stability at
the cement-bone interface.
eral and distal displacement of the abduc-tor muscle.
Astraight8to 10inch incision is centered
over or just posterior to the greater tro-chanter and extends along the femoral shaft towards the iliac crest. The fascia lata is incised and the tensor fascia femoris muscle is retracted anteriorly. The junction between the origin of the vastus lateralis and the insertion of the gluteus minimus
and medius is identified. The fatty tissue
and investing fibers of the vastus lateralis are then reflected from the joint capsule. The anterior capsuleis incisedin the
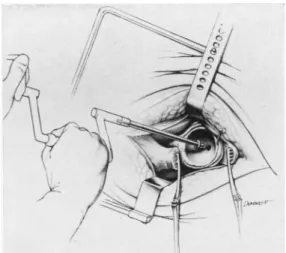
direc-tion ofthe femoral neck and a largs chole-cystectomy clamp is introduced intracapsu-larly, superior to the femoral neck and just medial to the greater trochanter (Fig.
2).
This allows placement ofaGiglisawwhichis used to osteotomized the greater
tro-Ann. Surg. * Oct. 1971 Vol. 174 No. 4
chanter. A limited capsular excision is usually necessary to allow anterior disloca-tion of the femoral head which is accomp-lished by flexion, adduction, and external rotation of the patient's leg. The Gigli saw
is used again to resect the femoral head at
the mid-neck level. Self-retaining retractors
are used to expose the acetabulum which is deepened and widened with special reamers (Fig. 3). The high density poly-ethylene acetabular socket is cemented in
the deepened acetabulum at a 45-degree angle from the horizontal and in neutral rotation. After the cement holding the
ace-tabular component has hardened, attention
is directed toward the femoral shaft. The medullary canal is then reamed for recep-tion of the metal prosthesis. A trial pros-thesis is introduced into the prepared shaft. The hip joint is relocated and a range of
motion is carried out. Anyosteophytes that impinge upon the prosthesis or restrict hip
motion are removed. After placing hori-zontal and vertical trochanteric fixation wires, the permanentprosthesisiscemented
inplace. The hip isrelocated asecond time
and the greater trochanter is secured in its
newposition withthetwo#18 gaugewires.
FIG. A cholecystectomy clamp is used to route the Gigli saw intracapsularly, medial to the hip abductors prior to osteotomy of the greater
TOTAL HIP REPLACEMENT Patient Selection
Newness of the operative technic and the use of methylmethacrylate cement prompted us to restrict our indications for
total hipreplacement.9 Sixty years of age is
the approximate lower limit for patients
withunilateral hip disease. A slightly lower
age limit is allowed forthose patients with
bilateral hip disease since disability is so
much greater when both hips are involved.
Many of the candidates for low friction arthroplasty have had previous attempts
at conventional arthroplasty which have
failed. The ideal candidate for the
proce-dure is one in whom the only alternative
is a Girdlestone resection. In all of the
above situations pain is the primary
indi-cation for surgical treatment while limited
range of motion and gait disturbance are
only secondary considerations.
An absolute contraindication to the
pro-cedure is a history of infection in the
ipsi-lateral hip joint. Patients who have had
multiple hip surgery in the past must
un-dergo careful tests to rule out late, low-grade infection. The surgeon must be
pre-pared to abandon the procedure if during
the operation a positive bacterial smear is
obtained from the operative wound, or if
suspiciousgranulationtissue ispresent.
Rel-ative contraindi@ations are patients having
littledisabilityorwho arestill able towork
when their pain is relieved by analgesics.
Table 1 lists the frequency ofvarious hip
disorders referred to our institution which
warranted total hip replacement.
Hip Assessment
A prospective study has been established
on all patients for low friction arthroplasty
(LFA) at The New York Orthopaedic Hospital. The 6-6-6 numerical grading
system of D'Aubigne and Postel has been
adopted to measure the degree of pain,
function, and mobility in each hip.8 Grade
1 denotes the most severe condition while
Grade 6 indicates the normal. Each
pa-tient is then placed in one of three groups
657
FIG. 3. The acetabulum is exposed laterally.
After deepening it with reamers, fixation holes are
drilled in the acetabulum to increase the contract
area ofcement and bone.
accordingtothetypeof involvement.Group
A indicates unilateral hip disease; Group
B bilateral hip disease and Group C
in-cludes patients with either unilateral or
bilateral hip disease who have some
addi-tional medical or orthopaedic condition
which restricts function. Results of Surgery
Thefirstone hundredlow friction
arthro-plasties were performed at The New York
Orthopaedic Hospital between April 1969 and May 1970. This study group consisted of 93 patients, sevenof whom hadbilateral
arthroplasties. Two died from unrelated causes before their follow-up visit.
Eighty-four patients actually returned for
exami-nation. The shortest interval between
sur-gery and the time of hip assessment was
six months and the longest period was
eighteen months. The average follow-up time was ten months. The actual time
elapsed between surgery and the reading
of this paper ranged from ten to
twenty-three months. This additional follow-up
time is important when considering the incidence ofposssible late wound infection. Pain. Every patientinterviewed had sig-nificant and many times dramatic relief of
pain. Table 2 shows that all but seven
pa-tientswere graded5 and6, postoperatively.
Ann. Surg. Oct. 1971 Vol. 174 * No. 4
STINCHFIELD AND WHITE
Mobility. Table 3. The majority of
pa-tients had a striking increase in range of motion. Afewpatients havinghadmultiple procedures and who formed heterotopic bone, did not have any increase in range
ofmotion. No one, however, had less than
his preoperative range of motion.
Function.Table 4. Our analysis of
func-tion has been divided into the three
pre-viously mentioned categories, A, B, and C. It should be emphasized that function
re-lates to gait pattern and overall activity.
The patients inGroup Adiduniformly well. ThoseinGroup B didnotfarequiteaswell.
Our interpretation of this finding is that
Ann. Surg. * Oct. 1971 Vol. 174 * No. 4
FIG. 4A. J. B., is a
56-year-old man with
osteoarthritis secondary
tocongenitallysubluxated
hips. Five years ago he
underwent bilateral osteo-tomies but didnotobtain permanent relief from pain. At the time of evaluation for LFA, he had Grade 3painandwas unable to work.
FIG. 4B. The failed osteotomies were
con-verted to low friction
arthroplasties. At one-yearfollowup, hehas
re-turned to work as a traveling salesman and walks with no pain and noaids.
many of the Group B patients are limited
by arthritic involvement of their opposite hip. When those patients with
sympto-matic disease in the opposite hip come to
surgery, the results in Group B should
ap-proach that of Group A. Improvement in
Group C after surgery was quite variable.
We believe that this reflects the degree of
limitations imposed bysystemic medical or
orthopaedic conditions rather than hip function, per se.
Complications
Tables 5 and 6. The data on our
com-plications have been updated to include
-ourfirst200 procedures. Althoughthe most
TOTAL HIP REPLACEMENT
frequent postoperative complication was
urinary retention requiring a Foley
cathe-ter, two more important problems warrant discussion.
Thromboembolism. Because ofthe
dan-ger of deep wound hematoma and the risk
of subsequent wound infection,7 we have
been selectively rather than routinely,
anti-coagulating our patients with coumadin.
After analyzing the results of our first 100
procedures, the incidence of thromboembo-lic complications was alarmingly high, 15
per cent. This prompted us to take very
stringent measures duringthepostoperative
periodtopreventthrombophlebitis. In
addi-tion, we have instituted a controlled study to evaluate the use of Dextran-40 as a
prophylactic anticoagulant. Although re-cent reports in the surgical literature have appeared favoring the use of Dextran," 10
our preliminary results based upon 60
treated and60 controlledpatients showjust
as manypulmonary emboli and episodes of
thrombophlebitis in the treated groups as
the control group.14 Further studies are nowbeing carried out inrespect to the use
of Dextran 70.
Infection. The most important and
dan-gerous complication of LFA is postopera-tive deepwound infection. Fortunately, we
have had little experience in this regard. Although we have had three superficial
wound hematomas whichdrained and grew
out an organism, there have been no early
and no late deep wound infections.
Charmley's wound infection rate in a large
series of patients was unacceptable priorto the institution of stringent measures to
pre-vent intraoperative contamination. These
included the use ofsterile laminar air flow system and the complete isolation of the
surgeons'florafrom the operative field.5We
currently do not have a laminar air flow
operatingroom for implant surgery.
Never-theless,everyeffort ismadeto carryoutthe strictestaseptic technic inordertoeliminate
any potential source of intraoperative
wound inoculation.
Another factor to be considered in the
659
TABLE 1.Diagnostic Categories Primaryosteoarthritis 120
Failed previous surgery 36 Secondaryosteoarthritis 16 Rheumatoidarthritis 15 Avascularnecrosispostfracture 7
Mixed arthritis 6
TABLE 2. Pre-andPostoperative Pain (90Hips)
Grade 1 2 3 4 5 6
Preop. - 20 49 18 3
Postop. - - 1 6 21 62
TABLE3.Pre-andPostoperativeMobility (90Hips)
Grade 1 2 3 4 5 6
Preop. 12 22 33 19 3 1
Postop. - - 3 18 37 32
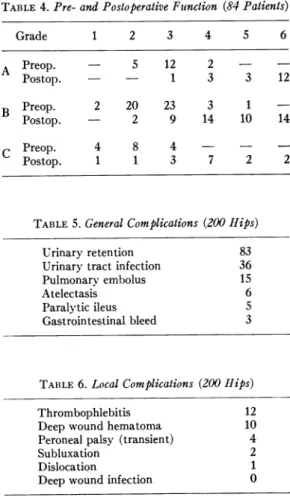
TABLE 4.Pre-andPostoperativeFunction (84Patients)
Grade 1 2 3 4 5 6 A Preop. - 5 12 2 Postop. - - 1 3 3 12 B Preop. 2 20 23 3 1 Postop. - 2 9 14 10 14 C Preop. 4 8 4 - -Postop. 1 1 3 7 2 2
TABLE5.GeneralComplications (200 Hips)
Urinaryretention 83 Urinarytractinfection 36 Pulmonary embolus 15
Atelectasis 6
Paralytic ileus 5
Gastrointestinal bleed 3
TABLE 6.LocalComplications (200flips)
Thrombophlebitis 12
Deepwound hematoma 10
Peroneal palsy (transient) 4
Subluxation 2
Dislocation 1
Deepwound infection 0
Ann. Surg. * Oct. 1971 Vol. 174 No. 4
STINCHFIELD AND WHITE Ann. 8urg. * Oct. 1971
Vol. 174 No. 4
FIG. 5A. L. J.,is a70
year-old woman with a
congenital dislocation of
her left hip. In recent
years, her hip had be-come painful and limited her activity.
prevention of wound infection is the use
ofprophylactic antibiotics. Our department
published a paperinJanuary 1970
advocat-ing the use of prophylactic antibiotics in
major hip and backsurgery." This was
re-commended on the basis of a controlled
comparison of postoperative wound
infec-tions utilizing Penicillin-G as the
prophy-lactic antibiotic choice. Whenever
select-ing a prophylactic antibiotic, one must be
familiar with his own hospital's infecting
organisms and their sensitivities. All of the
patients undergoing LFA received
Peni-cillin-G or an alternate antibiotic before,
during, and after operation.
Technical Complications. Technical complications of LFA also can lead to a
poorresult. Most patients undergoing LFA
as their initial surgical treatment for pri-mary osteoarthritis present no difficulty for thoseproperly trained inthe technic.
How-ever, revisionsurgeryforapreviouslyfailed
arthroplasty is considerably more difficult.
Dislocation of the hip joint, resection of heterotopic bone, preparation of the
aceta-bulum andaligmentof theprosthesis areall
technical barriers with whichonemust
con-tend. The followingtwo examples illustrate difficulties imposed by a deficient
aceta-bulum. The first patient (Fig. 4) represents
failed bilateral osteotomies which
pre-viously had been performed for
congeni-tally subluxated hips. Although hardware
removal, dislocation, and acetabular
pre-paration were difficult, a good end result was achieved. The secondexample (Fig. 5)
is that of an elderly lady with a congenital
Fic. 5B. An LFA was performed but the acet-abular component was not well seated because of
an inadequate bony roof.
Ann. Surg. Oct. 1971 TOTAL HIP REPLACEMENT 661
Vol. 174 No. 4
r_r
FiG,. 5G. Two months after operation, fixation of the acetabular socket waslostand theprosthesis
dislocated.
dislocation. No acetabulum is present. At-tempts to create an acetabulum failed
be-cause of lack of
bony
support over the acetabular socket. Two months afteropera-tion and after a limited amount of
weight-bearing,
thisprosthesis
loosened and dis-located. The entireprosthesis, including
cement, had to be removed. Thepatient
was in no way
helped by
heroriginal
operation.
Summary
The
early
results of our low frictionarthroplasty
series are very encouraging. We believe that totalhip
replacement
is here tostay,
but we know that thisproce-dure carries with it the potential of many
and
major complications.
Inherent in this method of low frictionarthroplasty
is thepossibility
ofcatastrophic
results unless theprinciples
laid down arecarefully
followed. We believe thatthoughtful
selection ofpa-tients and strict attention to
operative
FIG. 5D. The entire prosthesis had to be
re-moved leaving the patient with her preoperative
deformity, after two major surgical procedures.
asepsis are the two most important factors in this procedure.
Acknowledgment
The authors wish to acknowledge the con-tribution of Nasseroddin S. Eftekhar, M. D. and
Kenneth M. Kurokawa, M. D., in the initiation and continuation of this prospective study.
References
1. Atik, M., Harkness, J. W. and Wichman, H.
W.: Prevention Fatal Pulmonary Embolism. Surg. Gynec. Obstet., 130:403, 1970. 2. Charnley, J.: Arthroplasty of the Hip. A New
Operation. Lancet. 1:1129, 1961.
3. Charnley, J., Kamangar, A. and Longfield,
M. D.: The Optimum Size of Prosthetic
Heads in Relation to the Wear of Plastic Sockets in Total Replacement of the Hip. Med. Biol. Engin., 7:31, 1969.
4. Charnley, J.: Acrylic Cement in Orthopaedic
Surgery. Balitmore, Maryland, Williams and
Wllins Co., 1970.
5. Charnley, J.andEftekhar, N.S.: Postoperative Infection in Total Prosthetic Replacement Arthroplasty of the Hip Joint. Brit. J. Surg., 56:641, 1969.
6. Charnley, J.: Total Hip Replacement by Low Friction Arthroplasty. Clin. Orthop., 72:7, 1970.
STINCHFIELD AND WHITE Ann. Surg. Oct. 1971
662
Vol. 174 No. 47. Crawford, W. J., Hillman, F. and Charnley, J.: A Clinical Trial of Prophylactic
Anticoagu-lant Therapy in Elective Hip Surgery, Cen-ter for Hip Surgery, Wrightington. Hospital
Internal Publication, No. 14, May 1968.
8. D'Aubigne, R. M. and Postel, M.: Functional Results of Hip Arthroplasty with Acrylic Prosthesis. J. Bone Joint Surg., 36A:451, 1954.
9. Eftekhar, N. S.: Low Friction Arthroplasty: Indications, Contraindications, and
Com-plications. Presented at The Section on
Orthopaedic Surgery, 119 Annual Meeting, American Medical Association, Chicago,
Illinois, June1970.
10. Evarts, C. M. and Feil, E. I.:
Thrombo-embolism after Elective Surgery of the Hip. Orthop. Clin. N. Amer.,2:167, 1971.
11. Fogelberg, E. V., Zitzmann, E. K. and
Stinchfield, F. E.: Prophylactic Penicillin in
Orthopaedic Surgery. J. Bone Joint Surg., 52A:95, 1970.
12. Henrichsen,E., Jansen, K.andKrough-Poulson,
W.: Experimental Investigationof the Tissue Reaction to Acrylic Plastics. Acta Orthop. Scand., 22:141, 1952.
13. Kurokawa, K. M. and Pawluk, R.: Response
of Canine Bone to Self-Curing Methyl-methacrylate. In preparation.
14. Rothermel, J. E.: Personal communication. 15. Wiltse, L. L., Hall, R. H. and Stenejem, J. C.:
Experimental Studies Regarding the Possible
Use of Self-Curing Cement in Orthopaedic Surgery. J. Bone Joint Surg., 39A:961, 1957.
DIscusSION PRESIDENT-ELECr MooRE:
I would like to ask Dr. Stinchfield acouple of questions.
What about Paget's disease? Is that a con-traindication? How do you choose this, versus a cupor aprosthesis, or do you pretty much just go overthis?
Finally, our group, has been concerned over this late sepsis, and we wonder if the plastic sets up a reaction intheacetabulum which favors later
localization of organisms from the bloodstream. In
other words, could it be blood-borne to the site, rather than true, surgical infection?
DR. KENNETH W. WARREN (Boston).Charnley gives considerable credit to the "greenhouse" in
reducing the incidence of infection in total hip
replacement. Do you feel that the "greenhouse" or someformoflaminar airflow is asignificantfactor
in controlling infection in this procedure? Do you use local antibiotic spray or irrigation during the
operation?
DR. EDWIN W. SALZMAN (Boston): We have recently completed a study of 169 patients with
Vitallium mold arthroplasty, in whom we
com-pared the efficacy of agents affecting platelet
function with warfarin for the prophylaxis of
venous thromboembolism. In that study dextran
and aspirin were each as effective as warfarin,
which was significantly more effective than the
control.
Ina companion study of totalhip arthroplasty
whichisstillinprogress, theincidence of thrombo-embolism appears higher than following the cups;
perhaps Dr. Stinchfield would comment on this difference.
The preliminary results of this second study appear to show that dextran is not as effective as
warfarin in these high risk patients.
DR. FRANK E. STINCHFDELD (Closing): We have operated upon five patients with Paget's
Disease. However, this type of patient is not the ideal one on whom to operate-if one expects to obtainanexcellentresult. Paget's, per se,produces
painandonecannoteliminate thediseasebydoing
a total hip replacement. In the five patients
operatedupon, two results were disappointing and three patients said they received relief from pain -butstill had their Paget's pain.
The question was asked-"When do you use
cups?"Iwant to saythat I still consider the mold
operation to be an excellent one and continue to
use itonpatients inthe younger age group-those
between the ages of 20 to 55 years. Also, we use
the cup arthroplasty in those patients where there has been previous infection. One should never attempt a total hip replacement where there has been priorinfection.
Late sepsis is something thatIcannotcomment
onbecause we have been doing this procedure for but the past2 years. We may experience this
com-plication in another 1 to 3 years but to date we havehadnone. Ithink that when infection occurs it probably is introduced at the time of operation
andisnot bloodborne. Actually, there is
consider-able evidence to prove that methylmethacrylate
does not really give very much soft tissue reaction. The question by Dr. Warren relative to the 'greenhouse,' the laminar air flow, and the space suit, is very appropriate- as all of these
contrib-ute todiscipline. There is no doubt ofthat. How-ever, inour series, we have not foundthe
'green-house' tobeessential.
Relative to the use of antibiotics we have re-ported our findings in a previous study. In that
study we reported on 236 patients who had had
mold arthroplasties. The infection rate was
re-duced from 5.4 to 1.2 by the use of appropriate prophylactic antibiotics.
Regarding the use of anticoagulants, I agree that anticoagulation is helpful. We anticoagulate
all of our patients who have had a mold
arthro-plasty, in an effort to prevent thrombophlebitis.
However, inthe totalhip replacement patient, we fearhematomamorethanthromboembolism.
Anti-coagulation may cause bleeding and hematoma more thanthromboembolism. Anticoagulationmay cause bleeding and hematoma-which could lead to infection. Therefore, we do not routinely anti-coagulatethe totalhippatient.