How to
“
ENGAGE
”
Multilevel Learner
Groups in the Clinical Setting
Patricia D. Quigley, MD, MME, a Nicholas M. Potisek, MD, b Michael A. Barone, MD, MPHc
In many clinical settings, multiple trainees work alongside a single preceptor. Not surprisingly, there is great variability in the knowledge and skills of medical students, residents, fellows, and other health professions trainees. In such settings, it can be challenging to engage the entire team while avoiding teaching that any particular trainee would perceive as too elementary or too complex. Thus, great clinical teachers employ strategies to develop different learners’ clinical skills and independence. Unfortunately, not much information is available on this topic, and clinical teachers may only find effective teaching strategies for such multilevel learner (MLL) groups by trial and error.1–4
A quick assessment of learners’ needs and educational levels forms the foundation of teaching MLLs. When joining an inpatient team or starting a day in the outpatient clinic, the great clinical teacher finds out who are the medical, physician assistant, nursing, or therapy students and who are the interns, senior residents, or fellows. Experienced preceptors seek opportunities to talk with learners one-to-one, ask about their interests, and work with them to develop 1 or 2 specific learning goals. Great teachers ask skillful questions to gain insight into each learner’s unique experiences, knowledge base, and
adeptness with clinical reasoning.5
The reporter-interpreter-manager-educator framework may provide a useful approach to assessing a learner’s sophistication with clinical reasoning and patient care.6
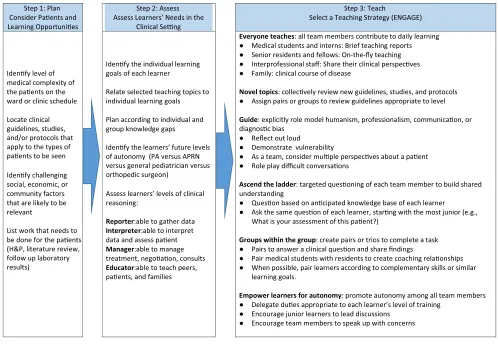
In this article from the Council on Medical Students in Pediatrics series on great clinical teachers, we offer specific strategies for teaching learners who are at different levels. The ENGAGE mnemonic (Everyone teaches, Novel topics, Guide, Ascend the ladder, Groups within the group, Empower learners for autonomy) provides preceptors with a toolbox for engaging all levels of learners (Fig 1). Throughout this article, we provide examples for teaching through an illustrative case of a 4-year-old boy presenting with symptoms of Kawasaki disease (KD).
E: EvEryonE TEachEs
Great clinical teachers set the expectation that all learners will contribute to teaching, often relating opportunities for teaching to each learner’s individualized learning goals.7 The clinical
teacher can guide learners to present succinct, clinically relevant teaching points that fill knowledge gaps for those on the team. Topics can be assigned or learners may volunteer insights from their own studying. Interprofessional staff offer unique perspectives, and
aDivision of General Pediatrics, Johns Hopkins All Children’s Hospital, St. Petersburg, Florida; bDepartment of Pediatrics, Wake Forest Baptist Medical Center, Winston-Salem, North Carolina; and cDepartment of Pediatrics, School of Medicine, Johns Hopkins University, Baltimore, Maryland
Dr Quigley conceptualized the ENGAGE mnemonic, drafted the initial manuscript, revised the manuscript, and developed Fig 1; Dr Potisek conceptualized the ENGAGE mnemonic, drafted portions of the initial manuscript, and revised subsequent versions; Dr Barone conceptualized the ENGAGE mnemonic and reviewed and revised the manuscript; and all authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
DoI: https:// doi. org/ 10. 1542/ peds. 2017- 2861 Accepted for publication Aug 23, 2017
Address correspondence to Patricia D. Quigley, MD, MME, Johns Hopkins All Children’s Hospital, Office of Medical Education, 601 5th Ave S, Saint Petersburg, FL 33701. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2017 by the American Academy of Pediatrics
FInancIaL DIscLosUrE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUnDInG: No external funding.
PoTEnTIaL conFLIcT oF InTErEsT: The authors have indicated they have no potential conflicts of interest to disclose.
patients and family members can teach about their experiences with diagnosis, treatment, and advocacy.
In our example, the 4-year-old boy initially presents to clinic. The intern, interested in pediatric rheumatology, has never cared for a child with KD. The great clinical teacher, aware of the learner’s interests and that this patient may have KD, asks the intern to evaluate the patient and review the diagnostic criteria with other learners. After the encounter, the students may teach features of incomplete KD. During the hospital admission, the inpatient team may ask pharmacy staff to teach about side effects of intravenous immunoglobulin (IVIg) and nursing staff to discuss monitoring parameters during IVIg administration. Families may provide
a narrative of the natural history of KD in their child.
n: novEL ToPIcs
Clinical teachers can introduce recent publications, hospital protocols, clinical guidelines, and new understandings of disease mechanisms or treatments. By teaching novel topics, the clinical teacher models “keeping up to date” throughout one’s career.
In our patient encounter, the teacher can compare new KD guidelines with previous versions. Junior learners could present the rationale for revisions or other aspects of the new guidelines keyed to their level of learning. During a time set aside for teaching, senior learners can analyze how the coexistence of KD and viral
infection can lead to diagnostic uncertainty.
G: GUIDE
Role modeling is a powerful teaching strategy for MLLs, particularly for harder-to-teach competencies such as professionalism and humanism. Clinical teachers might assume learners notice the way they interact with a patient, but learners, who are not primed to notice these actions, may miss them. Saying, “I said [this] to the patient because…” often helps learners notice and internalize the learning point.
For example, the clinical teacher could model family-centered care. When hearing a parent’s concerns about the risks of IVIg treatment, the clinical teacher may take an extra moment to understand and address
QuIGLEy et al 2
Quigley et al
How to “ENGAGE” Multilevel Learner Groups in the Clinical Setting
2017
https://doi.org/10.1542/peds.2017-2861
5
Pediatrics
ROUGH GALLEY PROOF
November 2017
140
Step 1: Plan Consider Paents and Learning Opportunies
Step 2: Assess Assess Learners’ Needs in the
Clinical Seng
Step 3: Teach
Select a Teaching Strategy (ENGAGE)
Idenfy level of medical complexity of the paents on the ward or clinic schedule
Locate clinical guidelines, studies, and/or protocols that apply to the types of paents to be seen
Idenfy challenging social, economic, or community factors that are likely to be relevant
List work that needs to be done for the paents (H&P, literature review, follow up laboratory results)
Idenfy the individual learning goals of each learner
Relate selected teaching topics to individual learning goals
Plan according to individual and group knowledge gaps
Idenfy the learners’ future levels of autonomy (PA versus APRN versus general pediatrician versus orthopedic surgeon)
Assess learners’ levels of clinical reasoning:
Reporter:able to gather data
Interpreter:able to interpret data and assess paent
Manager:able to manage treatment, negoaon, consults
Educator:able to teach peers, paents, and families
Everyone teaches: all team members contribute to daily learning ● Medical students and interns: Brief teaching reports ● Senior residents and fellows: On-the-fly teaching ● Interprofessional staff: Share their clinical perspecves ● Family: clinical course of disease
Novel topics:collecvely review new guidelines, studies, and protocols ● Assign pairs or groups to review guidelines appropriate to level
Guide: explicitlyrole model humanism, professionalism, communicaon, or diagnosc bias
● Reflect out loud
● Demonstrate vulnerability
● As a team, consider mulple perspecves about a paent ● Role play difficult conversaons
Ascend the ladder: targeted quesoning of each team member to build shared understanding
● Queson based on ancipated knowledge base of each learner ● Ask the same queson of each learner, starng with the most junior (e.g.,
What is your assessment of this paent?)
Groups within the group: create pairs or trios to complete a task ● Pairs to answer a clinical queson and share findings
● Pair medical students with residents to create coaching relaonships ● When possible, pair learners according to complementary skills or similar
learning goals.
Empower learners for autonomy: promote autonomy among all team members ● Delegate dues appropriate to each learner’s level of training
● Encourage junior learners to lead discussions ● Encourage team members to speak up with concerns
FIGUrE 1
Steps to ENGAGE learners in MLL setting. APRN, advanced practice registered nurse; H&P, history and physical examination; PA, physician’s assistant.
at Viet Nam:AAP Sponsored on August 28, 2020
www.aappublications.org/news
the parent’s concern rather than quoting data on the effectiveness of IVIg. Afterward, the teacher can lead a reflective discussion of the encounter. The teacher could ask the medical student to identify the differing perspectives that emerged from the conversation, the interns to reflect on how the varied perspectives converge or conflict, and/or a senior resident to walk the team through ways to reassure the worried parent, all without compromising treatment.7
a: ascEnD ThE LaDDEr
Questioning by ascending “up the ladder”8 helps the clinical teacher
target specific learning objectives for each team member. The teacher asks developmentally appropriate questions of each learner based on their needs. Initially, the teacher may ask students foundational questions, such as questions about disease pathophysiology. Building on this discussion, the clinical teacher may prompt a more experienced learner to address diagnostic and treatment options. To conclude the discussion, the most experienced learner may be asked to describe a higher-order concept, such as case synthesis.5 Questioning
requires special attention, and many recommendations for skillful questioning appear in a previous Council on Medical Students in Pediatrics article.5
In our example, the clinical teacher may ask a medical student to discuss the pharmacotherapy of KD, whereas an intern may be asked to review the rates of IVIg treatment failure. A senior resident could review treatment options available should IVIg and aspirin fail.
G: GroUPs WIThIn ThE GroUP
Establishing small groups (pairs or trios) within the larger clinical team, with each group focusing on a task,
promotes collaboration, teamwork, and leadership. Pair a senior resident with a medical student to create a coaching dyad for feedback on history and physical examinations and documentation or to staff patients in clinic. During group teaching, generate discussion and build consensus. For example, when faced with clinical uncertainty, as in refractory KD, pair learners to debate treatment options. After a brief discussion, join pairs to make a group of 4 and so on until 2 groups remain to debate and recommend treatment.
E: EmPoWEr LEarnErs For aUTonomy
Physicians and other health care providers are expected to develop increasing autonomy in caring for patients. Opportunities for autonomy are more apparent for senior learners, although there are ways to encourage autonomy among junior learners. Delegate duties appropriate to each learner’s level and skill set. For example, allow the intern in the clinic to call the inpatient team to admit the patient with KD while the senior resident coordinates bed placement. Ask junior learners to lead discussions. Remind them to speak up with concerns about patient care. Support senior learners leading rounds with and without an attending physician present.9, 10 Recognize that readiness
for autonomy does not necessarily correlate with the learner’s level in their program, and encourage learners to follow their individual trajectories.
concLUsIons
ENGAGE strategies for MLLs apply to both inpatient and ambulatory settings and will enable the great clinical teacher to meet the needs of individual learners while ensuring that patients and families receive timely and excellent care. After incorporating these strategies, the
clinical teacher will find that any setting with learners at multiple levels can become a dynamic environment in which everyone learns.
acknoWLEDGmEnTs
We thank Janice Hanson, PhD, and Robert Dudas, MD, for their thoughtful reviews of the manuscript. Dr Hanson also helped to conceptualize Figure 1.
abbrEvIaTIons
IVIg: intravenous immunoglobulin KD: Kawasaki disease MLL: multilevel learner
rEFErEncEs
1. Castiglioni A, Shewchuk RM, Willett LL, Heudebert GR, Centor RM. A pilot study using nominal group technique to assess
residents’ perceptions of successful attending rounds. J Gen Intern Med. 2008;23(7):1060–1065
2. Tariq M, Motiwala A, Ali Su, Riaz M, Awan S, Akhter J. The learners’ perspective on internal medicine ward rounds: a cross-sectional study. BMC Med Educ. 2010;10:53
3. Stickrath C, Aagaard E, Anderson M. MiPLAN: a learner-centered model for bedside teaching in today’s academic medical centers. Acad Med. 2013;88(3):322–327
4. Chen HC, Fogh S, Kobashi B, Teherani A, Ten Cate O, O’Sullivan P. An interview study of how clinical teachers develop skills to attend to different level learners. Med Teach. 2016;38(6):578–584
5. Long M, Blankenburg R, Butani L. Questioning as a teaching tool. Pediatrics. 2015;135(3):406–408
7. Lockspeiser T, Schmitter P, Lane J, Hanson J, Rosenberg A. A validated rubric for scoring learning goals. MedEdPORTAL Publications. 2013;9:9369 8. Certain LK, Guarino AJ, Greenwald
JL. Effective multilevel teaching techniques on attending rounds:
a pilot survey and systematic review of the literature. Med Teach. 2011;33(12):
e644–e650
9. Seltz LB, Preloger E, Hanson JL, Lane L. Ward rounds with or without an attending physician: how interns
learn most successfully. Acad Pediatr. 2016;16(7):638–644
10. Montacute T, Chan Teng V, Chen yu G, Schillinger E, Lin S. Qualities of resident teachers valued by medical students. Fam Med. 2016;48(5):381–384
QuIGLEy et al 4
Quigley et al
How to “ENGAGE” Multilevel Learner Groups in the Clinical Setting
2017
https://doi.org/10.1542/peds.2017-2861
5
Pediatrics
ROUGH GALLEY PROOF
November 2017
140
at Viet Nam:AAP Sponsored on August 28, 2020
www.aappublications.org/news
DOI: 10.1542/peds.2017-2861 originally published online October 10, 2017;
2017;140;
Pediatrics
Patricia D. Quigley, Nicholas M. Potisek and Michael A. Barone
How to ''ENGAGE'' Multilevel Learner Groups in the Clinical Setting
Services
Updated Information &
http://pediatrics.aappublications.org/content/140/5/e20172861
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/140/5/e20172861#BIBL
This article cites 10 articles, 1 of which you can access for free at:
Subspecialty Collections
dev_sub
http://www.aappublications.org/cgi/collection/teaching_curriculum_
Teaching/Curriculum Development
b
http://www.aappublications.org/cgi/collection/medical_education_su
Medical Education following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2017-2861 originally published online October 10, 2017;
2017;140;
Pediatrics
Patricia D. Quigley, Nicholas M. Potisek and Michael A. Barone
How to ''ENGAGE'' Multilevel Learner Groups in the Clinical Setting
http://pediatrics.aappublications.org/content/140/5/e20172861
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2017 has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
at Viet Nam:AAP Sponsored on August 28, 2020
www.aappublications.org/news