DEVOLUTION AND NURSING
WORKFORCE POLICY AND PLANNING IN
THE FOUR COUNTRIES OF THE UNITED
KINGDOM 1997-2009
PAULINE MILNE
A thesis submitted in partial fulfilment of the
requirements for the degree of Doctor of
Philosophy
QUEEN MARGARET UNIVERSITY
Abstract
This thesis examines how political devolution in the UK impacted upon nursing workforce policy and planning by investigating the following research questions:
What has been the impact of devolution on nursing workforce policy and planning across the four countries of the UK (1997-2009)?
How and why have the approaches to nursing workforce policy and planning changed across the four countries of the UK (1997-2009)?
The research methodology used was a mixed methods approach which included semi-structured interviews with 30 stakeholders from the fields of nursing, healthcare policy or workforce planning across the UK. A purposive sampling strategy was adopted and the distribution of interviewees was England (11), Scotland (7), Wales (6) and Northern Ireland (6).
A realist review approach to inquiry was taken which involved establishing what works for who, in what circumstances and why? The qualitative data from the interviews was supplemented by analysis of quantitative data on nursing workforce trends and information from the analysis of health policies from the four countries.
The key findings include: changing patterns of power and influence in the devolved administrations; continued cycles of ‘boom and bust’ in nursing workforce supply; variable growth in the nursing workforce across the UK; the unwillingness of England to ‘let go’ and the perception by interviewees that some national nursing policies were unimportant.
The conclusions were that although devolution enabled greater freedoms in terms of policy and workforce flexibility, just under half of the interviewees reported that devolution had a positive impact upon nursing. There was reluctance from senior nursing leaders to share and learn from good practice across countries and despite the rhetoric from numerous reports around the need to improve nursing workforce planning, there was little evidence of lessons being learned which would have improved the effectiveness of planning the future nursing workforce.
Key Words:
nursing workforce planning; nursing workforce policy; United Kingdom devolution; realist review.
Acknowledgements
I am indebted to the following people:
My supervisors Professor James Buchan, School of Health Sciences, Queen Margaret University and Professor Alan Gilloran, Vice Principal (Academic), Queen Margaret University for their on-going support, direction, constructive feedback and critical challenge throughout this research study.
My friend and colleague Professor Mike Cook whose inspiration helped me remain focused and motivated particularly in trying to balance the demands of full-time employment whilst undertaking this research.
The 30 experts who consented to be involved in this study and who generously gave up their time to participate in the interviews. I wish to thank them for their willingness to actively engage with the research, their openness and honesty without which this research would not have been possible.
My husband David for his enduring patience, encouragement and support.
I also wish to acknowledge the generous funding I received during the course of my PhD studies from the following sources:
Scottish Executive Health Department
Melvill Sheppherd Fund for Trained Nurses (Mid Essex)
NHS East of England and the East of England Multi-Professional Deanery
The Florence Nightingale Foundation, the Sandra Charitable Trust and the Department of Health (England) who funded a Travel Scholarship to Ontario, Canada in 2009 to review Nursing Workforce Planning leading to the completion of a report ‘Improving Nursing Workforce Planning – What are the Lessons from Canada for the United Kingdom?’
Table of Contents
Abstract
iAcknowledgements
iiList of Tables
xiList of Figures and Charts
xiiAppendices
xiiiChapter One – Setting the Context
11.1 Introduction and Research Questions 1
1.2 Development of a Conceptual Framework 3
1.2.1 Rationale for the Conceptual Framework 3
1.2.2 Developing the Conceptual Framework 4
1.2.3 Implementing the Conceptual Framework 7
1.3 Background to Researcher’s Interest in Nursing Workforce Planning
7
1.4 Summary of Key Points 9
Chapter Two – Health Policy Analysis
102.1 Introduction to the Policy Analysis 10
2.2 Healthcare Policies from 1997 to 1999 15
2.3 Healthcare Policies Post-Devolution 16
2.3.1 Overview 16
2.3.2 England 16
2.3.3 Scotland 18
2.3.4 Wales 21
2.3.5 Northern Ireland 22
2.3.6 Shift in Care to the Community 23
2.4 Summary of Health Policies and the Implications for Nursing
23
2.5 Human Resource and Nursing Strategies 24
2.5.1 Human Resource Strategies 25
2.5.3 Summary on Human Resource and Nursing Strategies 29
2.6 UK Wide Policies with Implications for the NHS Workforce
29
2.7 Summary on Health Policies 31
Chapter Three – Literature Review
323.1 Introduction to Literature Review 32
3.2 Devolution 35
3.2.1 Introduction to Devolution 35
3.2.2 Key Sources of Data and Information 35
3.2.3 Background to Devolution 37
3.2.4 Overview of the Healthcare Structures and Policy Priorities in each of the Four Countries
38
3.2.4.1 England 39
3.2.4.2 Scotland 41
3.2.4.3 Wales 42
3.2.4.4 Northern Ireland 43
3.2.4.5 Summary on the Four Countries 45
3.2.5 Reserved and Devolved Powers 46
3.2.5.1 Overview of Powers 46
3.2.5.2 The Impact of Changes in Government 48
3.2.5.3 Professional Regulation of Nursing 49
3.2.6 Mechanisms of Power and Influence 50
3.2.6.1 Routes of Influence 50
3.2.6.2 Models of Professional Leadership in the Four Countries
53
3.2.7 Policy Divergence across the Four Countries 54
3.2.7.1 Overview of Health Policy Divergence 54
3.2.7.2 Reasons for Divergence 56
3.2.7.3 Implications for Nursing Policy 57
3.2.8 Gaps in the Evidence Base on Devolution 59
3.3 Nursing Workforce Planning 59
3.3.2 Workforce Planning Reports, Policies and Structures in the Four Countries
61
3.3.2.1 England 61
3.3.2.2 Scotland 65
3.3.2.3 Wales 67
3.3.2.4 Northern Ireland 70
3.3.2.5 Summary on Workforce Planning Reports, Policies and Structures
71
3.3.3 Nursing Workforce Planning Initiatives and Tools 72 3.3.4 Summary of Key Themes from Workforce Planning
Literature
74
3.3.5 Gaps in the Nursing Workforce Planning Evidence Base 77
3.4 Nursing Recruitment and Retention 79
3.4.1 Introduction to Nursing Recruitment and Retention 79
3.4.2 Overview of Nursing Shortages 79
3.4.3 Recruitment Initiatives 81
3.4.3.1 Increased Pre-Registration Nursing Commissions 81
3.4.3.2 Widening access to Pre-Registration Programmes 83
3.4.3.3 International Nursing Recruitment 84
3.4.3.4 Nursing Skill Mix 85
3.4.4 Retention Initiatives 87
3.4.4.1 Opportunities for Flexible Working 87
3.4.4.2 Pay and Reward 89
3.4.4.3 Satisfaction with Work Environment 89 3.4.5 Summary of Key Points on Nursing Recruitment and
Retention
90
3.5 Summary of the Literature Review 90
Chapter Four - The Research Approach
934.1 Research Methods 93
4.1.1 Overview of Research Methods 93
4.1.2 Paradigm Worldview 99
4.1.4 Ontology 101
4.1.5 Theoretical Lens 102
4.1.6 Methodological Approach 105
4.1.7 Overview of Data Collection Methods 111
4.1.8 Characteristics of the Researcher 111
4.1.9 Constraints of the Study 114
4.1.10 Summary of Key Points on Research Methods 117
4.2 Implementation of Research Methodology and Data Collection Methods
118
4.2.1 Overview of Research Methodology and Data Collection 118
4.2.2 Initial Planning 118
4.2.3 Ethics Approval 119
4.2.3 Rationale for Choice of Data Collection Method 120
4.2.3.1 Interview 120 4.2.3.2 Questionnaire 123 4.2.3.3 Focus Group 124 4.2.4 The Sample 125 4.2.4.1 Sampling Strategy 125 4.2.4.2 Selection of Sample 126
4.2.4.3 Characteristics of the Sample 128
4.2.5 Development of Interview Schedule 129
4.2.6 Planning the Interviews 130
4.2.6.1 Pilot Interview 130
4.2.6.2 Consent to Participate in Study 131
4.2.6.3 Scheduling of the Interviews 131
4.2.6.4 Conducting the Interviews 133
4.2.7 Transcription and Approval of Interview Data 135
4.2.8 Confidentiality and Anonymity 136
4.2.9 Reflections on the Data Collection Method 138
4.2.10 Summary of Key Points on Implementation of Research Methodology and Data Collection Methods
4.3 Process for Analysing Data 139
4.3.1 Overview of Data Analysis 139
4.3.2 Data Reduction 139
4.3.3 Selection of Data Analysis Method 140
4.3.3.1 FrameWork 140
4.3.3.2 Mind Maps 142
4.3.4 Application of the Data Analysis Method 144
4.3.5 Reflection on the Data Transcription and Analysis Processes
146
4.3.6 Summary of Key Points on Data Analysis 147
4.4 Summary of the Research Approach Chapter 147
Chapter Five - Nursing Workforce Data
1495.1 Introduction 149
5.2 Background Information Regarding Nursing Workforce Data
149
5.3 Overview of the Nursing Workforce Statistics and Trends (NHS data)
152
5.3.1 Rates of Workforce Growth 152
5.3.2 Nursing Skill Mix 157
5.3.3 Levels of Part Time Working 158
5.4 Profile of the Registered Nursing and Midwifery Profession (NMC data)
160
5.4.1 Demographics of the NMC Register 161
5.4.2 Profile of those Joining the NMC Register 162
5.4.3 Joiners, Leavers and Intentions to Leave NMC Register 164
5.5 Limitations of Available Datasets 165
5.6 Summary of Key Points 167
Chapter Six
– Analysis of Interview Data and
Reporting of Findings
169
6.1 Overview of Analysis of Data and Reporting of Findings
6.2 Devolution
170
6.2.1 Setting the Context 170
6.2.2 The Impact of Devolution upon Nursing 171
6.2.3 Divergence as a Consequence of Devolution 174
6.2.3.1 Policy Divergence across the Four Countries 175
6.2.3.2 The Implications of Policy Divergence upon Nursing 178
6.2.3.3 Sharing and Adopting Best Practice 181 6.2.4 Nursing Leadership in Relation to Nursing Workforce
Policy and Planning in the Four Countries
185
6.2.4.1 The Role of Chief Nursing Officers 185
6.2.4.2 Modernising Nursing Careers 186 6.2.5 The Shifting Power Bases of Individuals and
Organisations in the Devolved Administrations
190
6.2.6 Summary of Key Points 195
6.3 Key Health Policies 197
6.3.1 Overview of Key Health Policies 197
6.3.2 Reported Key Health Policies and Policy Drivers 199
6.3.2.1 Shift in Care from the Acute Sector 200
6.3.2.2 Changes to Nursing Roles 201
6.3.2.3 Policy Themes within Countries 202 6.3.3 Policies Which Were Not Identified as Priorities 205
6.3.4 Summary of Key Points 208
6.4 Nursing Workforce Planning 209
6.4.1 Overview of Nursing Workforce Planning 209
6.4.2 Responsibility for Ensuring the Nursing Workforce is Considered When New Health Policies are Developed
210
6.4.3 Workforce Planning Capacity 216
6.4.3.1 Workforce Planning Capacity in England 217
6.4.3.2 Workforce Planning Capacity in Scotland 218
6.4.3.3 Workforce Planning Capacity in Wales 219
6.4.3.5 Summary on Workforce Planning Capacity 222 6.4.4 Centralised versus Decentralised Workforce Planning 223
6.4.5 Integration of Workforce Planning 224
6.4.5.1 Views on Integration of Workforce Planning 225
6.4.5.2 Multi-Professional Workforce Planning 226
6.4.5.3 Summary on Integration 228 6.4.6 Opportunities for Nursing Workforce Planning on a
UK- Wide Basis
228
6.4.7 Summary of the Key Points Related to Nursing Workforce Planning
231
6.5 Nursing Recruitment and Retention 233
6.5.1 Introduction to Recruitment and Retention 233
6.5.2 Nursing Recruitment and Retention Initiatives and Influencing Factors
234
6.5.2.1 Flexible Approaches to Training Nurses 234
6.5.2.2 Increased Funding for Nursing Recruitment and Retention
236
6.5.2.3 International Nursing Recruitment 237
6.5.2.4 Flexible Employment Practices 237
6.5.2.5 Preceptorship 238
6.5.2.6 Pressures of Work 239
6.5.2.7 Additional Factors Impacting Upon Nursing Recruitment and Retention
239
6.5.3 Summary of Key Points on Nursing Recruitment and Retention
240
6.6 Summary 240
Chapter Seven – Key Findings
2427.1 Overview 242
7.2 Context of Findings 242
7.3 Changing Patterns of Power and Influence in Nursing 243 7.3.1 Closer Working Relationships with Politicians and
Government Ministers
7.3.2 The Role, Impact and Sphere of Influence of the Chief Nursing Officers
246
7.4 Chief Nursing Officer Involvement in Ensuring the Nursing Workforce was Considered During Policy Development
247
7.5 Changes in Approaches to Nursing Workforce Planning Following Devolution
248
7.6 Variable Growth in the Nursing Workforce across the UK
251
7.7 Reluctance to Share and Learn from Good Practice across Countries
252
7.8 Unwillingness of England to ‘Let Go’ 253
7.9 Policies Reported to have Impacted Most Upon Nursing
255
7.9.1 Policies Regarded as Important 255
7.9.2 Policies Regarded as Unimportant 256
Chapter Eight – The Researcher’s Reflections
2588.1 The Contexts within Realist Review 258
8.2 Reflection on Dual Role of Practitioner and Researcher 262
8.3 The Limitations of this Study 264
Chapter Nine – Conclusions & Recommendations
2679.1 Conclusions 267 9.2 Recommendations 273 9.2.1 Overview of Recommendations 273 9.2.2 Recommendation One 274 9.2.3 Recommendation Two 277 9.2.4 Recommendation Three 278 9.2.5 Recommendation Four 280
9.2.6 Areas for Further Research 282
References
283List of Tables
Table 2.1 Scotland - Policy / Event Log 11
Table 3.1 Literature Review Inclusion and Exclusion Criteria 33 Table 3.2 Pre-Registration Nursing Commissions in the Four
Countries of the UK at Three Points in Time
82
Table 3.3 Admissions to the NMC Register 84
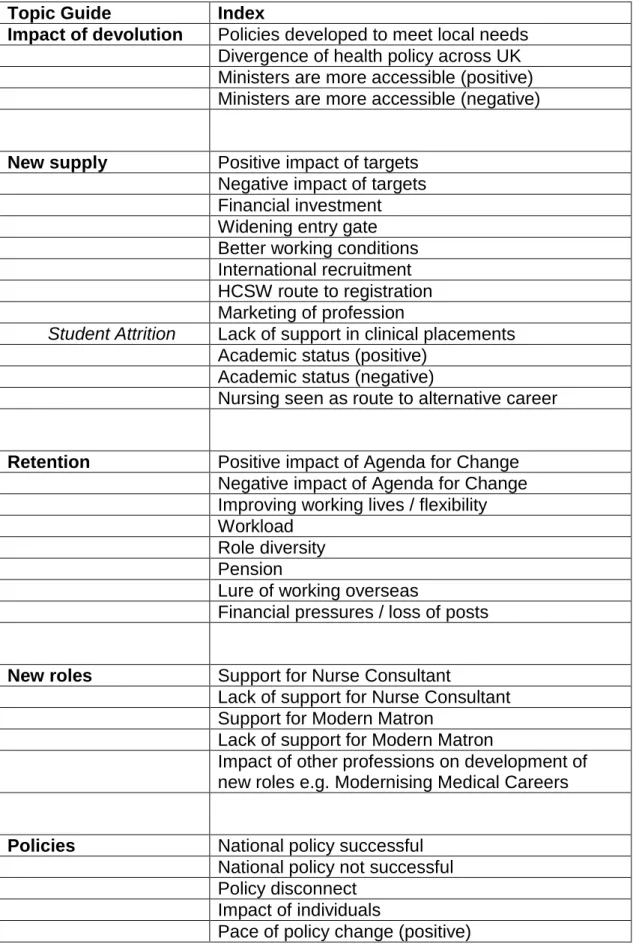
Table 4.1 Thematic Framework 141
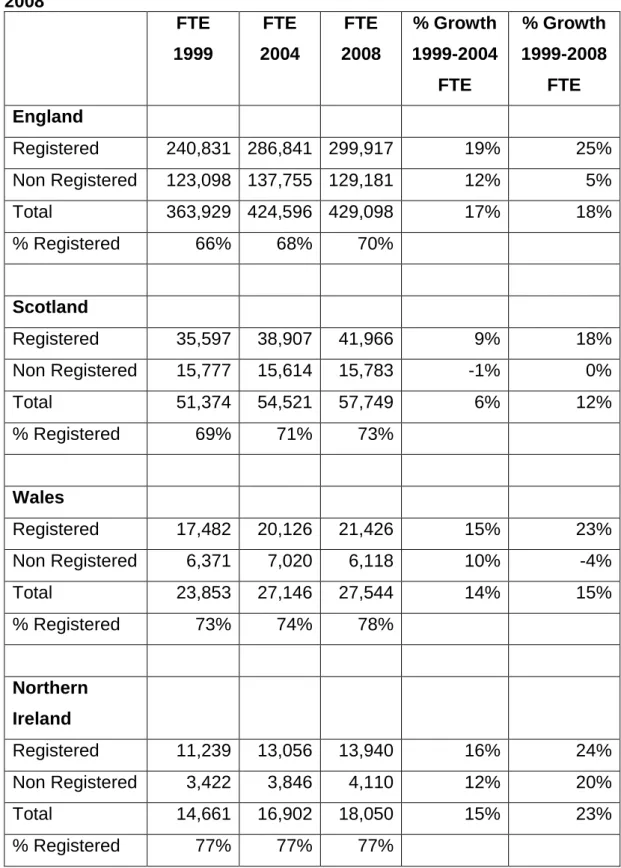
Table 5.1 The Nursing and Midwifery Workforce as at 1999, 2004 and 2008
List of Figures and Charts
Figure 1.1 Final Conceptual Framework (Version Four) 5
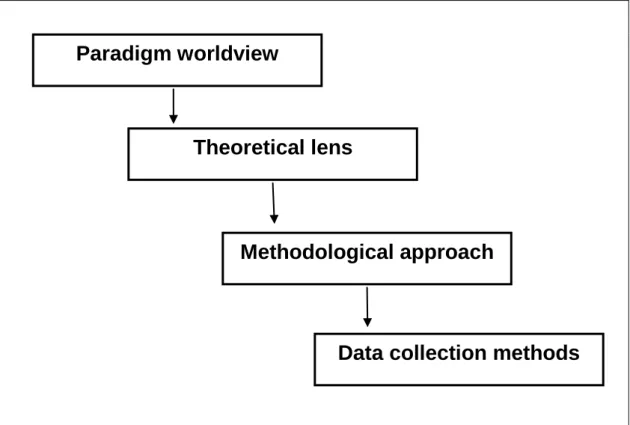
Figure 4.1 The Four Levels of Developing a Research Study 96
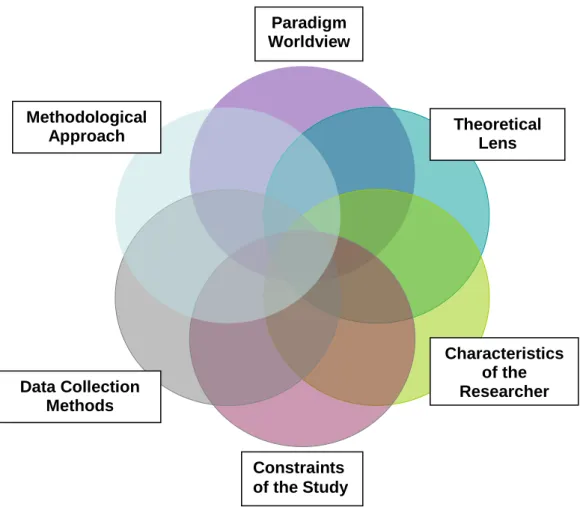
Figure 4.2 Adapted Representation of the Elements of the Research Process and Associated Factors
98
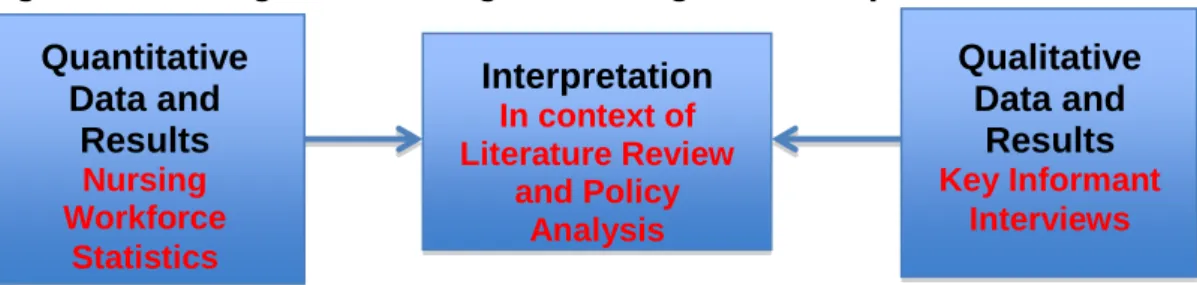
Figure 4.3 Triangulation Design 108
Figure 4.4 Triangulation Design including Data Components 111
Chart 5.1 Percentage Change in Nursing and Midwifery FTE (1999-2008)
154
Chart 5.2 Registered Nurses and Midwives as a Percentage of Total Nurses and Midwives in FTE (1999-2008)
158
Chart 5.3 Trends in FTE/HC Ratio for Total Nursing and Midwifery Workforce
159
Chart 5.4 Trends in FTE/HC Ratio for Registered Nursing and Midwifery Workforce
159
Chart 5.5 Trend in Percentage of Nurses on NMC Register who were Male (1997-2008)
161
Chart 5.6 Percentage of NMC Registrants Aged Under and Over 40 years (1997-2008)
162
Chart 5.7 Initial Entrants to NMC Register by Source 164
Chart 5.8 Initial Entrants, Leavers and Intentions to Leave the NMC Register
Appendices
Conceptual Framework (Version One) I 332
Conceptual Framework (Version Two) II 333
Conceptual Framework (Version Three) III 334
England - Policy / Event Log IV 335
Wales - Policy / Event Log V 339
Northern Ireland - Policy / Event Log VI 342
UK - Policy / Event Log
VII 345
Scanned Copy of Letter from Committee (A) Multi-Centre Research Ethics Committee (MREC) for Scotland
VIII 346
Flyer Providing Overview of Research Study IX 347
Copy of Letter Sent to Potential Participants X 348
Copy of Information Sheet for Potential Participants XI 349
Copy of Consent Form for Participants XII 351
Interview Progress Record XIII 352
Sample Mind Map (Devolution) XIV 355
Summary of Key Policies Over the Period 1997-2008 as Reported by Interviewees
Chapter One – Setting the Context
1.1 Introduction and Research QuestionsDevolution, the decentralisation of power from the Whitehall Government in London to the three devolved administrations in Scotland, Wales and Northern Ireland was established in law by the Labour Government in 1998 and introduced in 1999. Devolution extended to only 15% of the United Kingdom (UK) (Paun and Hazell 2008).
As healthcare is a devolved matter this has resulted in each country of the UK having increased but varying degrees of legislative powers over policy and planning matters related to the National Health Service (NHS). Since devolution each country has developed different policies and approaches to address the health needs of their local populations.
Although programmes of research have been undertaken to investigate the impact of UK devolution on health services (including Hazell and Jervis 1998; Jervis and Plowden 2003; Greer 2003; Greer and Trench 2008, Jervis 2008) there is an absence of research into the impact of devolution specifically upon nursing. The literature published on this is confined to examples of commentary on what devolution means for nursing (including Catton 1999; Bradley 2000; O’Neill 2000; Maslin-Prothero, Masterson and Jones 2008; Fyffe 2008, Moore 2009) but there are no known published research studies specifically on the impact of UK devolution on nursing workforce policy or nursing workforce planning.
The key focus of this thesis is to address this gap in the research and compare approaches to nursing workforce policy and planning across the four UK countries over the period when devolution was being implemented and the subsequent decade (1997-2009), with the intention of establishing a greater insight into the impact of devolution. The main evidence base for this thesis is the data from qualitative interviews conducted in 2008 with 30 key stakeholders from the fields of nursing policy and workforce planning.
This study investigates the following tworesearch questions:
What has been the impact of devolution on nursing workforce policy and planning across the four UK countries 1997-2009?
How and why have the approaches to nursing workforce policy and planning changed across the four UK countries 1997-2009?
At the time of the fieldwork for this study in 2008 there were 622,8511 nurses, midwives and related support staff working in the NHS in the UK, 70% of which were Registered Nurses or Midwives. As nurses are the main deliverers of patient care, robust systems of workforce planning are essential to ensure an adequate supply of the nursing workforce, with the right skills and competencies, to meet future healthcare needs and provide safe and effective patient care. If there are insufficient nurses in the workforce then short term temporary staffing solutions, for example bank and agency staff, may be relied upon and these can be more expensive options with the potential to have an adverse impact upon the quality of patient care.
The study focuses primarily on all four fields2 of nursing (adult, children, mental health and learning disability) but excludes midwifery. The rationale for the exclusion of midwifery is that it is a separate professional group from nursing, governed by a range of distinct health policies and has a specific set of workforce issues. It should be noted that some of the data included in the study is for the nursing and midwifery workforce and this has been used only where it was not been possible to obtain a separate breakdown for the nursing workforce.
1
This figure relates to headcount and was derived from a collation of official government datasets from each of the four UK countries.
2
1.2 Development of a Conceptual Framework
1.2.1 Rationale for the Conceptual Framework
As this research study spans the four countries of the UK (England, Scotland, Wales and Northern Ireland) over the twelve year period from 1997-2009, there was a need to develop an approach to the research that would enable a significant volume of policy information and literature to be reviewed, analysed, synthesised and contextualised.
At the outset of undertaking a research study the researcher will have some ideas about the phenomenon under study but at this stage further thinking will be required to develop the research questions and formulate the underpinning theory (Miles and Huberman 1994). In order to facilitate this process a conceptual framework was developed which provided a systematic approach and subject matter boundaries for the policy analysis and literature review. Teddlie and Tashakkori described the process of developing a conceptual framework as being ‘highly inductive’ (2009, p.89). In this thesis it was used to frame the overall research process including formulating the research questions, the development of the schedules for the key informant interviews as well as providing a structure to ensure a consistent sequencing of information reported through the literature review and the presentation of findings.
The conceptual framework developed for the study was informed by the work of Miles and Huberman (1994, p.18) who described the key purpose of the framework as being a means of explaining ‘the main things to be studied – the key factors, constructs or variables – and the presumed relationships among them’. A conceptual framework has also been described as being a ‘model of what is out there that you plan to study, and of what is going on with these things and why - a tentative theory of the phenomena that you are investigating’ (Maxwell 2005, p.33). The process of developing the conceptual framework for the study provided the researcher with the opportunity to plot out the key themes visually and to explore the potential
linkages between the themes in a more meaningful way than could have been achieved through the use of narrative alone.
1.2.2 Developing the Conceptual Framework
The development of the conceptual framework for the study was an iterative process which evolved as the researcher tested out different ways of ordering and presenting the information until the final version of the framework was achieved. The final version of the conceptual framework, which was used in the study is outlined below and is shown at Figure 1.1. Earlier versions of the conceptual framework are included in Appendices I, II and III for information and to illustrate the process of iteration.
The conceptual framework was informed by the researcher’s professional background and previous work experience, and by the policy analysis, initial review of the literature and the views of experts in the field of nursing workforce policy and planning.
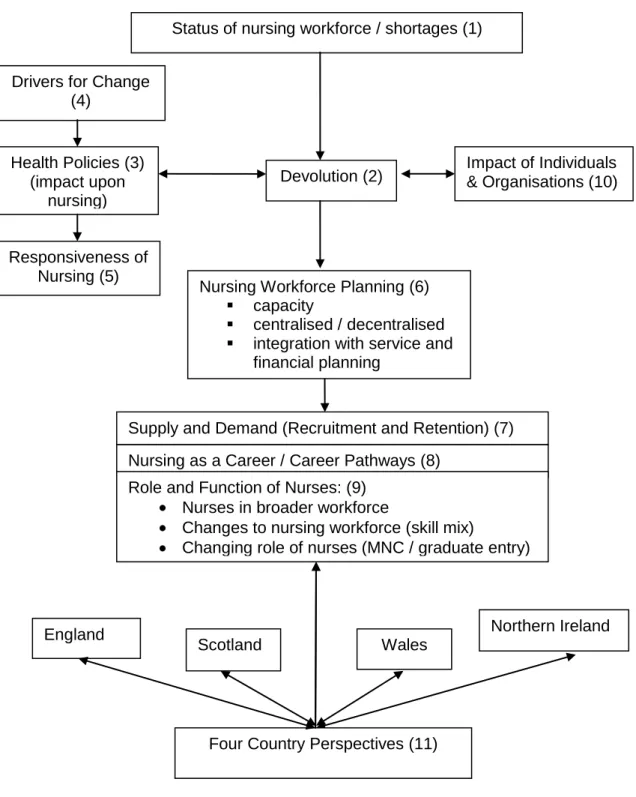
The key components of the conceptual framework and the inter-relationships between the individual elements will now be considered in more detail. The numbers in brackets link to points on the framework outlined below.
Nursing Workforce Planning (6)
capacity
centralised / decentralised
integration with service and financial planning
Devolution (2) Impact of Individuals & Organisations (10) Status of nursing workforce / shortages (1)
Drivers for Change (4) Health Policies (3) (impact upon nursing) Responsiveness of Nursing (5)
Figure 1.1 Final Conceptual Framework (Version Four)
Nursing as a Career / Career Pathways (8) Role and Function of Nurses: (9)
Nurses in broader workforce
Changes to nursing workforce (skill mix)
Changing role of nurses (MNC / graduate entry)
Scotland Wales
Northern Ireland England
Four Country Perspectives (11)
Adapted from Miles & Huberman (1994)
The starting point for this study was the researcher’s interest in the status of the nursing workforce and the repeated cycles of reported workforce shortages (1). The researcher wanted to develop greater insight into the factors which contributed to the fluctuations in the nursing workforce and began to identify potential influencing factors. Central to this study was the impact of devolution (2) on the nursing workforce and how nursing workforce policy and planning has evolved with devolution.
Following devolution, health policies were implemented in each of the three devolved countries in line with the new strategies of the respective governments and health departments (3) and many of these policies had implications for the nursing workforce. New health policies were also implemented in England reflecting the priorities of the Whitehall government. Within each of the devolved administrations there were drivers for change (4) which influenced policy development, for example changing health needs of the population or the identification of new healthcare treatments. The implementation of healthcare policies frequently have implications for the nursing workforce, which may include the need for more nurses, changes in the registered to non-registered ratio or for nurses to acquire new skills to work in different ways or in alternative settings (5). This in turn influences nursing workforce planning (6), nursing recruitment and retention (7), nursing career paths (8) and nursing roles (9).
In undertaking this research, the researcher also wanted to understand if the patterns of power and influence had changed as a consequence of devolution and the associated implications for nursing workforce policy and planning (10). The UK-wide implications of each of the factors outlined in the conceptual framework were considered initially, followed by a review of the areas of similarity or difference between the four countries (11).
1.2.3 Implementing the Conceptual Framework
The conceptual framework was used to support a consistent approach to analysis throughout the study and resulted in the same headings being used both for the literature review and for the analysis of data and reporting of findings sections of this thesis:
devolution
key health policies 3
nursing workforce planning
nursing recruitment and retention.
1.3 Background to Researcher’s Interest in Nursing Workforce Planning
In this section the researcher explains the background to her interest in nursing workforce planning and provides an overview of her prior experience in this area. It also outlines the rationale for the specific focus of this research on the impact of devolution on nursing workforce policy and planning.
Throughout a varied nursing career, the researcher developed a desire to ensure that nursing workforce planning is given sufficient consideration and is undertaken in an efficient and effective manner. This interest in NHS policy and nursing workforce planning began in the early 1990s when the researcher worked as a Ward Sister in a busy ward in an acute hospital and was keen to use a robust methodology to ensure appropriate staffing levels enabling the delivery of high quality patient care.
During the mid 1990s the researcher was employed as a Project Nurse for a Hospital Redevelopment Project in Edinburgh and one of her specific responsibilities was to determine the future nurse staffing requirements for the entire organisation, capitalising on opportunities for new ways of working across professional boundaries and in line with efficient hospital design
3
As there is a separate chapter on key health policies (chapter two), which precedes the literature review (chapter three) there is not a section on key health policies within the literature review.
principles. Consequently the researcher developed a greater knowledge of this subject area and an understanding of the tools and techniques available to support planning for the nursing workforce.
Several years later the researcher was seconded to the Scottish Executive Health Department as the Programme Manager for Nursing Workload and Workforce Planning and led a national project across NHSScotland, which resulted in the publication of the Nursing and Midwifery Workload and Workforce Planning Project report (Scottish Executive Health Department 2004a). It was following completion of this report that the researcher decided to embark upon a PhD study on this topic. Whilst researching this area it became clear that although significant attention had been placed on the impact of devolution in the UK there was a lack of research looking specifically at the impact of devolution on nursing policy or nursing workforce planning. The researcher became keen to undertake a study into this subject matter including gaining a greater insight into how health policy has diverged in the four countries following devolution and how this has affected nursing workforce policy and planning, including nursing recruitment and retention.
When the researcher embarked upon this research in 2005, as a part-time PhD student, she was seconded from NHS Lothian to the Scottish Executive Health Department. This provided her with valuable experience and insight of working within a devolved administration. The researcher subsequently relocated to England and since 2006 has been employed full time within the NHS in England, latterly working within a Local Education and Training Board of Health Education England.
Additionally, in 2009 the researcher was awarded a Florence Nightingale Foundation Travel Scholarship to visit Canada to examine the nursing workforce planning systems in place in Ontario and to identify what learning could be applied to the UK healthcare context.
Overall this professional background and experience has resulted in the researcher having a sound understanding of the complexities of nursing workforce policy and planning with the aspiration to undertake further research in this area.
1.4 Summary of Key Points
This chapter provided an introduction to the research questions; an overview of the conceptual framework developed to inform the structure of the thesis and the background to the researcher’s interest in nursing workforce policy and planning. In the next chapter the key health policies from each of the four countries over the period 1997 – 2009 will be presented and the implications for nursing workforce policy and planning considered.
Chapter Two – Health Policy Analysis
2.1 Introduction to the Policy AnalysisThis chapter provides an overview of the policy terrain across the UK over the period under review and it focuses on the policies of relevance to the nursing workforce issues examined in this thesis. At the outset of this study the researcher undertook a preliminary analysis of the health policies from each of the four UK countries. The aim of the policy analysis was to identify the main policy themes and areas of consistency and divergence between the four countries, which focused directly or indirectly on nursing workforce issues. The particular focus of this work was to gain a broad understanding of the policy context in each country at the outset of the study period in 1997 through to the key informant interviews in 2008. During the course of this research, some policies were also considered from 2009, the year after the interviews, and the principal reason for this was to provide further context to the data analysis and findings sections of the thesis. Additionally several of the policies published during 2009 were in development at the time of the interviews and some interviewees may have been involved in this policy development work.
This policy analysis assisted the researcher to develop and refine the conceptual framework for the study, as discussed in chapter one. The policy analysis also provided background information for inclusion in the literature review for example details of health policy divergence between the four UK countries is included in the devolution section, whilst polices related to nursing workforce planning or nursing recruitment and retention are summarised in these sections of the literature review. Furthermore the policy analysis enabled the researcher to identify themes for further investigation during the semi-structured interviews.
The researcher identified the health policies from each country principally through searches of the websites of the government health departments in
England, Scotland, Wales and Northern Ireland and from the reference listings in some policy documents and reports. At the outset of this study the researcher reviewed the health policies published in each of the four countries over the study period to distill the key themes and record the main implications for the healthcare workforce, particularly nursing. Throughout the research study an awareness of more current policy publications was maintained by reviewing health or nursing journals.
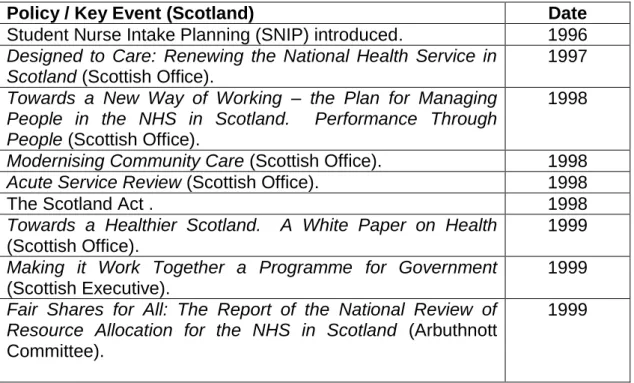
A table was developed for each of the four countries and all the health policies reviewed were listed in chronological order in the relevant table. Owing to the sheer volume of health policy documents developed across the four countries of the UK over the twelve year period under review, it was beyond the scope of this thesis to include an in-depth analysis of all the policy documents published. A summary listing of the policies analysed has been prepared for each of the four countries. The policy and key event information for Scotland is included as an exemplar in table 2.1 below, whilst the policy and key event information for England, Wales, Northern Ireland and the UK is included in Appendices IV, V, VI and VII.
Table 2.1 Scotland - Policy / Event Log
Policy / Key Event (Scotland) Date
Student Nurse Intake Planning (SNIP) introduced. 1996
Designed to Care: Renewing the National Health Service in Scotland (Scottish Office).
1997
Towards a New Way of Working – the Plan for Managing People in the NHS in Scotland. Performance Through People (Scottish Office).
1998
Modernising Community Care (Scottish Office). 1998
Acute Service Review (Scottish Office). 1998
The Scotland Act . 1998
Towards a Healthier Scotland. A White Paper on Health
(Scottish Office).
1999
Making it Work Together a Programme for Government
(Scottish Executive).
1999
Fair Shares for All: The Report of the National Review of Resource Allocation for the NHS in Scotland (Arbuthnott Committee).
Policy / Key Event (Scotland) Date
Learning Together – A Strategy for Education, Training and Lifelong Learning for all staff in the National Health Service in Scotland (Scottish Executive Health Department).
1999
Devolution introduced in Scotland. 1999
Our National Health: A Plan for Action, a Plan for Change
(Scottish Executive Health Department).
2000
Temporary Measures Managing Bank and Agency Staff
(Accounts Commission).
2000
Report of the Joint Future Group. 2000
Caring for Scotland. The Strategy for Nursing and Midwifery in Scotland (Scottish Executive Health Department).
2001
Nursing for Health – a Review of the Contribution of Nurses, Midwives and Health Visitors to Improving the Public’s Health in Scotland (Scottish Executive Health Department).
2001
Pilot of Family Health Nurse. 2001
Launch of Facing the Future Group. 2001
Facing the Future. Report of the 19th November 2001 Convention on Recruitment and Retention in Nursing and Midwifery (Scottish Executive Health Department).
2001
Planning Together (Scottish Integrated Workforce Planning Group)
2002
Response to Planning Together. Final Report of the Scottish Integrated Workforce Planning Group (Scottish Executive Health Department).
2002
Planning ward nursing – Legacy or Design? (Audit Scotland). 2002
Working for Health: The Workforce Development Action Plan for NHSScotland (Scottish Executive Health Department).
2002
Choices and Challenges: a Strategy for Research and Development in Nursing and Midwifery in Scotland (Scottish Executive Health Department).
2002
National Workforce Committee established. 2002
National Workforce Planning Unit established. 2002
NHS Education for Scotland (NES) established as a Special Health Board.
2002
Promoting Health, Supporting Inclusion: the National Review of the Contribution of all Nurses and Midwives to the Care and Support of People with Learning Disabilities (Scottish Executive Health Department).
2003
Partnership for Care: Scotland’s Health White Paper (Scottish Executive Health Department).
2003
A Scottish Framework for Nursing in Schools (Scottish Executive Health Department).
2003
A Partnership for a Better Scotland: the Policies and Programme for the Scottish Executive for the Next Four Years 2003-2007 (Scottish Parliament).
Policy / Key Event (Scotland) Date
Improving Health in Scotland – the Challenge (Scottish Executive Health Department).
2003
NHS Reform Bill. 2003
Nursing and Midwifery Workload and Workforce Planning Project (Scottish Executive Health Department).
2004
Framework for Nursing in General Practice (Scottish Executive Health Department).
2004
Nursing People with Cancer in Scotland: a Framework
(Scottish Executive Health Department).
2004
Fair to All, Personal to Each (Scottish Executive Health Department).
2004
Scottish Health Workforce Plan 2004 Baseline (Scottish Executive Health Department).
2004
NHSReform (Scotland) Act. 2004
Amendment introduced to NHS Reform Act which placed a statutory duty on all NHS Boards to have in place
arrangements for workforce planning
2004
NHS Trusts disbanded and replaced by 14 Health Boards. 2004 Appointment of new Chief Nursing Officer – Paul Martin. 2004
Workforce Numbers Group established . 2004
Nationally Co-ordinated Nurse Bank Arrangements Report and Action Plan (Scottish Executive Health Department).
2005
Framework for Developing Nursing Roles (Scottish Executive Health Department).
2005
Building a Health Service Fit for the Future A National Framework for Service Change in the NHS in Scotland
(Scottish Executive Health Department).
2005
Delivering for Health (Scottish Executive Health Department). 2005
Delivery through Leadership (Scottish Executive Health Department).
2005
National Workforce Planning Framework (Scottish Executive Health Department).
2005
The Impact of Nursing on Patient Clinical Outcomes – Developing Quality Indicators to Improve Care (NHS Quality Improvement Scotland).
2005
Reshaping the NHS? Workforce planning in the National Health Service in Scotland (Scottish Parliament Health Committee)
2005
Building a Health Service Fit for the Future. A National Framework for Service Change in the NHS in Scotland (Scottish Executive Health Department).
2005
Delivering for Health (Scottish Executive Health Department). 2005
Review of Student Nurse Intake Planning. 2005
Policy / Key Event (Scotland) Date
National Workforce Plan 2006 (Scottish Executive Health Department). Report from the first year of the new workforce planning cycle.
2006
Rights, Relationships and Recovery – the Review of Mental Health Nursing in Scotland (Scottish Executive Health Department).
2006
From Knowing to Doing: Transforming Knowledge into Practice in NHSScotland (NHS Education for Scotland).
2006
Visible, Accessible and Integrated Care – Report of the Review of Nursing in the Community in Scotland (Scottish Executive Health Department).
2006
Delivering Care, Enabling health. Harnessing the Nursing, Midwifery and Allied Health Professions’ Contribution to Implementing Delivering for Health in Scotland (Scottish Executive Health Department).
2006
The WHO Europe Family Health Nursing Pilot in Scotland: Final Report (Scottish Executive Health Department).
2006
Code of Practice for the International Recruitment of Healthcare Professionals in Scotland (Scottish Executive Health Department).
2006
Better Health, Better Care Action Plan (Scottish Government).
2007
Better Health Better Care Planning Tomorrow’s Workforce Today (Scottish Government).
2007
Implementation of Nursing and Midwifery Workload and Workforce Planning Tools and Methodologies CEL 6
(Scottish Executive).
2007
Nursing and Midwifery Workload and Workforce Planning Project. A Good Practice Guide in the Use of Supplementary Staffing (Scottish Government).
2007
Recruitment and Retention. Report of Facing the Future Sub Group and Working Groups (Scottish Government).
2007
Planning Ward Nursing – Legacy or Design. A Follow Up Report (Audit Scotland).
2007
Leading Better Care. Report of the Senior Charge Nurse Review and Clinical Quality Indicators Project (Scottish Government).
2008
Advanced Nursing Practice Toolkit (Scottish Government). 2008
Healthcare Support Workers in Scotland: Evaluation of a National Pilot of Standards and Listing in Three NHS Boards
(Scottish Government).
2009
Code of Practice for Employers of Healthcare Support Workers in Scotland (Scottish Government).
2009
A Force for Improvement: the Workforce Response to Better Health Better Care (Scottish Government).
2.2 Healthcare Policies from 1997 to 1999
Shortly after the election of the Labour Government in 1997, policies were developed in England, Scotland and Wales which outlined the strategic vision for healthcare within the respective countries (Department of Health 1997; Scottish Office 1997; Secretary of State for Wales 1998). Although these policies detailed plans for specific structural reform of the health services within each country there were several common themes across the policies including:
changes to the internal market, introduced by the Conservative Government in 1991, which separated the functions of the purchase and provision of healthcare (Department of Health, 1989). The internal market was terminated in Scotland and modified in England and Wales. GP fund-holding was also abolished across the UK (Health Act 1999)
the need to improve access to care and an increased focus on the quality of care
a stronger emphasis on partnership working both with patients and between agencies
a shift towards the provision of more services in primary care, including greater opportunities for healthcare professionals to shape local services including the development of nurse led clinics and one-stop diagnostic clinics.
There was less policy activity in Northern Ireland where, during the period 1997-1999, the main focus of attention was a consultation on the future arrangements for health and social care. This consultation outlined proposals for the establishment of a new body the Department of Health, Social Services and Public Safety aimed at maximising the benefits of the country’s unique integrated health and social care system along with other structural reforms to support this new body (Department of Health and Social Services 1998a).
There was also a policy focus in the UK countries aimed at the rationalisation of acute hospital services, with a view to providing safer and more cost effective services for acute patient care (Scottish Office 1998a; Department of Health and Social Services 1998b; National Assembly for Wales 2000a4).
Overall the commonality in healthcare policy themes in England, Scotland and Wales between 1997 and 1999 was principally due to one political party being in Government across these countries. At this time in Northern Ireland there was a greater focus on health and social care restructuring and less health policy activity.
2.3 Healthcare Policies Post-Devolution
2.3.1 Overview
Following the introduction of devolution in 1999 there was evidence of greater health policy divergence between the four UK countries, although it took some time for these differences to emerge. Two years after the introduction of devolution in 2001, it was reported that the Green and White papers from the different countries detailed ‘challenging agendas which would not be implemented overnight’ (Constitution Unit 2001, p.8), however differences were already emerging in the way health services were being delivered particularly primary care services. At the outset of devolution there was also a commitment from all four countries to deliver policies rooted in ‘investment and reform’ (Woods 2004, p.337) and related to this targets were set for nursing workforce growth in England, Scotland and Wales. The different policy priorities for each of the four countries are outlined in the sections below.
2.3.2 England
The NHS Plan. A plan for investment. A plan for reform (Department of Health 2000a) outlined plans for the NHS in England over the next decade. The key focus of this policy was on ‘modernisation’ of the health service.
4
Commitments were made to cut waiting times, reduce health inequalities, address inequities in access to care, improve quality of care and cleanliness of hospitals. These reforms would be delivered through re-design of services, supported by the NHS Modernisation Agency, and an increased focus on performance management. Core national standards and performance targets would be monitored and action taken where healthcare organisations were seen to be failing. The NHS Plan also included proposals for a concordat between the NHS and Private Sector enabling the NHS to make use of extra capacity in this sector to benefit the care and treatment of NHS patients.
Commitments were made to improve pay and working conditions for NHS staff along with increased numbers of staff including targets for 20,000 additional nurses and 1,000 Nurse Consultants. The Modern Matron role, unique to the English healthcare context, was introduced to oversee the quality of care in clinical areas. Opportunities were cited for nurses to take on new roles and increased responsibilities.
The publication of The NHS Improvement Plan Putting People at the Heart of Public Services (Department of Health 2004a) reinforced the principles of reform and improved performance associated with implementing the second phase of the NHS Plan. The focus of this policy was on the next stage of the NHS in England’s journey to: ‘ensure that a drive for responsive, convenient and personalised services takes root across the whole of the NHS and for all patients’ (p.8). It emphasised the need for staff to work flexibly and in new ways to deliver more personalised patient care in a modernised health service.
Subsequently, the NHS Next Stage Review programme of work led by Professor the Lord Darzi, required each of the ten Strategic Health Authorities in England to develop plans to transform services across eight defined care pathways; staying healthy; maternity and newborn; children;
acute care; planned care; mental health; long term conditions and end of life. The principal aim of A High Quality Care for All: NHS Next Stage Review
(Department of Health 2008a) was to stimulate locally led changes across these care pathways which were both patient focused and clinician driven. There was a strong emphasis on improving the quality of care, increasing patient choice and creating opportunities for greater personalisation in healthcare.
The key role of nurses in leading and delivering these improvements was highlighted in A High Quality Care for All, whilst the accompanying policy document A High Quality Workforce (Department of Health 2008b) detailed the expectations of clinicians in delivering the aims of the NHS Next Stage Review. This included work to ‘reaffirm the role of the nurse’ and update definitions of current day nursing; develop mechanisms to measure the quality of nursing care; increase investment in preceptorship periods for newly qualified staff; greater flexibility in career paths including strengthening clinical academic careers; new national standards for advanced nursing roles and the proposal to explore options for graduate entry to pre-registration nursing (Department of Health 2008b, p.18).
2.3.3 Scotland
In Scotland Our National Health: A Plan for Action, a Plan for Change
(Scottish Executive Health Department 2000) outlined plans to re-build the NHS and identified the national priorities for health. There was a clear focus on the opportunities for health created through devolution. Increased investment would be directed at improving health and creating a health service fit for the 21st century. Proposals included a national health improvement fund, increased hospital redevelopment programmes, new GP practices and community health services. Managed Clinical Networks would be established linking local and regional services, strengthening clinical leadership and improving the quality of care. The key clinical priorities were reaffirmed as being: coronary heart disease, cancer and mental health.
Commitments were made to modernise pay for NHS staff, in line with the other UK health departments and there was increased investment planned to support learning and development. Partnership working with staff was seen as essential as was the need to develop consistent personnel policies for use across the NHS in Scotland.
The Partnership Agreement committed to bring 12,000 nurses and midwives into the NHS by 2007 as part of an initiative to deliver improvements in the NHS in Scotland (Scottish Executive Health Department 2003a).
In 2005, Building a Health Service Fit for the Future commonly known as the ‘Kerr Report’ was published (Scottish Executive Health Department 2005a).
The recommendations included the rationalisation of specialist and complex care into fewer centres to reduce clinical risk; the importance of supported self care for long term conditions; maintaining local services particularly to meet the needs of remote and rural areas; harnessing the use of telemedicine and information technology to improve efficiencies and further action to reduce waiting times and health inequalities. It acknowledged that in order to deliver these changes a re-profiling of the existing workforce was required including investment in education and training to develop new ways of working for example the implementation of Hospital at Night teams. There were opportunities for nurses to have a lead role in these new teams.
Delivering for Health (Scottish Executive Health Department 2005b) the Government’s response to Building a Health Service Fit for the Future
(Scottish Executive Health Department 2005a) endorsed the report’s recommendations and identified actions aimed at shifting the balance of care from acute hospitals to an increased delivery of health and wellbeing services in the local community. It also included plans to strengthen performance management of key priorities and targets.
Following the change of Government in Scotland in 2007, the strategic vision of the new Scottish National Party was outlined in the Better Health, Better Care: Action Plan (Scottish Government 2007a). There were three main themes in this policy:
developing a ‘mutual’ NHS
supporting health improvement and tackling health inequalities, with a particular focus on disadvantaged communities
better, local access to healthcare including improved patient safety, quality, efficiency and effectiveness.
Central to this policy was the concept of a mutual NHS where the public and staff are partners in the NHS. This included a prominence on the shift in the ownership and responsibility for health to individual citizens. Performance management targets were revised to address health improvement; efficiency and governance; access and treatment. The importance of Managed Clinical Networks was reinforced and plans were included to expand and strengthen these. There was a clear statement in the policy foreword detailing that NHSScotland was distancing itself further from the ‘market orientated models’ (Scottish Government 2007a, p.v), which was Scotland signaling its rejection of the model of healthcare in place in England.
Although the Better Health, Better Care: Action Plan made specific reference to workforce planning, new roles and leadership development, a related document ‘Better Health, Better Care: Planning Tomorrow’s Workforce
Today’ (Scottish Government 2007b) was published outlining proposals to deliver further improvements in workforce planning, including developing workforce planning capacity at NHS Board level. There was also a focus on creating new roles based on patient needs and the importance of education and training for both the current and future healthcare workforce.
2.3.4 Wales
In 2001 Improving Health in Wales: a Plan for the NHS and its Partners
(National Assembly for Wales 2001a) set the strategic direction for the NHS in Wales over the next decade. The main focus was on improving health and addressing inequalities in health. The vision was for an integrated healthcare system across primary, secondary and tertiary services, with stronger partnership working across organisational boundaries and greater patient involvement. This plan also committed to modernising pay and terms and conditions for staff and a number of initiatives were included to ensure the workforce was prepared for future roles: for example leadership development, partnership working, reviews of job design and increased opportunities for flexible working.
Building upon and updating the work of Improving Health in Wales, in 2005 a further ten year strategy was published Designed for Life – Creating World Class Health and Social Care for Wales in the 21st Century (Welsh Assembly Government 2005a) the focus of this policy was on promoting a national health service for the people of Wales, as opposed to a national illness service. This vision encompassed increased personal responsibility for health and well-being amongst the public. Targets were included for prevention, better access to services and improvements in quality for the following priorities: mental health; chronic disease management; children and young people’s services; older people’s services and cancer services. A range of enablers were identified encompassing performance management; service reconfiguration; professional leadership; clinical networks; research and evaluation; education, training and workforce re-design. A commitment was made for 6,000 additional nurses and the development of a workforce strategy to support the implementation of Designed for Life.
In 2006 Designed to Work (Welsh Assembly Government) was published and this workforce strategy was aimed at supporting the development of new roles and different ways of working. The key principles included more
responsive workforce planning and education commissioning; working in partnership with staff to deliver change and workforce re-design based on patient pathways, across both professional and organisational boundaries. This strategy also included the introduction of two new organisations: the Workforce Development and Contracting Unit and the National Leadership and Innovation Agency for Healthcare.
2.3.5 Northern Ireland
It was reported that after the prolonged period of direct rule from Westminster, the resultant position in Northern Ireland was that health policies were out of date and did not meet the needs of the population, additionally the delivery of structural change was slow (Greer 2001). The political situation in Northern Ireland resulted in a culture of ‘minimal policy activity’ where the main focus was on keeping health and social care services running during the civil war (Greer 2004a, p.159).
Between 1999 and 2002 the policy activity in Northern Ireland was centred on developing primary care services and reviewing acute care provision (Department of Health, Social Services and Public Safety 2000, 2001, 2002a). Following the suspension of the Northern Ireland Assembly in October 2002 and the consequent reversion back to direct rule by Westminster, the policy activity was mainly directed at modernising health and social services in Northern Ireland (Department of Health, Social Services and Public Safety 2004; 2005a).
The sections above provided an outline of the key policy documents in each of the four countries, however there was one particular area of common policy across the four countries worthy of note which was the shift of care from acute hospitals into community settings.
2.3.6 Shift in Care to the Community
Over the period since devolution, a range of health policies have been developed detailing the need to shift care from acute hospital settings to the community or primary care (including Department of Health 2001a, 2006a, 2008a; Scottish Executive Health Department 2003b, 2005a, 2005b, 2006a; National Assembly for Wales 2001a, 2001b; Welsh Assembly Government 2003a, 2005a 2007; Department of Health, Social Services and Public Safety 2001, 2004; 2005a, 2005b). Integral to these policies was a greater emphasis on working in partnership with patients and service users.
2.4 Summary of Health Policies and the Implications for Nursing
The policy analysis provided background information on the health policy landscape in each of the four countries over the period 1997 to 2009. It outlined an overview of the strategic visions for healthcare in each of the four countries and set the context for the interviews in 2008.
Different areas of policy were given notably more attention in specific countries. For example in England there was a greater emphasis on quality improvement and performance management. Scotland was more focused on collaboration and engagement with professionals and patients, whilst priorities in Wales were aimed at improving public health and reducing inequalities.
Differentiation in policies in Northern Ireland was less noticeable but this was mainly due to the fact that for approximately half of the review period, Northern Ireland was under direct rule from Westminster. When devolution was restored in 2007 there were wider political and policy issues which needed to be addressed and therefore there was less health policy activity in Northern Ireland than in the other three countries.
The policy divergence across the four countries had potential implications for nursing and the targets for nursing workforce growth, set in three of the four countries, would require extensive recruitment activity.
The policy drive for shift in care from acute to community settings across all four countries would require nurses employed in acute settings to be trained to work autonomously in community settings. Additionally the increased focus on primary care and reducing health inequalities would require nurses to work in new roles for example as Case Managers or Community Matrons promoting the principles of supported self-care and personalisation, working with people with long term conditions to improve health and avoid admissions to acute hospitals. The opportunities created for nurses to expand their roles, through the introduction of non-medical prescribing, were also critical in supporting the changing focus of care to community and primary care settings.
In addition to the nursing workforce implications of shift in care from acute to community settings, the centralisation of specialist services onto fewer acute hospital sites would necessitate highly skilled nursing staff being employed in the specialist centres but equally nurses working in the district general hospital settings would require skills in the early recognition of deteriorating patients. Overall the combination of these healthcare policies and the new service reconfigurations has significant implications for the knowledge and skills required of the future nursing workforce.
2.5 Human Resource and Nursing Strategies
Over the period under review in this thesis (1997-2009) each of the four countries published a Human Resource Strategy and at least one Nursing Strategy. As this thesis is concerned with the changing approaches to nursing workforce policy and planning these policies were reviewed by the researcher to identify the key implications for the NHS workforce and nursing in particular.
2.5.1 Human Resource Strategies
The development of a Human Resource strategy in each country highlighted an increased recognition of the importance of the workforce in delivering high quality care. The strategies were significant policies in term of determining the future direction for the NHS workforce, of which nursing is the largest staff group.
In England, Working Together: Securing a Quality Workforce for the NHS
(Department of Health 1998), outlined proposals for recruiting, retaining and developing the NHS workforce to support modernisation of the health service in England. It included requirements for organisations to deliver improved retention rates; reduced sickness / absence rates; training and development plans and for annual workforce plans to be implemented by 2000.
In Scotland, Towards a New Way of Working – the Plan for Managing People
in the NHS in Scotland (Scottish Office 1998b) included a commitment to deliver partnership working and the creation of the Scottish Partnership Forum. Other actions in this strategy included the promotion of fair employment practice; opportunities for flexible working through family friendly policies; the importance of life long learning realised through education and training plans and the establishment of the Scottish Integrated Workforce Planning Group, as the single advisory group for strategic workforce planning.
In Wales, Delivering for Patients (National Assembly for Wales 2000b) focused on the development of a high quality, motivated and competent healthcare workforce; appropriate staffing levels and a national recruitment and retention initiative for all healthcare professions in Wales.
In Northern Ireland, The Employer of Choice. A Strategy for Managing and Developing People in the Health and Personal Social Services (Department
of Health, Social Service and Public Safety 2002b), included proposals for comprehensive workforce planning across all healthcare professions; strategies for improved recruitment and retention; reduced reliance on temporary staff; lower sickness / absence rates and a range of education and training initiatives.
Overall, the content of each of the four countries’ Human Resource Strategies was broadly consistent, although the strong focus on partnership working was unique to Scotland. The key priorities common to the Human Resource strategies related to improved recruitment and retention, commitments to develop the existing workforce, increased opportunities for flexible working and reduction in sickness / absence rates.
2.5.2 Nursing Strategies
Over the period 1998 to 2001, the Chief Nursing Officer in each of the four countries published a Nursing Strategy, essentially detailing the vision and ambition for the nursing profession in the respective countries.
The first of these four Nursing Strategies was published by Northern Ireland.
Valuing Diversity – a way forward (Department of Health and Social Services 1998c) acknowledged the need to reshape the profession to meet the healthcare needs of the next millennium, particularly through an increased focus on health promotion and illness prevention. It highlighted that ‘the problems with role negotiation, role confusion and role blurring must be addressed’ (p.17), recommending that new nursing roles must be in response to patient needs and underpinned by relevant education programmes. Test sites for nurse prescribing were announced. Opportunities for development were identified including the role of nursing in the commissioning of services to improve quality of care and the contribution of nurses to policy making. In relation to workforce planning, the need to undertake skill mix reviews in line with patient care needs and the importance of vocationally trained support staff in the nursing workforce were raised.