international journal of medical informatics 82 (2013)473–491
jo u r n al ho m e p a g e :w w w . i j m i j o u r n a l . c o m
Review
Impacts
of
second-generation
electronic
prescriptions
on
the
medication
management
process
in
primary
care:
A
systematic
review
Aude
Motulsky
∗,
Lise
Lamothe,
Claude
Sicotte
UniversitédeMontréalResearchInstituteofPublicHealth,UniversitédeMontréal,Montreal,Canada
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received1May2012 Receivedinrevisedform 5January2013 Accepted25January2013 Keywords: Electronicprescription Medicationmanagement Primarycare Systematicreview Electronicallytransmitted prescription
a
b
s
t
r
a
c
t
Objective: To describesecond-generation electronic prescription (eRx) technologies and
identifytheirimpactsonthemedicationmanagementprocessinprimarycare. Second-generationeRxtechnologieshavefocusedonnetworkingvariousstakeholderssothatthey cancommunicateelectronically.
Method:Usingkeywords,asearchwasconductedoftherelevantdatabasesuptoJanuary
2011.Amanualsearchwasconductedofthebibliographiesofthestudiesaswellastheprior systematicreviewsfound.Thetablesofcontentsofthemajorperiodicalsinthefieldwere alsosearched.ThisincludedstudiesoftheimpactsofeRxtechnologiesthatallowelectronic circulationofinformationbetweenprescriptionsitesanddispensingsites,independentof themethodologyused.Astructuredformwasusedtoextractthedata.Thestudies’impacts wereclassifiedbystageinthemedicationmanagementprocess(prescription,transmission oftheprescription,executionoftheprescriptionanduseofthemedication).
Results:Nineteenobservationalstudieswereincludedinthisreview.Mostofthem(10/19)
haveevaluatedusers’perceptionsusinginterviews,focusgroupsorquestionnaires.Two technologymodelsstandout:thepushmodel,underwhichtheprescriberdirectsthe pre-scriptiontoward aspecificpharmacy, andthepullmodel,underwhichanyauthorized pharmacycandownloadagivenprescriptionintoitssystem.Thepushmodelisthemost widelyused,particularlyintheUnitedStates.Communicationbetweenprescribersand dis-pensersisusuallyunidirectional,andcommunicationsstandardshavetoberefined.The onlydemonstratedimpactsofsecond-generationeRxtechnologieswerefoundattwolevels: positiveimpactsonthequalityofthepharmacologicalprofileavailabletoprofessionals,and negativeimpactsontheexecutionofprescriptionsinpharmacies.Stakeholders’perceptions weremixedandreflectedconsiderabledifferencesaccordingtocontext,thetypeof technol-ogyused,theintensityofitsuseanditsmaturity.Electronictransmissionofprescriptions providesanewwaytomonitorpatientcompliance.
∗ Correspondingauthor.Tel.:+15148144707.
E-mailaddress:[email protected](A.Motulsky).
1386-5056/$–seefrontmatter©2013ElsevierIrelandLtd.Allrightsreserved. http://dx.doi.org/10.1016/j.ijmedinf.2013.01.012
Conclusion:Thereislittleempiricaldatademonstratingbenefitstosecond-generationeRx technologies,evenifitisahighlypromotedmodelforimprovingprimarycarequality.More researchisrequired,withstudiesthatmeasuretheimpactsofsecond-generation tech-nologiesusingempiricaldataandconductedinthecontextofactualuse.Futurestudies shouldalsoemploythesameterminologyandprovidefulldescriptionsofcontext,typeof technologyandintensityofuse.
©2013ElsevierIrelandLtd.Allrightsreserved.
Contents
1. Introduction... 474 2. Method... 475 2.1. Literaturesearch... 475 2.2. Dataextraction... 475 3. Results... 4753.1. Generaldescriptionofthestudies... 475
3.2. Impactsassociatedwiththeprescriptionstage... 478
3.3. Impactsassociatedwiththetransmissionstage... 478
3.4. Impactsassociatedwiththepharmacistexecutionstage... 478
3.5. Impactsassociatedwiththepatientusestage... 480
4. Discussion... 480
5. Strengthsandlimitationsofthestudy ... 482
6. Conclusionandrecommendations ... 482
Authors’contributions ... 482
Conflictofinterest... 482
Appendix... 482
References... 490
1.
Introduction
Electronicprescription(eRx)technologiespromisetoimprove quality ofmedication use[1–3], which makesthem partic-ularly attractive. There are many problems related to the (mis)useofmedicationsinprimarycaresincethenumberof moleculescontinuestoincreaseandmoreandmorepatients are polymedicated. Majorinvestmentshave thereforebeen madeoverthelastdecadetoincreaseuseofeRxinprimary care.
Electronicprescriptiontechnologiesareusedindifferent ways.Bydefinition,eRx referstoanycomputerizedsystem usedtoenter,modify,reviewandcommunicateinformation onmedicationprescriptions[4].Thetechnologymaybeused on its own or linkedto an electronichealth record.There havebeentwogenerationsofeRxtechnologies:those used to“enter,modifyandreview”andthoseusedto “communi-cate.”Thefirstisfocusedondecisionsupportforphysicians andgeneratesaprintedprescription,withapapercopygiven tothepatient.Thisisastand-alonetechnologythatuseslocal electronicinformation(e.g.,thephysician’spatientrecordor medication databases)toimprove prescription quality. The second and latest generation has focused on networking variousstakeholderssothattheycancommunicate electron-ically.Itisdesignedtogivephysiciansaccesstoup-to-date pharmacological profiles on their patients as prescriptions are being written, based on the medications that patients have actually purchased at their pharmacies. In addition,
second-generationeRxtechnologiesallowprescriptionstobe transmittedelectronicallytothedispensingpharmacy.This typeoftechnologypresentsnewchallengescomparedtothe first-generation technologies,sincecoordinationisrequired betweendifferentorganizations.Thecoordinationismanaged byaprimarycaremanagement structure:private organiza-tions and localor national authorities. In some cases the communicationsnetworksarerelativelylimited (encompass-ingjustafeworganizations),butinothercasesthenetworks are designed toincludeall the organizationsinvolved ina country’smedicationmanagement.
DespitetheexistenceofmanysystematicreviewsofeRx technologies[5–7],littleisknownabouttheimpactsof second-generationtechnologies,evenifanetworkhealthinformation exchangemodelishighlypromotedfromapolicyperspective. First,fewresearchershadsofarmadeadistinctionbetween the twogenerations,comparing theimpacts ofvery differ-ent technologies. Furthermore, several systematic reviews have comparedtheimpacts oftechnologiesused in hospi-talswiththoseusedinprimarycareasiftheywerethesame thing(e.g.,thesystematicreviewbyAmmenwerthetal.[5]). Neverthelessthemedicationmanagementprocessisvery dif-ferent:inhospitals,prescriptionsareenteredintosystemsat the same placethattheyare filled,whereasinambulatory care,the informationisfragmented acrossseveral sites,in particularbecauseapatientmayconsultseveralprescribers (general practitioners, specialists). All this information is anchoredineithertheinsurerorthepharmacist,depending
international journal of medical informatics 82 (2013)473–491
475
onthecontext.Effortstoimplementsecond-generationeRx technologieshavenotbeensofarabletodrawonafull under-standingofthepotentialimpactsofthesetechnologies.This iswherewemakeacontribution.
Themainobjectiveofthissystematicreviewisto synthe-sizetheknowledgefrompublishedstudiesthatevaluatedthe impactsofasecond-generationeRxtechnologyonmedication managementinprimarycare.Morespecifically,weanswerthe followingquestions:(1)whatisthecurrentstateofresearch onsecond-generationeRxtechnologies,and(2)whatarethe impacts,bothdemonstratedandpotential,ofthese technolo-giesonthemedicationmanagementprocessinprimarycare? Forthepurposesofthisreview,anelectronicallytransmitted prescription(ETP)referstothedirect,computer-to-computer transmission of information on prescriptions, from a pre-scribertoamedicationdispenserand,dependingonthetype oftechnology,throughathirdparty[8,9].Thereforethis sys-tematicreviewdoesnotconsiderhandwrittenprescriptions, prescriptionsprintedoutusinganeRx technologyand pre-scriptionssentelectronicallybyfax.
The results ofthis review may prove useful to admin-istrators and decision makers implementing the much sought-aftersecond-generationeRxtechnologies, profession-alsinvolvedintheuseofthesetechnologies,andinvestigators interestedintheirimplementationanduse.
2.
Method
2.1. Literaturesearch
WesearchedforrelevantarticlesinEnglishandFrenchbased onkeywordsinthetitleorabstract,andMeSHtermsusing Ovid MEDLINE (1950 to January 2011), Ovid MEDLINE In-Process,andEmbase(1980toJanuary2011).Inordertofind relevantarticlesinthe socialsciencesandincognitive sci-ence,wesearchedthefollowingdatabases:CurrentContent (1993toJanuary2011),PsychInfo(1967toJanuary2011),Social ScienceCitationIndex(1979toJanuary2011),ScienceCitation Index(1979to2011),ConferenceProceedingsCitationIndex –Science(1990toJanuary2011),andConferenceProceedings CitationIndex–SocialScience&Humanities(1990toJanuary 2011)(usingtheISIWebofKnowledge).Amanualsearchwas alsoconductedofthebibliographiesofcertainpublications (studiesandpriorsystematicreviews).Similarly,thetablesof contentsofmajorperiodicalsinthisfieldwerereviewed.Fig.1 presentsthecompleteresearchstrategy,includingtheterms used.
VersionX3ofEndNotewasusedtomanagethedataand eliminate duplications. First, the articles were selected on thebasisoftheirtitlesand abstracts,whenavailable. Rele-vantpublicationswereobtainedandeachwasevaluatedby tworeviewersapplyingtheinclusion andexclusioncriteria independently.Whentheirconclusionsdiffered,the review-ersdiscussed the casewith athird reviewerto arriveat a consensus.Inordertodevelopourunderstandingofexpected andunexpectedtechnology-relatedimpacts,wedecidednot tolimittheselectionofstudies basedon themethodology used.
2.2. Dataextraction
Data on the context,the technologyand its impactswere extracted from each article using a structured form. The impactsreportedbytheauthorswereextractediftheywere related to the medication management process, based on aclassificationschemedevelopedbyBelletal.[2,10].More specifically,wewereinterestedinthefollowingstagesinthe process:prescription,transmissionoftheprescription, exe-cution ofthe prescription and use ofthe medication.This modelallowedustorelatetheobservedimpactsonthe var-iousstakeholders involved inthe medication management process,withoutlimitingtheimpactstoonestakeholderin particular.Thestudies’methodologiesweredescribedusinga classificationschemedevelopedbytheUniversityofCalifornia SanFranciscoStanford Evidence-BasedPracticeCenterthat hasbeenusedbeforeintwosystematicreviews(Kaushaletal. [11]andEslamietal.[6]).
3.
Results
AspresentedinFig.1,ourdatabasesearchesledtoaninitial sampleof1140articlesonceduplicationshadbeenremoved. Initialscreeningofabstractsrendered77articleseligiblefor fulltextreview.Basedonthefull-textreview,19studieswere excludedbecausethetechnologydidnotcorrespondtoour definitionofsecond-generationeRxtechnology(e.g. electron-icallysentfaxprescription,smartcards).Thirty-eightstudies wereexcludedbecauseevaluationoftheimpactsoftheuse ofthetechnologywasnotamainobjectiveofthestudy(e.g. descriptivestudiesofadoption).Fourstudieswereexcluded becausetheevaluationaddressedanothercomponentofthe systemthanelectronicprescriptionanditstransmission(e.g. reminderstopatients,safetyalertstoprescribers).Onestudy wasexcludedbecausetheprescriptionwasdeliveredto hos-pitalized patients, leaving 15 articlesfor detailed analyses. Anotherfour articleswere addedtothesamplefollowinga manualreviewofthebibliographiesoftheincludedstudies, ofpriorsystematicreviewsandofthetablesofcontentsofthe majorjournalsinthefield.Thefinalsampleforthisreview thereforeconsistedofatotalof19articles.
3.1. Generaldescriptionofthestudies
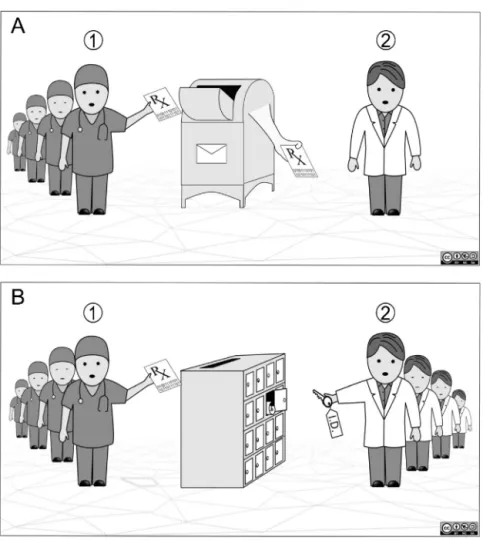
Detailedinformationonthestudies’characteristics(context, typeoftechnology,levelofuseofthetechnology,methodology, andevaluatedresults)ispresentedinTableA1inAppendix. MostofthestudieswereconductedintheU.S.(47%)[9,12–19] andSweden(26%)[20–24].Onestudywasconductedineach ofthefollowingcountries:Canada[25],theUnitedKingdom [26],theNetherlands[27], Italy[28]andSingapore[29].Two modes of prescription transmission were found: the push model(seeFig.2A),inwhichtheprescribermustspecifythe pharmacytowhichtheprescriptionwillbesent,andthepull model (seeFig. 2B),inwhich theprescriber sendsthe pre-scription to a datawarehouse that canbe accessed by all authorizedpharmacies. Inthe pullmodel, it isthe patient whogeneratesexecutionoftheprescription,whileinthepush model,thepharmacistcanexecutetheprescriptionwithout
CONCEPT1:Electronicprescription
1.Electronicprescribing*
2.DrugTherapy,Computer-assisted* 3.Communicationnetwork*
4. Electronic transfer of prescription 5. Electronic transmission of prescription 6.Electronicallytransmittedprescription 7. Electronically transfered prescription 8. Electronic prescription
9.E-prescribing 10.E-prescription
11.Electronicmedicalprescription 12.Electronicprescriptionsystem 13.E-Rx
14. On-line prescribing 15.On-lineprescription 16.1OR2OR3OR
~
OR15CONCEPT2:Ambulatorypharmacy
1.Outpatient* 2.Pharmacy* 3.Pharmacist*
4.Communityhealthservices* 5. Community network* 6. Ambulatory care* 7.Physicians,Family* 8.Familypractice* 9. Primary health care* 10.Outpatientclinic 11.Outpatientpharmacy 12.Primarymedicalcare 13. Outpatient Care 14.Primarycare 15.Generalpractitioners 16.Communitypharmacy 17.Chainpharmacy 18. Ambulatory pharmacy 19. 1 OR 2 OR 3 OR
~
OR 18 Searchquery:Concept1ANDConcept2
*:MeSHtermsusedinOVIDMedlineandEmbase
n=1063 Searchresults (n=1140) Articlesrequested andscreened (n=77) Articlesreviewed andincluded (n=19) Excluded
Mainreasonsforexclusion:
- Technologydidnotcorrespondtoourdefinitionof
second-generationelectronicprescription(n=19):electronicallysentfax
orprintedprescription(n=17);smartcards(n=2)
- Evaluationoftheimpactsoftheuseofthetechnologywasnota
mainobjectiveofthestudy(n=38)
- Evaluationofothercomponentsofthesystemthanelectronic
prescriptionand/oritstransmission(n=4)
- Electronicprescriptiondeliveredtohospitalizedpatients(n=1)
Excludedontitleandabstractreview
Mainreasonsforexclusion:
- Language
- Articletype:Literaturereviews,opinions,letters,comments,
descriptivereports
- Technology:referringtoothersystemsthanelectronic
prescription n=62 Addedby reviewing bibliogaphies n=4
Fig.1–KeywordsandMeSHterms(*)usedintheresearchstrategy,andsearchflow.
the patientbeing present.Thepush modelismore widely used(itisthepredominantmodelintheU.S.),andthe sam-pleincludedonlythreestudiesofthepushmodel[20,24,25]. ItshouldbenotedthatthedominantmodelinSwedenhas changed: studies conducted before 2006 studied the push
model[21–23],whichwasreplacedbythepullmodelthatis nowpresentthroughoutthecountry[20,24].Mostofthe stud-ies(14/19)wereconductedatoverfivedifferentprescription sendingsitesorprescriptionreceivingsites,whilethree stud-ies[12,14,28]wereconductedatasinglesite(onesendingsite
international journal of medical informatics 82 (2013)473–491
477
Fig.2–Thepushmodel(A)andthepullmodel(B)ofelectronicprescriptiontransmission.(A)Thepushmodelworkslikea
mailman:(1)whenprescribing,thephysicianindicateswhichpharmacytheprescriptionshouldbesentto;and(2)the technologydirectstheprescriptiontowardthepharmacyidentifiedwhenthephysicianenteredtheinformation.Onlythis pharmacycanreceivetheeRx,i.e.downloadtheprescriptionintoitssystem.(B)Thepullmodelworkslikeamailbox:(1) thephysiciansendstheprescriptiontoacentralizedwarehouse;and(2)allauthorizedpharmacistshaveaccesstotheeRx inthewarehouseandcandownloaditintotheirsystems.
andonereceivingsite).Ineightofthestudies,thetechnology usedwasthesameatallthesites(homogeneoussystem:same vendor,samesystem)[12,14,19,22,25,27–29],whileinnineof thestudies,differenttechnologieswereusedatdifferentsites (heterogeneoustechnology:differentvendors,different sys-tems)[9,13,15–18,20,24,26].Mostofthedatacollectedinthe publishedstudiescamefrom2006orbefore,withfivestudies conductedbefore2000[12,14,23,27,28],andonlythreestudies wereconductedafter2006[19,24,29],aparadoxical observa-tion inopposition withthe increasingpopularityof health informationexchangemodeltakingplaceinhealthcare sys-temreforms.
Thelevelofuseofthetechnologydiffersfromonestudy toanother(seeAppendixforadetailed description).Inten studies,ETPsrepresentedover15%oftheprescriptions writ-ten or processed [12,14,20–24,27–29]. In nine studies, the levelofusewashighlyvariableeitherbetweensitesorover time[9,13,15–19,25,26]. For example,attwo sitesvisited by Grossman et al. [13], the physicianscontinued to produce handwrittenprescriptions,anditwasthenurseswhoentered the prescriptions in the electronic system. This limits the
valueofphysicians’opinionsaboutthetechnology.Similarly, amongthephysiciansthatWangetal.[17]considertobeusers oftheeRxtechnology,only37%saidthattheyuseditinalltheir prescribing(anaverageof178eRx/month),while17%saidthat theyhadabandonedthetechnology.
Allthestudiesincludedinthisreviewareobservational, withorwithoutacontrolgroup(LevelIIIorLevelIV, respec-tively). Most of the studies (13/19) are Level III studies: transversal studies [9,15–18,20–23],before and afterstudies [12,14,26],andonelongitudinalstudywithacontrolgroup[27]. SixstudieshadLevelIVdesigns,meaningthattheyare obser-vational studies with no control group [13,19,24,25,28,29]. Finally, twoLevelIIIstudiesalsoincludedaLevelIVdesign for aportion ofthe study [21,22]. Thesample contains no experimentalstudy(LevelI)andnoquasi-experimentalstudy (LevelII).Thedatausedtoevaluatethe technologyusually camefromtheperceptionsofusers(physiciansor pharma-cistsandtheirstaff)(10/19studies)and/orpatients[9], and sometimesit was completedbythe investigators’ observa-tions [13,26] (but little detailed information isprovided on howtheseobservationswere includedintheanalysis).Two
studiesusedself-reportingofthework processor prescrip-tioninterventions[14,18],whileonestudydirectlyobserved thepharmacist’sworkinordertoanalyzetheimpactsofthe technology[20].Fourstudiescalculatedtherateofunclaimed prescriptionsbasedondatainthepharmacies’computersor thecomputersoftheorganizationsorcompanies distribut-ingthemedications,orbasedoncopiesoftheprescriptions obtainedfromparticipating pharmacies[12,21–23].In three studies,patients were questioned on the reasons fortheir non-compliance [21,22,28]. Finally, one study performed a comparativeanalysisofpatients’medicationrecordsby com-paringthelistofmedications givenverballybythepatient withthatgivenbythephysicianandthatgivenbythe phar-macist[27].
Themainresultsoftheincludedstudieshavebeen orga-nizedaccordingtothestageofthemedicationmanagement model(1–prescription,2–transmissionoftheprescription, 3–executionoftheprescriptionatthepharmacy,4–useof medication)andarepresentedinTable1.
3.2. Impactsassociatedwiththeprescriptionstage
Therearetwodistinctaspectstothequalityofaclinician’s prescription:afairandcompletepharmacologicalprofileand theselectionofaclinicallyandeconomicallyrelevant treat-ment.Onlyonestudymeasuredthetechnology’simpactson thequalityofpharmacologicalprofiles[27].Byassessingthe degreeoffitbetweenlistsgivenbypatients,physiciansand pharmacists,theresearchersobservedasignificantdifference betweenthegroupwithelectroniccommunications(45%)and thegroupthatreliedonpaper-basedcommunication(31%). Thepharmacologicalprofilesofpatientsweremorecomplete and up todatein thegroup communicatingelectronically. However,therewerestillsignificantdifferencesbetweenwhat medicationsthepatientssaidtheyweretakingandthosethat the physiciansand pharmacistsbelieved theywere taking. Professionalsinterviewedonthissubjectinotherstudiesdid notperceivepositiveimpactsofthetechnologywithregard tothecompletenessoraccuracyofpharmacologicalprofiles availabletophysicians[13,17,19,24].Inthesecases,itwould appearthatthisresultisrelatedtothetechnology’s imma-turity:thepharmacologicalprofileavailabletoclinicianswas notuptodate,usuallybecauseofthenumberofmedications cloggingthesystem’smemory.
Furthermore, seven studies report professionals’ per-ceptions of the impacts of eRx on prescription quality [13,15,17,19,24,25,29].Theseperceptionsweresometimes pos-itive[15,17,29]andsometimesneutralormixed[13,19,24,25]. Forexample,82%ofthephysiciansusingeRxsurveyedbyPizzi et al.[15] believed thatone ofthebenefits ofthe technol-ogywasthattherewerefewerprescriptionerrors.However, nostudyhasmeasuredsuchreductions.Similarly,the pro-fessionals participating in two studies mentioned that the technologyhadlittleeffectonadherencetoformularies,even ifthe prescribershad accesstothe formularieswhen they werechoosingthemedication[13,17].
Ontheotherhand,physicianshadmixedperceptionsof thetechnology’simpactonthetimeittakesforthemtowrite prescriptions. For example, 87% of physicianssurveyed by Tanetal.[29]weresatisfiedwiththetimeittooktowritea
prescription, and 52% of the physicians surveyed by Pizzi et al.[15]believedthatthe technologycould save prescrip-tion preparationtime,whilecertainprescribersinterviewed byWeingartetal.[19]believedthatsometimesittookmore timetowriteaprescriptionusingthetechnology.
3.3. Impactsassociatedwiththetransmissionstage
Herethetechnologypromisestoimprovesecurityand effi-ciency inthe transmission ofprescriptions to pharmacies. Noneofthestudiesevaluatedtheissueofprocesssecurity.As forefficiency,thestudiesdiscussedimpactswithrespectto thetimeittakestomanageprescriptiontransmissionandthe timespentbypatientswaitingattheirpharmacies.Two stud-iesreportclinicians’perceptionsthatthetechnologyallowed theirstafftospendlesstimesendingprescriptionsto pharma-cies[13,19].Inprinciple,underthepushmodelpatientsspend lesstimewaitingforprescriptionstobefilledatthepharmacy sincethepharmacistcan preparetheprescriptionsasthey arrivethroughouttheday.Thiswastheperceptionofsomeof thephysiciansparticipatingintwostudies[15,19],andmostof thepatientsparticipatingintheLapaneetal.study[9].Many pharmacists(andtheirteams)surveyedbyRuppand Warho-lak[16]werealsooftheopinionthatpatientsexpectedtheir prescriptionstobepreparedandreadywhentheyarrivedat theirpharmacies,whichwasperceivedaspressure.However, SugdenandWilson[26]reportedthatthepatients participat-inginpilotprojectsintheUnitedKingdomgenerallywaited longeratthepharmacyafterthetechnologyhadbeen imple-mented underboththepushand thepullmodels[26].The researchersattributedthisproblemtothepharmacists’ inex-perienceortodatatransmissionproblems.
3.4. Impactsassociatedwiththepharmacistexecution
stage
Benefitsarealsoexpectedintheprescriptionexecutionstage intermsofthequalityandefficiencyoftheprocess.Electronic prescriptions should in principle be of better quality, and theeliminationofdataentrybypharmacistsshouldreduce the risk oferrors (transcriptionand interpretation) as well asfacilitateexecutionbythepharmacist.Onthisissue,the resultsreportedbythestudiesweremixed.Professionalsin sixstudiesperceivedpositiveimpacts:theyfeltthatthe pre-scriptions were clearer, easier to read and more complete [13,15,16,19,25,29],andfeltthattheyhadtomakefewercalls tophysicians[13,25]andinterveneintheprescriptionsless often[29].Ontheotherhand,theseperceptionswerenot con-firmedinstudiesbyMurrayetal.[14]andAstrandetal.[20], whoseanalyseswerebasedonempiricaldata.Thesestudies analyzedpharmacists’workprocesses,comparingETPswith traditionalhand-writtenprescriptions,andobtainednegative results.Astrandetal.[20]observedanincreaseinthenumber ofcallsthatpharmacistshadtomaketoclarifyinformation before dispensing anETP (2% of ETPsrequire a call, com-paredto1.2%oftraditionalprescriptions).Thedatathatmost oftenneededtobecheckedwasondosageanddirectionsfor use.Accordingtotheauthors,thistypeofproblemresulted fromthewidespreaduseamongphysiciansofabbreviations thatpharmacists’computersystemscouldnotrecognize[20].
i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 8 2 ( 2 0 1 3 ) 473–491
479
Table1–Mainimpactsidentifiedinthestudies.
Processstage Impacton Positiveimpact Noimpactormixedimpact Negativeimpactorproblemcreated
Demonstrateda Perceivedb Demonstrated Perceived Demonstrated Perceived
Prescription Pharmacological profile
Moreaccurateand complete pharmacological profile[27]
Littleeffectonthe accuracyand completenessofthe pharmacologicalprofile [17,24] Incompleteor inaccurate pharmacologicalprofile [13,19]
Prescriptionquality Mayreduceprescription errors[15,17,29]
Littleeffecton prescriptionerrors
[13,19,24,25]
Littleeffecton
compliancewithdatain theformularies[13,17]
Timespentwritinga prescription
Satisfactionwiththetime spentwritingprescriptions
[29]
Littleeffectontime spentwriting prescriptions[13,15]
Incertaincases, increasesinthetime spentwriting prescriptions[19]
Transmission Managementof sending prescriptions
Mayreducethetimespent managingthesendingof prescriptionstopharmacies byclinicalstaff[13,19]
Patientwaitingtime atpharmacies
Mayreducepatients’ waitingtimeatpharmacies
[15,19]
Increasestimespent bypatientswaiting atthepharmacy[26]
orcreatespressure onpharmaciststo reducewaitingtime
[16]
Patientsexpecttobeableto receivetheirmedication morequicklyattheir pharmacy[9] Executionatthe pharmacy Technicalaspectsof theprescription Improvedprescription readabilityandclarityfor pharmacists
[13,15,16,19,25,29]
Madeprescriptionsmore complete[15]
Entryofprescription intothecomputer andverificationof theprescription
Madeprescriptionentry intothecomputereasierfor pharmacists[29] Noimpactonthe timespentby pharmacists entering prescriptionsinto thecomputer[14] Mixedimpacton prescriptionentrytimes (positivewhen prescriptionhadover threemedications)[25]
Morecallsmadeto physicianstoclarify prescriptionsas comparedto handwritten prescriptions[20]
Mayincreasethetime spententering prescriptionsintoa computersince technologycreates problemswith prescriptions[16,25]
T able 1 – ( Continued ) Pr ocess sta g e Impact on P ositi v e impact No impact or mixed impact Ne g ati v e impact or pr ob lem cr eated Demonstr ated a P e rc e ive d b Demonstr ated P e rc e ive d Demonstr ated P e rc e ive d Reduced the n umber of calls made by pharmacists to clarify pr escriptions or corr ect err ors [13,25] Mor e time spent mana g ing pr ob lems with pr escriptions compar ed to hand written pr escriptions [14] Cr eates pr ob lems that requir e an interv ention by the pharmacist to clarify the pr escription [16–18] Reduced the n umber of interv entions by pharmacists [29] Use of medication Allo w e d better patient compliance by identifying medications pr escribed but not pic ked up by patients [12,21–23,28] a Impacts we re consider ed demonstr ated when the authors measur ed and statisticall y compar ed them using an indicator . b Impacts we re consider ed per cei v e d when the y came fr om users’ per ce ptions (intervie ws or questionnair es). In addition, some studies appear in both the positi v e impacts column and the ne g ati v e impacts column when, in the same stud y, some stakeholders per cei v e d one type of impact while others per cei v e d the opposite .
Murrayetal.[14]observeda45.8%increaseinthetimespent on“problem-solvingactivitiesinvolvingprescription”(p.550). Accordingtotheauthors,“thishadmuchtodowith physi-cians’learningmoreaboutthevariousmedicationsstoredin thepharmacyinventoryandtheneedforpharmaciststohelp themdealwithavarietyofprescribingissuesthatwerenew tothem”(p.550).
Thistypeofnegativeimpactwasalsoreportedinstudies byRuppandWarholak[16](pharmacists),Motulskyetal.[25] (pharmacists)andWangetal.[17](physicians).Warholakand Rupp[18]foundthat3.8%ofETPsrequiredthatpharmacists intervene,mostofthetime(32.7%)becauseinformationwas missingfromtheprescription.Nostudyfoundthatthe tech-nologyresultedintimebeingsavedenteringprescriptionsinto thepharmacist’ssystem.IntheMurrayetal.study[14],the timespententeringprescriptionswasthe samebeforeand afterintroductionoftheeRxsystem.Thetimethat pharma-cistssaved by nothavingto enterprescriptions wasequal tothetimelostvalidatingthefieldsenteredintothesystem bythephysicians.ThepharmacistsinterviewedbyMotulsky etal.[25]feltthattheywerespendinglesstimeentering infor-mationwiththetechnologyonlywhentheETPhadoverthree medications.
3.5. Impactsassociatedwiththepatientusestage
In terms of the patient’s use of medication, the technol-ogyisexpectedtoimprovethequalityofmedicationuseas a resultofimprovementsto each stageinthe process.No studyinoursampleevaluatedsuchindicators.However,some studiesexaminedanewphenomenonresultingfromthe elec-tronictransmissionofprescriptions:evaluationsofpatients’ primary compliance through unclaimed prescriptions. Five studies[12,21–23,28]evaluatedtherateofprescriptions writ-ten but notclaimed,whichrangedfrom 1.55%[23]to2.8% [28].Threestudiesaskedpatientsabouttheirnon-compliance [21,22,28]. Overall, their non-compliance was either inten-tional (thepatientstill hadmedication athomeordidnot needtheprescription)orunintentional(thepatientdidnot knowthataprescriptionhadbeensenttothepharmacy,or theprescriptionhadbeensenttothewrongpharmacy).One studyanalyzedtheeffectivenessofimplementingsystematic calls to patientswhen the ETPswere considered essential bythemedicalteam[28].Thisinterventionwasconsidered effective sinceall ofthepatients involved(6–8 per month) eventually came topick up their medication following the call.
4.
Discussion
To our knowledge, this is the first systematic review on the impacts ofsecond-generation eRx technologies, which are used to circulate information by electronic means. Some systematic reviews have evaluated the impacts of eRx technologies, but they included all technologies with-outspecificallytargetingthesystem’scapacityforelectronic communication. Our searches led to the inclusion of 19 studies, only 3 of which were conducted since 2006. This trenddoesnotreflectcurrentresearchoneRxtechnologies,
international journal of medical informatics 82 (2013)473–491
481
whichhasgrownexponentially insince2000[6]. Also,this trend does not reflect the popularity in policy terms of healthinformationexchangemodels.Allthestudiesinthis reviewwereobservational. Excludingthestudies that have examined the phenomenon of non-compliance, only four studiesusedempiricaldata,whichcamefromsourcesother thanquestionnairesorinterviews/focusgroups[14,18,20,27]. Only two of these studies were conducted in the U.S. [14,18], including onethat was conducted almost 15 years ago[14].
ThemainimpactsofeRxareexpectedintheprescribing behaviorofphysicians:fasterdataentry,greater relevance, fewererrors,feweradversedrugreactions.Ourresults sug-gestthatsecond-generationtechnologiesdoesnotappearto reducethetimerequiredtoissueprescriptions,andmayeven increaseit[6,30,31].Thetechnologymaychangephysicians’ prescribingbehavior,butlittleisknownabouttheclinical con-sequencesofsuchchanges[32].Itisintermsofthequality of the information available to professionals that second-generationtechnologiesappeartohaveasignificantandnovel impact:theycan improvethe qualityofthe pharmacologi-calprofileavailabletophysiciansandpharmacists.Onestudy foundthispositiveimpactfromahomogeneoustechnology withbidirectionalelectroniccommunicationofinformation betweenprescribersandphysicians[27].Thishadnotbeen observedintheNorthAmericanstudies,wherethe technolo-giesandcommunicationstandardsareveryheterogeneous. Thissuggests thatthepharmacologicalprofilesavailableto differentcliniciansareoftenoutofdate.Thestudybyvander Kametal.[27]alsosuggestedanimportantroleforpatient validationsoftheinformationintheirfiles:therewerestill significantdifferencesbetweentheelectronicprofiles avail-abletotheprofessionalsandthemedicationsthatthepatients saidtheyweretaking.Whenprofessionalsuseonlyfilesfrom thelistofprescribedmedications,eitherasdispensedbythe pharmaciesorasreimbursedbyinsurers,theydonothavean accurateviewofmedicationuse.Morestudiesareneededto betterunderstandthescopeandextentofthistypeof prob-leminothercontexts.Thisresultnevertheless underscores theimportanceofdevelopingfunctionsthat allowpatients to check their pharmacological profiles and make correc-tions.
Second-generationeRxtechnologiesalsopromisespecific impacts in terms ofthe quality and efficiency of the pre-scription transmissionand executionstages. We foundno studydemonstratingimpactsonprocessquality,while pro-fessionals’perceptionswerefoundtobemixed.Asforprocess efficiency,thespecialistsfeltthatpharmacistsshouldbeable toprocessETPsmorequicklyandpatientsshouldnotwaitas long[3]. Ourreviewfoundnostudy thathasdemonstrated thistypeofpositiveimpact.Onthecontrary,twoofthe stud-ies analyzedpharmacists’work processes, comparing ETPs andhandwrittenprescriptions,andobtainednegativeresults. Thereappeartobevariousbarrierstothepotentialbenefits:
(1)delayed transmissionofthe prescription;(2) problems
inte-gratingtheprescriptionintothepharmacist’ssystem;and(3)
problemsinterpretingtheprescription,requiringpharmaciststo
callphysiciansforclarifications.Thecommunications prob-lemsserveasareminderthat, inadditiontobeingreliable andsecure,atransmissionnetworkneedstobefastifit is
to representanimprovementover the traditional informa-tiontransmissionmethod.Prescriptionintegrationproblems stemmedfromanincompletestandardizationofthe informa-tiongeneratedbyeRxtechnologies.AreportbytheNational
OpinionResearch Centeridentified twopriority standardsfor
electronicprescriptiontransmission:oneforinstructionsto patients(i.e.dosage)andonetoensurethecompatibilityof dif-ferentdatabasesonmedications,dosesandpharmaceutical forms[10].Theabundanceofdifferentdatabasesis compli-cating communication between systems. Similarly, greater harmonization of the practices ofpharmacists and physi-ciansmayimprovetheintegrationofanETPinpharmacists’ informationsystems.Lessuseoffreetextandpersonal abbre-viationsisessential.
Ourresultsalsosuggestthatwhenpharmacistsare inter-preting the prescription, the ETPs may create as many or moreproblemsthanhandwrittenprescriptions,ashasbeen observed in hospital settings [33,34]. Even though several studiesfoundthatprofessionalsappreciatetheclarityof pre-scriptions when handwritten prescriptions are eliminated, studieshavedemonstratedthattheproblemsincrease[14,20]. It should nevertheless bementioned that the resultsfrom Murray et al. [14] may not be transferable, since the pre-scriptionsweresenttoasinglepharmacyandthedatawas collectedonlyonemonthafterimplementingtheeRx technol-ogyinthepracticesetting.Otherstudiesarethereforerequired inordertobetterunderstandthedisturbancescreatedbyeRx intheprescriptionexecutionprocessinpharmacies,andin particularundertheheterogeneouspushmodelwidelyused inNorthAmerica.
Finally, ETPs offer an added value that was difficult to attain in the traditional context oforganization in pri-marycare.Prescriptions written but notclaimedended up in patients’ pockets under the traditional method. With second-generationeRxtechnologies,electronicprescriptions can be traced easily. The five studies that examined this phenomenonfoundthatthe problemwasnotencountered often (approximately 2% of the time), compared to esti-matesforhandwrittenprescriptions(approximately15%)[35]. This finding raises an important issue that should direct research onhow tobetter understanddifferences between patients’prescriptionandconsumptionhabitswhena tech-nologyisusedtogenerateprescriptions.Furthermore,given the great number of prescriptions prepared each day in a community pharmacy, these unclaimed prescriptions can quicklyfilltheshelvesofpharmaciesunderthepushmodel. Second-generationeRxtechnologiesthereforecreate distur-bances in pharmacists’ work processes that each setting needs to learn how to manage. Should an ETP be sys-tematically prepared, as soon as it enters the pharmacy? Should the patients be called first? Should some medica-tions be considered higher priority and the patients for themsystematicallycalled?Onestudydemonstratesthat sys-tematically calling patients about prescriptions considered essential ledtotheirfullcompliance[28].Morestudiesare thereforeneededinordertobetterunderstandhowto bet-ter integrate ETPs into the prescription execution process in pharmacies, and what typesof interventions are likely tohavesignificantand positiveimpactsonpatient compli-ance.
5.
Strengths
and
limitations
of
the
study
Aninherentlimitationofanysystematicreviewliesinthe research strategy and predefined inclusion and exclusion criteria.Thereisalwaysthepossibilitythatwemissedsome articles that, if included, would have affected the conclu-sionsofthisreview.However,we believethatour research strategy was for the most part inclusive, given the key words used and the databases consulted, which strength-ens our review. Furthermore, we decided to not limit the selection of studies based on the methodology used, and thisallowedustoincludeavarietyofstudiesinoursample andrevealawiderangeofimpactsthroughoutthe medica-tionmanagementprocess.Ontheotherhand,thisdecision complicatedanalysis,sinceitbecamedifficulttodistinguish perceived or even hoped-for impacts from actual impacts measuredusingempiricaldata.Second-generationeRx tech-nologies implya communication betweenvarious sites (at leastone prescriberand onedispenser site), which induce a greatheterogeneity inthe level ofuse, evenwithin one study (e.g.[13,29]),making itdifficulttoanalyze the differ-ent results. Moreover, ouranalysis revealed that often the studiesprovidedlittledetailedinformationonthe technolo-gies,which appearstobeacommon probleminpublished studiesevaluatingITinhealth[36].Consequently,it canat timesbedifficultto distinguishwhichimpacts resultfrom each of the technology’s specific functions. Finally, given thegreatheterogeneity ofstudy settings(medication man-agement models, community pharmacy practices), level of use and characteristics of eRx technologies in the various setting, the results of the studies are not easily transfer-able.6.
Conclusion
and
recommendations
Thissystematicreviewhasshedlightonthecurrentstateof ourknowledgeontheimpactsofsecond-generationeRx tech-nologiesonmedicationmanagement.Thereislittleempirical datasupportingthesupposedbenefitsofthesetechnologies. Infact,ourdatasuggestthatthetechnologiesarenotmature enough,inthe sensethat communicationisusually unidi-rectional, only from the prescriber to the dispenser, while informationonthemedicationsactuallyboughtin pharma-ciescannotbeconsultedwhenprescriptionsarewritten.In addition,communicationsstandardsdonotappeartohave beendefined,complicatingeffortstoharmonizevarious sys-tems provided by different vendors in a context of very heterogeneous practices. All efforts to developand imple-ment second-generationeRx technologies shouldtherefore be harmonized with standardization efforts. Furthermore, theobservationthatpharmacistsfacemoreproblemsshould beofinteresttobothcommunitypharmacistsand technol-ogydevelopers.Communitypharmacistshaveaninterestin becomingmoreinvolvedintechnologydevelopmentefforts inorder toensure thatthe different aspectsoftheir prac-ticeare well understoodand integrated.Developersshould also make an effort to develop functions that will allow patients tovalidate theirpharmacological profiles.Overall,
Summarypoints
Whatwasalreadyknownbeforethisstudy
• Theuseofelectronicprescription(eRx)technologiesis increasinginprimarycare
• eRx technologies are being promoted as a way to improvedthequalityofmedicationuse
Whatthisstudyhasaddedtoourknowledge
• The importance of distinguishing two generations of eRx technologies (first-generation (stand-alone technology)andsecond-generation(networking tech-nology)),andthedifferenttransmissionmodels(push andpullmodels)
• Anoverviewoftheimpactsofsecond-generationeRx onthedifferentstagesofthemedicationmanagement process
• Thefindingsthatlittleempiricaldatademonstratethe actualimpactsofsecond-generationeRxtechnologies, andthatafulldescriptionofcontext,typeof technol-ogyandintensityofusehastobeprovided.
more research is needed in terms of studies that mea-sure the impacts ofsecond-generation technologies based on empirical data, in the context of actual use. Further-more, the studies reveal that eRx can be used to assess patient compliance, paving the wayfor new interventions to improve compliance. Finally, we encourage researchers interested in eRx technologies to make detailed descrip-tions of the context of their studies and the technology’s specific functions, expressed with a shared terminology. Thiswillmakecomparisonsand knowledgesynthesis eas-ier.
Authors’
contributions
A.M.contributedtothesearch,theselection,theanalysisand themainwritingofthispaper.C.S.andL.L.respectively par-ticipatedasthesecondandthethirdreviewerintheselection step.L.L.andC.S.bothassistedwiththereadingandthe ana-lyzingoftheincludedstudies,andthewritingofthewhole paper.
Conflict
of
interest
None.Appendix.
TableA1r
e
f
e
r
e
n
c
e
s
i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 8 2 ( 2 0 1 3 ) 473–491
483
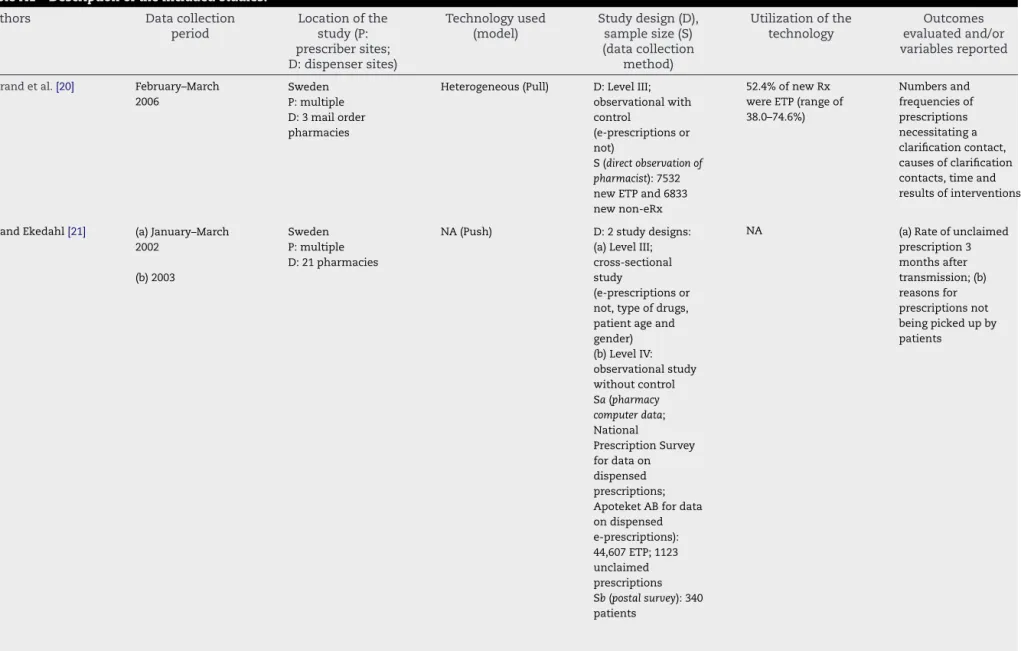
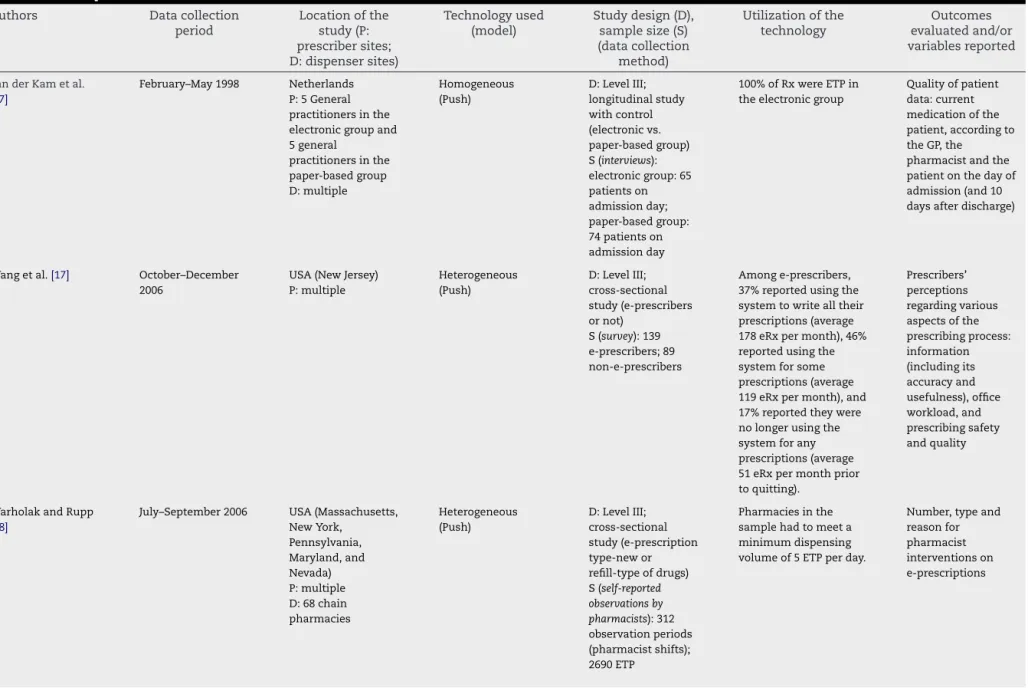
TableA1–Descriptionoftheincludedstudies.
Authors Datacollection
period Locationofthe study(P: prescribersites; D:dispensersites) Technologyused (model) Studydesign(D), samplesize(S) (datacollection method) Utilizationofthe technology Outcomes evaluatedand/or variablesreported Astrandetal.[20] February–March
2006
Sweden P:multiple D:3mailorder pharmacies
Heterogeneous(Pull) D:LevelIII; observationalwith control
(e-prescriptionsor not)
52.4%ofnewRx wereETP(rangeof 38.0–74.6%) Numbersand frequenciesof prescriptions necessitatinga clarificationcontact, causesofclarification contacts,timeand resultsofinterventions S(directobservationof
pharmacist):7532 newETPand6833 newnon-eRx AxandEkedahl[21] (a)January–March
2002 (b)2003
Sweden P:multiple D:21pharmacies
NA(Push) D:2studydesigns: (a)LevelIII; cross-sectional study
(e-prescriptionsor not,typeofdrugs, patientageand gender) (b)LevelIV: observationalstudy withoutcontrol Sa(pharmacy computerdata; National PrescriptionSurvey fordataon dispensed prescriptions; ApoteketABfordata ondispensed e-prescriptions): 44,607ETP;1123 unclaimed prescriptions Sb(postalsurvey):340 patients
NA (a)Rateofunclaimed prescription3 monthsafter transmission;(b) reasonsfor prescriptionsnot beingpickedupby patients
i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 8 2 ( 2 0 1 3 ) 473–491
TableA1–Descriptionoftheincludedstudies.
Authors Datacollection
period Locationofthe study(P: prescribersites; D:dispensersites) Technologyused (model) Studydesign(D), samplesize(S) (datacollection method) Utilizationofthe technology Outcomes evaluatedand/or variablesreported Cragheadand Wartski[12] February–March 1988 USA(Kentucky) (IrelandArmy Community Hospital) Homogeneous (Push) D:LevelIII; observational before–afterstudy (retrospective) NA Rateofunclaimed prescriptions5days aftertransmission P:onecommunity hospital D:oneoutpatient pharmacy S(pharmacycomputer data;noncompliance report–reportsent totheproviderifthe prescription remainedunclaimed after5days):15,945 ETP;293unclaimed prescriptions Ekedhaletal.[23] August–September
1997
Sweden P:multiple D:10pharmacies
NA(Push) D:LevelIII; cross-sectional study
(e-prescriptionsor not,typeofdrugs, patientage) S(copyofprescriptions frompharmacy; National PrescriptionSurvey fordataon dispensed prescriptions):8054 ETP;155unclaimed prescriptions
17%ofRxwereETP Rateof non-redeemed prescription
EkedhalandManson
[22] (a)March–May2000 (b)October2001 Sweden P:multiple D:21pharmacies Homogeneous (Push)
D:2studydesigns: 21.7%ofRxwereETP (a)Rateof non-redeemed prescription4–7 monthsafter transmission
i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 8 2 ( 2 0 1 3 ) 473–491
485
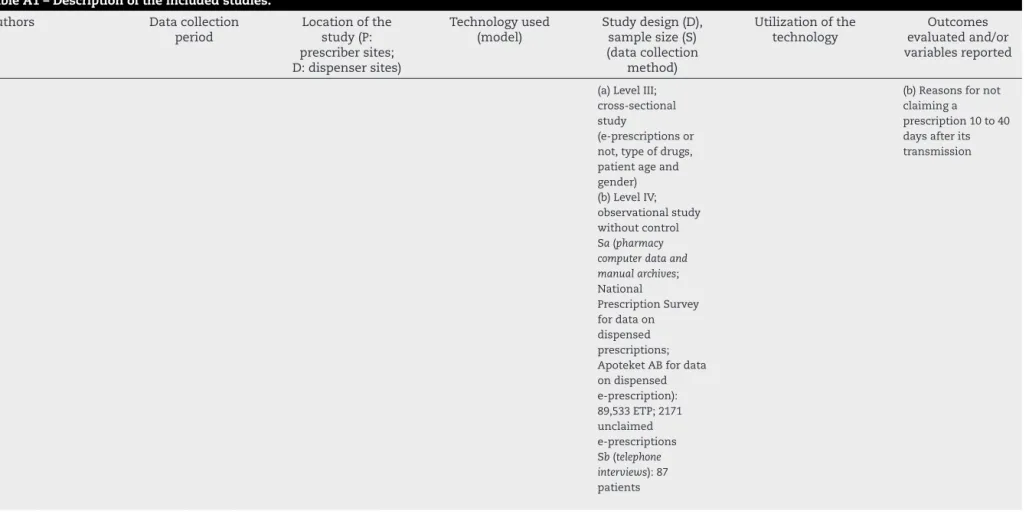
TableA1–Descriptionoftheincludedstudies.
Authors Datacollection
period Locationofthe study(P: prescribersites; D:dispensersites) Technologyused (model) Studydesign(D), samplesize(S) (datacollection method) Utilizationofthe technology Outcomes evaluatedand/or variablesreported (a)LevelIII;
cross-sectional study
(e-prescriptionsor not,typeofdrugs, patientageand gender)
(b)Reasonsfornot claiminga
prescription10to40 daysafterits transmission
(b)LevelIV; observationalstudy withoutcontrol Sa(pharmacy computerdataand manualarchives; National PrescriptionSurvey fordataon dispensed prescriptions; ApoteketABfordata ondispensed e-prescription): 89,533ETP;2171 unclaimed e-prescriptions Sb(telephone interviews):87 patients
i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 8 2 ( 2 0 1 3 ) 473–491
TableA1–Descriptionoftheincludedstudies.
Authors Datacollection
period Locationofthe study(P: prescribersites; D:dispensersites) Technologyused (model) Studydesign(D), samplesize(S) (datacollection method) Utilizationofthe technology Outcomes evaluatedand/or variablesreported Grossmanetal.[13] November
2005–March2006
USA(NewJersey) P:15practiceswith eRxand6practices withouteRx
Heterogeneous (Push)
D:LevelIV; observational withoutcontrol(few methodological details) S(interviews, observations):44 discussionswith respondentsfrom26 organizations
PracticeswitheRx: Themajorityof practiceshadfully implemented e-prescribing,with abouthalfofthe practices’systemsin placeformorethan twoyears. Onlythepractices withstand-alone e-prescribing systemswereusing electronicdata interchange(EDI), whichallows electronic transmission betweenphysician practicecomputers andpharmacy computers. Practiceestimatesof thepercentageof prescriptions printedrangedfrom only10%tocloseto 100%.
Facilitatorsand barriersto e-prescribing adoptionanduse; perceptionsofthe effectsof e-prescribingon practiceoperations, prescribingpatterns, andpatient satisfaction
Hellstrometal.[24] September–October 2007
Sweden P:7healthcare regions
Heterogeneous(Pull) D:LevelIV; observational withoutcontrol
Between50%and 86%ofdispensed e-prescriptionsin eachhealthcare regionstudied. Physicians’attitudes towarde-prescribing S(survey):180 physicians Fifteenpercentof therespondentshad usedanelectronic systemfortwo monthstooneyear, and85%formore thanoneyear.
i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 8 2 ( 2 0 1 3 ) 473–491
487
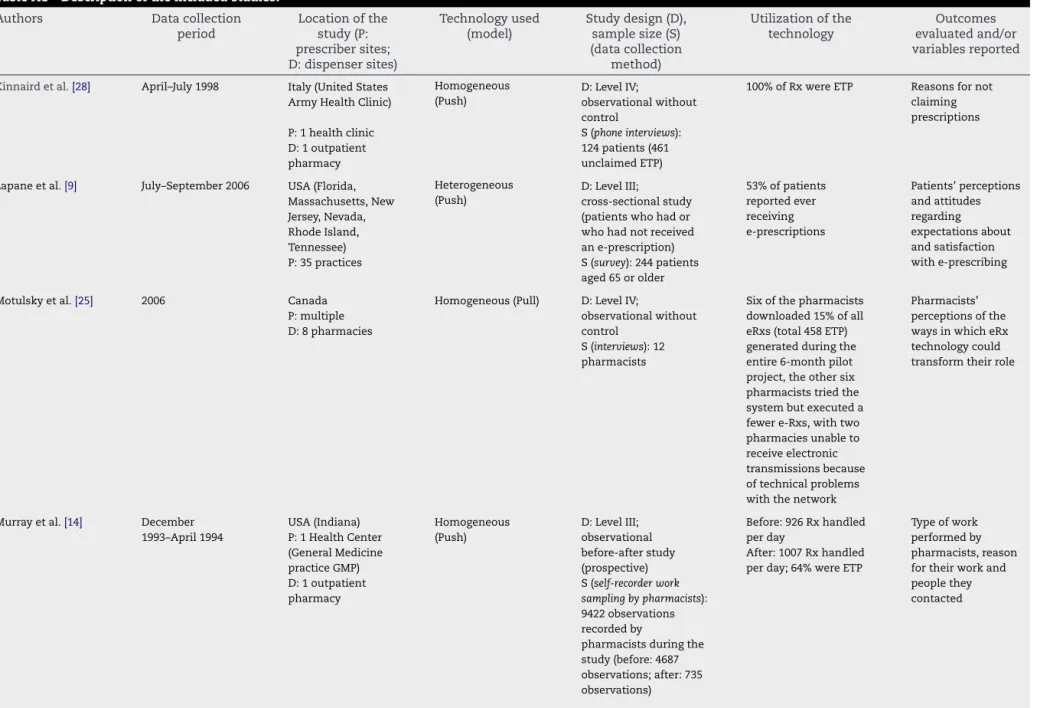
TableA1–Descriptionoftheincludedstudies.
Authors Datacollection
period Locationofthe study(P: prescribersites; D:dispensersites) Technologyused (model) Studydesign(D), samplesize(S) (datacollection method) Utilizationofthe technology Outcomes evaluatedand/or variablesreported Kinnairdetal.[28] April–July1998 Italy(UnitedStates
ArmyHealthClinic)
Homogeneous (Push)
D:LevelIV;
observationalwithout control
100%ofRxwereETP Reasonsfornot claiming prescriptions P:1healthclinic S(phoneinterviews):
124patients(461 unclaimedETP) D:1outpatient
pharmacy Lapaneetal.[9] July–September2006 USA(Florida,
Massachusetts,New Jersey,Nevada, RhodeIsland, Tennessee) Heterogeneous (Push) D:LevelIII; cross-sectionalstudy (patientswhohador whohadnotreceived ane-prescription) 53%ofpatients reportedever receiving e-prescriptions Patients’perceptions andattitudes regarding expectationsabout andsatisfaction withe-prescribing P:35practices S(survey):244patients
aged65orolder Motulskyetal.[25] 2006 Canada
P:multiple D:8pharmacies
Homogeneous(Pull) D:LevelIV;
observationalwithout control
S(interviews):12 pharmacists
Sixofthepharmacists downloaded15%ofall eRxs(total458ETP) generatedduringthe entire6-monthpilot project,theothersix pharmaciststriedthe systembutexecuteda fewere-Rxs,withtwo pharmaciesunableto receiveelectronic transmissionsbecause oftechnicalproblems withthenetwork
Pharmacists’ perceptionsofthe waysinwhicheRx technologycould transformtheirrole
Murrayetal.[14] December 1993–April1994 USA(Indiana) P:1HealthCenter (GeneralMedicine practiceGMP) D:1outpatient pharmacy Homogeneous (Push) D:LevelIII; observational before-afterstudy (prospective) S(self-recorderwork samplingbypharmacists): 9422observations recordedby
pharmacistsduringthe study(before:4687 observations;after:735 observations) Before:926Rxhandled perday After:1007Rxhandled perday;64%wereETP
Typeofwork performedby pharmacists,reason fortheirworkand peoplethey contacted
i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 8 2 ( 2 0 1 3 ) 473–491
TableA1–Descriptionoftheincludedstudies.
Authors Datacollection
period Locationofthe study(P: prescribersites; D:dispensersites) Technologyused (model) Studydesign(D), samplesize(S) (datacollection method) Utilizationofthe technology Outcomes evaluatedand/or variablesreported Pizzietal.[15] February2003 USA(Florida,
Massachusetts,New Jersey,Nevada, RhodeIsland,and Tennessee) Heterogeneous (Push) D:LevelIII; cross-sectional study(e-prescribers ornot) 14.85%of respondentswere eRxusers Perceivedbenefits andbarriersto adoptionanduseof eRxsystems P:multiple S(survey):164 e-prescribersand 842traditional prescribers (physicians) Ruppetal.[37] April–July2006 USA(Florida,
Massachusetts,New Jersey,Nevada, RhodeIsland,and Tennessee) Heterogeneous (Push) D:LevelIII; cross-sectional study(e-prescription ornot) Pharmaciesincluded inthesamplehadto meetaminimum dispensingvolume of5ETPperday
Attitudes,beliefs andsatisfaction withe-prescribing (comparedwith conventional prescribing) P:multiple S(survey):1094 pharmacypersonnel D:276chain pharmacies SugdenandWilson
[26] 2002–2003 UK 3pilots,including P:34practices D:23pharmacies Heterogeneous (Push-2pilots;Pull-1 pilot) D:LevelIII; observational before–afterstudy (fewmethodological details)
TakeupofETPwas muchslowerthan anticipated.Inthelast twomonthsof2002,it reachedsignificant volumes(anaggregate ofnearly15,000 dispensedprescriptions)
Contentofinformation, changesinprocessesof communication,service andqualityofcare, workloadandwork practicesof stakeholders, stakeholders’attitudes toETP,useofETP S(interviews,focus
group,observations): NA
Tanetal.[29] October2007 Singapore P:9polyclinics D:9pharmacies(one polycliniccan transmit prescriptionstoonly onepharmacy) Homogeneous (Push) D:LevelIV; observationalstudy withoutcontrol S(survey):118 physiciansand61 pharmacystaff 7.3%ofrespondents hadbeenusingeRx forlessthana month,23.6%for1–3 months,41%for morethan6months.
Usersatisfactions; perceptionsregardingthe impactoftheuseof electronicprescriptionson prescriptionerrorsand interventions
i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 8 2 ( 2 0 1 3 ) 473–491
489
TableA1–Descriptionoftheincludedstudies.
Authors Datacollection
period Locationofthe study(P: prescribersites; D:dispensersites) Technologyused (model) Studydesign(D), samplesize(S) (datacollection method) Utilizationofthe technology Outcomes evaluatedand/or variablesreported vanderKametal.
[27]
February–May1998 Netherlands P:5General practitionersinthe electronicgroupand 5general practitionersinthe paper-basedgroup D:multiple Homogeneous (Push) D:LevelIII; longitudinalstudy withcontrol (electronicvs. paper-basedgroup) S(interviews): electronicgroup:65 patientson admissionday; paper-basedgroup: 74patientson admissionday 100%ofRxwereETPin theelectronicgroup
Qualityofpatient data:current medicationofthe patient,accordingto theGP,the
pharmacistandthe patientonthedayof admission(and10 daysafterdischarge)
Wangetal.[17] October–December 2006
USA(NewJersey) P:multiple Heterogeneous (Push) D:LevelIII; cross-sectional study(e-prescribers ornot) S(survey):139 e-prescribers;89 non-e-prescribers Amonge-prescribers, 37%reportedusingthe systemtowritealltheir prescriptions(average 178eRxpermonth),46% reportedusingthe systemforsome prescriptions(average 119eRxpermonth),and 17%reportedtheywere nolongerusingthe systemforany prescriptions(average 51eRxpermonthprior toquitting). Prescribers’ perceptions regardingvarious aspectsofthe prescribingprocess: information (includingits accuracyand usefulness),office workload,and prescribingsafety andquality
WarholakandRupp
[18]
July–September2006 USA(Massachusetts, NewYork, Pennsylvania, Maryland,and Nevada) P:multiple D:68chain pharmacies Heterogeneous (Push) D:LevelIII; cross-sectional study(e-prescription type-newor refill-typeofdrugs) S(self-reported observationsby pharmacists):312 observationperiods (pharmacistshifts); 2690ETP Pharmaciesinthe samplehadtomeeta minimumdispensing volumeof5ETPperday.
Number,typeand reasonfor pharmacist interventionson e-prescriptions
T able A1 – Descr iption of the included studies. A uthors Data collection period Location of the stud y (P: pr escriber sites; D: dispenser sites) T e chnolo gy used (model) Stud y design (D), sample size (S) (data collection method) Utilization of the tec hnolo gy Outcomes e v aluated and/or v aria b les re ported W eing art et al. [19] Summer 2007 USA (Massac husetts) P: m ultiple Homo g eneous (Push) D: Le v e l IV ; observ ational without contr ol S ( focus gr oup ): 3 focus gr oups with 21 ph ysicians, 3 n urse pr actitioners, 1 ph ysician assistant Clinicians had used e-pr escribing for 2.5 y ears (r ang e 1.0–5.5) and wr ote the majority (89% rang e 15–100%) of their pr escriptions electr onicall y. P e rc e ptions re g a rding the use and v alue of e-pr escribing in g ener al and medication safety alerts in particular eRx: electr onic pr escription; ETP: electr onicall y tr ansmitted pr escription; NA : not a v aila b le; Rx: pr escription.
[1] M.H.Ridinger,Theelectronicprescriptionconundrum:why “e-Rx”isn’tso“e-Z”,Clin.Pharmacol.Ther.81(1)(2007) 13–15.
[2] D.Bell,S.Cretin,R.S.Marken,A.B.Landman,Aconceptual frameworkforevaluatingoutpatientelectronicprescribing systemsbasedontheirfunctionalcapabilities,J.Am.Med. Inform.Assoc.11(1)(2004)60–70.
[3] D.Papshev,A.M.Peterson,Electronicprescribingin ambulatorypractice:promises,pitfalls,andpotential solutions,Am.J.Manage.Care7(7)(2001)725–736. [4] A.D.Black,J.Car,C.Pagliari,C.Anandan,K.Cresswell,T.
Bokun,B.McKinstry,R.Procter,A.Majeed,A.Sheikh,The impactofehealthonthequalityandsafetyofhealthcare:a systematicoverview,PLoSMed.8(1)(2011)16.
[5] E.Ammenwerth,P.Schnell-Inderst,C.Machan,U.Siebert, Theeffectofelectronicprescribingonmedicationerrors andadversedrugevents:asystematicreview,J.Am.Med. Inform.Assoc.15(5)(2008)585–600.
[6] S.Eslami,A.Abu-Hanna,N.F.deKeizer,Evaluationof outpatientcomputerizedphysicianmedicationorderentry systems:asystematicreview,J.Am.Med.Inform.Assoc.14 (4)(2007)400–406.
[7] S.Eslami,N.F.deKeizer,A.Abu-Hanna,Theimpactof computerizedphysicianmedicationorderentryin hospitalizedpatients—asystematicreview,Int.J.Med. Inform.77(6)(2008)365–376.
[8] M.Makinen,J.Forsstrom,M.Aarimaa,P.Rautava,A Europeansurveyonthepossibilitiesandobstaclesof electronicprescriptionsincross-borderhealthcare, Telemed.e-Health12(4)(2006)484–489.
[9] K.L.Lapane,C.Dube,K.L.Schneider,B.J.Quilliam,Patient perceptionsregardingelectronicprescriptions:isthe geriatricpatientready?J.Am.Geriatr.Soc.55(8)(2007) 1254–1259.
[10] NationalOpinionResearchCenter,Findingsfromthe evaluationofe-prescribingpilotsites,AgencyforHealthcare ResearchandQuality,ReportNo.:07-0047-EF,2007.
[11] R.Kaushal,K.G.Shojania,D.W.Bates,Effectsof
computerizedphysicianorderentryandclinicaldecision supportsystemsonmedicationsafety:asystematicreview, Arch.Intern.Med.163(12)(2003)1409–1416.
[12] R.Craghead,D.Wartski,Effectofautomatedprescription transmittalonnumberofunclaimedprescriptions,Am.J. Health.Syst.Pharm.46(2)(1989)310–312.
[13] J.M.Grossman,A.Gerland,M.C.Reed,C.Fahlman,J.M. Grossman,A.Gerland,M.C.Reed,C.Fahlman,Physicians’ experiencesusingcommerciale-prescribingsystems, HealthAff.(Millwood)26(3)(2007)w393–w404. [14] M.D.Murray,B.Loos,W.Tu,G.J.Eckert,X.H.Zhou,W.M.
Tierney,Effectsofcomputer-basedprescribingon pharmacistworkpatterns,J.Am.Med.Inform.Assoc.5(6) (1998)546–553.
[15] L.T.Pizzi,D.C.Suh,J.Barone,D.B.Nash,Factorsrelatedto physicians’adoptionofelectronicprescribing:resultsfroma nationalsurvey,Am.J.Med.Qual.20(1)(2005)
22–32.
[16] M.T.Rupp,T.L.Warholak,Evaluationofe-prescribingin chaincommunitypharmacy:best-practice
recommendations,J.Am.Pharm.Assoc.48(3)(2008) 364–370.
[17] C.J.Wang,M.H.Patel,A.J.Schueth,M.Bradley,S.Wu,J.C. Crosson,P.A.Glassman,D.S.Bell,Perceptionsof standards-basedelectronicprescribingsystemsas
implementedinoutpatientprimarycare:aphysiciansurvey, J.Am.Med.Inform.Assoc.16(4)(2009)493–502.
[18] T.L.Warholak,M.T.Rupp,Analysisofcommunitychain pharmacists’interventionsonelectronicprescriptions,J. Am.Pharm.Assoc.49(1)(2009)59–64.
international journal of medical informatics 82 (2013)473–491
491
[19] S.N.Weingart,M.Massagli,A.Cyrulik,T.Isaac,L.Morway, D.Z.Sands,J.S.Weissman,Assessingthevalueofelectronic prescribinginambulatorycare:afocusgroupstudy,Int.J. Med.Inform.78(9)(2009)571–578.
[20] B.Astrand,E.Montelius,G.Petersson,A.Ekedahl,
AssessmentofePrescriptionquality:anobservationalstudy atthreemail-orderpharmacies,BMCMed.Inform.Decision Making9(2009)8.
[21] F.Ax,A.Ekedahl,Electronicallytransmittedprescriptions notpickedupatpharmaciesinSweden,Res.SocialAdm. Pharm.6(1)(2010)70–77.
[22] A.Ekedahl,N.Mansson,Unclaimedprescriptionsafter automatedprescriptiontransmittalstopharmacies,Pharm. WorldSci.26(1)(2004)26–31.
[23] A.Ekedahl,A.Wessling,A.Melanderr,Primary
non-compliancewithautomatedprescriptiontransmittals fromhealthcarecentresinSweden,J.SocialAdmin.Pharm. 19(4)(2002)137–140.
[24] L.Hellstrom,K.Waern,E.Montelius,B.Astrand,T.Rydberg, G.Petersson,Physicians’attitudestowards
ePrescribing—evaluationofaSwedishfull-scale implementation,BMCMed.Inform.DecisionMaking9 (2009)37.
[25] A.Motulsky,N.Winslade,R.Tamblyn,C.Sicotte,Theimpact ofelectronicprescribingontheprofessionalizationof communitypharmacists:aqualitativestudyofpharmacists’ perception,J.Pharm.Pharm.Sci.11(1)(2008)
131–146.
[26] B.Sugden,R.Wilson,Integratedcareandelectronic transmissionofprescriptions:experienceoftheevaluation ofETPpilots,HealthInform.J.10(4)(2004)277–290. [27] W.J.vanderKam,B.MeyboomdeJong,T.Tromp,P.W.
Moorman,J.vanderLei,Effectsofelectronic
communicationbetweentheGPandthepharmacist,the qualityofmedicationdataonadmissionandafter discharge,Fam.Pract.18(6)(2001)605–609.
[28] D.Kinnaird,T.Cox,J.P.Wilson,Unclaimedprescriptionsina clinicwithcomputerizedprescriberorderentry,Am.J. Health.Syst.Pharm.60(14)(2003)1468–1470.
[29] W.S.Tan,J.S.Phang,L.K.Tan,W.S.Tan,J.S.Phang,L.K.Tan, Evaluatingusersatisfactionwithanelectronicprescription systeminaprimarycaregroup,Ann.Acad.Med.Singapore 38(6)(2009)494–497.
[30] Z.Niazkhani,H.Pirnejad,M.Berg,J.Aarts,Theimpactof computerizedproviderorderentrysystemsoninpatient clinicalworkflow:aliteraturereview,J.Am.Med.Inform. Assoc.16(4)(2009)539–549.
[31] L.Poissant,J.Pereira,R.Tamblyn,Y.Kawasumi,Theimpact ofelectronichealthrecordsontimeefficiencyofphysicians andnurses:asystematicreview,J.Am.Med.Inform.Assoc. 12(5)(2005)505–516.
[32] A.Schedlbauer,V.Prasad,C.Mulvaney,S.Phansalkar,W. Stanton,D.W.Bates,A.J.Avery,Whatevidencesupportsthe useofcomputerizedalertsandpromptstoimprove clinicians’prescribingbehavior?J.Am.Med.Inform.Assoc. 16(4)(2009)531–538.
[33] C.Estellat,I.Colombet,S.Vautier,J.Huault-Quentel,P. Durieux,B.Sabatier,Impactofpharmacyvalidationina computerizedphysicianorderentrycontext,Int.J.Qual. HealthCare19(5)(2007)317–325.
[34] C.C.Inquilla,S.Szeinbach,E.Seoane-Vazquez,K.H. Kappeler,Pharmacists’perceptionsofcomputerized prescriber-order-entrysystems,Am.J.Health.Syst.Pharm. 64(15)(2007)1626–1632.
[35] A.S.Gadkari,C.A.McHorney,Medicationnonfulfillment ratesandreasons:narrativesystematicreview,Curr.Med. Res.Opin.26(3)(2010)683–705.
[36] B.Chaudhry,J.Wang,S.Wu,M.Maglione,W.Mojica,E.Roth, S.C.Morton,P.G.Shekelle,Systematicreview:impactof healthinformationtechnologyonquality,efficiency,and costsofmedicalcare,Ann.Intern.Med.144(2006)E12–E22. [37] M.T.Rupp,T.L.Warholak,M.T.Rupp,T.L.Warholak,
Evaluationofe-prescribinginchaincommunitypharmacy: best-practicerecommendations,J.Am.Pharm.Assoc.48(3) (2008)364–370.