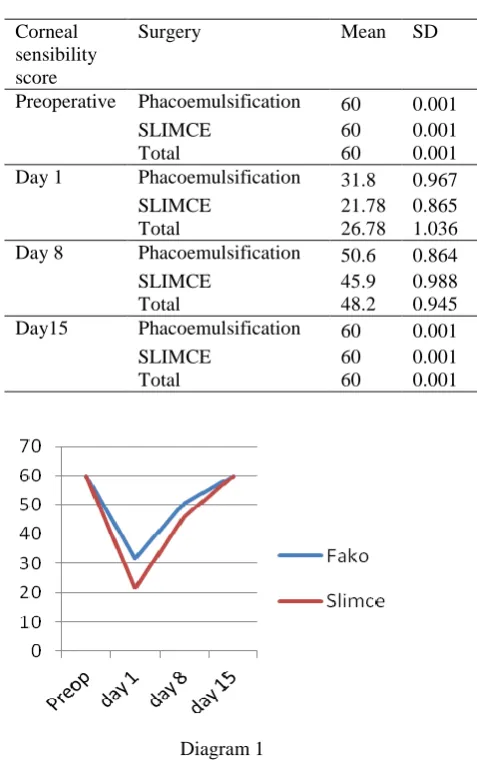
PHACOEMULSIFICATION AND SUTURELESS LARGE-INCISION MANUAL CATARACT EXTRACTION CHANGE CORNEAL SENSIBILITY
Full text
Figure
Related documents
Anti-adhesion layer makes Si mother mold easy to separate and reproduce CoNi stamp. EE lectronic lectronic M M aterials and aterials and PP rocessing rocessing
This is the first study that uses personal interviews to analyze gender differences in cyberstalking in Malaysia.Women report experiencing cyberstalking more than men,
Since its first enunciation by the British sociologist Ruth Glass in her work London: aspects of Change (Glass 1964), the term has been used to describe different forms of
Big data is mainly collection of data sets so large and complex that it is very difficult to handle them using on-hand database management tools. The main
I muntlig och skriftlig interaktion i olika, även formella och komplexa, sammanhang kan eleven uttrycka sig tydligt, ledigt och med flyt samt med anpassning till syfte, mottagare och
The study evaluated public opinion in South Africa concerning how the participants felt about strikes in the healthcare context; whether healthcare workers have a right to
Single case reports discussed successful use of anti-CD20 treatment in one case of neurosarcoido- sis [ 11 ], one of sarcoidosis-associated neuromyelitis optica [ 12 ], one of
Jungck, Common fixed point results for non commuting mappings without continuity in cone metric space, J. Hamlbarani, Some notes on the paper “Cone metric spaces and fixed point
