Reducing Immunization Discomfort in 4- to
6-Year-Old Children: A Randomized Clinical Trial
WHAT’S KNOWN ON THIS SUBJECT: A variety of mechanical, pharmacologic, and distraction techniques have each been shown to play a role in the reduction of immunization injection
discomfort.
WHAT THIS STUDY ADDS: This randomized clinical trial evaluates a unique approach that combines verbal suggestions of
diminished sensation, a visual focusing activity, and a topical analgesic spray to diminish injection discomfort in 4- to 6-year-old children.
abstract
OBJECTIVE:The goal was to test a multifaceted distraction method designed to reduce injection-associated pain in school-aged children.
METHODS:A clinical trial evaluated 41 children, 4 to 6 years of age, who were given 3 standard prekindergarten immunizations; 21 were as-signed randomly to an office routine control group, whereas 20 re-ceived a multifaceted, discomfort-reducing intervention. The interven-tion added verbal suggesinterven-tions of diminished sensainterven-tion and a visual focusing activity to the use of ethyl chloride, an established pain-reducing measure. The distraction materials used for the intervention consisted of topical ethyl chloride spray, an improvised, plastic, multi-pronged arm gripper, and a vibrating instrument descending on the contralateral arm, which provided the focusing task and visual distraction.
RESULTS:According to patient and parent Faces Pain Scale-Revised scores and nonblinded, video-taped observations scored according to the face-legs-activity-crying-consolability method, the intervention group showed highly significant reductions in pain and discomfort, compared with the control group (patient self-report,P⬍.0013; par-ent report,P⬍.0002; observation score,P⬍.0001).
CONCLUSION:This multifaceted distraction intervention reduced sig-nificantly the pain and discomfort of childhood immunizations in chil-dren 4 to 6 years of age.Pediatrics2009;124:e203–e209
CONTRIBUTORS:F. Ralph Berberich, MD, and Zachary Landman, BA
Pediatric Medical Group, Berkeley, California KEY WORDS
distraction, hypnosis, injections, immunization, pain, anxiety
ABBREVIATIONS
FPS-R—Faces Pain Scale-Revised
FLACC—face-legs-activity-crying-consolability MMR—measles-mumps-rubella
Address correspondence to F. Ralph Berberich, MD, Pediatric Medical Group, 2320 Woolsey St, Suite 301, Berkeley, CA 94705. E-mail: [email protected]
www.pediatrics.org/cgi/doi/10.1542/peds.2007-3466
doi:10.1542/peds.2007-3466
Accepted for publication Mar 12, 2009
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2009 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE:The authors have indicated they have no financial relationships relevant to this article to disclose.
tizer, and diminish patient rapport and parental compliance.1–5Children who
are about to enter kindergarten may exhibit marked anticipatory anxiety about injections, having retained cu-mulative memories of numerous pain-ful experiences.2 The relative
contri-butions of pure sensory pain and anticipatory anxiety are influenced by age and gender differences, stage of development, temperament, parental behavior, and cultural expectations.6–9
It should come as no surprise that, af-ter⬎20 separate immunization injec-tions, preschool-aged and older chil-dren greet us more frequently with “do I have to get a shot?” than with “hi, doctor.”7
Reviews by Schechter et al4,5 and by
Reis et al7 discussed different
ap-proaches to counter injection pain. Some techniques are mechanical (eg, use of proper needle bore and length), others are pharmacologic (eg, use of lidocaine-prilocaine or ethyl chloride), and yet others are behavioral. Blowing bubbles or pinwheels has been associ-ated with reduced injection discom-fort.10,11 Uman et al1 published an
ex-tensive review of randomized, clinical trials addressing psychological ap-proaches and concluded that, among behavioral modalities, only distrac-tion, hypnosis, and combinations of the 2 are effective in reducing self-reported pain or distress.
We hypothesized that we might achieve maximal diminution of injection pain by combining modalities, adding ver-bal suggestions of diminished sensa-tion to a visual gaze-fixing task, topical ethyl chloride, and another kinesthetic distracter. This constitutes the first randomized, clinical trial of this unique combination of several distinct dis-traction interventions, evaluated by both subjective and objective pain scales and compared to an office
rou-METHODS
Subjects
The research committee and institu-tional review board of Children’s Hos-pital Oakland (Oakland, CA) approved the study. Subjects were recruited prospectively from the patient popu-lation at the Pediatric Medical Group (Berkeley, CA) and were enrolled be-tween the middle of May 2007 and the middle of August 2007. Our group pri-vate practice is located near a major university and treats children en-rolled in private, preferred-provider organization, and health maintenance organization insurance plans. Patients were identified from charts and sched-ules as 4- to 6-year old children who were eligible to receive standard pre-kindergarten immunizations, specifi-cally diphtheria-tetanus-acellular per-tussis (Sanofi Pasteur, Swiftwater, PA), inactivated polio (Sanofi Pasteur, Swiftwater, PA), and measles-mumps-rubella (MMR) (Merck, Whitehouse Station, NJ) vaccines. Exclusion crite-ria were significant concurrent illness, being unable to follow the intervention directions or to answer the pain scale questions, recent (within 1 year) veni-puncture or hospitalization, and pre-vious invasive procedures other than perinatal circumcision. Parents of po-tential enrollees were approached by 1 of the investigators in advance or at the time of their child’s appointment and were given a consent form after the nature of the study was explained. Therefore, our study involved a conve-nience sample of eligible patients.
Study Design
After written informed parental con-sent was obtained and the child and parent agreed to be videotaped, an identifying number was assigned to the child and a flip of the coin deter-mined whether the patient was to
re-for both groups.
The diphtheria-tetanus-acellular per-tussis and inactivated polio vaccines were administered intramuscularly in one arm with a 25-gauge,5⁄8-inch
nee-dle, and then the MMR vaccine was administered subcutaneously in the other arm with a 26-gauge,5⁄8-inch
nee-dle. One of 3 office medical assistants gave the 3 injections, in accordance with their regular office schedules and availability. Directly after the proce-dure, all children were offered a va-nilla wafer (customary office routine), and pain reports were solicited.
The subjects were shown the Faces Pain Scale-Revised (FPS-R), a well-studied, reproducible, self-report pain tool12–15 in which the child views 6
gender- and age-neutral facial expres-sion images, ranging from slightly smiling to highly distressed, and is asked to choose the image that best represents the way he or she feels or recently felt. The first image is scored 0 and 2 points are added for each sub-sequent image indicating greater dis-comfort, reaching a maximum of 10. We deviated from soliciting the stan-dardized FPS-R responses to the words “pain” and “hurt,” because the words themselves are suggestive and may in-fluence the score as well as instill neg-ative associations for future immuni-zations.16Instead, we asked the child
to choose the face that most closely showed how he or she felt during the injection sequence. The parent, in the presence of the child, then was shown the FPS-R and was asked to score the degree of discomfort the child seemed to experience.
The co-investigator filmed the inter-vention, where applicable, and the ad-ministration of vaccines. He scored the face-legs-activity-crying-consolability (FLACC) scale items17,18at an
scores were recorded shortly before immunization, after the 2 intramuscu-lar injections, and after the subcutane-ous injection. The 5 indicators are each awarded 0, 1, or 2 points ac-cording to specified criteria, and scores are tallied to yield the total score of 0 to 10, with higher scores indicating greater discomfort.
Immunization Procedures
For children in the distraction group, the investigator began by demonstrat-ing the 3 elements that constituted the technique. First, the cooling spray (Gebauer’s ethyl chloride; Gebauer, Cleveland, OH) was applied to the child’s forearm, with a verbal sugges-tion of coolness and reduced sensa-tion. Next, an improvised, horseshoe-shaped, plastic, multipronged gripper resembling the Shot Blocker (Bionix, Toledo, OH) was demonstrated at the injection site, with the suggestion that the arm might become confused re-garding what was sharp and what was not. Finally, the child was instructed to watch a vibrating instrument (Wahl, Shelton, CT) descend slowly down the contralateral arm and to say loudly “el-bow” (or another word of the patient’s choice) when the instrument actually touched the tip of the elbow (Fig 1). The route of travel to the elbow was varied, which enticed the subject to focus vi-sually and to track the moving object and thus further promoted dissocia-tion from the injecdissocia-tion.
After the child demonstrated the will-ingness and ability to follow the direc-tions, ethyl chloride was sprayed on the injection site and the plastic grip-per was applied below and around it. Immediately thereafter, the child was told to follow the descent of the vi-brating instrument on the opposite arm, which was timed to reach the el-bow just as each of 2 injections took place. The investigator conducting the distraction actively reminded the child
to observe the instrument if the child’s attention wandered toward the arm receiving the injection. The entire in-tervention was then repeated on the opposite arm for the MMR vaccine in-jection. The immunizations were video-recorded from baseline through at least 1 to 2 minutes of recovery. Imple-mentation of the distraction method required 2 individuals, 1 to conduct the intervention and 1 to administer the injections.
Control group subjects received their immunizations in a similar manner but without the intervention steps de-scribed above. The investigators were present in the room, one filming and the other silently observing. There were no other identifiable differences between the 2 groups. Parents and medical assistants were given no di-rection or behavioral constraints and were neither discouraged from offer-ing nor encouraged to offer any form of support or consolation.
Statistical Methods
Nonparametric tests were used to an-alyze the data, because, given our
small sample size, they likely would provide more-stringent measures of significance than parametric tests and because patient and parent self-report scores were expected to follow a non-Gaussian distribution. Significance was set atP⬍.05. The Mann-WhitneyU
test was used to compare the means for the patients’ self-reports of pain, the parents’ reports of perceived pain for their children, the changes in ob-served pain, and the final amounts of observed pain for the treatment and control groups. The nonparametric Kruskal-Wallace test was used to ex-plore differences in reported and ob-servational pain with respect to demo-graphic factors such as age, gender, ethnicity, parent’s gender, siblings, and number of siblings present.
RESULTS
Forty-two children were enrolled dur-ing a 2-month period. One child was excluded after enrollment when it was revealed that, unbeknownst to the in-vestigators, he had been hospitalized recently with asthma. No child was ex-cluded because of an inability to follow FIGURE 1
Improvised arm gripper (top) and vibrating instrument (bottom).
the directions. The 20 study patients and 21 control patients were similar with respect to ethnicity, age, siblings, number of siblings present during im-munization, and baseline FLACC scores. Boys and girls were distributed equally, both within the group as a whole and within the intervention and control groups.
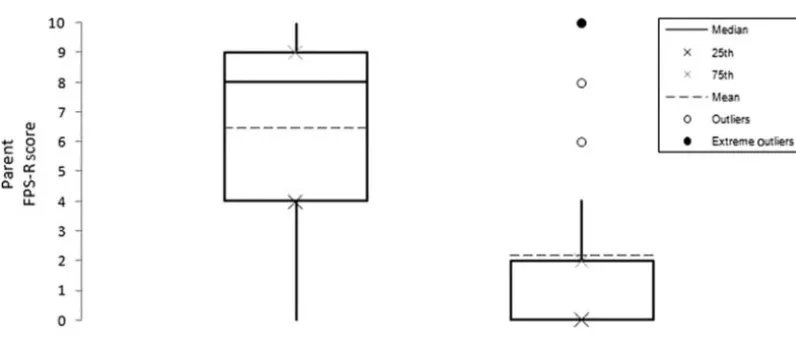
Statistically significant differences were found between the treatment and con-trol groups for both the self-report scores (P ⬍ .0013) and the parent-report scores (P⬍.0002) (Figs 2 and 3). The coefficient for the correlation
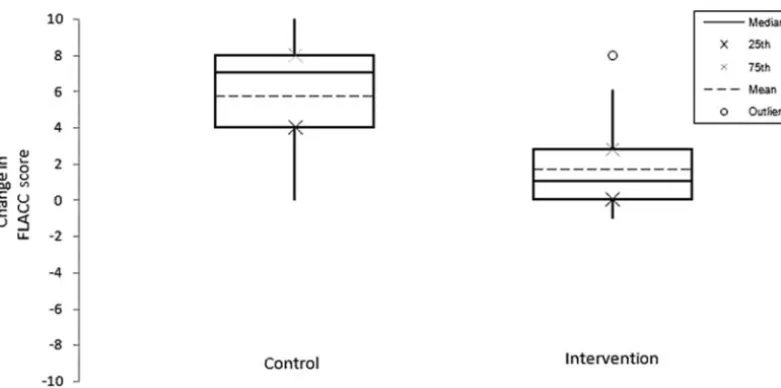
between patient and parent reports was 0.8275. The FLACC scores for base-line versus completion of the immuni-zation series showed a significant ad-vantage for the treatment group (P⬍
.0001) (Fig 4). The coefficient for the correlation between patient self-reports and final FLACC scores was 0.7433. The FLACC score difference be-tween the 2 groups from baseline to after the 2 intramuscular injections in the first arm was significant (P ⬍
.0001). To assess the impact of the sub-cutaneous MMR vaccine injection, we compared the FLACC score recorded
after the first 2 intramuscular injec-tions with the final FLACC score. The difference also was significant (P ⬍
.05).
DISCUSSION
A child entering kindergarten is apt to be sensitized to needle-related discomfort and to be apprehensive when immunizations are anticipated.2,3
Cassidy et al19reported that moderate
reduction of pain was achieved with application of lidocaine-prilocaine patches before diphtheria-pertussis-tetanus-polio immunization for 4- to
confidence interval: 0.39 –3.67; interquartile range: 0.00 –2.00), whereas the median score for the control group was 8.00 and the mean was 6.57 (95% confidence interval: 4.70 – 8.43; interquartile range: 2.00 –10.00).
FIGURE 3
6-year-old children. However, the effi-cacy of this pain reduction method is variable, and the method does not ad-dress the anticipatory anxiety that con-tributes to fear of injection, perhaps even more than the needle itself.20,21
As children grow and mature, the perception of “bother” and discomfort begins to diverge from whatever objective measure of pain may be present.6,22School-aged children given
approximately the same pain stimuli may report minimal discomfort or a wide range of degrees of “hurt” up to “worst ever.”6 The affective
contribu-tion to pain percepcontribu-tion provides an op-portunity for intervention that does not rely on pharmacologic diminution of sensory pain alone.6,11
The distraction method we devised re-quires minimal effort on the part of the child and presents a variety of sensory opportunities for dissociation during the injection sequence. Ethyl chloride spray, the multipronged arm gripper, and the vibrating instrument provide different kinds and locations of kines-thetic distraction. We chose ethyl chlo-ride spray because its effectiveness
has been shown to be comparable to that of lidocaine-prilocaine and it is easier to apply.7 Because hypnotic
measures can augment distraction,1
we offered the child verbal sugges-tions of diminished feeling as well as a visual tracking task to focus attention away from the injection.
The hypnotic elements in our interven-tion are based on findings that suggest that most children are in trance states when they exhibit general anxiety or anticipation of needle pain during their medical examination.11 In
hyp-notic trance, children enter an altered state of consciousness in which atten-tion is highly focused on specific sen-sations or activities, whereas aware-ness of others recedes to a point of dissociation. It is a core principle of pediatric hypnotherapy that whatever is used to guide the induction of trance is disclosed in advance, because hyp-nosis is self-induced and volitional.6
Therefore, our intervention goes be-yond simple distraction, which may ac-tually “trick” the patient, reduce trust and confidence, and foster future anxiety.6
The children in the age group we stud-ied likely had attained a developmental level that would allow them to engage in hypnotic suggestion and focusing distraction.2,3Selection of a
prekinder-garten population offered additional advantages, that is, the immunizations were uniform, included the relatively more painful MMR vaccine administra-tion, and were all required for kinder-garten entry.
We chose an accepted self-report mea-sure to evaluate perceived discomfort and associated anxiety, using the FPS-R scored by both the patient and the parent accompanying the child. By all measures, we showed reduction of discomfort in the intervention group at a highly statistically significant level. Furthermore, the parent-reported FPS-R data correlated well with the patient-reported data, although bias cannot be excluded entirely. We concluded that the subjective experience for the intervention group was marked re-duction in the perceived level of pain.
We selected the FLACC scale over simi-lar objective observation scales be-cause of its relative simplicity and ob-FIGURE 4
Box plots of final FLACC scores for the control and intervention groups. Indicated are the medians (solid lines), means (dashed lines), interquartile ranges (box ends), and 10th to 90th percentiles (whiskers). A positive change in the FLACC score represents an increase in total score between baseline and final measurements. The opposite holds true for a negative change. Subjects in the intervention group scored a median of 1.00 and a mean of 1.65 (95% confidence interval: 0.595–2.71; interquartile range: 0.00 –2.75), whereas the median score for the control group was 7.00 and the mean was 5.71 (95% confidence interval: 4.30 –7.13; interquartile range: 4.00 – 8.00).
ment also allowed us to conduct inter-val assessments of the patient’s re-sponses to the immunization series. FLACC scale comparisons corrobo-rated the subjective data for the entire injection series as well as for the 2 in-tramuscular injections by themselves and the subcutaneous MMR vaccine injection that followed. The correla-tion between patient FPS-R data and the final FLACC scores supports the conclusions.
Potential bias could not be eliminated entirely, given the confines of a small study in a private pediatric practice. A single investigator recorded the vid-eos and also scored the FLACC scale items. Although he did not know the patients, he was aware of the design and purpose of the study. Parents were aware of their child’s FPS-R score and might have been influenced by it. Video data corroborated our expecta-tion that the nature and intensity of en-couragement offered by parents or medical assistants would be similar in the 2 groups. We controlled for the mere presence of the investigators, who were careful not to lead the child
gestions already mentioned. Neverthe-less, it is conceivable that physician in-volvement and the investigator’s voice and coaching, as opposed to mere presence, played an independent role, separate from the intervention. We could not ensure that the 3 medical as-sistants who administered the injec-tions were rigorously uniform in their approaches to the 2 groups. The pro-cess of hugging, stroking, and reassur-ing is far too complex to allow for sta-tistical analysis, leaving open some possibility of participant bias.
Another notable limitation of the study is that the complex interplay of the physical and psychological interven-tions could not be analyzed individually in greater depth. Being multifaceted is intrinsic to hypnosis-based distrac-tion, which is designed to offer the child a variety of sensory distracters; however, it makes replication and cor-roboration more challenging. Addi-tional studies will be required to dispel any residual concerns about bias and to explore whether single or multiple components of our method might yield comparable results.
pain and anxiety. We should not simply accept children’s fear of shots as inev-itable and a normal part of pediatric care. Investing the additional time re-quired, with an additional individual, to administer the immunizations likely would be offset by the nursing and pa-rental efforts required to cajole or to comfort an anxious traumatized child. With this or a comparable intervention, the child and parent can leave the pe-diatrician’s office knowing that an ef-fort was made to acknowledge and to address what might be the most fright-ening aspect of well-child visits. The child can thus acquire positive expec-tations for future visits. Research should be undertaken to corroborate our findings, to isolate the most-efficacious components, and to extend similar methods to other age groups.
ACKNOWLEDGMENTS
We acknowledge the valuable contri-butions of Ran D. Anbar, MD, Carl von Baeyer, PhD, Daniel P. Kohen, MD, and Myles Abbott, MD, in the preparation of this manuscript.
REFERENCES
1. Uman LS, Chambers CT, McGrath PJ, Kisely S. Psychological interventions for needle-related procedural pain and distress in children and adolescents.Cochrane Database Syst Rev.2006;(4): CD005179
2. von Baeyer CL, Marche TA, Rocha EM, Salmon K. Children’s memory for pain: overview and impli-cations for practice.J Pain.2004;5(5):241–249
3. Woodin KA, Rodewald LE, Humiston SG, et al. Are children becoming pincushions from immuniza-tions?Arch Pediatr Adolesc Med.1995;149(8):845– 849
4. Schechter NL, Berde CB, Yaster M.Pain in Infants, Children, and Adolescents. Philadelphia, PA: Lippincot Williams & Wilkins; 2003
5. Schechter NL, Zempsky WT, Cohen LL, McGrath PJ, McMurty CM, Bright NS. Pain reduction during pediatric immunizations: evidence-based review and recommendations.Pediatrics.2007;119(5). Available at: www.pediatrics.org/cgi/content/full/119/5/e1184
6. Olness K, Kohen DP.Hypnosis and Hypnotherapy With Children. 3rd ed. New York, NY: Guilford; 1996 7. Reis EC, Jacobson RM, Tarbell S, Weniger BG. Taking the sting out of shots: control of
vaccination-associated pain and adverse reactions.Pediatr Ann.1998;27(6):375–386
8. Goodenough B, Thomas W, Champion GD, et al. Unraveling age and sex differences in needle pain: ratings of sensory intensity and unpleasantness of venipuncture pain by children and their parents.Pain.1999;80(1–2):179 –190
10. French GM, Painter EC, Coury DL. Blowing away shot pain: a technique for pain management during immunization.Pediatrics.1994;93(3):384 –388
11. Sugarman LI.Imaginative Medicine: Hypnosis in Pediatric Practice[DVD and learning guide]. Norwalk, CT: Crown House; 2007
12. von Baeyer CL. Children’s self-reports of pain intensity: scale selection, limitations, and interpre-tation.Pain Res Manag.2006;11(3):157–162
13. Spagrud LJ, Piira T, von Baeyer CL. Children’s self-report of pain intensity.Am J Nurs.2003;103(12): 62– 64
14. Chambers CT, Giesbrecht K, Craig KD, Bennet SM, Huntsman EA. Comparison of faces scales for the measurement of pediatric pain: children’s and parents’ ratings.Pain.1999;83(1):25–35 15. Hicks CL, von Baeyer CL, Spafford PA, van Korlaar I, Goodenough B. The Faces Pain Scale-Revised:
toward a common metric in pediatric pain measurement.Pain.2001;93(2):173–183
16. Berberich FR. Pediatric suggestions: using hypnosis in the routine examination of children.Am J Clin Hypn.2007;50(2):121–129
17. Merkel SI, Voepel-Lewis T, Shayevitz JR, Malviya S. The FLACC: a behavioral scale for scoring postoperative pain in young children.Pediatr Nurs.1997;23(3):293–297
18. von Baeyer CL, Spagrud LJ. Systematic review of observational (behavioral) measures of pain for children and adolescents aged 3 to 18 years.Pain.2007;127(1–2):140 –150
19. Cassidy KL, Reid GJ, McGrath PJ, Smith DJ, Brown TL, Finlay GA. A randomized double-blind, placebo-controlled trial of EMLA威patch for the reduction of pain associated with intramuscular injection in four- to six-year-old children.Acta Paediatr.2001;90(11):1329 –1336
20. Cohen LL, Blount RL, Cohen RJ, Ball CM, McClellan CB, Bernard RS. Children’s expectations and memories of acute distress: short and long-term efficacy of pain management interventions.
J Pediatr Pychol.2001;26(6):367–374
21. Tsao JC, Lu Q, Kim SC, Zeltzer LK. Relationships among anxious symptomatology, anxiety sensitivity and laboratory pain responsivity in children.Cogn Behav Ther.2006;35(4):207–215
22. Kuttner L.A Child in Pain. Point Roberts, WA: Hartley and Marks; 1996
DOI: 10.1542/peds.2007-3466 originally published online July 13, 2009;
2009;124;e203
Pediatrics
F. Ralph Berberich and Zachary Landman
Services
Updated Information &
http://pediatrics.aappublications.org/content/124/2/e203
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/124/2/e203#BIBL
This article cites 16 articles, 1 of which you can access for free at:
Subspecialty Collections
_sub
http://www.aappublications.org/cgi/collection/vaccine:immunization Vaccine/Immunization
b
http://www.aappublications.org/cgi/collection/infectious_diseases_su Infectious Disease
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2007-3466 originally published online July 13, 2009;
2009;124;e203
Pediatrics
F. Ralph Berberich and Zachary Landman
Randomized Clinical Trial
Reducing Immunization Discomfort in 4- to 6-Year-Old Children: A
http://pediatrics.aappublications.org/content/124/2/e203
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.