Exercise and Vascular Function in Child
Obesity: A Meta-Analysis
Katrin A. Dias, BExSSa, Daniel J. Green, PhDb,d, Charlotte B. Ingul, PhDc, Toby G. Pavey, PhDa, Jeff S. Coombes, PhDa
abstract
CONTEXT:Conduit arteryflow-mediated dilation (FMD) is a noninvasive index of preclinicalatherosclerosis in humans. Exercise interventions can improve FMD in both healthy and clinical populations.
OBJECTIVE:This systematic review and meta-analysis aimed to summarize the effect of exercise training on FMD in overweight and obese children and adolescents as well as investigate the role of cardiorespiratoryfitness (peak oxygen consumption [VO2peak]) on effects observed.
DATA SOURCES:PubMed, Medline, Embase, and Cinahl databases were searched from the earliest available date to February 2015.
STUDY SELECTION:Studies of children and/or adolescents who were overweight or obese were included.
DATA EXTRACTION:Standardized data extraction forms were used for patient and intervention characteristics, control/comparator groups, and key outcomes. Procedural quality of the studies was assessed using a modified version of the Physiotherapy Evidence Base Database scale.
RESULTS:A meta-analysis involving 219 participants compared the mean difference of pre-versus postintervention vascular function (FMD) and VO2peakbetween an exercise training
intervention and a control condition. There was a significantly greater improvement in FMD (mean difference 1.54%,P,.05) and VO2peak(mean difference 3.64 mL/kg/min,P ,.05)
after exercise training compared with controls.
LIMITATIONS:Given the diversity of exercise prescriptions, participant characteristics, and FMD measurement protocols, varying FMD effect size was noted between trials.
CONCLUSIONS:Exercise training improves vascular function in overweight and obese children, as indicated by enhanced FMD. Further research is required to establish the optimum exercise program for maintenance of healthy vascular function in this at-risk pediatric population.
a
School of Human Movement and Nutrition Sciences, The University of Queensland, St Lucia, Brisbane, Queensland, Australia;bSchool of Sport Science, Exercise and Health, The University of Western Australia, Crawley, Western Australia, Australia;cDepartment of Circulation and Medical Imaging, Norwegian University of Science and Technology, Trondheim, Norway; anddResearch
Institute for Sport and Exercise Sciences, Liverpool John Moores University, Merseyside, United Kingdom
Miss Dias and Drs Green and Coombes conceived and designed the research; Miss Dias and Dr Green acquired the data and performed statistical analysis; Drs Green and Coombes handled funding and supervision; Miss Dias and Drs Green, Ingul, and Pavey drafted the manuscript; and all authors made critical revisions of the manuscript for key intellectual content, approved thefinal manuscript as submitted, and agree to be accountable for all aspects of the work.
www.pediatrics.org/cgi/doi/10.1542/peds.2015-0616 DOI:10.1542/peds.2015-0616
Accepted for publication Jun 25, 2015
Address correspondence to Professor Jeff Coombes, School of Human Movement and Nutrition Sciences, The University of Queensland, St Lucia, QLD, Australia 4072. E-mail: [email protected]
Obesity has placed a large burden on the pediatric population over the last 30 years, with steady increases noted in several countries.1–3Pediatric
obesity is often carried into adulthood4,5and is associated with
risk factors for chronic diseases such as cardiovascular disease and type 2 diabetes.6,7Impaired vascular
function may contribute to increased cardiovascular disease risk, as atherosclerosis begins in childhood and endothelial dysfunction has been identified as an early event
contributing to the development of atherosclerosis.8There is strong
evidence that obese children and adolescents have lower arterial compliance and distensibility than their healthy matched controls, as well as depressed (2%) endothelium-dependent and -inendothelium-dependent conduit artery vasodilator function.9–12
Endothelial dysfunction is
prognostically significant, as it can predict future cardiovascular events, even after established risk factors for atherosclerosis are accounted for.13–15A meta-analysis found that
a 1% decrease inflow-mediated dilation (FMD) was associated with a 13% increase in risk of future cardiovascular events.13Retarding
atherosclerosis with early preventive measures that enhance vascular function may reduce the likelihood of future cardiovascular disease through a reduction of global cardiovascular risk.16
Previous reviews in adults found that impaired vasodilator function is improved with exercise training; however,findings are not as consistent in healthy populations with normal vascular function as they are in those with risk factors and cardiovascular disease,17,18 in part
owing to countervailing changes in vascular function and structure.19,20
The aim of this systematic review was to meta-analyze and examine the effects of exercise training on vascular function in obese children and adolescents. Changes in body
composition and cardiorespiratory fitness were also evaluated to examine the general efficacy of the exercise intervention and the relationship between
cardiorespiratoryfitness, body composition, and vascular function improvements.
METHODS
We conducted and reported this systematic review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.21
Literature Search
PubMed, Medline, Embase, and Cinahl databases were searched from the earliest available date to February 2015, limited to studies in humans and the English language. The Medical Subject Heading (MeSH) database was used to retrieve all articles related to exercise training and FMD in overweight or obese children and adolescents. MeSH terms used were“obesity”OR“overweight” OR“child”OR“adolescent”OR “atherosclerosis”and their related terms. Text words used in conjunction with the MeSH terms were (“exercise training”OR“physical training”OR“exercise”OR“exercise intervention”) AND (“arterial function”OR“vascular function”OR “vascular dysfunction”OR“fl ow-mediated dilation”OR“ endothelium-dependent dilation”). Reference lists of retrieved articles were also searched for other relevant studies.
Study Inclusion Criteria
Studies were considered eligible for inclusion if they met criteria regarding population, intervention, comparator, outcomes, and study design. Participants were required to be obese or overweight children or adolescents (according to age- and gender-specific criteria) who completed an exercise intervention using aerobic exercise training of $6 weeks in the form of a randomized controlled trial (individual or cluster).
Studies that included exercises additional to aerobic exercise training, such as resistance training or agility training, were also considered. A nonexercise comparator or control group was required for study inclusion. The measurement of FMD was necessary.
We excluded editorials, opinions, studies not published in a peer-reviewed journal, and studies available only as meeting abstracts.
Study Selection Process
All abstracts retrieved were screened, and clearly irrelevant studies were excluded. Full texts of all potentially eligible studies were examined. Supplemental Table 3 includes studies that were excluded after full-text examination. Figure 1 outlines the study selection process from initial search to inclusion.
Data Extraction
Data were extracted by using a standardized data extraction form. Patient characteristics (age, gender, and overweight/obesity
classification), intervention (exercise mode, frequency, duration, intensity, and supervision), control/comparator groups, methodological quality, and key outcomes were noted.
Corresponding authors were contacted for information not available in the journal article.
Risk of Bias Assessment
Methodological quality of all studies was assessed by 2 independent reviewers using a modified Physiotherapy Evidence Base
Database (PEDro) 10-point scale. One point was awarded for each criterion met (Fig 2). The average score was recorded when a discrepancy was noted.
Data Analysis and Synthesis Data synthesis was descriptive, with detailed tabular summaries
a quantitative summary using meta-analysis. For the secondary outcomes of weight/BMI and VO2peak, data were extracted from 6 and 3 studies,
respectively. We compared absolute changes and calculated a weighted mean difference (95% confidence interval [CI]) for each study.
Heterogeneity was investigated by reviewing study populations, methods, and interventions and by using thex2test for homogeneity and theI2statistic. Afixed-effects model for the meta-analysis was used unless statistical heterogeneity was identified (x2testP#.05 orI2$50%), for which a random effects model was used. We were unable to undertake a funnel plot for assessment of publication bias given the small number of studies meeting the criteria for meta-analysis. Analyses were conducted by using Review Manager 5.0 (Nordic Cochrane Centre, Copenhagen, Denmark).
RESULTS
Identification and Selection of Studies
The bibliographic search yielded 176 articles (Fig 1). After examining the titles and abstracts, 14 full-text articles were retrieved, with 6 identified as meeting the inclusion criteria.11,12,22–25The corresponding
authors of 4 of these 6 studies were successfully contacted for further data.11,22–24
Risk of Bias
A mean modified PEDro scale score of 8.2/10 was recorded for the 6 studies. All 6 studies satisfied the following criteria: eligibility criteria were specified, participants were randomly allocated to groups, assessors measuring the primary outcome were blinded, results of between-group statistical comparisons were reported for primary outcomes, and both point measures and measures of variability for$1 key outcome were provided. PEDro defines a key outcome as the primary measure of therapeutic effectiveness. Only 1 study reported having concealed allocation.12
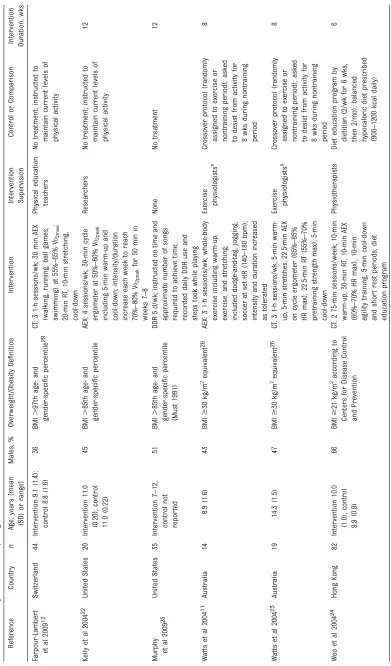
Study Characteristics
Table 1 summarizes the 6 included trials, which involved 219
participants (116 females and 103
FIGURE 1
Consolidated Standards of Reporting Trials (CONSORT) diagram of articles from initial search to inclusion. The systematic review process identified 6 articles for inclusion in the meta-analysis.
FIGURE 2
males), with 129 and 118 assigned to the exercise intervention and control groups, respectively.
Three of the 6 reviewed studies examined FMD in obese participants only,11,12,23whereas the remaining 3
studies included both overweight and obese participants.22,24,25Overweight
and obesity criteria varied, with use of the Cole dataset (2000),11,23,26
Centers for Disease Control and Prevention Growth Charts (2000),27
the Must dataset (1991),28and an
East German dataset developed by Kromeyer-Hauschild (2007).12,29
Because of the differing criteria for defining obesity, these participants were not meta-analyzed separately.
The World Health Organization defines adolescents as young people between the ages of 10 and 19 years, so 4 of the included studies involved both children and
adolescents,12,22,24,251 involved
children only,11and 1 involved
adolescents only.23Authors specified
whether the population of interest was prepubertal,11,12postpubertal,23
or mixed.22,24,25Two of the 6
investigations were conducted by the same research group at the University of Western Australia, albeit in different subjects.11,23
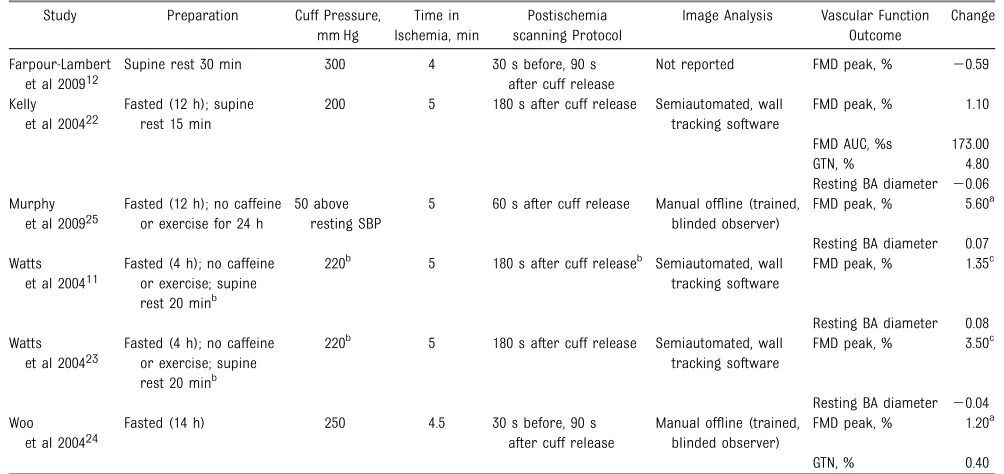
Vascular Assessment Protocols
Vascular assessment protocols varied with regard to cuff pressure, time in ischemia, ultrasound scanning duration, and timing after cuff release. All 6 protocols placed the cuff distal to the region of interest as per guidelines.30Inflated cuff pressure
ranged from 200 to 300 mm Hg, with 1 study inflating pressure to 50 mm Hg above resting systolic blood pressure.25The cuff was inflated for
5,11,22,23,254.5,24or 412minutes.
Timing of artery imaging varied, with 2 studies imaging for 30 seconds before and 90 seconds after cuff release.12,24In Kelly et al22and both
studies by Watts et al,11,23the artery
was imaged continuously for 180 seconds after cuff release, whereas Murphy et al25imaged the artery for
60 seconds after cuff release. Image analysis was performed by using automated edge detection and wall tracking software in 2
laboratories.11,22,23Farpour-Lambert
et al12did not state FMD analysis
techniques; Woo et al24and Murphy
et al25stated that scans were
analyzed offline by a trained, blinded observer, indicating that manual caliper-based analysis was used. In reporting reliability of the measure, Murphy et al25stated their laboratory
coefficient of variation for artery diameter (0.973,P,.01), whereas Woo et al24reported established FMD
coefficient of variation values, as published by Sorensen et al.31
Participant preparation varied between protocols. When participants had fasted,11,22–25fasting time ranged
from 411,23to 1424hours. Watts et al
and Murphy et al also asked participants to abstain from caffeine and exercise for 411,23and 2425hours
before testing. Additionally, 4 protocols stated that participants rested for a specified time period (15,2220,11,23and 3012minutes)
before vascular assessment.
Exercise Mode
Circuit training was used by 3 studies that incorporated aerobic exercise
TABLE 2 FMD Protocols and Outcomes
Study Preparation Cuff Pressure, mm Hg
Time in Ischemia, min
Postischemia scanning Protocol
Image Analysis Vascular Function Outcome
Change
Farpour-Lambert et al 200912
Supine rest 30 min 300 4 30 s before, 90 s after cuff release
Not reported FMD peak, % 20.59
Kelly et al 200422
Fasted (12 h); supine rest 15 min
200 5 180 s after cuff release Semiautomated, wall tracking software
FMD peak, % 1.10
FMD AUC, %s 173.00
GTN, % 4.80
Resting BA diameter 20.06 Murphy
et al 200925
Fasted (12 h); no caffeine or exercise for 24 h
50 above resting SBP
5 60 s after cuff release Manual offline (trained, blinded observer)
FMD peak, % 5.60a
Resting BA diameter 0.07 Watts
et al 200411
Fasted (4 h); no caffeine or exercise; supine rest 20 minb
220b 5 180 s after cuff releaseb Semiautomated, wall
tracking software
FMD peak, % 1.35c
Resting BA diameter 0.08 Watts
et al 200423
Fasted (4 h); no caffeine or exercise; supine rest 20 minb
220b 5 180 s after cuff release Semiautomated, wall tracking software
FMD peak, % 3.50c
Resting BA diameter 20.04 Woo
et al 200424
Fasted (14 h) 250 4.5 30 s before, 90 s after cuff release
Manual offline (trained, blinded observer)
FMD peak, % 1.20a
GTN, % 0.40
AUC, area under the curve; GTN, glyceryl trinitrate; BA, brachial artery.
aP,.01.
bCorrespondence with authors.
with other activities.12,23,24Circuit
training consisted of a combination of (1) aerobic exercise (walking, running, ball games, and swimming) with resistance training;12(2) aerobic
exercise on a cycle ergometer with resistance training;23and (3) aerobic
exercise (modality not stated) with resistance and agility training.24In 3
programs, aerobic exercise alone was performed by using (1) a cycle ergometer;22(2) activities including
dodge-and-tag, jogging, and soccer;11
and (3) Dance Dance Revolution (DDR).25Studies mostly included
a warm-up and/or cool-down period.11,12,22–24
Exercise Intensity
Aerobic exercise intensities were typically based on baseline maximal/peak testing data using a percentage of either maximal heart rate (MHR),23,24VO
2max,12or
VO2peak.22Watts et al23 prescribed a set heart rate zone (140 to 180 bpm), whereas Murphy et al25
did not specify or measure intensity of exercise performed. When
prescription involved a percentage of maximal/peak oxygen consumption, similar intensities were prescribed (55% to 65% VO2max12vs 50% to 60% VO2peak22). When MHR was used to define intensity, heart rate ranges specified were 65% to 85%23and
60% to 70%24MHR. Kelly et al22
stated that intensity was increased from 50% to 60% to“near”70% to 80% VO2peaktoward the end of the intervention. Of the 3 trials that included circuit training,12,23,24only 1
specified the intensity of the resistance training (55% to 70% of pretraining maximum strength).23
Exercise Duration
Farpour-Lambert et al12and Watts
et al11,23prescribed 60 minutes of
exercise, whereas Woo et al24used 75
minutes. Table 1 outlines the subduration of activities performed in this time. In Kelly et al,22duration
progressed from 30 to 50 minutes in the last 2 weeks, and Murphy et al25
increased duration from 10 to 30 minutes in week 5, by 5-minute increments each week.
Circuit training was used to
incorporate both aerobic exercise and resistance training. Training time of each modality varied, with ratios of 3: 2,121:3,24and 1:123(aerobic
exercise:resistance training).
Exercise Frequency
Frequency of training sessions ranged from 2 to 5 days/week, with a median of 3 days/week. Woo et al24
prescribed 2 training sessions each week, whereas Farpour-Lambert et al12and Watts et al11,23prescribed
3 training sessions each week. The remaining 2 studies prescribed training on 422and 525days per
week. The largest mean differences in FMD were seen in studies that prescribed 323and 525sessions per
week. Among the 3 interventions using a frequency of 3 weekly sessions, the mean difference in FMD varied from20.72% to 3.50%. This variation is likely due to disparities in prescribed modality, duration, and intensity between the studies. These disparities add difficulty in
attributing improvements in FMD to a particular session frequency.
Exercise Supervision
Three training programs entailed direct supervision for the duration of the intervention. This was provided
by 2 experienced physical education teachers,12researchers,22exercise
physiologists,11,23and a team of
physiotherapists.24A
self-administered home program was used in 1 study for the duration of the intervention, and participants did not receive any direct supervision.25The
researchers used a single training session to teach participants use of DDR equipment and daily logs. Daily logs recorded DDR use and steps taken while playing, which were confirmed with parental signature.
Exercise Adherence
When adherence to supervised training sessions was reported, high attendance (83% to 90%) was noted.11,12,23Murphy et al25
administered a home-training program in which adherence remained satisfactory, as 75% of participants completed sessions on 5 days per week, and 15% completed sessions on$3 days per week.
Vascular Function
Pooling the data from the 6 trials, the mean difference in FMD was 1.54% (95% CI 0.24 to 2.84), significantly favoring exercise (Fig 3).
Heterogeneity between the studies was displayed, withI2= 70%,x2test
P= .004, and was accounted for using random effects analysis.32
Watts et al11,23found that vascular
function (FMD) in obese children and
FIGURE 3
adolescents was significantly impaired relative to lean age-matched control participants (6.00%60.69% vs 12.32%63.14%,P,.0001; 5.3%6 0.9% vs 8.9%60.8%,P,.05, respectively). The improvement resulting from exercise training normalized vascular function in obese adolescents, with no significant differences seen compared with lean age-matched control participants (8.8%60.8% vs 8.9%61.5%,
P= NS).23
No significant differences were found in brachial artery baseline diameter after the exercise training
intervention.11,22,23,25Because of the
influence of vessel size on FMD response, baseline vessel diameter should remain relatively stable for valid comparisons to be
undertaken.33
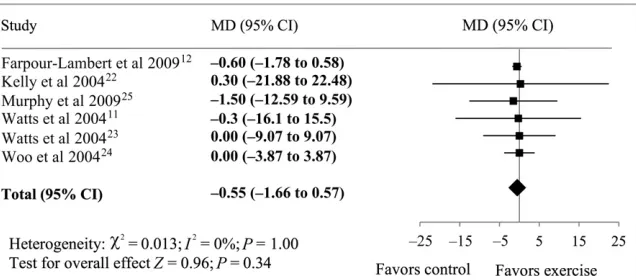
Body Composition
The mean difference in weight from the 6 studies was20.55 kg (95% CI 21.66 to 0.57), favoring exercise (Fig 4). These data were supported by a mean difference of20.14 kg/m2 (95% CI20.60 to 0.32) in BMI, favoring exercise (Fig 5). The mean differences of body composition variables were nonsignificant. The observations were homogeneous between the studies in both analyses, withI2= 0%,x2testP= 1.0 andP= .99, respectively, and therefore afixed-effects analysis was performed.32
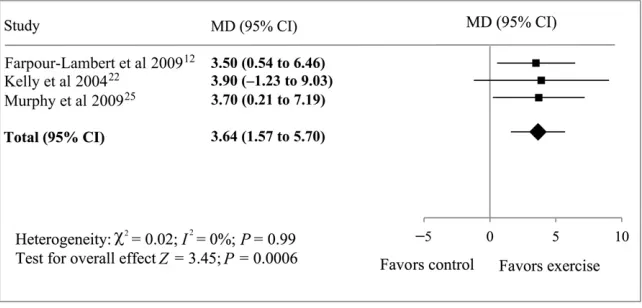
Cardiorespiratory Fitness
After pooling data from 3 studies that included maximal exercising testing and calculation of VO2peak,12,22,25the
mean difference in cardiorespiratory fitness was 3.64 mL/kg/min (95% CI 1.57 to 5.70), significantly favoring exercise (Fig 6). Again, observations were homogeneous (I2= 0%,x2test
P= .99).
DISCUSSION
The mainfinding from this meta-analysis of 219 overweight and obese children and adolescents was that exercise training instigated an improvement in endothelial function. Although exercise training had little effect on body composition,
significant increases in
cardiorespiratoryfitness were noted. Data pooling from 6 studies showed an increase of 1.54% in FMD, whereas data pooling from 3 studies showed an increase of 3.64 mL/kg/ min in cardiorespiratoryfitness.
The clinical relevance of the improvement in FMD can be assumed from previous prognostic studies. A meta-analysis of 5547 adults associated a 1% increase in FMD with a 13% decrease in cardiovascular events.13Therefore,
an improvement in FMD of 1.54% in this at-risk pediatric population would be expected to ameliorate their cardiovascular risk profile. Further reduction in risk may be
contributed by the 1-MET (metabolic equivalents) improvement in cardiorespiratoryfitness found in the analyzed studies. Myers et al34
demonstrated that in adults, every 1-MET increase in exercise capacity was associated with a 12% improvement in survival. Whereas elevated BMI, which remained unchanged over the exercise intervention, results in an increased risk of all-cause morbidity and mortality, increased
cardiorespiratoryfitness confers a reduction in this risk.35
Previous studies in adult chronic disease populations have shown that exercise training induces changes in FMD. Moderate-intensity exercise training improved endothelium-dependent function in adults with hypertension,36obesity,37diabetes,38
coronary disease,39,40and heart
failure,41whereas no changes were
observed in endothelium-independent function.42
Mechanistically, it is postulated that repetitive exposure to exercise results in upregulation of the nitric oxide dilator system.17,43The endothelium
is activated during bouts of activity owing to mechanical stimulation secondary to increased bloodflow and shear stress.19,43Improvements
in endothelium-dependent function can occur independently of
improvements in risk factors such as blood lipids, blood pressure, obesity, and glycemic control.44,45
Although exercise training has been shown to improve vascular function in both animals and humans, these changes are rapidly lost after the cessation of training.46In patients
with a recent myocardial infarction, 4 weeks of exercise training resulted in significant improvements in
endothelium-dependent dilation. However, almost complete reversal of the enhancement in endothelium-dependent dilation was reported in a time-equivalent detraining period.47
Woo et al24examined this effect in
a group of participants who withdrew
FIGURE 4
from the exercise training with a comparator group who continued to exercise until the 12-month time point. In those who withdrew, FMD returned toward baseline and was significantly lower than directly after the intervention. Even so, FMD of the exercise withdrawal group did remain superior to the control group at 1 year.
Although FMD is diminished in at-risk populations, compensation of vascular structure may occur in overweight and obese youth. Using pulse wave velocity and pulse wave analysis, Charakida et al48illustrated
that overweight and obese
children had reduced arterial stiffness compared with normal-weight children. The authors suggested that conduit artery adaptation may occur
to subdue the hemodynamic effects of adiposity.48Tryggestad et al49
proposed that increased artery compliance observed in obese children may be due to advanced growth and maturation compared with normal-weight children. Regardless, the current evidence suggests that overweight and obesity affects vascular function (FMD) and structure (stiffness) dissimilarly. It is also relevant in this context that studies have reported compensatory interrelated changes in vascular function and structure, with initial functional changes ultimately being superseded by changes in artery size and remodeling.19,20
The present meta-analysis was unable to extrapolate a relationship between
cardiorespiratoryfitness and FMD, as just 3 of the included studies conducted maximal exercise tests.12,22,25
Furthermore, the discrepancies in exercise prescription (mode, intensity, duration, and frequency) between studies add complexities when attempting to ascertain an optimal prescription. Therefore, the exact exercise prescription required to induce clinically significant improvements in FMD cannot be established until more data become available. It is also important to reinforce the competing effects of exercise on body composition and the consequent difficulty in using body weight indices such as BMI. Several studies have reported that, although body weight and BMI are not decreased by exercise training, beneficial countervailing effects occur through increases in lean body mass and decreases in fat mass.11,23We recommend that
future studies focus on the impact of exercise training on body composition, not BMI or body weight.
Limitations
Although this review does illustrate the positive impact of exercise on FMD, a measure of vascular function, the included studies had methodological limitations. Heterogeneity of the FMD measure was high (x2= 17.53,I2= 70%,P= .004), perhaps owing to varying exercise training regimens or technical preparation and analytical approaches. Although this limitation suggests that results should be interpreted with caution owing to variation in true effect sizes, statistical heterogeneity was addressed through random effects modeling within the meta-analysis. The optimum exercise training protocol to maximize health benefits in obese pediatric populations is yet to be established. As such, current research consists of varying exercise modes and intensity as well as differing session duration and
frequency. Furthermore, heterogeneity may be due to the different FMD measurement protocols used, with
FIGURE 5
Forest plot illustrating treatment effect of exercise on BMI compared with control. MD, mean difference.
FIGURE 6
evolving guidelines and technology the primary source of this
variability. Discrepancies were present in image acquisition alongside analysis techniques, ie, automated software11,22,23
compared with user-dependent manual measurements,12,24,25
which are likely to influence the outcome. A recent guidelines document was produced to overcome some of the technical difficulties between laboratories using the FMD approach.30 The
current review did not include studies of vascular structure, measured as arterial stiffness, because of a limited number of studies reporting both vascular function (FMD) and structure (arterial stiffness) measures. Furthermore, publication bias may have been introduced by limiting the meta-analysis to studies in the English language.
Whereas the mean difference of FMD% was 1.54%, this value lies within the range of variability of the different protocols. It is important to note, however, that 5 of the 6 studies reported improvements greater than the clinically significant value of 1.0%.11,22–25
Furthermore, 3 of these studies11,22,23used the gold
standard automated analysis approach, suggesting greater reliability and validity offindings.30
Most studies reviewed involved small sample sizes, with a total of 219 participants included in the meta-analysis, and male-to-female ratios were unequal in 2 of 6 studies.12,24
Differing study and participant characteristics such as chronological and maturational age are confounding factors that may have influenced FMD results. Not only did the criteria for overweight and obesity vary between reviewed studies, but 3 of 6 studies presented pooled FMD data for overweight and obese
participants, therefore restricting the meta-analysis to the entire
population. Combining overweight and obesity may result in varying stages of vascular dysfunction among the population studied. The influence of exercise at each stage of vascular remodeling and dysfunction is currently unknown. Further research concentrating on specific populations with particular exercise interventions will allow for more concise prescription guidelines to become available.
Feasibility
Strong adherence to any exercise program is required for short- and long-term efficacy. In the studies identified in this review, adherence was high, ranging from 83% to 90% in supervised programs. However, long-term adherence to the intervention was not examined, ie, whether individuals continue the exercise program after the
supervised exercise-training period. Previous examinations of the effectiveness of lifestyle
interventions in pediatric obesity suggest that these interventions are effective in improving cardiometabolic outcomes for #1 year.50Again, uncertainty surrounds
the effectiveness of such programs over a longer period of time.
Practitioners and public health officials face much difficulty in encouraging regular exercise among children and adolescents. Current worldwide data suggest that only 5% to 50% of children and adolescents are meeting physical activity guidelines (60 minutes each day), implying that permanent adoption of daily physical activity and exercise in these populations may be difficult.51–56Supervision
and enjoyment are components positively related to adherence, and consideration must be made when designing a training program. Watts et al11 designed a game-based
exercise program involving activities such as dodge-and-tag, jogging, and soccer, which resulted in a high attendance rate. Educating
children and adolescents about ways to incorporate regular exercise into daily routines may be helpful in establishing appropriate lifestyle behaviors from an early age. Large, longitudinal studies are required to further investigate this notion. Although the current evidence regarding physical activity tracking throughout life is mixed, several studies suggest that physical activity behaviors in late childhood and early adolescence can track into adulthood, emphasizing the
importance of early-life interventions.57–60
CONCLUSIONS
This meta-analysis indicates that exercise is able to induce
improvements in FMD in overweight and obese children and adolescents. The magnitude of increase (∼1.5%) would be expected to restore diminished vascular function reported in this at-risk pediatric population. This review therefore supports the notion that exercise can be used as a therapy in pediatric obesity to reverse reduced vascular function, restoring FMD to levels comparable to those observed in normal-weight children and adolescents. Considering the
heterogeneity and small sample size of this analysis, further research is warranted to establish
dose–response effects together with optimal exercise modality. Extended postintervention follow-up will ascertain the long-term sustainability of exercise in the treatment of diminished vascular function.
ABBREVIATIONS CI: confidence interval DDR: Dance Dance Revolution FMD:flow-mediated dilation MeSH: Medical Subject Heading MHR: maximal heart rate PEDro: Physiotherapy Evidence
FINANCIAL DISCLOSURE:The authors have indicated they have nofinancial relationships relevant to this article to disclose.
FUNDING:This work was supported by St Olav’s Hospital, the Norwegian University of Science and Technology (grant #9527), and the Wesley St Andrew’s Research Institute (grant #2014-01).
POTENTIAL CONFLICT OF INTEREST:The authors have indicated they have no potential conflicts of interest to disclose.
REFERENCES
1. Swinburn B, Wood A. Progress on obesity prevention over 20 years in
Australia and New Zealand.Obes Rev.
2013;14(suppl 2):60–68
2. Lobstein T, Baur L, Uauy R, IASO International Obesity TaskForce. Obesity in children and young people: a crisis in
public health.Obes Rev. 2004;5(suppl 1):
4–104
3. Ahluwalia N, Dalmasso P, Rasmussen M, et al. Trends in overweight prevalence among 11-, 13- and 15-year-olds in 25 countries in Europe, Canada and USA
from 2002 to 2010.Eur J Public Health.
2015;25(suppl 2):28–32
4. Singh AS, Mulder C, Twisk JWR, van Mechelen W, Chinapaw MJM. Tracking of childhood overweight into adulthood: a systematic review of the literature.
Obes Rev. 2008;9(5):474–488
5. Deckelbaum RJ, Williams CL. Childhood
obesity: the health issue.Obes Res. 2001;
9(suppl 4):239S–243S
6. Freedman DS, Khan LK, Dietz WH, Srinivasan SR, Berenson GS. Relationship of childhood obesity to coronary heart disease risk factors in adulthood: the
Bogalusa Heart Study.Pediatrics. 2001;
108(3). Available at: www.pediatrics.org/ cgi/content/full/108/3/e712
7. Doak CM, Visscher TL, Renders CM, Seidell JC. The prevention of overweight and obesity in children and adolescents: a review of interventions and
programmes.Obes Rev. 2006;7(1):111–136
8. Celermajer DS, Sorensen KE, Gooch VM, et al. Non-invasive detection of endothelial dysfunction in children and
adults at risk of atherosclerosis.Lancet.
1992;340(8828):1111–1115
9. Tounian P, Aggoun Y, Dubern B, et al. Presence of increased stiffness of the common carotid artery and endothelial dysfunction in severely obese children:
a prospective study.Lancet. 2001;
358(9291):1400–1404
10. Meyer AA, Kundt G, Lenschow U, Schuff-Werner P, Kienast W. Improvement of
early vascular changes and cardiovascular risk factors in obese children after a six-month exercise
program.J Am Coll Cardiol. 2006;48(9):
1865–1870
11. Watts K, Beye P, Siafarikas A, et al. Effects of exercise training on vascular
function in obese children.J Pediatr.
2004;144(5):620–625
12. Farpour-Lambert NJ, Aggoun Y, Marchand LM, Martin XE, Herrmann FR, Beghetti M. Physical activity reduces systemic blood pressure and improves early markers of atherosclerosis in
pre-pubertal obese children.J Am Coll
Cardiol. 2009;54(25):2396–2406
13. Inaba Y, Chen JA, Bergmann SR. Prediction of future cardiovascular
outcomes byflow-mediated
vasodilatation of brachial artery:
a meta-analysis.Int J Cardiovasc
Imaging. 2010;26(6):631–640
14. Green DJ, Jones H, Thijssen D, Cable NT, Atkinson G. Flow-mediated dilation and cardiovascular event prediction: does
nitric oxide matter?Hypertension.
2011;57(3):363–369
15. Ras RT, Streppel MT, Draijer R, Zock PL. Flow-mediated dilation and
cardiovascular risk prediction: a systematic review with meta-analysis.
Int J Cardiol. 2013;168(1):344–351
16. Versari D, Daghini E, Virdis A, Ghiadoni L, Taddei S. Endothelial dysfunction as a target for prevention of cardiovascular
disease.Diabetes Care. 2009;32(suppl 2):
S314–S321
17. Green DJ, Maiorana A, O’Driscoll G,
Taylor R. Effect of exercise training on endothelium-derived nitric oxide function
in humans.J Physiol. 2004;561(pt 1):1–25
18. Thijssen DHJ, Maiorana AJ, O’Driscoll G,
Cable NT, Hopman MTE, Green DJ. Impact of inactivity and exercise on the
vasculature in humans.Eur J Appl
Physiol. 2010;108(5):845–875
19. Tinken TM, Thijssen DHJ, Hopkins N, Dawson EA, Cable NT, Green DJ. Shear
stress mediates endothelial adaptations to exercise training in humans.
Hypertension. 2010;55(2):312–318
20. Tinken TM, Thijssen DHJ, Black MA, Cable NT, Green DJ. Time course of change in vasodilator function and capacity in response to exercise training in humans.
J Physiol. 2008;586(pt 20):5003–5012
21. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and
meta-analyses: the PRISMA statement.BMJ.
2009;339:b2535
22. Kelly AS, Wetzsteon RJ, Kaiser DR, Steinberger J, Bank AJ, Dengel DR.
Inflammation, insulin, and endothelial
function in overweight children and
adolescents: the role of exercise.J
Pediatr. 2004;145(6):731–736
23. Watts K, Beye P, Siafarikas A, et al. Exercise training normalizes vascular dysfunction and improves central
adiposity in obese adolescents.J Am Coll
Cardiol. 2004;43(10):1823–1827
24. Woo KS, Chook P, Yu CW, et al. Effects of diet and exercise on obesity-related vascular dysfunction in children.
Circulation. 2004;109(16):1981–1986
25. Murphy EC-S, Carson L, Neal W, Baylis C, Donley D, Yeater R. Effects of an exercise intervention using Dance Dance Revolution on endothelial function and other risk factors in overweight
children.Int J Pediatr Obes. 2009;4(4):
205–214
26. Cole TJ, Bellizzi MC, Flegal KM, Dietz WH.
Establishing a standard definition for
child overweight and obesity worldwide:
international survey.BMJ. 2000;
320(7244):1240–1243
27. Ogden CL, Kuczmarski RJ, Flegal KM, et al. Centers for Disease Control and Prevention 2000 growth charts for the United States: improvements to the 1977 National Center for Health Statistics
version.Pediatrics. 2002;109(1):45–60
percentiles of body mass index (wt/ht2)
and triceps skinfold thickness.Am J Clin
Nutr. 1991;53(4):839–846
29. Kromeyer-Hauschild K, Zellner K. Trends in overweight and obesity and changes in the distribution of body mass index in schoolchildren of Jena, East Germany.
Eur J Clin Nutr. 2007;61(3):404–411
30. Thijssen DHJ, Black MA, Pyke KE, et al.
Assessment offlow-mediated dilation in
humans: a methodological and
physiological guideline.Am J Physiol
Heart Circ Physiol. 2011;300(1):H2–H12
31. Sorensen KE, Celermajer DS, Spiegelhalter DJ, et al. Non-invasive measurement of human endothelium dependent arterial responses: accuracy and reproducibility.
Br Heart J. 1995;74(3):247–253
32. DerSimonian R, Laird N. Meta-analysis in
clinical trials.Control Clin Trials. 1986;
7(3):177–188
33. Atkinson G, Batterham AM, Thijssen DHJ, Green DJ. A new approach to improve
the specificity offlow-mediated dilation
for indicating endothelial function in
cardiovascular research.J Hypertens.
2013;31(2):287–291
34. Myers J, Prakash M, Froelicher V, Do D, Partington S, Atwood JE. Exercise capacity and mortality among men
referred for exercise testing.N Engl J
Med. 2002;346(11):793–801
35. Barry VW, Baruth M, Beets MW, Durstine JL, Liu J, Blair SN. Fitness vs. fatness on all-cause mortality: a meta-analysis.
Prog Cardiovasc Dis. 2014;56(4):382–390
36. Higashi Y, Sasaki S, Kurisu S, et al. Regular aerobic exercise augments endothelium-dependent vascular relaxation in normotensive as well as hypertensive subjects: role of endothelium-derived nitric oxide.
Circulation. 1999;100(11):1194–1202
37. Sciacqua A, Candigliota M, Ceravolo R, et al. Weight loss in combination with physical activity improves endothelial
dysfunction in human obesity.Diabetes
Care. 2003;26(6):1673–1678
38. Montero D, Walther G, Benamo E, Perez-Martin A, Vinet A. Effects of exercise training on arterial function in type 2 diabetes mellitus: a systematic review
and meta-analysis.Sports Med. 2013;
43(11):1191–1199
39. Hambrecht R, Walther C, Möbius-Winkler S, et al. Percutaneous coronary
angioplasty compared with exercise training in patients with stable coronary artery disease: a randomized trial.
Circulation. 2004;109(11):1371–1378
40. Walsh JH, Bilsborough W, Maiorana A, et al. Exercise training improves conduit vessel function in patients with coronary
artery disease.J Appl Physiol (1985).
2003;95(1):20–25
41. Maiorana A, O’Driscoll G, Dembo L, et al.
Effect of aerobic and resistance exercise training on vascular function in heart
failure.Am J Physiol Heart Circ Physiol.
2000;279(4):H1999–H2005
42. Sessa WC, Pritchard K, Seyedi N, Wang J, Hintze TH. Chronic exercise in dogs increases coronary vascular nitric oxide production and endothelial cell nitric
oxide synthase gene expression.Circ
Res. 1994;74(2):349–353
43. Maiorana A, O’Driscoll G, Taylor R, Green
D. Exercise and the nitric oxide
vasodilator system.Sports Med.
2003;33(14):1013–1035
44. Green DJ, Walsh JH, Maiorana A, Best MJ,
Taylor RR, O’Driscoll JG. Exercise-induced
improvement in endothelial dysfunction is not mediated by changes in CV risk factors: pooled analysis of diverse
patient populations.Am J Physiol Heart
Circ Physiol. 2003;285(6):H2679–H2687
45. Green DJ, Eijsvogels T, Bouts YM, et al. Exercise training and artery function in humans: nonresponse and its relationship to cardiovascular risk
factors.J Appl Physiol (1985).
2014;117(4):345–352
46. Maiorana A, O’Driscoll G, Cheetham C,
et al. The effect of combined aerobic and resistance exercise training on vascular
function in type 2 diabetes.J Am Coll
Cardiol. 2001;38(3):860–866
47. Vona M, Codeluppi GM, Iannino T, Ferrari E, Bogousslavsky J, von Segesser LK. Effects of different types of exercise training followed by detraining on endothelium-dependent dilation in patients with recent myocardial
infarction.Circulation. 2009;119(12):
1601–1608
48. Charakida M, Jones A, Falaschetti E, et al. Childhood obesity and vascular
phenotypes: a population study.J Am
Coll Cardiol. 2012;60(25):2643–2650
49. Tryggestad JB, Thompson DM, Copeland KC, Short KR. Obese children have higher
arterial elasticity without a difference in endothelial function: the role of body
composition.Obesity (Silver Spring).
2012;20(1):165–171
50. Ho M, Garnett SP, Baur L, et al. Effectiveness of lifestyle interventions in child obesity: systematic review with
meta-analysis.Pediatrics. 2012;130(6).
Available at: www.pediatrics.org/cgi/ content/full/130/6/e1647
51. Schranz N, Olds T, Cliff D, et al. Results
from Australia’s 2014 report card on
physical activity for children and youth.
J Phys Act Health. 2014;11(4 suppl 1):
S21–S25
52. Gray CE, Barnes JD, Cowie Bonne J, et al.
Results from Canada’s 2014 report card
on physical activity for children and
youth.J Phys Act Health. 2014;11(4 suppl
1):S26–S32
53. Standage M, Wilkie HJ, Jago R, Foster C, Goad MA, Cumming SP. Results from
England’s 2014 report card on physical
activity for children and youth.J Phys Act
Health. 2014;11(4 suppl 1):S45–S50
54. Liukkonen J, Jaakkola T, Kokko S, et al.
Results from Finland’s 2014 Report Card
on Physical Activity for Children and
Youth.J Phys Act Health. 2014;11(suppl
1):S51–S57
55. Dentro KN, Beals K, Crouter SE, et al.
Results from the United States’2014
report card on physical activity for
children and youth.J Phys Act Health.
2014;11(4 suppl 1):S105–S112
56. Tremblay MS, Gray CE, Akinroye K, et al. Physical activity of children: a global matrix of grades comparing 15
countries.J Phys Act Health. 2014;11
(suppl 1):S113–S125
57. Craigie AM, Lake AA, Kelly SA, Adamson AJ, Mathers JC. Tracking of obesity-related behaviours from childhood to adulthood: a systematic review.
Maturitas. 2011;70(3):266–284
58. Tammelin T, Näyhä S, Hills AP, Järvelin M-R. Adolescent participation in sports
and adult physical activity.Am J Prev
Med. 2003;24(1):22–28
59. Telama R, Yang X, Viikari J, Välimäki I, Wanne O, Raitakari O. Physical activity from childhood to adulthood: a 21-year
tracking study.Am J Prev Med. 2005;
28(3):267–273
physical activity from childhood to adulthood: the Physical Activity
Longitudinal Study.Int J Pediatr Obes.
2009;4(4):281–288
61. Kelishadi R, Hashemi M, Mohammadifard N, Asgary S, Khavarian N. Association of changes in oxidative and
proinflammatory states with changes in
vascular function after a lifestyle
modification trial among obese children.
Clin Chem. 2008;54(1):147–153
62. Huang F, del-Río-Navarro BE, de Castro GT, et al. Weight loss induced by 6-month lifestyle intervention improves early
endothelial activation andfibrinolysis in
obese adolescents.Child Care Health
Dev. 2011;37(3):377–384
63. Koncsos P, Seres I, Harangi M, et al. Favorable effect of short-term lifestyle intervention on human paraoxonase-1 activity and adipokine levels in childhood
obesity.J Am Coll Nutr. 2011;30(5):
333–339
64. Maggio AB, Aggoun Y, Martin XE, Marchand LM, Beghetti M, Farpour-Lambert NJ. Long-term follow-up of cardiovascular risk factors after
exercise training in obese children.Int
J Pediatr Obes. 2011;6(2–2):e603–e610
65. Meyer AA, Kundt G, Lenschow U, Schuff-Werner P, Kienast W. Improvement of early vascular changes and
cardiovascular risk factors in obese children after a six-month exercise
program.J Am Coll Cardiol. 2006;48(9):
1865–1870
66. Woelfle J, Roth CL, Wunsch R, Reinehr T.
Pregnancy-associated plasma protein A in obese children: relationship to markers and risk factors of atherosclerosis and
members of the IGF system.Eur J
Endocrinol. 2011;165(4):613–622
67. Kleber M, Schaefer A, Winkel K, et al.
Lifestyle intervention“Obeldicks Mini”
for obese children aged 4 to 7 years.Klin
Padiatr. 2009;221(5):290–294
68. Levent E, Ozyürek AR, Göks¸en D, Darcan S, Coker M. Effects of exercise training on vascular function in obese children.
J Pediatr. 2005;146(2):296, author reply
DOI: 10.1542/peds.2015-0616 originally published online August 10, 2015;
2015;136;e648
Pediatrics
Coombes
Katrin A. Dias, Daniel J. Green, Charlotte B. Ingul, Toby G. Pavey and Jeff S.
Exercise and Vascular Function in Child Obesity: A Meta-Analysis
Services
Updated Information &
http://pediatrics.aappublications.org/content/136/3/e648
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/136/3/e648#BIBL
This article cites 60 articles, 16 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/obesity_new_sub
Obesity
cal_fitness_sub
http://www.aappublications.org/cgi/collection/sports_medicine:physi
Sports Medicine/Physical Fitness following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2015-0616 originally published online August 10, 2015;
2015;136;e648
Pediatrics
Coombes
Katrin A. Dias, Daniel J. Green, Charlotte B. Ingul, Toby G. Pavey and Jeff S.
Exercise and Vascular Function in Child Obesity: A Meta-Analysis
http://pediatrics.aappublications.org/content/136/3/e648
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2015/08/05/peds.2015-0616.DCSupplemental
Data Supplement at:
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.