Comprehensive Journal of Educational Research Vol. 1(1), pp. 1 - 8, May. 2013 Copyright © 2013 Knowledgebase Publishers.
Research Article
Athletic training education program directors’ and
athletic trainers’ perceptions of the psychosocial
intervention and referral competencies
*Brian D. Seiler
1, Noah B. Gentner
2, Susan P. Wehring
3and A. Barry Joyner
4,
1
ATC, University of South Carolina,1Blatt Physical Education Center – 202E,University of South Carolina,1300 Wheat Street, Columbia, SC 29208
2
Humber College,205 Humber College Blvd.Toronto, ON M9W5L7
3
ATC, Southeast Missouri State University, One University Plaza,Cape Girardeau, Missouri 63701
4
Georgia Southern University, Post Office Box 8067, Statesboro, Georgia 30460-8076
*Corresponding Author Email: [email protected], Phone: (803) 348-1067, Fax: (803) 777-6250
ABSTRACT
Education of the psychosocial content is mandated within all athletic training education programs. Previous research has evaluated educators’ confidence in students’ abilities, students’ perceptions, and athletic trainers’ satisfaction within this content area. This study explored program directors’ and athletic trainers’ perceptions of the importance, criticality and preparedness of the psychosocial competencies. A convenience-sample of non-collegiate, NAIA, and NCAA athletic trainers (n=88; RR=8.8%) and program directors (n=53; RR=15.4%) completed the Athletic Training Education Competency Questionnaire (ATECQ), a web-based survey replicating the Board of Certification’s content evaluation. A pilot study determined content-related and face-validity of the ATECQ (α=0.933). One-tailed independent t-tests evaluated the importance, criticality, and preparedness of each psychosocial competency. Athletic trainers’ and program directors’ perceptions of the psychosocial competencies did not differ (P≤0.0147). However, program directors rated the roles/function of
community based healthcare providers (P=0.008), signs/symptoms of eating disorders (P=0.01) and basic counseling principles (P=0.015) as more important than athletic trainers, as well as signs/symptoms of mental/emotional disorders as more prepared than athletic trainers (P=0.016). Though the sample size is limited, the psychosocial content area was ranked in the lower 25%, indicating that the participants may not perceive psychosocial concerns as important or critical as other athletic training content areas.
Key Words: psychological skills, sport psychology, instruction, competencies
INTRODUCTION
Undergraduate athletic training education programs have been competency based since their early development,
coinciding with the National Athletic Trainers’ Association Athletic Training Educational Competencies manual and
standards of care set by the Board of Certification. Current with the newest edition of this manual (5th Ed.), all entry-level athletic trainers graduating from an accredited program must demonstrate proficiency and competence in eight specific content areas. This manual further dictates the minimum amount of knowledge and skills that are essential for a students’ professional education in athletic training (NATA 2011). Entry-level athletic trainers are acknowledged to have mastered the competencies within this manual upon passing the national Board of Certification examination. In this context, becoming proficient, or, in other words, mastering these competencies, is the ability to perform with “expert correctness and facility” (NATA 2011, p. 4). However, perceptions from anecdotal evidence suggest that the educational competencies are emphasized to varying degrees, even when minimum requirements have been established for today’s entry-level practitioner.
The Psychosocial Intervention and Referral content area contained within this manual, which has recently been renamed to Psychosocial Strategies and Referral in the fifth edition of the educational competencies (2011), is one that the National Athletic Trainers’ Association dictates its inclusion within all accredited programs. This area includes recognizing and having the ability to intervene and refer clients/patients exhibiting abnormal mental health behaviors (NATA 2011). Currently, accredited academic programs do not require a detailed psychosocial course despite the competency requirements posed by the National Athletic Trainers’ Association (Stiller-Ostrowski et al. 2009a). This allows for individual program interpretation and flexibility in how to address these required standards of practice.
Due to the nature of the athletic training profession, most athletic trainers are predominantly concerned with the physical characteristics of injuries and illnesses, even though they are also coupled with psychological components. Often times, the psychological aspects have just as much impact during the injury process (Williams et al. 2006; Wiese et al. 1991). Although most patients have shown to be physically ready to return to sport, it has been determined they may not be psychologically prepared (Ford et al. 1994). Such research suggests that patients may benefit from athletic trainers’ increased education and incorporation of psychological skills into the rehabilitation process. Even with improvements and an increase in the standards of practice in athletic training, the knowledge and skills within the psychosocial content area appear to be continually overlooked in academic preparation and are often not incorporated into patients’ rehabilitation programs (Larson et al. 1996; Washington-Lofgren et al. 2004).
Most, if not all, healthcare providers recognize the importance of treating the psychological factors associated with injury (Wiese et al. 1991; Arvinen-Barrow et al. 2007). However, many are reluctant to address the psychological dynamics during treatment, potentially
Brian et al 2
hindering the athlete’s recovery process. A lack of education and, more importantly, the need to educate athletic trainers on the use of psychosocial strategies in clinical practice has been previously illustrated (Stiller-Ostrowski et al. 2009a; Wiese et al. 1991; Arvinen-Barrow et al. 2007). To that end, a substantial amount of athletic trainers have stated a desire for increased preparation attributable to feeling inadequately trained in the psychological aspects of injury leading to the belief that they are unable to fully assist their patients with their recovery (Washington-Lofgren et al. 2004).
Previous research has provided information regarding athletic trainers’ educational satisfaction with and technique use within the psychosocial content area (Thomas et al. 2008), athletic trainers’ perceptions of the effectiveness of psychological skills (Hamson-Utley et al. 208), entry-level athletic trainers’ preparation in the psychosocial content area (Stiller-Ostrowski et al. 2009b; Kamphoff et al. 2010), and athletic trainers’ perceptions and attitudes toward a course addressing psychological issues (Harris et al. 2005). Additional unpublished data by Hamson-Utley and Stiller-Ostrowski surveyed program directors and asked them to rank the instructional emphasis placed on each content area. However, no research to our knowledge has systematically examined program directors’ perceptions of the psychosocial competencies in relation to athletic trainers’ perceptions. It stands to reason that if athletic trainers perceive the psychosocial content area to be important and critical, they would want to be more prepared and inclined to advocate the use of these psychological strategies with their clients. Therefore, the purpose of this study was to examine program directors’ and athletic trainers’ perceptions of the psychosocial competencies in terms of three variables stemming from the Board of Certification’s Role Delineation Study: (1) importance, (2) criticality, and (3) preparedness. We were also interested in where the psychosocial content area was ranked in relation to the other content areas according to these same variables.
METHODS
Participants
An e-mail request was developed by the researchers and reviewed by the National Athletic Trainers’ Association Ethics Committee to send to the potential participants. The potential respondents were contacted by e-mail at the start of the data collection time period, and were also sent a follow-up e-mail to remind them to complete the questionnaire. All potential respondents were promised confidentiality regarding their participation and responses. The project was approved by the institutional review board of the host university, and all participants gave written consent. The survey was conducted over a span of three months.
Athletic trainers were recruited through the National Athletic Trainers’ Association contact list request form. Inclusion criteria consisted of those members of the National Athletic Trainers’
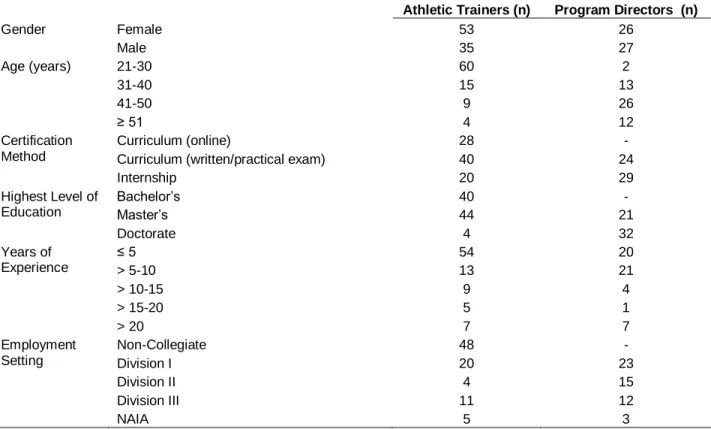
Table 1. Participant Demographics
Athletic Trainers (n) Program Directors (n)
Gender Female Male 53 35 26 27 Age (years) 21-30 31-40 41-50 ≥ 51 60 15 9 4 2 13 26 12 Certification Method Curriculum (online)
Curriculum (written/practical exam) Internship 28 40 20 - 24 29 Highest Level of Education Bachelor’s Master’s Doctorate 40 44 4 - 21 32 Years of Experience ≤ 5 > 5-10 > 10-15 > 15-20 > 20 54 13 9 5 7 20 21 4 1 7 Employment Setting Non-Collegiate Division I Division II Division III NAIA 48 20 4 11 5 - 23 15 12 3 Note: Athletic trainers (n = 88); Program directors (n = 53).
Note: In reference to the initial set of requests sent, the total samples for each participant group is small attributable to the low response rate
Association that were currently certified from all districts within the United States and working in the college/university, secondary school or clinic settings (N = 1000). Recruited program directors included those individuals holding this position according to the Commission on Accreditation of Athletic Training Education website (N = 345). Of the requests sent, an exceptionally undersized response rate of 10.5% was recorded in relation to the number of potential participants. Not all participants responded to every question or provided valid responses; thus, these participants were not included in the final analysis.
Of the 1000 athletic trainers who received our request to participate in the research study, 88 athletic trainers fully completed the questionnaire (8.8% response rate). Our sample of athletic trainers covered a wide range of employment settings including graduate assistants (n = 6, 6.8%), high schools (n = 21, 23.9%), high schools/clinics (n = 21, 23.9%), junior colleges (n = 6, 38.6%), and four year colleges/universities (n = 34, 38.6%). Of the individuals that responded, 83% (n = 73) indicated that they felt responsible/accountable for treating the psychosocial aspects affecting patients in their daily practice.
Of the 345 program directors who received our request to complete the study, 53 program directors responded (15.4% response rate). Our sample of program directors’ employment settings included NCAA Division I institutions (n = 23, 28.3%), NCAA Division II institutions (n = 15, 28.3%), NCAA Division III institutions (n = 12, 22.6%), and NAIA institutions (n = 3, 5.7%). In addition, only 22 (41%) of these participants indicated that
their program required undergraduate students to complete a psychosocial course related to aspects in athletic training. (See Table 1 for additional participant demographic information)
Instrument
Athletic Training Education Competency Questionnaire (ATECQ): The ATECQ was developed for the purpose of this study to examine the participants’ perceptions of the importance, criticality, and preparedness of the psychosocial competencies. The instrument was modeled and structured after the fourth edition of the Board of Certification Role Delineation Study and was designed to contain three valid scales that were appropriate to assess the educational competencies in athletic training. Two of the variables previously defined by the Board of Certification, importance (α > 0.7) and criticality (α > 0.7), were employed and a third complimentary importance, preparedness, was included. (See Table 2 for definitions of variables)
Comprised of two sections, the ATECQ was developed to specifically assess the educational competencies, as well as to determine how athletic trainers and program directors rank the educational content areas. Specifically, the psychosocial competencies were addressed in this study, but the ATECQ can be modified to use with the other content areas. Accordingly, each of the fifteen psychosocial competencies were rated according to the importance, criticality, and preparedness
Brian et al 4
Table 2. Definitions of Instrument Variables
Variable Description
Importance Importance is deemed as the degree to which knowledge and competence in the content area/competency is essential to the job performance of a minimally competent athletic trainer. Participants will indicate how important each content area/competency is to the performance of a minimally competent athletic trainer.
Criticality Criticality is defined as the degree to which adverse effects could result if the athletic trainer is not competent in a content area/competency. Participants will indicate how critical to which the inability to perform tasks within each content area/competency would be seen as causing harm to a client, co-worker, the public, the environment, etc. Harm may be physical, emotional, financial, etc.
Preparedness Preparedness is defined as the degree to which a minimally competent athletic trainer perceives to be prepared in each educational content area/competency. Participants will indicate the amount of preparation in which they perceive their athletic training education program provides/provided them in each educational content area/competency to be a minimally competent athletic trainer.
Table 3. Rank of Athletic Training Educational Content Areas
Importance Criticality Preparedness Athletic Trainers Program Directors Athletic Trainers Program Directors Athletic Trainers Program Directors RM 3 3 3 3 3 3 PA 5 4 4/5 7 4 4 DI 2 2 2 2 2 1 MC 7 6 4/5 4 7 7 AC 1 1 1 1 1 2 TM 8 7 7 6 6 6 EX 6 5 6 5 5 5 PH 12 10 8 8 12 10/11 PS 9 9 9 9 10 12 NU 10 8 10 10 9 8 AD 11 11 12 11 11 10/11 PD 4 12 11 12 8 9
Note: Rank was determined by ordering the overall mean from least to greatest for each content area.
Note: RM (Risk Management and Injury Prevention), PA (Pathology of Injuries and Illnesses), DI (Orthopedic Clinical Examination and Diagnosis), MC (Medical Conditions and Disabilities), AC (Acute Care of Injuries and Illnesses), TM
(Therapeutic Modalities), EX (Conditioning and Rehabilitative Exercise), PH (Pharmacology), PS (Psychosocial Intervention and Referral), NU (Nutritional Aspects of Injuries and Illnesses), AD (Health Care Administration), PD
(Professional Development and Responsibility) (NATA, 2006).
variables using a four-point Likert-scale (0 = lowest rating; 3 = highest rating). For example, one of the items in the questionnaire asked the participants to rate how important they perceived the competency of describing basic principles of mental preparation, relaxation, visualization, and desensitization techniques to be. Item stems and Likert-scale anchors, according to the Board of Certification Role Delineation Study (2010), remained unchanged. In addition, the educational content areas were rank ordered according to these same variables (1 = lowest rank; 12 = highest rank). The survey also included a number of questions about the participant’s practice settings, work experiences, and demographics. The entire survey was conducted online (http://www.surveymonkey.com) and took approximately 20 minutes to complete.
An initial pilot study was completed using non-probability
sampling with a specific convenience sample of athletic trainers (n = 9) and kinesiology professors (n = 2) to determine the content-related and face-validity of the ATECQ. This sample was instructed to provide feedback and comments concerning the content and clarity of the questionnaire. Only slight changes to the variable definitions and questionnaire directions for clarity were indicated, allowing for the initial structure of the questionnaire to remain intact. In addition, a reliability check of the ATECQ presented a Cronbach’s alpha of 0.933 (α = 0.929 with item deletion) indicating that the questionnaire was reliable.
Data Analysis
(version 17.0; SPSS Inc, Chicago, IL) to generate descriptive statistics for each survey question and to evaluate group differences (athletic trainers vs. program directors) in importance, criticality, and preparedness of the psychosocial competencies. One-tailed independent t-tests were employed to determine differences among athletic trainers and program directors according to each variable. Additional t-tests were completed to determine variation across athletic trainers and program directors in how they rated the individual psychosocial competencies. Before completing these analyses a Bonferroni adjustment was performed to decrease the likelihood of making a Type I error, setting the significance level at a more conservative level (α = 0.017). Frequency statistics were also calculated to determine the ranking of the educational content areas regarding their importance, criticality, and preparedness.
RESULTS
Examination of the overall mean ratings of the psychosocial competencies indicated that there were no significant differences across the importance (P = 0.14), criticality (P = 0.38), or preparedness (P = 0.38) variables. In addition, t-tests for equality of means showed no differences between program directors’ and athletic trainers’ perceptions in how they rated the importance, criticality, or preparedness of the psychosocial competencies.
More specifically, analyses treating each psychosocial competency as a single-item were completed. These analyses indicated that the importance of identifying the signs and symptoms of common eating disorders was rated higher by program directors (2.62 ± 0.56) than athletic trainers (2.38 ± 0.63) (P = 0.01). In addition, program directors perceived the importance of describing the roles of and proper referral to other healthcare providers (e.g., psychologists and counselors) (program directors = 1.98 ± 0.80, athletic trainers = 1.65 ± 0.77, P = 0.008), and explaining basic counseling principles (program directors = 2.09 ± 0.77, athletic trainers = 1.83 ± 0.65, P = 0.015) higher than athletic trainers. Finally, the preparedness of describing signs and symptoms of mental and emotional disorders, and personal/social conflict was perceived higher by program directors (1.64 ± 0.86) than athletic trainers (1.30 ± 0.95) (P = 0.016). When asked to rank the content areas in terms of importance, criticality, and preparedness, acute care of injuries and illnesses, orthopedic clinical examination and diagnosis, and risk management and injury prevention were ranked as the top three educational content areas. Overall, the psychosocial content area was ranked in the lower 25% of the content areas for all three variables. Specifically, program directors ranked the psychosocial content area ninth for importance and criticality, and twelfth for preparedness. Similar results were obtained with athletic trainers ranking the psychosocial content area eighth for importance, ninth for criticality, and tenth for preparedness. (See Table 3 for the complete rankings of the content areas)
DISCUSSION
The purpose of this investigation was to examine program directors’ and athletic trainers’ perceptions of the importance, criticality and preparedness of the psychosocial competencies in athletic training. Additionally, identification of the rankings of the athletic training educational content areas using the same variables was assessed. These aims are aligned with the understanding that all athletic training educational content areas are established to fulfill the knowledge and skill requirements necessary to perform tasks safely and competently as an entry-level athletic trainer (Board of Certification 2004, 2010). In general, this sample of athletic trainers’ and program directors’ equally perceive the importance, criticality, and preparedness of the psychosocial content area as relatively low. In addition, regardless of the type of institution, level of education, experience, or certification method participants agreed that the psychosocial content area is not perceived as highly relative to other content areas (e.g., Acute Care of Injuries and Illnesses, and Orthopedic Clinical Examination and Diagnosis).
Unlike previous research that isolated the psychosocial content area to evaluate, this study examined participants’ perceptions of the psychosocial content area relative to others. Contradictory to previous reports indicating that athletic trainers hold positive attitudes on the effectiveness and importance of psychological skills, (Wiese et al. 1991; Arvinen-Barrow et al. 2007; Hamson-Utley et al. 2008; Kamphoff et al. 2010) our results suggest decreased perceptions of the psychosocial content area. These perceptions may simply be a reflection of how the participants perceive the content area when compared to others and not an indication of their general feelings toward the psychosocial content area. However, the discrepancy between the present responses and those from previous research indicates that the value of the psychosocial competencies may have further decreased.
On the other hand, the results of this study are comparable to those reported by Stiller-Ostrowski and Ostrowski’s focus group interview study (2009b) in which they showed that recently certified athletic trainers reported being less proficient and knowledgeable about the psychosocial competencies. It is important to note that the reported means for preparedness of the psychosocial content area resembled personal reports of athletic trainers and were apparently lower compared to the other content areas. This suggests that both athletic trainers and program directors may not have as positive of perceptions of the psychosocial content area when evaluated among the other content areas. It also proposes that accredited athletic training programs may not be providing entry-level athletic trainers with an adequate amount of information regarding how to deal with patient-related issues in the areas of motivation and adherence, counseling and social support, mental skills
training, and potential psychosocial referral situations that can be used in their profession, which was also previously found by Stiller-Ostrowski and Ostrowski (2008b).
In addition, the present results contradict Kamphoff et al.’s (2010) findings in that athletic training students exhibited positive perceptions of psychological skills. Presently, we found that perceptions of the competencies were lower, although not necessarily negative, for all variables examined. This is surprising given that we expected participants’ perceptions to be comparable to previous literature. This finding may be due to differences between the education level and experience of the present study’s sample and the student sample included in the study completed by Kamphoff et al. (2010). Nevertheless, some semblance in responses was anticipated complementing previous research findings. Furthermore, it is likely that experienced athletic trainers, compared to students, have formed individual perceptions of what they perceive is necessary to practice as a competent athletic trainer.
An area of concern is how program directors and athletic trainers ranked the psychosocial content area compared to the other educational content areas. Our findings are similar to research by Hamson-Utley and Stiller-Ostrowski (under review) indicating that both athletic trainers and program directors ranked the psychosocial content area in the lower quarter for importance, criticality, and preparedness. When examining all content area rankings, we find that the data clearly show the perceived criticality, importance and preparation of injury recognition and emergency management (e.g. Acute Care of Injuries and Illnesses, Orthopedic Clinical Examination and Diagnosis, and Risk Management and Injury Prevention), with the psychosocial aspects well toward the bottom. This would suggest that the amount of time spent in the presentation of material relating to these areas would follow suit. Despite this, athletic training education programs are designed to follow a set of standards to thoroughly include each content area without placing an emphasis on any one particular content area. Therefore, the time spent in the presentation of material should be similar, reflecting the competencies within each content area. As this is the first study to examine the psychosocial content area, according to importance, criticality and preparedness, together with the other content areas in a ranking fashion, it is hard to conclude if it extends previous literature. However, we hypothesize that there is a relationship that exists between athletic trainers in the present study ranking the psychosocial content area relatively low and students in previous studies that do not feel prepared to implement psychological skills (Hamson-Utley et al. 2008; Stiller-Ostrowski et al. 2009b; Kamphoff et al. 2010). Of additional concern, barely half of program directors indicated that they required undergraduate
Brian et al 6
students to complete a course specifically in the psychosocial aspects in athletic training. Previous studies have reported similar findings that roughly half of surveyed undergraduate students and entry-level athletic trainers completed a course in sport psychology (Larson et al. 1996; Hamson-Utley et al. 2008; Hamson-Utley et al. under review). This is concerning since athletic trainers continually report that they do not feel comfortable or confident (Cramer Roh et al. 2000) as well as underprepared (Stiller-Ostrowski et al. 2009) and inadequately trained (Gordon et al. 1991) in the psychological aspects of injury. Due to these perceptions it is not unexpected that athletic trainers and program directors currently perceive the psychosocial content area lacking importance and criticality, possible leading to decreased preparation. Even if a specific course in sport psychology is not required or this content area is incorporated into one or several other courses, these results suggest that many programs still may not effectively incorporate this content area into their curriculum. Overall, this is alarming given that research regarding the education and training of the psychosocial content in athletic training has repetitively exhibited similar findings.
The benefits of including psychological skills in athletic training practice have been recognized across multiple studies (Weise et al. 1991; Hamson-Utley et al. 2008; Harris et al. 2005; Cramer Roh et al. 2000); however, formal education is limited (Thomas et al. 2008). The traditional sport psychology course may not address the use of sport psychology skills with injured patients and how to handle psychosocial problems. Adding to this, studies by Weise et al. (1991) and Kamphoff et al. (2010) stated that faculty who are instructing athletic training students are unfamiliar with the psychosocial content, lack formal training in this area, and have decreased confidence in implementing these skills. Therefore, it is recommended that instructors who are familiar with and have adequate knowledge in the implementation of psychological skills in clinical practice be used, which may include instructors outside of the athletic training program. It is encouraging, however, that in this study and in previous research (Lafferty et al. 2008) athletic trainers indicated that they felt responsible and/or accountable for treating the psychosocial aspects affecting patients as well as indicating a strong interest in learning psychological skills (Kampoff et al. 2010).
This study was exploratory in nature and designed to provide an initial understanding of program directors’ and athletic trainers’ perceptions of the importance, criticality, and preparedness using the definitions of these factors proposed by the Board of Certification. Although all athletic training education programs follow the same set of educational guidelines, the results of this study are exceedingly limited due to the low response rate. As a result, interpretation of the data may not indicate the true perceptions of athletic trainers and program directors,
and inferences to the broader population of athletic trainers may not be accurate. Therefore, review of the format and content of the questionnaire may be necessary to have fewer and more direct questions allowing for an increased response rate allowing for the generalization of the results. In addition, the accumulated responses of the athletic trainers in this study may not match with the program directors as these individuals may not be preceptors. By completing an additional study matching program directors with preceptors at a few randomized athletic training education programs, based on division or number of years accredited, there may be a better connection than program directors and random athletic trainers. Furthermore, the authors chose to analyze the current data with independent t-tests with an adjusted P-level using the Bonferroni adjustment. Instead, it may have been more appropriate to use one-way analyses of variance for each of the variables. Using this analysis in its place may provide more direct and interpretable results. Lastly, since a newer edition of the educational competencies (5th Ed.) was recently published, the current results do not address this version of the competencies. Even so, the information gained from this study complements current literature and helps direct and indicate a need for future research.
Since the ATECQ was the first to apply the definitions established by the Board of Certification (importance and criticality, with an additional factor, preparedness, developed according to these definitions), future research could be done to include these definitions to compliment and expand the results of this study as well as the work by Stiller Ostrowski and Ostrowski (2009b) and Kamphoff et al. (2010). As this study was not part of a larger study addressing all educational competencies, future research could examine all content areas in a similar fashion, especially those receiving lower reported perceptions in this study (e.g., Nutritional Aspects of Injuries and Illnesses, Pharmacology, and Health Care Administration). This information would be particularly important to close the gap between the didactic learning presented in the classroom setting compared to what is used in clinical practice.
Additionally, qualitative and additional quantitative approaches could also be used to examine the pedagogical effectiveness in teaching the psychosocial content area. Currently, accredited programs are providing education in most psychosocial competencies; however, athletic trainers still do not implement them in clinical practice (Hamson-Utley et al. under review). Preliminary research by Thomas, Torres-McGehee and Monsma (2008) found that most athletic trainers learned techniques through hands-on experiences or observation. A better understanding of how the psychosocial content is presently delivered and assessed is particularly important in order to implement the most effective teaching strategies.
CONCLUSIONS
Psychological effects have been found to occur and greatly influence all aspects of sport. Our findings, although based on the perceptions of a small sample who responded, highlight athletic trainers’ and program directors’ decreased perceptions of the importance and criticality of the psychosocial content area which may lead to an athletic trainer’s lack of preparation. Even though we cannot automatically generalize our findings to the broader population, initial attention appears to be needed in regard to the effectiveness of athletic training education program faculty in the instruction of the psychosocial content. It would be worthwhile; therefore, to adjunct those with a background in sport psychology to instruct students in the psychosocial aspects of sport. This will help place instructional importance on the psychosocial competencies as outlined by the athletic training educational competencies manual.
Injuries tend to have both physical and psychological components. Though somewhat outdate, but still central to the issue at hand, research by Wiese, Weiss and Yukelson (1991) stressed that psychological rehabilitation from injury is, just as, if not more important than the physical rehabilitation process. This concept is apparent in the present holistic framework of rehabilitation practice that includes both physical and mental treatments (Sordoni et al. 2002). For this to occur, a students’ understanding of the psychological aspects of injury should be increased. In addition, further preparation of how students can implement psychological skills should be addressed in respect to the benefits these skills can have in the clinical setting. Due to the small sample size, this study provides preliminary evidence implying that if program directors and athletic trainers do not perceive the psychosocial content as important and critical, it is less likely that time is spent preparing students in these competencies (Thomas et al. 2008; Stiller-Ostrowski et al. 2009b; Kamphoff et al. 2010; Harris et al. 2005). We recommend that the importance and criticality of these skills be stressed to faculty and athletic trainers to increase their understanding and perceptions of the psychosocial competencies with the hope of creating a “domino effect” within their instructional practice.
REFERENCES
Arvinen-Barrow M, Hemmings B, Weigand D, Becker C & Booth L. (2007). Views of chartered physiotherapists on the psych content of their practice: A follow-up survey in the UK. J. of
Sport Rehab. 16(2), pp 111-121.
Board of Certification. (2004). Role delineation study: For the
entry-level certified athlet trainer (5th ed.). Omaha, NE:
National Athlet Trainers’ Association Board of Certification. Board of Certification. (2010). Athletic trainer role
delineation/practice analysis study for the entry-level certified
Cramer Roh JL & Perna FM. (2000). Psych/counseling: A universal competency in athlet trainer. J. of Athlet. Training, 35(4), pp 458-465.
Evans L, Hare R & Mullen R (2006). Imagery use during rehab from injury. J. of Imagery Res. in Sport and Phys. Act. 1(1) 1-19.
Ford IW & Gordon S (1994). Perspectives on the psych curricula in professional training programs of sport physiotherapists and sport/athlete trainers: A cross-cultural
survey. Presentation at the annual meeting of the Association
for Applied Sport Psych, Lake Tahoe, CA.
Gordon S, Milios D & Grove JR. (1991). Psychological aspects of the recovery process from sport injury: The perspective of sport physiotherapists. The Aust. J. Sci. and Med. in Sport, 23(2) 53-66.
Hamson-Utley JJ, Martin S & Walters J. (2008). Athlet trainers’ and phys therapists’ perceptions of the effectiveness of psych skills within sport injury rehab programs. J. of Athlet Training, 43(3), 258-264.
Harris LL, Demb A & Pastore DL. (2005). Perceptions and attitudes of athlet training students toward a course addressing psych issues in rehab. J. of Allied Health, 34(2), 101-109.
Kamphoff CS, Hamson-Utley JJ, Antoine B, Knutson R, Thomae J & Hoenig C. (2010). Athleti training students’ perceptions of and academic preparation in the use of psych skills in sport injury rehab. Athlet Training Educ J., 5(3), 109-116.
Lafferty ME, Kenyon R & Wright CJ. (2008). Club-based and non-club-based physiotherapists’ views on the psych content of their practice when treating sports injuries. Res in Sports
Med, 16, 295-306.
Larson GA, Starkey C & Zaichkowsky LD. (1996). Psych aspects of athletic injuries as perceived by athletic trainers.
The Sport Psychol, 10(1), 37-47.
National Athletic Trainers’ Assoc (2006). Athlet training educ
competencies (4th ed.). Dallas, TX: National Athletic Trainers’
Assoc.
Brian et al 8
National Athlet Trainers’ Assoc (2011). Athletic training educ
competencies (5th ed.). Dallas, TX: National Athlet Trainers’
Assoc.
Sordoni C, Hall C & Forwell L. (2002). The use of imagery in athlet injury rehab and its relationship to self-efficacy.
Physiother Canada, 54(3), 177-185.
Stiller-Ostrowski JL, Gould DR & Covassin T. (2009a). An evaluation of an educ intervention in psych of injury for athlet training students. J. of Athlet Training, 44(5), 482-489. Stiller-Ostrowski JL & Ostrowski JA. (2009b). Recently certified
athlet trainers’ undergraduate educ preparation in psychosocial intervention and referral. J. of Athletic Training, 44(1), 67-75.
Thomas EH, Torres-McGehee TM, Monsma E. (2008). Athlet trainers’ use of sport psych techniques in clinical practice. J.
of Athlet Training, 43(3), S-36.
Washington-Lofgren L, Westerman BJ, Sullivan PA & Nashman HW. (2004). The role of the athlet trainer in the post-injury psych recovery of collegiate athlet. Int Sports J. 8(2), 94-104. Wiese DM, Weiss MR & Yukelson DP (1991). Sport psych in
the training room: A survey of athlet trainers. The Sport
Psychol, 5, 15-24.
Williams JM & Scherzer CB. (2006). Injury risk and rehab: Psych considerations. In J. M. Williams (Eds.), Applied Sport
Psych: Personal Growth to Peak Performance (565-587).