5
Drivers for change: Western Australia
Patient Blood Management Program
(WA PBMP), World Health Assembly
(WHA) and Advisory Committee on
Blood Safety and Availability (ACBSA)
Shannon L. Farmer, Research Fellow, Consultant,
Adjunct Research Fellow, Adjunct Senior
Research Fellow
a,b,c,*, Simon C. Towler, FCICM, FANZCA,
FAMA, Staff Specialist Intensive Care, Medical Advisor,
Adjunct Professor
a,c,d,e,h, Michael F. Leahy, MB ChB, FRACP,
FRCP, FRCPath, Clinical Professor, Consultant Haematologist.
Director, Clinical Professor in Medicine
a,g,f,i, Axel Hofmann,
ME MD, Medical Economist, Consultant,
Adjunct Associate Professor, Visiting Professor
a,b,c,jaPatient Blood Management Program Team, Office of the Chief Medical Officer, Western Australia
Department of Health, Perth, Western Australia, Australia
bSchool of Surgery, Faculty of Medicine Dentistry and Health Sciences, University of Western
Australia, Perth, Western Australia, Australia
cCentre for Population Health Research, Curtin Health Innovation Research Institute, Curtin University,
Perth, Western Australia, Australia
dIntensive Care Unit, Royal Perth Hospital, Perth, Western Australia, Australia eEdith Cowan University, Perth, Western Australia, Australia
fSchools of Medicine and Pharmacology, Pathology and Laboratory Medicine, University of Western
Australia, Perth, Western Australia, Australia
gHaematology Department & Patient Blood Management Program, Fremantle Hospital, Fremantle,
Western Australia, Australia
*Corresponding author. PO Box 232, Glen Forrest, WA 6071, Australia. Tel.:þ61 419 959 989; Fax:þ61 9298 8655. E-mail addresses:[email protected](S.L. Farmer),[email protected](S.C. Towler),[email protected]
(M.F. Leahy),[email protected](A. Hofmann).
hPO Box 3034, Broadway Nedlands LPO, Nedlands, WA 6009, Australia. Tel.:þ61 434 071 421. i PO Box 480, Fremantle, WA 6959, Australia. Tel.:
þ61 8 9431 2886; Fax:þ61 8 9431 2881.
j Institute of Anaesthesiology, University Hospital of Zurich, Rämistrasse 100, CH-8091 Zurich, Switzerland. Tel.:
þ41 44 255 2695; Fax:þ41 44 255 4409.
Contents lists available atSciVerse ScienceDirect
Best Practice & Research Clinical
Anaesthesiology
j o u r n a l h o m e p a g e : w w w . e l s e v i e r . c o m / l o c a t e / b e a n
1521-6896/$–see front matter !2012 Elsevier Ltd. All rights reserved.
Keywords:
patient blood management anaemia
blood loss transfusion practice change
Patient blood management is now high on national and interna-tional health-system agendas. Serious supply challenges as a result of changing population dynamics, escalating cost of blood, ongoing safety challenges and questions about transfusion efficacy and outcomes are necessitating change in transfusion practice. Numerous initiatives are underway to bring about change, including the institution of comprehensive patient blood management pro-grammes. In 2008, the Western Australia Department of Health initiated a 5-year project to implement a comprehensive health-system-wide Patient Blood Management Program with the aim of improving patient outcomes while reducing costs. Clinically, the Program was structured on the three pillars of patient blood management, namely (1) optimising the patient’s own red cell mass, (2) minimising blood loss and (3) harnessing and optimising the patient-specific anaemia reserve. It employs multiple strategies to bring about a cultural change from a blood-product focus to a patient focus. This Program was undertaken in a State that already had one of the lowest red blood cell issuance rates per 1000 pop-ulation in the developed world (30.47 red blood cell units per 1000 population). The Program identified reasons and drivers for practice change. Fromfinancial years 2008–09 to 2011–12, issuance has progressively decreased in Western Australia to 27.54 units per 1000. During the same years, despite increasing activity, total issuance of red blood cells to the entire State decreased from 70,103 units to 65,742. Nationally and internationally, other initiatives are underway to bring about change and implement patient blood management. The World Health Assembly in May 2010 adopted resolution WHA63.12 endorsing patient blood management and its three-pillar application. The United States Advisory Committee on Blood Safety and Availability met in 2011 to consider the implica-tions of this resolution and its implementation.
!2012 Elsevier Ltd. All rights reserved.
The Western Australia Patient Blood Management Program Background
Authorities have been highlighting a need for change in transfusion practice over the last two decades.1–3Historically, however, changing medical practice in a sustainable manner has been chal-lenging, and it is equally so in transfusion practice.2In mid-2008, the Western Australia (WA) State Health Executive Forum approved a 5-year project to implement a sustainable health-system-wide comprehensive Patient Blood Management Program (PBMP).4The aim of the Program, in line with the principles of patient blood management (PBM) as described by Isbister, was to change transfusion practice from a‘product’focus to a‘patient’focus.5Bringing about such a change requires a cultural shift at every level of the health system.6Fundamentally it was a quality, safety and effectiveness issue with profound resource and economic implications.7The WA PBMP is thefirst proposed on a juris-dictional system-wide basis. A successfully implemented programme has implications for transfusion practice around the globe. Consultants (including two of the authors, SLF and AH) were engaged, initially to develop a concept paper and then to design and guide implementation of a sustainable comprehensive PBMP.
Programme rationale and drivers for change
A review of the medical and change-management literature was conducted to identify successful PBMP models, change-management models and drivers for change. This review, confirmed by
subsequent published studies and reviews, identified compelling reasons to modify practice and drivers to bring about this change.
Formal comprehensive multidisciplinary multimodal programmes have demonstrated an ability to successfully change practice in surgical patients, resulting in significant reductions in blood usage.8–12 These programmes reported between 10% and 95% reductions, depending on baseline blood use and extent of programme implementation.13–28 They also reported positive patient outcomes while reducing costs.
A subsequent systematic review of the literature conducted for the development of the Australian national ‘Patient Blood Management Guidelines: Module 2 Perioperative’resulted in an evidence-based recommendation (Grade C) being made that“Health-care services should establish a multidis-ciplinary, multimodal perioperative patient blood management program.”29 Since that time other programmes have reported results showing reduced transfusion, morbidity, mortality and hospital length of stay with the implementation of a PBMP.30,31
Kotter has described a three-stage, eight-step model for implementing change within organisa-tions.32,33Each step is associated with success and failure of change: Stage 1,‘Defrosting a hardened status quo’, includes four of the eight steps: (1) establishing a sense of urgency, (2) creating the guiding coalition–leadership, (3) developing a vision and strategy and (4) communicating the change vision; Stage 2,‘Introducing many new practices’, includes steps (5) empowering a broad base of people to take action, (6) generating short-term wins and (7) consolidating gains and producing even more change. Stage 3,‘Grounding the changes in the culture’involves step 8, namely institutionalising the new approaches in the culture.
Although not necessarily by design, the structure of successful PBMPs incorporates the principles of the Kotter model for successful change management. Common elements of successful programmes include:
"identifying and establishing a sense of urgency to motivate change; "leadership for successful coordination and implementation;
"developing a vision statement of where the organisation wants to go and why, and strategies to achieve the vision;
"multiple ongoing education strategies for all stakeholders to communicate the vision and strate-gies to bring about a sustained realignment of the organisation’s culture;
"empowerment of a broad base of people (multiple disciplines) to take action and introduce new evidence-based approaches and practices;
"accurate data collection and monitoring as a basis for evaluation, feedback, continuous practice improvement and risk management;
"adoption of a coordinated, integrated, multidisciplinary and multimodality‘team approach’; and "development of policies, protocols, algorithms and guidelines to embed the approach in practice
and the institution’s culture.
Kotter identified that 50% of organisations fail in change because of not being able to establish a sense of urgency. The review identified a number of drivers that represented an urgent need for change in practice,34including the following.
Supply driver
Changing population dynamics represent significant challenges for blood-product inventory in WA, as it does in health systems in most jurisdictions and countries around the globe. In many countries, a looming problem involves what is described as the‘age dependency ratio’, that is, the socio-economic burden of the non-working population carried by the working population.35In this metric, dividing the non-working-age population (65 years and over) by the working population (aged 15–65 years) and multiplying the quotient by 100 produces a ratio. Data from 25 European Union (EU) countries show an age-dependency ratio of 24.8 in 2005. This means that, on average, 24.8 elderly persons were depending on the economic activities of 100 working individuals. Based on current population data, this may climb drastically to almost 40 over the next 20 years.36Hofmann et al. proposed that this can
be translated to a‘total transfusion dependency ratio’(TTDR) as it also means a changing ratio between the donating and the non-donating population age segments.35The non-blood donating population consists of individuals aged 0–17 years plus individuals aged 65 years and over (maximum cut-off ages for donors vary from country to country), and the donating population of individuals aged 18–64 years (in some countries the age for eligible donors is now 16 years and, with certain conditions, older donors may be accepted). Additionally, analysis has shown that the majority of blood is used in the older age segment of the population. Patients 70 years of age and over account for more than 45% of all red blood cells (RBCs) transfused.35Ali et al. demonstrated an eightfold higher RBC consumption in the 70–80-year-old age group than 20–40-70–80-year-olds.37In WA, as with many other countries, the donating age group is growing less than the rapidly growing non-donating but greater blood-using older age segment.Fig. 1shows modelling of the TTDR in a number of countries using the non-donating cut-off ages of 0–14 years and>70 years. Up until 2010, the TTDR favoured the donor population. However, beyond 2010, with thefirst of the baby boomers turning 65 on 1 January 2011, the TTDR predicts a chronically outstripped blood supply if current donation patterns prevail and transfusion practice remains unchanged.
Cost driver
The escalating total cost of blood is becoming unsustainable. Direct product costs have progressively increased as a result of improved collection, testing and processing.38However, broader costing of the total societal cost of blood needs to take into account, not just the direct costs, but also the process of testing and administering blood products within the hospital and the associated costs of monitoring and treating adverse events of transfusion.39,40A recent study showed that the cost of administering an RBC transfusion within the hospital might be 2–5 times that of the product cost.41In 2010 the cost of transfusing a single unit of RBCs, including acquisition costs, in WA was about AU$875.7 If all transfusion-related costs are calculated, including adverse transfusion outcomes, the total cost of transfusion may represent>4.5% of a jurisdiction’s total health-care budget.7
Practice variability driver
Wide variations in transfusion practice exist between countries, institutions and between indi-vidual clinicians within the same institution.42–45 RBC transfusion rates vary from 8% to 93% in
Fig. 1.Modelling of the total transfusion dependency ratio (TTDR) [35] in selected countries demonstrating the potential impact of the ageing population on blood supply. Population data extracted August 23, 2010 fromwww.census.gov/ipc/www/idb/country.php.
cardiac surgery,459%–92% in orthopaedic surgery,4617%–82% in colorectal surgery,470% to>28% in acute coronary syndrome48 and 20%–53% in critical care.49 This wide variation in similar patient populations suggests that a significant number of transfusions may be inappropriate and avoidable. This variation may also reflect a lack of evidence to guide practice. The recent International Consensus Conference on Transfusion Outcomes examined the impact of RBC transfusion on health outcomes in clinical scenarios where transfusions are most commonly considered, representing a substantial percentage of transfusions administered in hospitals. The expert panel found that RBC transfusion was likely to improve health outcomes in only 12% of scenarios, not likely to improve outcome in 59% and in 29% of the scenarios the impact of transfusion was uncertain, requiring further investigation.50
Safety driver
Rigorous screening of donors and testing of blood have reduced the risk of known infectious agents such as human immunodeficiency virus (HIV), hepatitis C virus (HCV) and hepatitis B virus (HBV) to very low levels in developed countries. However, new infectious agents present ongoing safety chal-lenges.51,52Additionally, transfusion-associated circulatory overload (TACO), transfusion-related acute lung injury (TRALI), wrong blood component transfused, acute transfusion reactions and bacterial contamination of blood remain the leading causes of transfusion-related death and major morbidity.53 Clinical driver–a triad of independent risk factors for adverse patient outcomes
The literature review identified a triad of independent risk factors for adverse patient outcomes: anaemia, blood loss (both surgical blood loss and coagulopathic bleeding) and transfusion (Fig. 2). Numerous studies have identified anaemia as an independent and dose-dependent risk factor for increased morbidity, hospital length of stay, mortality and increased risk of transfusion.46,54–57Blood loss during surgery has also been identified as a dose-dependent independent risk factor for adverse patient outcomes.58,59Transfusion to treat blood loss and anaemia has been shown to be an inde-pendent and additive risk factor for adverse patient outcomes.56,60–66The literature reveals a strong independent association between transfusion and increased mortality, intensive care unit (ICU) admission, ICU and hospital length of stay and morbidity, including increased incidence of infection, septicaemia, ischaemic events (including stroke, myocardial infarction and renal impairment/failure), thrombo-embolism, multisystem organ failure, systemic inflammatory response syndrome and acute respiratory distress syndrome.3,61,67–74There is also a dose-dependent relationship, with increasing exposure resulting in increasing risk. Recent studies have demonstrated that even a single unit of RBCs may have a negative impact on patient outcomes.63,65
Fig. 2.A triad of independent risk factors for adverse patient outcomes, modifiable with the application of the three pillars of patient blood management.
A significant percentage of patients present to surgery with anaemia.55Surgery and blood loss induce or contribute further to anaemia. Blood loss and anaemia (or the haemoglobin value) are common triggers for transfusion. Some work suggests that transfusion may contribute to more bleeding.75–77This triad of anaemia, blood loss and transfusion also represents three modifiable risk factors, and can be modified with the application of the three pillars of PBM, namely, (1) optimise the patient’s red cell mass, (2) minimise blood loss and (3) harness and optimise the patient’s physiological anaemia reserve. In surgical patients these three pillars are applied in three integrated phases, the pre-, intra- and postoperative phase. Accordingly, as part of an implementation plan for the WA PBMP, a three-pillar nine-field matrix (Fig. 3) of the multiple perioperative PBM strategies was designed around which clinical education and programme implementation could be structured. The emphasis is on optimising, conserving and managing the patient’s own blood and haemopoietic and haemostatic systems in the perioperative period in order to minimise the triad of risk factors.
In medical, haematology and oncology patients, the three-pillar principle may be applied pre-, intra- and post-event with strategies focussing on optimising haemopoiesis, reducing blood loss and bleeding and using the increased knowledge of the physiological responses to and tolerance and management of anaemia.34
Baseline of WA practice
Part of the challenge of making changes in Australia is the existence of two relatively independent systems of care: (1) universally accessible, free hospital services–largely owned and managed by the
Fig. 3.The 3-pillar 9-field matrix of perioperative patient blood management. This matrix, designed for the Western Australia Patient Blood Management Program, highlights the multiple patient blood management strategies that may be considered in the perioperative period in a patient/procedure-specific context. Adapted from Hofmann A, Friedman D, Farmer S. Western Australian patient blood management project 2008–2012: analysis, strategy, implementation andfinancial projections. Western Australia Department of Health 2007; 1–154.
governments of the States and Territories (the public health system)–which are the major providers of emergency healthcare and much of the high-cost/high-complexity procedures and interventions, and (2) an independent private sector with ownership by both for-profit and charitable providers for which funding comes in a complex manner from private health insurers, governments and patients (the private health sector).
Within this‘pleuralistic’system where funding arrangements and costs are kept relatively separate, fresh blood products–whether used in the public or private sectors–are provided free to the patient. As a consequence all fresh blood products are free on the order of a medical practitioner and there is virtually no price signal in the health sector regarding blood.
At the level of the provision of blood products, the Commonwealth Government is the major funder, providing 63% of the costs to support the procurement and distribution of blood products, with the states providing the balance.
In this context, WA was both uniquely positioned and uniquely challenged. Representing nearly one-third of the land mass of Australia–2.5 million km2–WA has a population of close to 2.4 million persons and has the most rapidly growing population of any state in Australia. Nearly 74% of the population live in the major city, Perth. The health community is relatively isolated with the major opinion leaders largely restricted to the single major city. Perth has 13 publicly funded hospitals, including thefive major tertiary hospitals and these sites consume nearly 60% of the fresh product used in the State. The city also hosts all the major private hospitals in the State and clinicians often have appointments in both hospital systems. Furthermore, the administration of the State budget and policy on the use of blood products co-exist within the WA Department of Health. These unique character-istics of size and distribution of the health services, combined with a long history of lower dependence on the use of fresh blood products but sustained quality in patient outcomes, meant that WA repre-sented a major opportunity for the implementation of a coordinated PBMP.
WA already had a conservative approach to transfusion.78In 1990 a comprehensive blood conser-vation programme was established and co-founded by one of the authors (SLF) in a private hospital that had links with a nearby teaching hospital.7This programme saw significant reductions in blood utilisation in surgery and in time resulted in collaborations with clinicians across all the tertiary hospitals in the State.8,12Despite a conservative transfusion culture and having one of the lowest RBC transfusion rates per 1000 population in the developed world, total issuance to the State was increasing. Published audits and an initial linkage of the transfusion, clinical, laboratory and admin-istrative databases identified wide transfusion practice variation (consistent with the literature), inappropriately high transfusion triggers and inadequate preoperative assessment and management of anaemia.79,80
Programme implementation
The WA PBMP would be progressively phased in over a 5-year period and would concentrate on the public health sector with initial focus on thefive major tertiary hospitals in the city, including the children’s hospital and the women’s hospital. The programme’s vision is to improve patient outcomes while reducing costs by the effective conservation and management of the patient’s own blood. Clinical strategies to achieve this would be built around the three pillars of PBM. Implementation would be based on established PBMP models and employ multiple strategies and professional change-management principles.
Leadership, programme structure and multidisciplinary engagement
Initial key elements of the WA PBMP included an Implementation Board made up of an Authorising and Controlling Unit consisting of the Chief Medical Officer as the Executive Sponsor of the programme and senior health executives, and an Implementation Unit consisting of the Program consultants. The Program would engage a Clinical Reference Group (CRG), information technologists and data managers and external international experts in PBM as educational/consultation faculty. The Implementation Board would be phased out and replaced by a Steering Committee as the Program became self-sustaining. The literature identified two key positions in a successful hospital-based PBMP, namely
a Medical Director and a PBM Nurse Coordinator.9,10,12,25A purpose-formed multidisciplinary repre-sentative PBM Committee (with wider terms of reference than a conventional transfusion committee) provides lead within the institution in developing, implementing and evaluating the Program. Therefore, within each hospital and servicing each Area Health Service there would be a PBMP Medical Director and a Clinical Nurse Consultant (CNC) appointed along with the formation of a PBMP Committee. A jurisdictional wide programme would require overall leadership; therefore, a State PBMP Medical Director and State PBMP CNC would be appointed.
The first phase of the project involved identifying and putting together a multidisciplinary (including physicians of all disciplines, nurses, pharmacists and transfusion scientists) CRG of inter-ested individuals from the various institutions who would take a central clinical role in realigning culture to more appropriate patient-focussed blood management at the institutional/clinical practice level. Expressions of Interest were developed for clinicians to register their interest in participating in the CRG, committees and working groups or to receive educational updates. A symposium was arranged to announce and introduce the programme to the 71-member CRG in November 2008. Additional workshops were conducted with other health-care-provider groups including existing transfusion nurses and transfusion scientists. Work also started on identifying the various clinical and administrative databases that could be accessed to develop a PBM data reporting system to establish baseline data and ultimately a monitoring and feedback system. Job descriptions were developed and approved for the new PBM staff roles. However, the globalfinancial crisis brought about freezes on staff appointments within the health system, resulting in delays and challenges in the appointment of PBM staff positions. The Implementation Unit along with a PBM team within the Department of Health managed the programme with considerable work being performedpro bonoby clinicians across the health service to educate staff and implement various PBM strategies. The programme was fully endorsed by the Australian Red Cross Blood Service and educational initiatives were jointly undertaken at the various sites during thefirst year of the project.
A pilot PBMP was initiated in August 2009 at one of the major tertiary hospitals (a 450-bed acute-care teaching hospital) to develop and refine an Australian-context model.81A PBM Medical Director (one of the authors, MFL, the Director of Haematology) and a PBM CNC were appointed in the pilot hospital in November 2009 and a PBM committee established. Concurrently, MFL was appointed as State PBM Clinical Lead. In September 2011 the State PBMP Clinical Nurse Coordinator was appointed. The Patient Blood Management Guidelines: Module 2 Perioperative states that anaesthetists (anaes-thesiologists) play a key role in multidisciplinary PBM.29As anaesthetists are involved with many of the strategies outlined in the nine-field matrix, two sites have adopted a Co-Director model between a haematologist and an anaesthetist. In late 2011 a haematologist and an anaesthetist were appointed as Co-Directors of the Program at the tertiary women’s hospital with the PBMP CNC appointment to start in November 2012. At the time of writing (October 2012), a haematologist/anaesthetist Co-Director and a PBMP CNC had just been appointed and a PBM Committee established at one other tertiary site. Recruiting of PBMP staff has begun at another site.
Multiple ongoing education and communication strategies for all stakeholders
An initial round of presentations was made to hospital executive committees, and an introduction to PBM was presented at all sites by a group from the international PBM faculty.
An educational website was developed with material for clinicians and consumers. A patient fact sheet on PBM was developed in cooperation with the Australian Red Cross Blood Service along with other patient information materials.4
Educational initiatives have included one-on-one meetings with executives, department heads and programme leads and participants. A continual programme of PBM presentations to major departments at all sites presents the rationale of PBM, the drivers, the current literature and department-specific information from the PBM data system. Periodic multidisciplinary multicentre PBM symposia and workshops have been held with visiting faculty. An email mailing list was compiled to deliver updates from regular reviews of the literature on PBM relevant to various specialties.
A number of education initiatives were undertaken with a view to reducing surgical blood loss in line with the second pillar of the three pillars of PBM. One of these was the development of surgical hae-mostasis workshops at the Clinical Training and Education Centre (CTEC) of the University of Western Australia.82The 1-day workshops include didactic sessions providing data on the perioperative multi-disciplinary multimodal approach of PBM and practical surgical haemostasis sessions in the laboratory. Establishing effective data collection and monitoring systems to facilitate evaluation, continuous practice improvement and risk management
A vital element of a PBMP is the ability to monitor clinical practice, product utilisation and patient outcomes. An early goal of the project was to explore the possibility of developing an integrated infor-mation system for the PBMP. WA has a single unique patient identifier across the metropolitan public health system. This would enable linking of multiple clinical, administrative, laboratory and demo-graphic databases, providing a potentially powerful benchmarking, quality improvement, risk management and change practice tool. Initial work identified the key data elements a PBMP would require and the various databases that would contain this information. During 2009/10 such a PBM database was developed linking the patient administration system with the laboratory management system, enabling analysis and reporting on blood utilisation by a diagnostic-related group (DRG), procedure code and diagnostic code for the metropolitan hospitals. Reports can be produced by hospital, department and individual clinicians. This has already proved to be a useful benchmarking tool, enabling more targeted approaches of PBM strategies. Work is currently underway to produce automated quarterly benchmarking reports to institutions, departments and individual clinicians within depart-ments. At the time of writing, details on the development of this system have been submitted for publication elsewhere (Mukhtar SA, Leahy MF, Trentino K, et al.89A linked data system to provide better opportunities for Patient Blood Management Programs. Submitted for publication 2012).
Developing and implementing PBM clinical policies, procedures and guidelines
One of thefirst tasks identified was the need to develop a preoperative anaemia/iron-deficiency identification, evaluation and management programme.83 The Patient Blood Management Guide-lines: Module 2 Perioperative state that, for implementation of PBMPs, health-care services would need to“re-engineer the way perioperative care is delivered.”29This was identified very early in the WA PBMP in relation to preoperative anaemia management. Contemporary hospital systems and patientflows did not allow for such timely identification and assessment of anaemia and optimisation of patients’haemoglobin and iron stores and, where appropriate, to delay surgery to facilitate opti-misation. Accordingly, a multidisciplinary group with representation from all tertiary sites participated in a 1-day workshop with contribution from national and international experts in thefield to identify barriers and solutions. One outcome was the development of PBM and preoperative anaemia and suboptimal iron store-management guidelines within the‘State Elective Joint Replacement Service Model of Care’.84A number of institutions have subsequently remodelled their preoperative clinics to accommodate this preoperative management. Initiatives were also introduced to engage general practitioners in the initial process of preoperative assessment and optimisation, and a research project is underway to study the cost-effectiveness of early general-practitioner involvement compared to hospital preoperative clinics.
Work is continuing on the development of best-practice protocols, policies, procedures and algorithms based on elements of the nine-field matrix and the 22 evidence-based recommendations and 20 practice points contained within the Patient Blood Management Guidelines: Module 2 Perioperative.29 Conducting outcomes research
Quality research plays a vital role in improving health care; however, it requires effective processes to translate research into clinical practice and patient care.85,86There are potentially powerful syner-gies between research and the implementation stratesyner-gies of PBMPs in getting research to the bedside. The WA PBMP, along with its extensive data collection system, provides numerous research
opportunities. A Research Committee was established and a number of trials are already underway to further investigate various PBM strategies and their translation into practice.
Benchmarking locally and with international centres of excellence
Benchmarking is a powerful change-management tool and the WA PBMP is exploring numerous benchmarking initiatives including benchmarking locally, nationally and internationally with PBM centres of excellence.
Preliminary program results
The pilot PBMP site instituted a number of PBM strategies including clinical staff education, reduced blood sample volumes, computerised prescriber order entry with pop-up alerts and enhanced preoperative clinics to include screening and management of anaemia and suboptimal iron stores. Initiatives were undertaken to reduce surgical blood loss using point-of-care coagulation testing. A single-RBC-unit transfusion policy for symptomatic non-actively bleeding patients was introduced along with a‘fast-track’perioperative anaemia team for management advice. From 2008 to 2011 admissions at the pilot hospital increased by 22%. Despite this increase in activity, RBC units transfused per admission decreased by 26%, fresh frozen plasma by 38% and platelets by 16%. Cryoprecipitate increased by 7%.81More details of the pilot programme have been submitted for publication (Leahy MF, Roberts HA, Mukhtar SA, Farmer SL, et al. A pragmatic approach to embedding Patient Blood Management in a tertiary hospital. Submitted for publication 2012.)
RBC transfusion rates per 1000 population vary considerably between countries with Denmark, Germany and Austria having the highest at 60.0, 57.3 and 52.9, respectively. Australia and the UK at
Fig. 4.Red blood cell issues data for the state of Western Australia 2002–03 to 2011–12 and private and public sector in metro-politan hospitals and laboratorities in Perth, Western Australia 2008–09 to 2011–12 (unpublished NBA data). Printed with permission by the National Blood Authority (Australia). Issuance of red blood cells was progressively increasing in Western Australia. With the introduction of the Patient Blood Management Program in 2008–09 this upward trend was arrested and issuance has decreased each year since.
36.6 and 36.3 have relatively low rates.87WA’s rate of 30.47 was one of the lowest reported in the developed world. However, total issuance to the State had been progressively increasing. During the first year of the programme’s preliminary work, 70,143 RBC units were issued to the State, up from 65,281 the previousfinancial year. Based on historical data, projected age distribution and population and activity increases, RBC issuance was expected to approximate 78,000 units by 2012. However, implementation of the various PBMP initiatives has been associated with a decrease in total issuance of RBCs to the State and issuance per 1000 population each year after programme commencement (Figs. 4 and 5). Issuance to the 19 Perth metropolitan public hospitals, of which thefive major tertiaries were the main focus of the Program, decreased during this period despite a 22.9% increase in case-mix-adjusted acute activity or weighted separations (Fig. 6).
World Health Assembly
In May 2010 the Sixty-third session of the World Health Assembly, the supreme decision-making body of the World Health Organization (WHO), adopted resolution WHA63.12, which contained a number of recommendations on availability and safety of blood products.88The resolution included the following on PBM:
“Bearing in mind that patient blood management means that before surgery every reasonable measure should be taken to optimize the patient’s own blood volume, to minimize the patient’s blood loss and to harness and optimize the patient-specific physiological tolerance of anaemia following WHO’s guide for optimal clinical use (three pillars of patient blood management).” This resolution has important implications for all 193 Member States. WHO is required to report back to the WHA in 4 years on actions taken to implement resolution WHA63.12, providing a further international driver for implementation of PBM and improved patient outcomes.
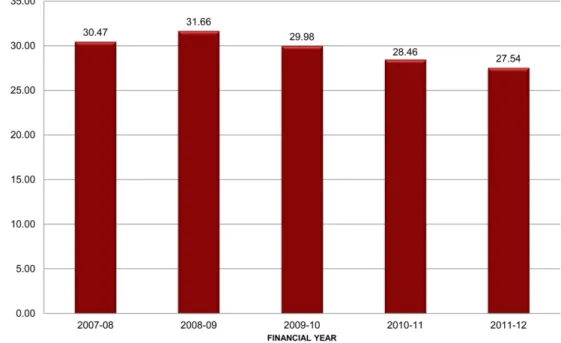
Fig. 5.Red blood cell units issued per 1000 population for the state of Western Australia 2007–08 to 2011–12 (published and unpublished NBA data). Printed with permission by the National Blood Authority (Australia). Red blood cell units issued per 1000 population in the state of Western Australia has decreased each year since the commencement of the Patient Blood Management Program in 2008–09.
Advisory Committee on Blood Safety and Availability
The United States Department of Health and Human Services Advisory Committee on Blood Safety and Availability (ACBSA) provides advice on a range of policy issues to the Secretary and the Assistant Secretary for Health. On 8 June 2011 the ACBSA met to review and comment on World Health Assembly resolution WHA63.12 and its implications for the United States. The committee made several recommendations including obtaining data on PBM, blood utilisation and patient outcomes, promoting education for medical students, practitioners and patients, evaluating available guidelines, sponsoring research and supporting demonstration PBM projects (http://www.hhs.gov/ ash/bloodsafety/advisorycommittee/recommendations/reommendations_201106.pdf).
The United States already has a number of leading PBMPs. Initiatives that derive out of the ACBSA recommendations will no doubt provide further impetus for implementing PBMPs and the adoption of PBM principles into clinical practice.
Summary
Changing from a product focus to individualised PBM requires a change in practice with a proactive and timely approach to the investigation and management of anaemia, blood-loss reduction and improved clinician understanding of the patient-specific physiological anaemia reserve. There are numerous drivers for this practice change. A reducing donor population and an increasing proportion of elderly high consumers of blood products indicate that blood is likely to be in increasingly short supply. Escalating costs of blood will consume disproportionate amounts of health-care budgets. An increasing body of literature identifies wide variations in transfusion Fig. 6.Red blood cell issues data and weighted admissions for metropolitan public hospitals in Perth, Western Australia. Red cell issues data (unpublished NBA data). Activity data extracted from metropolitan health Service Annual report 2011–12 accessed November 23, 2012http://www.health.wa.gov.au/publications/documents/annualreports/2012/MHS_Annual_Report_Part_2011-12. pdfThe Patient Blood Management Program focused initially on the 5 major tertiary public hospitals in Perth, Western Australia. With the introduction of the Program in 2008–09, red cell issuance to all Perth metropolitan public hospitals has decreased each year despite an increase in weighted acute separations.
practice despite limited evidence for transfusion improving health outcomes and strong associations between transfusion and adverse patient outcomes. PBMPs have demonstrated an ability to change practice and reduce blood-product utilisation with positive outcomes. Endorsement of PBM by health bodies such as the WA Department of Health, the WHA and the ACBSA provide further drivers for practice change. Implementation of PBMPs requires multiple strategies and the engagement of health administrators, clinicians and consumers. Preliminary results from the WA PBMP have shown that despite a rapidly growing population and increasing activity blood utilisation across the entire State progressively decreased. The Program brings together unique skill sets and attributes with a clear connection between administration, investment in the resource and the engagement of the clinical community. It demonstrates the opportunities of coordinated jurisdiction-based PBMPs.
Practice points
- PBM is high on jurisdictional, national and international health-service agendas.
- Drivers for change in transfusion practice include supply pressures, escalating cost of blood, ongoing safety challenges, limited evidence for benefit and a growing body of literature demonstrating a strong dose-dependent association between transfusion and adverse outcomes.
- A triad of independent risk factors for adverse patient outcomes–anaemia, blood loss and transfusion–represent three modifiable risk factors that may be reduced by the application of the three pillars of PBM.
- Programmatic approaches to PBM have demonstrated an ability to change practice and effect reductions in transfusion utilisation with equivalent to superior patient outcomes.
- Implementation of PBMPs requires multiple strategies including:
> employment of change-management principles, > effective clinical leadership and programme structure,
> identifying and engaging multiple disciplines with anaesthetists taking a major role in perioperative care,
> ongoing education and communication strategies,
> effective data collection systems to assess and feedback statistics by specialty and
clinician,
> develop policies and procedures for the multimodal approach including a perioperative
anaemia/iron-deficiency identification, evaluation and management programme and
> research initiatives to address knowledge gaps.
Research agenda
- Research into how to more effectively traverse the typical hospital specialty boundaries to implement a multispecialty, multimodal PBMP
- Research to identify the most cost-effective, risk-adjusted models to better measure patient outcomes within PBMP
- Identify knowledge gaps in relation to the individual strategies within the nine-field matrix and conduct outcomes research
- Basic research and development of explanatory models to better understand the possible mechanisms underlying the association between transfusion and adverse patient outcomes - Explore how PBM principles in surgical patients may be translated into the haematology/
Statement of conflict of interest
SLF: Consulting/lecture honoraria or travel support: WA, Qld, NSW, SA Departments of Health, Australian Red Cross Blood Service, Australian National Blood Authority, Australian Jurisdictional Blood Committee, Novo Nordisk, Vifor Pharma Ltd. and Johnson & Johnson Ethicon Biosurgery. SCT: Travel support to present lectures from NATA and SABM and travel support from Ethicon Biosurgery to participate in an educational webinar for procedural specialists about patient blood management in surgical practice. There are no conflicts of interest. MFL: none. AH: Consulting/lecture honoraria or travel support from–Austrian Ministry of Health and the WA Department of Health, Amgen GmbH, Australian Red Cross Blood Service, CSL Behring GmbH, Fresenius Kabi GmbH, Haemonetics GmbH, Janssen-Cilag GmbH, Johnson & Johnson Ethicon Biosurgery, Novo Nordisk, Pentapharm/TEM GmbH, United Biosource Corporation, Vifor Pharma Ltd. and The Institute for Patient Blood Management & Bloodless Medicine and Surgery.
Acknowledgements
The authors gratefully acknowledge the National Blood Authority (NBA) Australia for supplying RBC issue data. There was no funding for this manuscript.
References
1. Isbister JP. The paradigm shift in blood transfusion.Med J Aust1988 Mar 21;148(6):306–308.
2. NHMRC/ASBT.Clinical practice guidelines on the use of blood and blood components. Commonwealth of Australia, 2001. *3. Thomson A, Farmer S, Hofmann A et al. Patient blood management–a new paradigm for transfusion medicine?ISBT Sci Ser
2009;4:423–435.
*4. Western Australia Department of Health.Patient blood management program. Perth: Department of Health, Western Australia, 2009. Available from:http://www.health.wa.gov.au/bloodmanagement/home/.
5. Farmer SL, Isbister JP & Leahy MF. History of transfusion. In Jabbour N (ed.).Transfusion-free medicine. 2nd ed. Malden, Mass: Blackwell Pub, 2012.
6. Mortimer PP. Making blood safer.BMJ2002 Aug 24;325(7361):400–401.
7. Leahy MF & Mukhtar SA. From blood transfusion to patient blood management: a new paradigm for patient care and cost assessment of blood transfusion practice.Int Med J2012 Mar;42(3):332–338.
8. Farmer SL & Webb D.Your body, your choice. Singapore: Media Masters, 2000.
9. Seeber P & Shander A.Basics of blood management. Massachusetts: Blackwell Publishing, 2008.
10. Spiess B, Spence R & Shander A (eds.).Perioperative transfusion medicine. Philadelphia: Lippincott Williams & Wilkins, 2006.
11. Goodnough LT & Shander A. Blood management.Arch Pathol Lab Med2007 May;131(5):695–701.
12. Martyn V, Farmer SL, Wren MN et al. The theory and practice of bloodless surgery.Transfus Apheresis Sci2002 Aug;27(1): 29–43.
13. Wong CJ, Vandervoort MK, Vandervoort SL et al. A cluster-randomized controlled trial of a blood conservation algorithm in patients undergoing total hip joint arthroplasty.Transfusion2007 May;47(5):832–841.
14. Ghiglione M. Blood management: a model of excellence.Clin Leadersh Manag Rev2007 Mar–Apr;21(2):E2.
15. Helm RE, Rosengart TK, Gomez M et al. Comprehensive multimodality blood conservation: 100 consecutive CABG oper-ations without transfusion.Ann Thorac Surg1998 Jan;65(1):125–136.
16. Moskowitz DM, Klein JJ, Shander A et al. Predictors of transfusion requirements for cardiac surgical procedures at a blood conservation center.Ann Thorac Surg2004 Feb;77(2):626–634.
17. Freedman J, Luke K, Escobar M, Vernich L & Chiavetta JA. Experience of a network of transfusion coordinators for blood conservation (Ontario Transfusion Coordinators [ONTraC]).Transfusion2008 Feb;48(2):237–250.
18. DeAnda Jr. A, Baker KM, Roseff SD et al. Developing a blood conservation program in cardiac surgery.Am J Med Qual2006 Jul–Aug;21(4):230–237.
19. Ferraris VA, Ferraris SP, Saha SP et al. Perioperative blood transfusion and blood conservation in cardiac surgery: The Society of Thoracic Surgeons and The Society of Cardiovascular Anesthesiologists clinical practice guideline.Ann Thorac Surg2007 May;83(Suppl. 5):S27–S86.
20. Bui LL, Smith AJ, Bercovici M et al. Minimising blood loss and transfusion requirements in hepatic resection.HPB (Oxford) 2002;4(1):5–10.
21. Slappendel R, Dirksen R, Weber EW et al. An algorithm to reduce allogenic red blood cell transfusions for major orthopedic surgery.Acta Orthop Scand2003 Oct;74(5):569–575.
22. Pierson JL, Hannon TJ & Earles DR. A blood-conservation algorithm to reduce blood transfusions after total hip and knee arthroplasty.J Bone Jt Surg Am2004 Jul;86-A(7):1512–1518.
23. Van der Linden P, De Hert S, Daper A et al. A standardized multidisciplinary approach reduces the use of allogeneic blood products in patients undergoing cardiac surgery.Can J Anaesth2001 Oct;48(9):894–901.
24. Green JA. Blood conservation in cardiac surgery: the Virginia Commonwealth University (VCU) experience.J Cardiothorac Vasc Anesth2004 Aug;18(Suppl. 5):18S–23S.
25. Freedman J, Luke K, Monga N et al. A provincial program of blood conservation: The Ontario Transfusion Coordinators (ONTraC).Transfus Apheresis Sci2005 Nov;33(3):343–349.
26. Reddy SM, Talwar S, Velayoudam D et al. Multi-modality blood conservation strategy in open-heart surgery: an audit. Interact Cardiovasc Thorac Surg2009 Sep;9(3):480–482.
27. Kourtzis N, Pafilas D & Kasimatis G. Blood saving protocol in elective total knee arthroplasty.Am J Surg2004 Feb;187(2): 261–267.
28. Martinez V, Monsaingeon-Lion A, Cherif K et al. Transfusion strategy for primary knee and hip arthroplasty: impact of an algorithm to lower transfusion rates and hospital costs.Br J Anaesth2007 Dec;99(6):794–800.
*29.Patient blood management guidelines: module 2-perioperative: National Blood Authority (Australia)2012 [cited October 2012]. Available from:http://www.nba.gov.au/guidelines/review.html.
*30. Moskowitz DM, McCullough JN, Shander A et al. The impact of blood conservation on outcomes in cardiac surgery: is it safe and effective?Ann Thorac Surg2010 Aug;90(2):451–458.
*31. Kotze A, Carter LA & Scally AJ. Effect of a patient blood management programme on preoperative anaemia, transfusion rate, and outcome after primary hip or knee arthroplasty: a quality improvement cycle.Br J Anaesth2012 Jun;108(6):943–952. 32. Kotter JP & Schlesinger LA. Choosing strategies for change.Harv Bus Rev1979 Mar–Apr;57(2):106–114.
33. Kotter J & Cohen D.The heart of change. Boston: Harvard Business School Press, 2002.
*34. Hofmann A, Farmer S & Shander A. Five drivers shifting the paradigm from product-focused transfusion practice to patient blood management.Oncologist2011;16(Suppl. 3):3–11.
*35. Hofmann A, Farmer S & Shander A. Cost-effectiveness in haemotherapies and transfusion medicine.ISBT Sci Ser2009;4: 423–435.
36. 2007http://www.europa.eu.int/comm/eurostat/.
37. Ali A, Auvinen MK & Rautonen J. The aging population poses a global challenge for blood services.Transfusion2010 Mar; 50(3):584–588.
38. Kamper-Jorgensen M, Hjalgrim H, Edgren G et al. Expensive blood safety initiatives may offer less benefit than we think. Transfusion2010 Jan;50(1):240–242.
39. The cost of blood: multidisciplinary consensus conference for a standard methodology.Transfus Med Rev2005 Jan;19(1): 66–78.
40. Shander A, Hofmann A, Gombotz H et al. Estimating the cost of blood: past, present, and future directions.Best Pract Res Clin Anaesthesiol2007 Jun;21(2):271–289.
41. Shander A, Hofmann A, Ozawa S et al. Activity-based costs of blood transfusions in surgical patients at four hospitals. Transfusion2010 Dec 9;50:753–765.
42. Gombotz H, Rehak PH, Shander A et al. Blood use in elective surgery: the Austrian benchmark study.Transfusion2007 Aug; 47(8):1468–1480.
43. Daly DJ, Myles PS, Smith JA et al. Anticoagulation, bleeding and blood transfusion practices in Australasian cardiac surgical practice.Anaesth Intensive Care2007 Oct;35(5):760–768.
44. Rao SV, Chiswell K, Sun JL et al. International variation in the use of blood transfusion in patients with non-ST-segment elevation acute coronary syndromes.Am J Cardiol2008 Jan 1;101(1):25–29.
45. Bennett-Guerrero E, Zhao Y, O’Brien SM et al. Variation in use of blood transfusion in coronary artery bypass graft surgery. JAMA2010 Oct 13;304(14):1568–1575.
46. Spahn DR. Anemia and patient blood management in hip and knee surgery: a systematic review of the literature. Anes-thesiology2010 Aug;113(2):482–495.
47. Acheson AG, Brookes MJ & Spahn DR. Effects of allogeneic red blood cell transfusions on clinical outcomes in patients undergoing colorectal cancer surgery: a systematic review and meta-analysis.Ann Surg2012 Aug;256(2):235–244. 48. Yang X, Alexander KP, Chen AY et al. The implications of blood transfusions for patients with non-ST-segment elevation
acute coronary syndromes: results from the CRUSADE National Quality Improvement Initiative.J Am Coll Cardiol2005 Oct 18;46(8):1490–1495.
49. Hutton B, Fergusson D, Tinmouth A et al. Transfusion rates vary significantly amongst Canadian medical centres.Can J Anaesth2005 Jun-Jul;52(6):581–590.
*50. Shander A, Fink A, Javidroozi M et al. Appropriateness of allogeneic red blood cell transfusion: the international consensus conference on transfusion outcomes.Transfus Med Rev2011 Jul;25(3):232–246. e53.
51. Blajchman MA & Vamvakas EC. The continuing risk of transfusion-transmitted infections.N Engl J Med2006 Sep 28; 355(13):1303–1305.
52. Stramer SL, Hollinger FB, Katz LM et al. Emerging infectious disease agents and their potential threat to transfusion safety. Transfusion2009 Aug;49(Suppl. 2):1S–29S.
53. Vamvakas EC & Blajchman MA. Blood still kills: six strategies to further reduce allogeneic blood transfusion-related mortality.Transfus Med Rev2010 Apr;24(2):77–124.
54. Dunne JR, Malone D, Tracy JK et al. Perioperative anemia: an independent risk factor for infection, mortality, and resource utilization in surgery.J Surg Res2002 Feb;102(2):237–244.
55. Shander A, Knight K, Thurer R et al. Prevalence and outcomes of anemia in surgery: a systematic review of the literature. Am J Med2004 Apr 5;116(Suppl. 7A):58S–69S.
56. Beattie WS, Karkouti K, Wijeysundera DN et al. Risk associated with preoperative anemia in noncardiac surgery: a single-center cohort study.Anesthesiology2009 Mar;110(3):574–581.
57. Musallam KM, Tamim HM, Richards T et al. Preoperative anaemia and postoperative outcomes in non-cardiac surgery: a retrospective cohort study.Lancet2011 Oct 15;378(9800):1396–1407.
58. Shander A. Financial and clinical outcomes associated with surgical bleeding complications. Surgery 2007 Oct; 142(Suppl. 4):S20–S25.
59. Christensen MC, Krapf S, Kempel A et al. Costs of excessive postoperative hemorrhage in cardiac surgery.J Thorac Car-diovasc Surg2009 Sep;138(3):687–693.
60. Kulier A, Levin J, Moser R et al. Impact of preoperative anemia on outcome in patients undergoing coronary artery bypass graft surgery.Circulation2007 Jul 31;116(5):471–479.
61. Murphy GJ, Reeves BC, Rogers CA et al. Increased mortality, postoperative morbidity, and cost after red blood cell transfusion in patients having cardiac surgery.Circulation2007 Nov 27;116(22):2544–2552.
62. Salim A, Hadjizacharia P, DuBose J et al. Role of anemia in traumatic brain injury.J Am Coll Surg2008 Sep;207(3):398–406. 63. Bernard AC, Davenport DL, Chang PK et al. Intraoperative transfusion of 1 U to 2 U packed red blood cells is associated with increased 30-day mortality, surgical-site infection, pneumonia, and sepsis in general surgery patients.J Am Coll Surg2009 May;208(5). 931-7, 7 e1-2; discussion 8–9.
64. Ranucci M, Aronson S, Dietrich W et al. Patient blood management during cardiac surgery: do we have enough evidence for clinical practice?J Thorac Cardiovasc Surg2011 Aug;142(2):249.e1–249.e32.
65. Ferraris VA, Davenport DL, Saha SP et al. Surgical outcomes and transfusion of minimal amounts of blood in the operating room.Arch Surg2012 Jan;147(1):49–55.
*66. Isbister JP, Shander A, Spahn DR et al. Adverse blood transfusion outcomes: establishing causation.Transfus Med Rev2011 Apr;25(2):89–101.
67. Marik PE & Corwin HL. Efficacy of red blood cell transfusion in the critically ill: a systematic review of the literature.Crit Care Med2008 Sep;36(9):2667–2674.
68. Bateman ST, Lacroix J, Boven K et al. Anemia, blood loss, and blood transfusions in North American children in the intensive care unit.Am J Respir Crit Care Med2008 Jul 1;178(1):26–33.
69. Corwin HL, Gettinger A, Pearl RG et al. The CRIT study: anemia and blood transfusion in the critically ill–current clinical practice in the United States.Crit Care Med2004 Jan;32(1):39–52.
70. Taylor RW, O’Brien J, Trottier SJ et al. Red blood cell transfusions and nosocomial infections in critically ill patients.Crit Care Med2006 Sep;34(9):2302–2308. quiz 9.
71. Malone DL, Dunne J, Tracy JK et al. Blood transfusion, independent of shock severity, is associated with worse outcome in trauma.J Trauma2003 May;54(5):898–905. discussion-7.
72. Dunne JR, Malone DL, Tracy JK et al. Allogenic blood transfusion in thefirst 24 hours after trauma is associated with increased systemic inflammatory response syndrome (SIRS) and death.Surg Infect (Larchmt)2004 Winter;5(4):395–404. 73. Marik PE & Corwin HL. Acute lung injury following blood transfusion: expanding the definition.Crit Care Med2008 Nov;
36(11):3080–3084.
74. Koch CG, Li L, Duncan AI et al. Morbidity and mortality risk associated with red blood cell and blood-component trans-fusion in isolated coronary artery bypass grafting.Crit Care Med2006 Jun;34(6):1608–1616.
75. Blair SD, Janvrin SB, McCollum CN et al. Effect of early blood transfusion on gastrointestinal haemorrhage.Br J Surg1986 Oct;73(10):783–785.
76. Hearnshaw SA, Logan RF, Palmer KR et al. Outcomes following early red blood cell transfusion in acute upper gastroin-testinal bleeding.Aliment Pharmacol Ther2010 Jul;32(2):215–224.
77. Sieunarine K, Lawrence-Brown MM, Brennan D et al. The quality of blood used for transfusion.J Cardiovasc Surg (Torino) 1992 Jan-Feb;33(1):98–105.
78. Cobain TJ, Vamvakas EC, Wells A et al. A survey of the demographics of blood use.Transfus Med2007 Feb;17(1):1–15. 79. Grey DE, Smith V, Villanueva G et al. The utility of an automated electronic system to monitor and audit transfusion
practice.Vox Sang2006 May;90(4):316–324.
80. Grey DE & Finlayson J. Red cell transfusion for iron-deficiency anaemia: a retrospective audit at a tertiary hospital.Vox Sang2008 Feb;94(2):138–142.
81. Leahy MF, Roberts HA, Mukhtar SA et al. The development of patient blood management in a Western Australian (WA) tertiary hospital.Transfusion2012;52(8). Suppl 9A.
82. CTEC. Patient blood management workshop: CTEC. The University of Western Australia. Patient blood management surgical workshop. Available from:http://www.ctec.uwa.edu.au/index.php/pbm-patient-blood-management-1621/[cited 12.10.12].
83. Goodnough LT, Shander A, Spivak JL et al. Detection, evaluation, and management of anemia in the elective surgical patient.Anesth Analg2005 Dec;101(6):1858–1861.
84. Department of Health, Western Australia. Elective joint replacement service model of care. Perth: Health Networks, Department of Health, Western Australia, 2010. Available from: http://www.healthnetworks.health.wa.gov.au/ modelsofcare/docs/Elective_Joint_Replacement.pdf.
85. Scott IA & Glasziou PP. Improving the effectiveness of clinical medicine: the need for better science.Med J Aust2012 Mar 19;196(5):304–308.
86. Scott IA & Glasziou PP. Improving effectiveness of clinical medicine: the need for better translation of science into practice. Med J Aust2012 Oct 1;197(7):374–378.
*87. Hofmann A, Farmer S & Towler SC. Strategies to preempt and reduce the use of blood products: an Australian perspective. Curr Opin Anaesthesiol2012 Feb;25(1):66–73.
88. Sixty-third World Health Assembly, Resolution WHA63.12.Availability, safety and quality of blood products2010. Available from:http://apps.who.int/gb/ebwha/pdf_files/WHA63/A63_R12-en.pdf.
89. Mukhtar SA, Leahy MF, Trentino K, et al. Effectiveness of a linked Patient Blood Management data system to monitor blood use.Anaesth Intensive Care, in press.
![Fig. 1. Modelling of the total transfusion dependency ratio (TTDR) [35] in selected countries demonstrating the potential impact of the ageing population on blood supply](https://thumb-us.123doks.com/thumbv2/123dok_us/9618834.2840768/4.701.293.622.652.902/modelling-transfusion-dependency-selected-countries-demonstrating-potential-population.webp)