A hospital’s ability to deliver care for patients safely and efficiently is partly dependent on effectively managing patient throughput.1, 2 A key driver of throughput is the discharge process.3–5 Bottlenecks occur when there is a mismatch between bed availability (supply) and need (demand). In an attempt to improve patient throughput, many hospital administrators institute policies aimed at discharging patients earlier.6, 7 In previous throughput studies, researchers have focused on
the emergency department or inpatient adult medical units and nursing-led initiatives.3, 5 There are few published studies in which researchers examine throughput in the newborn nursery and none in which physician-led quality improvement initiatives are documented.8–11 There are numerous published studies in which researchers describe how checklist use improves safety by standardizing processes.12–14 Although there are few studies in which researchers address their impact
Facilitating the Timely Discharge
of Well Newborns by Using
Quality Improvement Methods
Nicole T. Rochester, MD, a, b, c Laurie P. Banach, MD, a, b, c Wendy Hoffner, MD, a, b, c Deena Zeltser, MD, dPhyllis Lewis, MD, e Elizabeth Seelbach, MD, e Sandra Cuzzi, MDa, b, c
BACKGROUND AND OBJECTIVES: Discharges are a key driver of hospital throughput.
Our pediatric hospitalist team sought to improve newborn nursery
throughput by increasing the percentage of newborns on our service with a discharge order by 11 am. We hypothesized that implementing a discharge checklist would result in earlier discharge times for newborns who met discharge criteria.
METHODS: We identified barriers to timely discharge through focus groups
with key stakeholders, chart reviews, and brainstorming sessions. We subsequently created and implemented a discharge checklist to identify and address barriers before daily rounds. We tracked mean monthly discharge order times. Finally, we performed chart reviews to determine causes for significantly delayed discharge orders and used this information to modify rounding practices during a second plan-do-study-act cycle.
RESULTS: During the 2-year period before the intervention, 24% of 3224
newborns had a discharge order entered by 11 am. In the 20 months after the
intervention, 39% of 2739 newborns had a discharge order by 11 am, a 63%
increase compared with the baseline. Observation for group B Streptococcus
exposure was the most frequent reason for a late discharge order.
CONCLUSIONS: There are many factors that affect the timely discharge of well
newborns. The development and implementation of a discharge checklist improved our ability to discharge newborns on our pediatric hospitalist service by 11 am. Future studies to identify nonphysician barriers to timely newborn discharges may lead to further improvements in throughput between the labor and delivery and maternity suites units.
abstract
To cite: Rochester NT, Banach LP, Hoffner W, et al.
Facilitating the Timely Discharge of Well Newborns by Using Quality Improvement Methods. Pediatrics. 2018;141(5):e20170872
aDivision of Hospital Medicine, Children’s National
Health System, Washington, District of Columbia; bHoly
Cross Hospital, Silver Spring, Maryland; cDepartment
of Pediatrics, School of Medicine, George Washington University, Washington, District of Columbia; dNational
Institute of Child Health and Human Development, National Institutes of Health, Bethesda, Maryland; and eDepartment
of Pediatrics, College of Medicine, University of Kentucky, Lexington, Kentucky
Dr Rochester coordinated planning and implementation of the study, conducted the initial analyses, and drafted and edited the manuscript; Drs Banach, Cuzzi, Hoffner, Zeltser, Lewis, and Seelbach analyzed and interpreted the data and reviewed and revised the manuscript; and all authors approved the final manuscript as submitted.
DOI: https:// doi. org/ 10. 1542/ peds. 2017- 0872
Accepted for publication Jan 2, 2018 Address correspondence to Sandra Cuzzi, MD, Division of Hospital Medicine, Children’s National Health System, 111 Michigan Ave, NW Suite M4800, Washington, DC 20010. E-mail: cuzzis@ holycrosshealth.org
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2018 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have
indicated they have no financial relationships relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors
on efficiency, we hypothesized that a checklist would improve timely discharges by standardizing the discharge process and identifying key barriers before rounds.6
With over 8500 deliveries annually, our hospital is often faced with throughput challenges in both the labor and delivery (L&D) and maternity suites units. During times of high volume, throughput delays develop on maternity suites, requiring postpartum mothers to board with their infants in L&D for extended periods. Mother-infant dyads present a unique challenge to throughput initiatives because discharge is dependent on the readiness of both patients, and the coordination of discharge typically occurs asynchronously.15 Efforts to improve throughput led to a directive from our hospital administration to discharge mother-infant couples by 11 am. Although there were
adjustments made to nursing roles, including the creation of a “discharge nurse, ” there was no comprehensive attempt to engage physicians despite assumptions that the newborn discharge order was frequently the rate-limiting step. Our objective with this study was to evaluate our newborn discharge process and improve timely discharge of well newborns on the pediatric hospitalist service in our community teaching hospital.
Review of baseline data established that 24% of well newborns on the hospitalist service had discharge orders entered by 11 am. Frequently,
barriers to discharge were not identified until the late morning, during rounds. Our aim was to increase the percentage of newborns with a discharge order by 11 am by
50% compared with our baseline.
METHODS
This study received exemption from the Institutional Review Board at Holy Cross Hospital.
Context
Holy Cross Hospital is a 443-bed community teaching hospital located in suburban Maryland. It is the highest-volume delivery hospital in the state, with 8500 to 9000 deliveries per year. Our hospitalist team cares for ∼20% of the well newborns and consists of 3 pediatric interns, 1 to 2 third-year medical students, and the pediatric hospitalist attending. The trainees preround on the newborns, prepare daily notes, and examine the newborns before the attending’s arrival. After examining the infants, the attending cosigns the notes either before or during patient rounds. Discharge orders are then entered by either the intern or attending when the patient has met established criteria.
There are 6 core hospitalists and 5 moonlighter physicians. We care for a small subset of insured newborns whose pediatricians are either on vacation or do not have hospital privileges. We are the sole provider for unassigned newborns with state Medicaid and those born to uninsured mothers, many of whom are recent immigrants with limited resources. Because of language barriers, social stressors, and other concerns, these newborns are at particularly high risk for complications after discharge, and extreme care is necessary when coordinating discharge planning.16, 17
Intervention
We organized a multidisciplinary team composed of key stakeholders, including representatives from hospital administration, nursing leadership, frontline nursing staff, pediatric interns, and the pediatric hospitalist group. Focus groups were conducted and we used brainstorming sessions to identify key drivers and perceived barriers to timely newborn discharge (Fig 1). We collected baseline data
(discharge order times) for well newborns on our service discharged
between July 1, 2010, and June 30, 2012. Chart reviews were performed on a randomly selected sample of 120 newborns discharged over a 12-month period to further delineate barriers to timely discharge. The initial list of barriers included maternal age, parity, insurance status, primary language, ethnicity, gestational age, delivery type, day of the week, holiday, bilirubin check, weight loss, group B Streptococcus
(GBS) exposure, follow-up, car seat test, and lactation consult. We created a discharge checklist (Supplemental Fig 4) using a subset of the commonly identified barriers as determined by group consensus. This checklist was used solely for newborns on the hospitalist service. The discharge checklist was implemented on November 5, 2012, and data were collected through June 30, 2014.
The pediatric hospitalists were educated regarding the discharge checklist. Reminders were sent via e-mail and problems with implementation were discussed during monthly group meetings. Every 4 weeks a new pediatric intern group was oriented to the checklist on the first day of its rotation. This posed a significant challenge because the project’s success relied on the interns’ accurate completion of the checklist before the attending’s arrival. Interns were re-educated as needed and reminders were provided when the checklist was not completed. The checklist was completed daily by the interns during prerounding and reviewed by the attending on arrival, with the goal of identifying issues preventing an 11 am discharge order. These issues
the hospitalist group monthly via e-mail and at meetings. Our initial plan was to limit use of the checklist to weekdays because weekend rounding practices varied among our hospitalists and there was concern about our ability to comply with the intervention. However, after 1 month we decided to use the checklist daily (including weekends and holidays) to ensure consistent implementation and to maximize improvement. Several months after implementation it was evident that our rounding process and attending workflow were not conducive to entering timely discharge orders. After 6 months, a second plan-do-study-act (PDSA) cycle was initiated to improve workflow. Hospitalists changed their rounding practices so that discharges were prioritized. Workflow was interrupted to follow-up on outstanding barriers. Reminder phone calls were placed to multidisciplinary team members when their outstanding tasks required completion.
Core hospitalists were incentivized to fully participate in this project because it was included in the
group’s annual faculty goals and tied to a performance-based bonus. Because our primary aim was to improve discharge order times, a potential ethical concern was that physicians might modify existing practices such that newborns would be discharged before meeting established criteria to achieve our goal. The team made an a priori decision to continue following existing newborn care clinical guidelines established by the American Academy of Pediatrics.18, 19 In addition, we decided not to enter conditional orders, which would theoretically improve discharge order times but would not reflect the actual time the patient was ready for discharge.
Study of the Intervention
An informatician provided monthly spreadsheets with discharge order times for all newborns on the pediatric hospitalist service. Newborns transferred to the pediatric inpatient unit or to the NICU were excluded. The principal investigator (PI) reviewed the spreadsheets for accuracy; incorrect
and duplicate entries were deleted. There were no additional quality improvement initiatives or process changes related to newborn throughput launched during our study period. Therefore, the observed changes are felt to be due largely to our implementation of the discharge checklist and practice changes resulting from this project.
Measures
Our primary outcome measure was the percentage of newborns on the hospitalist service with a discharge order by 11 am. To gain additional
insight regarding discharge delays, we determined the actual causes for moderately delayed discharge orders, defined a priori as discharge orders placed >1 hour after the goal of 11 am.
The primary process measure was compliance with checklist completion. The PI monitored the number of missing checklists monthly and provided formative feedback when necessary.
Analysis
The percentage of newborns on the hospitalist service with a discharge order by 11 am was calculated
monthly and plotted on a control chart. Data were analyzed by using statistical process control methodology. The mean was shifted when 8 consecutive data points were either above or below the centerline, signaling special cause variation. To analyze the causes for moderately delayed discharge orders, the core hospitalists performed retrospective chart reviews for all newborns with discharge orders after 12 pm
during the study period. We identified all documented causes for delayed discharge orders by using a standardized data abstraction tool (Supplemental Fig 5). The primary source for data abstraction was the patient’s discharge summary. Additional information was obtained by reviewing orders and laboratory results when necessary. All issues
Specific Aim Key Drivers Intervenons
Increase the percentage of newborns with a discharge order by 11 by 50% by June 2014
Buy-in from physicians and staff
Focus groups and local experse Retrospecve chart review Literature review Idenfy common barriers
to discharge
Resoluon of medical issues Communicaon
Timely feedback
Hospitalist and intern educaon and reminders
Monthly feedback to hospitalists Hospital direcve to discharge by 11 Discussions with key stakeholders
Implement discharge checklist Frequent status updates Timely clinical documentaon
Track discharge mes
Chart review with data abstracon tool Iniate new PDSA cycle
Idenfy and address issues proacvely Workflow interrupon to address issues Reminder phone calls to muldisciplinary team members
Improvement in process and minimize avoidable delays
FIGURE 1
unresolved by 12 pm were counted as
reasons for delayed discharge orders. If no clear time stamp was available on review, the time of the intern’s addendum in the electronic medical record was accepted as a proxy for the time the issue was resolved. In some cases, there was a single identifiable cause, but in many cases multiple issues contributed to the delayed discharge order. If a clinical or social issue not included on the discharge checklist contributed to a delay, this cause was categorized as “other” and additional details were provided on the data abstraction tool. When there was no identifiable cause for the delay, the reason was categorized as “unknown.” If the patient was inadvertently omitted from the checklist or the daily checklist was missing, the cause was categorized as “missing data.” Reviewers were encouraged to include narratives, particularly when there were questions regarding the cause for delayed discharge orders. The PI reviewed each data abstraction sheet, and reasons for delayed discharge were confirmed. Disagreements in attribution of cause were discussed and ultimately resolved by the PI, who provided feedback regarding errors in data abstraction such that accuracy improved over time and disagreements became less common.
RESULTS
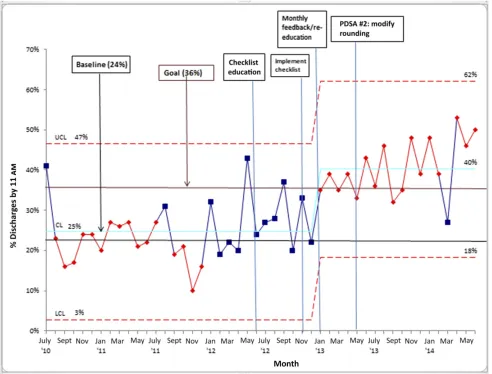
At baseline, 24% of 3224 newborns were discharged by 11 am. Our aim
was to improve this rate by 50%. We met our discharge goal for only 2 of the first 6 months after implementation of the checklist. During this time an average of 34% of 775 discharge orders (monthly range 22%–40%) were entered by 11 am.
Chart review revealed many barriers outside of the physician’s control. However, we identified numerous occasions in which the patient appeared to be ready for discharge
but the order was not entered in a timely manner because of attending workflow. This was discussed in team meetings and a second PDSA cycle was started. Over the next 14 months of the second PDSA cycle, an average of 43% of 1964 discharge orders (monthly range 27%–53%) were entered by 11 am (Fig 2).
During the first full month of the intervention (December 2012), 28 of 31 checklists were inadvertently discarded, and information regarding causes for late discharge orders could not be analyzed. Subsequently, team members were re-educated and the number of missing checklists improved, with a median of 1.5 per month (range 0–4).
Our secondary aim was to determine the actual reasons for discharge delays. Our analysis revealed that the most frequent cause (12.5%) of late discharge orders was
in-hospital observation of newborns for maternal GBS colonization. The second most frequent cause (12.1%) was “missing data, ” a category assigned to infants discharged after 12 pm whose names
were inadvertently omitted from the discharge checklist or whose checklist was missing. The third most frequent cause (10.4%) was a combination of reasons categorized as “other.” The majority of these were clinical issues not included on the checklist, such as pending studies, decreased elimination, and observation for late preterm birth. In contrast to the aforementioned infants, whose late discharge orders were due to unresolved clinical or social issues, a fair number of apparently discharge-ready infants had discharge orders entered late for no identifiable reason. These were categorized as “unknown” (Fig 3). Of note, the proportion of late discharge orders in this category decreased from 22% in the first 6 months of the study to only 9% in the remainder of the study after the second PDSA cycle.
DISCUSSION
Implementation of a discharge checklist led to a significant and sustained improvement in the percentage of well newborns on the hospitalist service with a discharge order by 11 am.
Chart review identified that many discharge delays were due to nonmodifiable factors related to the provision of medical care, such as observation for maternal GBS colonization. At times, however, there were no obvious medical or social barriers to discharge, and it appeared the delay was in the attending’s evaluation of the infant. The proportion of late discharge orders attributed to seemingly modifiable factors decreased after a subsequent PDSA cycle that focused on improving attending workflow. Peak hospital occupancy typically occurs at midday, when new patients arrive and must wait for other patients to be discharged.20 Scheduled morning cesarean
deliveries pose a particular challenge on our maternity suites unit. Hospital administration responded with a goal discharge time of 11 am to
facilitate throughput. Although timed discharges may not be feasible or medically appropriate in other units, the issues affecting postpartum mothers and well newborns are largely predictable.21 A discharge time goal was therefore felt to be appropriate in this setting.
Communication has been identified as the most important challenge to patient throughput.22 The discharge checklist was designed to improve communication between interns and attending physicians, who are often in physically separate locations during morning prerounding. We predicted that a document shared between interns and attending physicians would draw attention to remaining barriers to discharge. Interns could then focus on resolving issues quickly so that a timely discharge order could be entered. Finally, we hoped that identifying common, recurring causes for discharge delays would help inform future throughput improvement efforts.
It is indicated in our study results that the following factors led to a sustained improvement in newborn discharge order times: identifying throughput as a significant
problem over which our group had influence, obtaining buy-in from key stakeholders, creating and implementing the discharge checklist to identify barriers to discharge and facilitate communication, and tracking discharge times with monthly updates to the group (Fig 2). Barriers to improvement included the need to train a new group of interns every 4 weeks and incomplete spread to moonlighting physicians.
Although the particular systems issues at our community teaching hospital may not be universal, it is likely that many hospitals face similar challenges and can apply our intervention in their newborn nursery setting. Physician groups can determine their own barriers to discharge and modify the checklist to meet their needs. All institutions share certain medical barriers to discharge, such as GBS observation or hyperbilirubinemia. Because of these medical barriers, adopting a goal to discharge 100% of newborns by 11 am
is undesirable and would likely represent improper medical care at the expense of throughput.21 A better goal is to identify and eliminate
FIGURE 2
preventable causes of discharge delay.
Although we involved many discharged patients in our study and showed sustained
improvements over several years, this study did have several limitations. First, we were unable to address how daily census may have impacted the percentage of newborns discharged on time because there was no straightforward way to track volume retrospectively. We suspect that a higher daily census was associated with discharge delays.
Also, by limiting chart analysis of late discharges to those with discharge orders after 12 pm, we
may have missed opportunities for improvement.
In our study we examined discharge order times (a variable we could control) and not the time the patient physically left the unit, which more directly affects throughput. In our experience there were often moderate delays in discharge of the mother-infant dyad after the newborn discharge order was placed. To further improve throughput, hospital and
nursing administration can consider investigating and troubleshooting causes of these delays.
It is difficult to know how much improvement was due to the discharge checklist itself versus attending awareness of the project and increased attention to discharges. We adhered to our usual rounding practices until modifications were agreed on as part of a subsequent PDSA cycle. However, it is possible that subtle or subconscious changes took place, leading to more timely discharges.
FIGURE 3
Although we agreed to continue following all applicable hospital protocols and American Academy of Pediatrics recommendations, there is the possibility that patients were discharged prematurely to improve results. However, there was no evidence of this practice on chart review.
Finally, we also had issues with missing data, in which checklists could not be found for review. We may therefore have missed opportunities to identify areas for improvement. One possible solution would be to transition to an electronic discharge board accessible to both physicians and nursing staff, which would lead to further improvements in communication.9
CONCLUSIONS
Throughput is an important factor in a hospital’s ability to deliver safe and efficient patient care as well as a driver of patient satisfaction. In our study, implementation of a discharge checklist led to significant and sustained improvement in timely discharges of well newborns. The discharge checklist functions as a simple tool to facilitate communication between team members and focus attention on outstanding issues. To maintain these improvements over time, ongoing surveillance and adjustments will be needed. Future studies to identify nonphysician barriers to timely newborn discharges may lead to further improvements in throughput between the L&D and maternity suites units.
ABBREVIATIONS
GBS: group B Streptococcus
L&D: labor and delivery PDSA: plan-do-study-act PI: principal investigator
REFERENCES
1. Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academies Press; 2001. Available at: www. nap. edu/ books/ 0309072808/ html/ . Accessed March 30, 2016
2. Terrell LA, Vidrine D. Expediting obstetric patient throughput: decreasing lengths of stay and optimizing hidden bed capacity. In: AWHONN Convention; June 12–16, 2010; Las Vegas, NV
3. Throughput initiatives lower discharge time by two hours. Hosp Case Manag. 2009;17(8):119–120
4. Hospital discharge process can be more efficient. Hosp Case Manag. 2009;17(7):105–106
5. Throughput drive lowers discharge time, LOS. Hosp Case Manag. 2010;18(1):9–10
6. Wertheimer B, Jacobs RE, Bailey M, et al. Discharge before noon: an achievable hospital goal. J Hosp Med. 2014;9(4):210–214
7. Discharge planning advisor. New system streamlines patient throughput. Hosp Peer Rev. 2005;30(4):51–53
8. Ciaramella J, Longworth N, Larraz L, Murphy S. Improving efficiency, consistency and satisfaction on a mother-baby unit with the discharge nurse position. Nurs Womens Health. 2014;18(4):333–339
9. Jimenez J, DeSanto A. Timely discharge of clinically eligible patients in the postpartum setting. J Obstet Gynecol Neonatal Nurs. 2011;40(S1):S79 10. Maurer P. Discharge timeliness for
mother baby couplets: a six sigma project to improve throughput. In: AWHONN Convention; June 15–19, 2013; Nashville, TN
11. Kobokovich LJ. Use of accelerating clinical improvement in reorganization of care: the Dartmouth-Hitchcock Medical Center experience. J Obstet Gynecol Neonatal Nurs. 1997;26(3):334–341
12. Soong C, Daub S, Lee J, et al. Development of a checklist of safe discharge practices for
hospital patients. J Hosp Med. 2013;8(8):444–449
13. Halasyamani L, Kripalani S, Coleman E, et al. Transition of care for hospitalized elderly patients—development of a discharge checklist for hospitalists. J Hosp Med. 2006;1(6):354–360
14. Schulman J, Stricof R, Stevens TP, et al; New York State Regional Perinatal Care Centers. Statewide NICU central-line-associated bloodstream infection rates decline after bundles and checklists. Pediatrics. 2011;127(3):436–444 15. Bernstein HH, Spino C, Finch S, et al.
Decision-making for postpartum discharge of 4300 mothers and their healthy infants: the Life Around Newborn Discharge study. Pediatrics. 2007;120(2). Available at: www. pediatrics. org/ cgi/ content/ full/ 120/ 2/ e391
16. Lorenz JM, Ananth CV, Polin RA, D’Alton ME. Infant mortality in the United States. J Perinatol. 2016;36(10):797–801
17. Osterman MJK, Kochanek KD, MacDorman MF, Strobino DM, Guyer B. Annual summary of vital statistics: 2012-2013. Pediatrics. 2015;135(6):1115–1125
18. American Academy of Pediatrics; Committee on Fetus and Newborn. Hospital stay for healthy
term newborns. Pediatrics. 2010;125(2):405–409
19. Goyal NK, Fager C, Lorch SA. Adherence to discharge guidelines for late-preterm newborns. Pediatrics. 2011;128(1):62–71
20. Fieldston E, Ragavan M, Jayaraman B, Metlay J, Pati S. Traditional measures of hospital utilization may not accurately reflect dynamic patient demand: findings from a children’s hospital. Hosp Pediatr. 2012;2(1):10–18
21. Iantorno S, Fieldston E. Hospitals are not hotels: high-quality discharges occur around the clock. JAMA Pediatr. 2013;167(7):596–597
DOI: 10.1542/peds.2017-0872 originally published online April 11, 2018;
2018;141;
Pediatrics
Elizabeth Seelbach and Sandra Cuzzi
Nicole T. Rochester, Laurie P. Banach, Wendy Hoffner, Deena Zeltser, Phyllis Lewis,
Improvement Methods
Facilitating the Timely Discharge of Well Newborns by Using Quality
Services
Updated Information &
http://pediatrics.aappublications.org/content/141/5/e20170872 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/141/5/e20170872#BIBL This article cites 18 articles, 6 of which you can access for free at:
Subspecialty Collections
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_
Fetus/Newborn Infant
sub
http://www.aappublications.org/cgi/collection/quality_improvement_
Quality Improvement
_management_sub
http://www.aappublications.org/cgi/collection/administration:practice
Administration/Practice Management following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2017-0872 originally published online April 11, 2018;
2018;141;
Pediatrics
Elizabeth Seelbach and Sandra Cuzzi
Nicole T. Rochester, Laurie P. Banach, Wendy Hoffner, Deena Zeltser, Phyllis Lewis,
Improvement Methods
Facilitating the Timely Discharge of Well Newborns by Using Quality
http://pediatrics.aappublications.org/content/141/5/e20170872
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2018/04/09/peds.2017-0872.DCSupplemental Data Supplement at:
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.