A Case of Severe Eosinophilia in a Preterm Infant
abstract
Eosinophilia of prematurity is commonly seen in premature infants as a result of many causes, although a sustained or progressive form is uncommon. Different pathophysiological hypotheses include de-creased circulating adrenal steroids and foreign antigen exposure. We present here a case of prolonged extreme eosinophilia in a preterm infant complicated by thrombocytopenia. The patient’s eosinophil count reached 91.48⫻109/L and remitted with nonspecific treatment.
A comprehensive clinical, laboratory, and radiologic assessment is usually required in the context of a hypereosinophilic preterm infant to recognize the triggering etiology. Nonspecific treatment was the mo-dality of choice because of unclear etiology in our case. Preterm in-fants with blood eosinophilia might not need immunomodulatory treat-ment despite extremely high absolute eosinophil counts. Pediatrics
2011;127:e767–e771
AUTHORS:Abdul R. Shahein, MBChB, MSc,aSilvio
Gonzalez, MD,bManuel Carcao, MD, FRCPC, MSc,a
Mohamed Abdelhaleem, MD,cJonathan Hellmann, MD,b
and Patrick J. McNamara, MD, MRCPCHb
Divisions ofaHematology/Oncology andbNeonatology, Department of Pediatrics, andcDepartment of Pediatric Laboratory Medicine, Hospital for Sick Children, Toronto, Ontario, Canada
KEY WORDS
eosinophilia, prematurity ABBREVIATION
RSV—respiratory syncytial virus
www.pediatrics.org/cgi/doi/10.1542/peds.2010-0260 doi:10.1542/peds.2010-0260
Accepted for publication Nov 30, 2010
Address correspondence to Patrick J. McNamara, MD, MRCPCH, Hospital for Sick Children, 555 University Ave, Toronto, Ontario, Canada M5G 1X8. E-mail: [email protected] PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2011 by the American Academy of Pediatrics FINANCIAL DISCLOSURE:The authors have indicated they have no financial relationships relevant to this article to disclose.
of premature infants and is commonly referred to as eosinophilia of prematu-rity.1Sustained or progressive
eosino-philia is an uncommon diagnostic dilemma in neonates. Previous hypoth-eses to explain the nature of the eosinophilia have included a decrease in circulating adrenal steroids2;
estab-lishment of a positive nitrogen bal-ance as indicated by steady weight gain3; response to foreign antigen
presented to the body through the gastrointestinal tract, upper airway, or intravenous routes4; and maternal
ingestion of L-tryptophan
supple-ments during pregnancy.5
In children, the main causes of eosino-philia include allergies and parasitic infestations. In rare cases it may be associated with some fungal or viral infections, malignant tumors, gastro-enteritis, or autoimmune diseases. We present here a case of prolonged ex-treme eosinophilia in a preterm infant complicated by thrombocytopenia. There was no obvious underlying etiol-ogy or specific treatment required.
CASE REPORT
Our patient was a female infant born at 24 weeks’ gestational age with a weight of 780 g. She was born at a level II community hospital by emergency cesarean delivery performed for fetal bradycardia and placenta previa. Her mother was a 40-year-old gravida 2, para 1, rubella-immune, hepatitis B surface antigen–negative, HIV-negative, and VDRL test–nonreactive woman of Filipino descent. The only medication taken during pregnancy was a short course of nasal steroids for seasonal allergies; the prenatal course was smooth otherwise. The parents have another 14-year-old girl with mild asthma who is otherwise healthy.
The infant required endotracheal intu-bation, positive-pressure ventilation, and 2 doses of endotracheal epineph-rine. Her Apgar scores were 1 at 1 minute, 2 at 5 minutes, and 8 at 10 min-utes, and her cord pH was 7.27. Her clinical evaluation at birth was unre-markable. An initial chest radiograph was consistent with respiratory dis-tress syndrome, and the patient re-ceived 1 dose of surfactant (BLES Biochemicals Inc, London, Ontario, Canada). After this initial stabilization, the patient was transferred to a qua-ternary NICU. The early neonatal course was complicated by pulmonary hemorrhage on day 3 secondary to a large ductus arteriosus for which she received 1 course of indomethacin. There were no clinical or radiologic signs of central nervous system bleed-ing. She remained intubated and re-ceived mechanical ventilation for the first month of life.
On day 23 of life she was assessed for suspected necrotizing enterocolitis. An increase in the plasma eosinophil count was noted (2.96⫻109/L), and it
remained elevated for ⬃6 days. She was treated with a 10-day course of metronidazole, ampicillin, and tobra-mycin, and by day 47 of life her
eosino-phil count had normalized. It should be noted that she received the first 21-mg dose of intramuscular palivizumab (Synagis [Abbott Laboratories, Ltd, Saint-Laurent, Quebec, Canada]) (hu-manized monoclonal antibody directed at respiratory syncytial virus [RSV]) on day 47 and had no immediate adverse events.
The eosinophil count again rose to 6.27⫻ 109/L (white blood cell count:
17.4⫻109/L) on day 59. Over the next
14 days her eosinophil and total white blood cell counts continued to rise and reached maximums of 91.8 ⫻ 109/L
and 112⫻109/L, respectively, by day
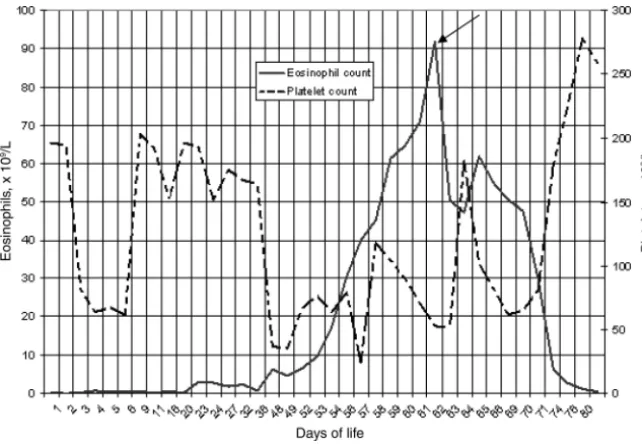
73 of life with no obvious clinical dete-rioration. The increase in eosinophil levels was temporally associated with a decrease in the platelet count to 53⫻109/L at the peak of the
hypere-osinophilia. She received 7 platelet transfusions for persistent thrombo-cytopenia during the period of eosino-philia (Fig 1).
Although there was no obvious respi-ratory deterioration, a chest radio-graph revealed a homogenous pattern of diffuse parenchymal lung infiltra-tion. She remained stable on nasal continuous positive airway pressure
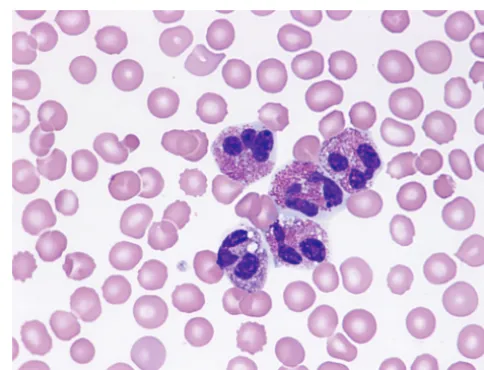
FIGURE 1
Blood film at 62 days of age (eosinophil count: 70.2⫻109/L), which shows 5 active eosinophils with a
during the eosinophilia (Fig 2). Two-dimensional echocardiography showed normal myocardial
perfor-mance and no evidence of infective en-docarditis. Abdominal ultrasound re-vealed homogenous splenomegaly and
no hepatomegaly. Results of a compre-hensive infectious workup were nega-tive. An endotracheal lavage on the day
of maximum eosinophil count (day 73 of life) revealed few Gram-positive cocci and no eosinophils. Normal tryptase levels ruled out mastocytosis.
Results of lymphocyte immunopheno-typing were normal. Mitogen-induced lymphocyte proliferation study results were normal. Peripheral blood conven-tional cytogenetics and flow cytometry
were negative for abnormal clones. Her plasma immunoglobulin E level was 42 IU/mL (normal: 6 –20 IU/mL) (Table 1).
The onset of eosinophilia coincided with receipt of a packed red blood cell
FIGURE 2
Chest radiographs that show a diffuse mixed alveolar and interstitial infiltrate pattern during the peak of the eosinophilia (A) and after normalization of the eosinophil count, showing resolution of infil-trates (B).
TABLE 1 Results of Patient Investigations Regarding Etiology and Complications of Eosinophilia
Etiology/Complication of Eosinophilia Investigation Result
Infection RSV antigen (NP swab) Negative
Parainfluenza virus types 1, 2, and 3 Negative
Virology Adenovirus (NP swab) Negative
Metapneumovirus (NP swab) Negative EM examination (urine and stool) Negative VZV, HHV-6, and HHV-7 PCR (blood) Negative HSV-1 and HSV-2, CMV, EBV, and HHV-8 PCR (blood) Negative CMV cell culture (urine) Negative Viral cell culture (urine) Negative Blood culture (aerobic) Negative
Bacteriology Urine culture (catheter) Negative
CSF culture Negative
Mycobacterial microscopy and culture (blood, BAL, gastric washing fluid)
Negative
Legionella FA and culture (BAL) Negative MRSA screening (nasal and rectal) Negative Bordetella PCR (nasal swab) Negative
Chlamydia trachomatisPCR (BAL) Negative
Chlamydia pneumoniaePCR (BAL) Negative
Mycoplasma pneumoniaePCR (BAL) Negative
Ureaplasma PCR (NP swab and BAL) Negative Malassezia culture (blood) Negative Pneumocystis examination (BAL) Negative Fungal Fungal culture (blood, urine, and nasal) Negative Fungal-panel PCR (blood) Negative Immunodeficiencies Lymphocyte mitogen stimulation (day 3) Normal
Hyper IgE syndrome IgE 42 IU/mL (normal: 6–20 IU/mL)
Mastocytosis Serum tryptase Normal
Blood malignancy and myeloproliferative syndrome
Peripheral blood conventional flow cytometry and cytogenetics No abnormalities Lymphocyte immune phenotyping No abnormal clones
Abdominal ultrasound Possible NEC, homogenous splenomegaly Bronchopulmonary dysplasia and chest
complications
Chest radiograph Homogenous pattern of alveolar space disease Endotracheal lavage No eosinophils found
Cardiac complications Echocardiogram Normal function, no pericardial effusion
Electrocardiogram Normal
Brain complications Brain ultrasound Mild periventricular leukomalacia
RSV indicates respiratory syncytial virus; NP, nasopharyngeal; EM, electron microscopy; VZV, varicella-zoster virus; HHV, human herpesvirus; PCR, polymerase chain reaction; HSV, herpes simplex virus; CMV, cytomegalovirus; EBV, Epstein-Barr virus; CSF, cerebrospinal fluid; BAL, bronchoalveolar lavage; FA, fluorescent antibodies; MRSA, methicillin-resistantStaphylococcus aureus; IgE, immunoglobulin E; NEC, necrotizing enterocolitis.
transfusion, initiation of intravenous vancomycin, tobramycin, and metroni-dazole, and recommencement of intra-venous ranitidine. In response to the unexplained increase in eosinophils she was also empirically treated with intravenous cefotaxime (4 days), am-photericin B (7 days), erythromycin (23 days), piperacillin (7 days), and ta-zobactam (7 days). Because of the the-oretical toxic end-organ effects of hy-pereosinophilia, a decision was made to perform a single-volume exchange transfusion using red cell concen-trate reconstituted with fresh-frozen plasma. Her plasma eosinophil level decreased to 47.28 ⫻ 109/L
immedi-ately after exchange transfusion but increased to 61.93⫻109/L the
follow-ing day. The level subsequently nor-malized over the next 2 weeks, as did the platelet count (Fig 3).
Her neonatal course was otherwise uneventful. Serial ultrasound scans showed subtle foci of increased echo-genicity within periventricular white matter with no definite cysts. She was transferred to a level II neonatal unit at 3 months of age and discharged from
the hospital⬃10 days later. Her motor and social development during her follow-up did not show any delay.
DISCUSSION
Our patient developed marked eosino-philia (maximum count: 91.48⫻109/L)
that was temporally associated with thrombocytopenia, but there was no evidence of significant organ damage. A nonspecific approach to manage-ment may be desirable for immature patients, in cases of unclear etiology, or in the case of a benign clinical course.
Eosinophilia is considered when the absolute eosinophil count is ⬎1.5 ⫻ 109/L. Eosinophils are produced and
mature in the bone marrow within 5 to 6 days under the control of interleu-kins 3, 5, and 15. Afterward, they are released into the bloodstream, where they circulate for a few hours before interleukin 4 induces their migration into peripheral tissues. Eosinophil counts vary according to a person’s age, gender, and ethnicity.6
Eosino-phils contain highly toxic granules that are responsible for organ damage
sinophilia for at least 6 months in association with organ/tissue damage and without an underlying secondary cause of eosinophilia.7 The
conse-quences of toxic-granule release in-clude myocarditis, thromboembolic disease, central diffuse encephalopa-thy, polyneuropaencephalopa-thy, angioedematous and urticarial skin lesions, eczema, re-strictive lung disease, eosinophilic gastroenteritis, necrotizing enterocoli-tis, anemia, thrombocytopenia, and joint effusions. The minimal duration of eosinophilia necessary to cause clinical or subclinical complications is not known. The complication spectrum of eosinophilia is wide and varies cording to which organ eosinophils ac-cumulate. The most important factor for organ predilection depends on the triggering etiology. Our patient did not manifest any clinically or laboratory-recognized organ damage. She did, however, develop severe thrombocyto-penia, which is a recognized complica-tion in 20% of adults with eosinophilia. Although the mechanism is not well un-derstood, peripheral platelet destruc-tion is the most acceptable hypothe-sis.8The highest eosinophil level ever
reported (300⫻109/L) occurred in a
6-month-old infant without proven eti-ology.9The infant had isolated
spleno-megaly, and his eosinophil count reached a normal level after 2 weeks of interferon␣treatment. This patient did not develop thrombocytopenia.
After comprehensive clinical, labora-tory, and radiologic assessments we were unable to determine the specific etiology in our case (Table 1). The spe-cific etiology of the increased eosino-phil count in our case is not known, but risk factors such as extremely low birth weight (780 g), prematurity, or necrotizing enterocolitis may have contributed. The temporal relationship
FIGURE 3
of the onset of hypereosinophilia in the child to the child receiving antibodies to RSV (palivizumab) does raise the is-sue as to whether the hypereosino-philia was a complication of the palivi-zumab vaccine. We could not find any previous reports of eosinophilia after palivizumab, but there have been re-ports of eosinophilia associated with RSV vaccine (formalin-inactivated RSV) that is not available commercially.10
Activated eosinophils were also found to promote clearance of RSV and pre-cipitate organ damage by a release function.11
Treatment of eosinophilia is usually di-rected toward the cause. Eosinophilia of hematologic origin can be divided into 2 groups: lymphocytic and myelo-proliferative. Management of the lym-phocytic type (eg, lymphoma) may include steroids, interferon ␣, cyclo-sporine A, and mepolizumab (anti–
interleukin 5 monoclonal antibodies). The approach to the myeloprolifera-tive variant (eg, acute myeloid leuke-mia) may include interferon ␣, gleevec, and hydroxyurea. Alemtu-zumab (anti-CD52 monoclonal antibod-ies) has been tried successfully on both variants and for the hypereosino-philic syndrome.12Our patient did not
show any abnormal clones in her blood. This fact made it harder to choose 1 of the above medications, which can lead to considerable comorbidity. Nevertheless, we still were pushed to undertake exchange transfusion for fear of the child devel-oping a sudden embolic event or death.
The decision to perform a single-volume exchange transfusion using red cell concentrate reconstituted with fresh-frozen plasma was made on the basis of a theoretical risk of
in-creased blood viscosity and end-organ compromise. Although there have been no previous reports about ex-change transfusion in premature in-fants with eosinophilia, the eosinophil counts decreased immediately after the exchange transfusion to 50% of its original level and continued to normalize along with the platelets over the next 2 weeks. The benign course of our patient raises some doubt over the role of immunomodu-lating treatments offered to patients with eosinophilia without a defined etiology or evidence of significant or-gan damage.
CONCLUSIONS
Blood eosinophilia in preterm infants may be a benign finding despite ex-tremely high or prolonged absolute cell counts. The specific cause in our case remains unknown.
REFERENCES
1. Hann IM. The normal blood picture in neo-nates. In: Hann IM, Gibson BES, Letsky EA, eds.Fetal and Neonatal Haematology. Lon-don, United Kingdom: Balliere Tindall; 1991: 29 –50
2. Medoff HS, Barbero GJ. Total blood eosino-phil counts in the newborn period. Pediat-rics. 1950;6(5):737
3. Gibson EL, Vaucher Y, Corrigan J. Eosino-philia in premature infants: relationship to weight gain. J Pediatr. 1979;95(1): 99 –101
4. Bhat AM, Scanlon JW. The pattern of eosin-ophilia in premature infants. J Pediatr. 1981;98(4):612– 616
5. Hatch DL, Garona JE, Goidman LR, Waller KO.
Persistent eosinophilia in an infant with p r o b a b l e i n t r a u t e r i n e e x p o s u r e t o
L-tryptophan containing supplements. Pedi-atrics. 1991;88(4):810 – 813
6. Weller PF, Bubley GJ. The idiopathic hypere-osinophilic syndrome.Blood. 1994;83(10): 2759 –2779
7. Chusid MJ, Dale DC, West BC, Wolff SM. The hypereosinophilic syndrome: analysis of fourteen cases with review of the literature.
Medicine (Baltimore). 1975;54(1):1–27 8. Ballanger F, Barbarot S. Primary
hypereosi-nophilic syndrome.Ann Dermatol Venereol. 2006;133(5 pt 1):487– 494
9. Leblond P, Lepers S, Thebaud E, et al. Idio-pathic hypereosinophilic syndrome: a case
report in an infant [in French].Arch Pediatr. 2004;11(3):219 –222
10. Rosenberg HF, Dyer KD, Domachowske JB. Respiratory viruses and eosinophils: ex-ploring the connections.Antiviral Res. 2009; 83(1):1–9
11. Phipps S, Lam CE, Mahalingam S, et al. Eo-sinophils contribute to innate antiviral im-munity and promote clearance of respira-tory syncytial virus. Blood. 2007;110(5): 1578 –1586
12. Verstovsek S, Tefferi A, Kantarjian H, et al. Alemtuzumab therapy for hypereosino-philic syndrome and chronic eosinohypereosino-philic leukemia. Clin Cancer Res. 2009;15(1): 368 –373
DOI: 10.1542/peds.2010-0260 originally published online February 28, 2011;
2011;127;e767
Pediatrics
Services
Updated Information &
http://pediatrics.aappublications.org/content/127/3/e767
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/127/3/e767#BIBL
This article cites 11 articles, 5 of which you can access for free at:
Subspecialty Collections
b
http://www.aappublications.org/cgi/collection/infectious_diseases_su
Infectious Disease
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2010-0260 originally published online February 28, 2011;
2011;127;e767
Pediatrics
Jonathan Hellmann and Patrick J. McNamara
Abdul R. Shahein, Silvio Gonzalez, Manuel Carcao, Mohamed Abdelhaleem,
A Case of Severe Eosinophilia in a Preterm Infant
http://pediatrics.aappublications.org/content/127/3/e767
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.