This essay was the culminating project for my Writing 101 class: Coffee and Health, taught by Professor Moskovitz. As a coffee
fiend interested in a career in medicine, this class was right up my alley, combining two of my favorite things! Little did I know, however, that we would be reading professional, scientific journal articles right from the start! As an incoming freshman with no exposure to this style of writing before, I was naturally quite intimidated. Professor Moskovitz eased us through this learning curve however, by working through strategies for researching and reading scientific articles- by the end of the semester, we were nearly pros!
For my final paper, I chose to focus on the relationship between coffee and maternal health because this field is an area of interest for me, sparked by a Biology seminar I took last fall: Ethics of Human Reproduction.
This topic proved to be challenging, as there actually aren’t conclusive data on the research topic I chose to write about! A few weeks into the assignment, as I came to this realization, I panicked and met with Dr. Moskovitz expecting to have to scrap the project altogether and start fresh. Instead, he posed brainstorm questions that got me moving on a different angle, ultimately forming the basis for this final product. This writing process was definitely the most challenging I have undergone, but was consequently the most rewarding. I hope you enjoy!
The Issue
In May 1978, the Food and Drug Administration issued a statement about the safety of caffeine consumption in the Generally Recognized as Safe Database. The notice indicated “it is inappropriate to include caffeine among the substances generally recognized as safe” based on animal studies, and called for the increased investigation of the substance with human subjects.1
The FDA report was based in part on studies that showed correlation between coffee consumption in rats and fetal malformations or spontaneous abortions.2 As these studies used only animal subjects, it would be premature to apply results directly to humans. As such, this FDA recommendation clearly indicated more research was needed before conclusions could be drawn. Media latched on to the news, however, and the public’s feeling about the drug changed perceptibly. While “75 percent of the population drank coffee in 1962… the figure dropped to 56 percent” three years after the warning was issued.3Though many additional factors may have played into this drastic drop in coffee consumption, it is a significant change nonetheless.
Today, about 83 percent of American adults drink coffee, according to the surveys published by America’s first coffee trade organization.4 Evidently, consumption rates have, for the general population, recovered and grown since the FDA statement was issued 34 years ago. Guidelines for consumption in pregnant women, however, are still vague. As such a huge population drinks coffee regularly, it is imperative that concrete advice is available for pregnant women, grounded in the evidence of human-subject studies and standardized measures of caffeine content.
Caffeinated Coffee: Contradictory Data
The first step to determining the best recommendation for pregnant women is to identify the risks that caffeine poses to a fetus. As a woman’s pregnancy progresses, her metabolism slows down, meaning that consumed chemicals have more time to pass to the fetus before being metabolized and safely excreted.5 As caffeine crosses placental tissue freely due to its high lipid solubility,6 this can
Java for Expecting
Mamas?
Can the debate on co
ff
ee consumption during
pregnancy
fi
nally be put to rest?
Emilie Melvin
Coffee and Health (Spring 2013) Professor Cary Moskovitz
increase risk of miscarriage.7 Additionally, caffeine is a vasoconstrictor; tightening
blood vessels and therefore reducing blood and oxygen flow to the placenta.8 If
severe enough, a reduced nutrient flow poses risks for growth malformations or even miscarriage to a developing fetus. Caffeine, then, may be harmful for an unborn baby, but is there a safe amount of caffeine that can be consumed without producing these effects?
Risk of biological consequences of caffeine on a pregnant woman’s body increase with the amount of coffee she drinks. In support of this claim, researchers at McGill University in Canada investigated the effect of caffeine consumption on pregnancy outcomes using a population of 331 women who had been hospitalized with a spontaneous abortion.9The researchers carried out a face-to-face interview
with each subject. They adjusted for confounding factors including smoking and drinking habits, age, and race. A strong correlation was observed between the amount of caffeine consumed and potential for spontaneous abortion - researchers found that the rate of miscarriage increased
linearly with caffeine consumption.
If adverse effects become increasingly likely as more coffee is consumed, then excessive coffee consumption should be discouraged. In striving to provide women with a concrete recommendation, the term “excessive” must be defined in terms of cups of coffee. In a study including more than 88,000 women recruited through the Danish National Birth Cohort, self-report data showed that “women who drank eight or more cups of coffee per day had twice the risk of fetal death of women who did not drink coffee.”10 There is certainly an
excessive consumption threshold, in this case defined as eight or more cups of coffee per day. When crossed, this volume of coffee is proven to generate significant negative outcomes for pregnancies. While it is intuitive that large amounts of caffeine would prove harmful, a specific threshold of eight cups moves towards the concrete recommendation that needs to be solidified for expectant mothers.
While great quantities of caffeinated coffee are harmful to a fetus, if the McGill research team proved that negative effects increase linearly with consumption, is there some limited dosage acceptable? There are in fact several well-designed studies showing no correlation between caffeine consumption and spontaneous abortion.11, 12 For example, Mills et al11, of the National Institutes of
Health, published a thorough investigation that included 431 women involved in a study of Diabetes in Early Pregnancy. Subjects were monitored beginning before the 21st day of pregnancy, and any spontaneous abortions occurring after that point were recorded. Data adjusted for smoking and drinking habits showed no statistically significant relationship between caffeine consumption and spontaneous abortion.
Data available for this topic are in direct opposition. Specifically, both Mills et al11, who determined no correlation between caffeine consumption and fetal loss,
and Infante-Rivard et al9 at McGill University, who determined that the rate of
miscarriage increased linearly with consumption, published their studies in the same year. Their contradictory results, determined from similarly designed studies with comparable sample size, give an example of how this issue proves difficult to interpret. When determining a position on an issue regarding the life of an unborn
child, however, there is no choice but to err on the side of caution: even though some well designed studies show no correlation, expecting mothers should still avoid consuming excessive caffeine to be cautious.
Combining results of the opposing studies: as risk increases linearly with consumption, and many studies show no correlation at all, essentially all of the data presented show
that consuming a low dose of caffeine is safe for expectant
mothers. Returning to the goal of defining a concrete recommendation for pregnant women, it is necessary to define the term “low dose” in terms of specific cups of coffee. After comprehensive review of available studies in 2010, the American Congress of Obstetricians and Gynecologists determined that the safe caffeine dosage is 200 mg per day,13
which is roughly 1-2 cups of coffee per day. As this is only a fraction of what some women were typically drinking before pregnancy, it is necessary
to investigate alternatives to caffeinated coffee.
Deca
ff
einated Co
ff
ee as
an Alternative
For many women, coffee each morning is part of a regular routine that is nearly impossible to change due to the habituation that occurs. Thus if caffeine has been identified as the harmful
component in coffee, can
drinking decaffeinated coffee be a viable alternative?
Compared to
research on caffeinated coffee, few studies have investigated whether decaffeinated coffee consumption is hazardous
for pregnant women.
Investigating a variable like this is challenging, as the “green light” for drinking
decaffeinated coffee is the absence of a data trend. However, the absence of data showing harm is not evidence of safety.
The only way to demonstrate that decaffeinated coffee is not harmful is to conduct controlled experiments that show no correlation, which is a weak form of evidence.
The best available data come from cohort studies
comparing the pregnancy outcomes of caffeinated versus
decaffeinated coffee drinkers. As there is a dearth of studies that meet these criteria, analyzing each study in depth is necessary to confirm sound research design. A study by University of California Berkeley researchers, published in the 1999 Epidemiology Journal, was one of the first well-executed studies to address the effects of caffeinated versus decaffeinated coffee.14 For three months in 1992, all mothers
who delivered within four counties in southern California were involved in this study. A page-long form inquiring about habits during pregnancy, including caffeinated and decaffeinated coffee consumption, was attached to birth
certificate forms. Data including birth weight and maternal
age at delivery were taken from the birth certificate itself. As with all studies on this topic, these general data were used much like an overall rating of the health of the infant. While the weight of a baby does not explicitly show good health, for a study with 7,855 participants, it is a practical and concrete
method of assessment. The researchers found no adverse
effects for decaffeinated-only consumers, while caffeinated
coffee consumers had an increased risk of preterm delivery
and fetal growth retardation. As the study had a very large sample size and data were adjusted for standard variables, this study can be viewed as sound, and its results can be accepted, indicating no adverse effects
of drinking decaffeinated
coffee on the fetus.
Similar results were
obtained through the Danish Epidemiology Centre, the organization that produced the large cohort study identifying eight cups of coffee as a harmful upper limit.15 Two years after the
previously mentioned study, researchers again enlisted participants through the
Danish National Birth
Cohort. Pregnant women who drank more than three cups of coffee a day were randomized to either the caffeinated or decaffeinated coffee group, and asked to replace their typical coffee beverage with the one provided. The coffee provided was unlabeled, so women were not aware if they were consuming decaffeinated or caffeinated coffee. After delivery, outcomes such as gestation length, birth weight, head circumference and Apgar score
were analyzed. There were no data trends demonstrating
negative effects of drinking decaffeinated coffee in this study, although it should be noted that none of the results reached statistical significance.16
Both of these studies contain design flaws that affect the credibility of their conclusions. The studies are large, observational designs that ask women to recall caffeine consumption habits during their pregnancies. Both studies use a self-report design at some phase of their investigation which is not ideal, as data accuracy is lost with this method of collection. In the UC Berkeley study specifically, the
amount of caffeine in each cup can vary greatly based preparation, so in comparing outcomes between decaffeinated and caffeinated consumers, trends cannot be confirmed with the certainty of a randomized control study.17
While a randomized controlled design, as used in the Danish study, would produce the most sound evidence, that approach is generally considered to be unethical since a harmful outcome could be anticipated from assigning participants to the caffeine control group.16Therefore, further data would need to be gleaned
from studies for which pregnancies were followed closely from the beginning, but participants were randomized to drinking decaffeinated coffee or no coffee at all, and excluding a caffeinated coffee control group.
For expectant mothers who are habituated to a few cups of coffee throughout the day, decaffeinated coffee could be a viable replacement for the caffeinated version during her nine months of pregnancy. Though the studies above indicate that drinking decaffeinated coffee does not have harmful effects on pregnancy, it must be noted that the beverage still contains trace amounts of caffeine.18 Just as excessive caffeinated coffee
drinking is unsafe during pregnancy, so is consuming excessive amounts of decaffeinated coffee. As decaffeinated coffee contains about one tenth the amount of caffeine as regular coffee, however, the term “excessive” in the case of decaf is roughly ten times larger than that of caffeinated coffee.17
Now What?
It is time to define a concrete recommendation for pregnant coffee consumers, based on a compilation of all available evidence. It has been over thirty years since the original FDA recommendation to limit coffee consumption in pregnant women was issued. Though significant investigation has occurred within this time, there is still no definitive answer on the safety of these drinks during pregnancy. Without controlled, randomized studies, however, there will most likely never be a definitive answer on this matter, and as these studies would be unethical to conduct, it is necessary to provide women with concrete recommendations based on the data that are available.
A development in August 2010 made great steps towards defining a concrete amount of coffee that is safe for pregnant women to consume. After a review of the most current studies at the time, Dr. William H. Barth, a representative for the American Congress of Obstetricians and Gynecologists (ACOG), announced that, “given the evidence, we should reassure our pregnant patients and let them know that it’s OK to have a cup of coffee.”19 Specifically, the College defines a safe level
of consumption at “moderate” - about 200 mg of caffeine per day.13 Following the
publication of this evidence, medical sites for general audiences such as WebMD and March of Dimes updated their recommendations to women to mirror the new announcement.20, 21
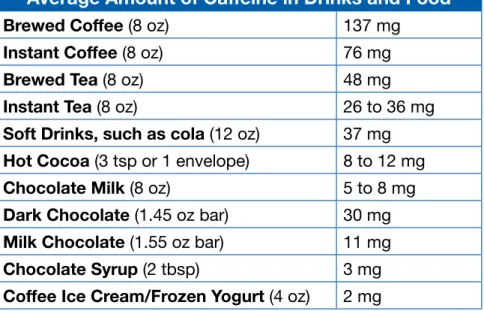
One may think that with a recommendation issued from a reputable institution, adopted by layperson medical information sites, this issue may be put to rest. While a recommendation of 200 mg of caffeine is very straightforward when applied to a can of soda or a bar of chocolate, is unhelpful in applying to cups of coffee, as preparation varies widely. It is necessary, however, to translate between the two units of measure, as well as identify the caffeine content of common foods that contain the drug. Estimates can be neatly organized in a table that is readily accessible to expectant mothers in Table 1.
This entire issue is not resolved so simply, however. According to the Center for Science in the Public Interest, 16 ounces of coffee could contain anywhere from 150-330 milligrams based on brewing method and preparation.17 Table 1 indicates
“It is time to
define a concrete
recommendation
for pregnant coffee
consumers.”
the average amount in brewed coffee is 274 milligrams, but if actual caffeine consumption can fall within such a wide range, it is impossible to determine a precise amount of coffee that is safe to drink. Therefore, though a recommendation of a maximum of 200 mg of caffeine intake per day is theoretically useful, it would only help pregnant women make informed decisions if caffeine content was standardized. Certainly, standardizing content with traditional home brewers that utilize a filter and coffee grounds is not feasible. However, the relatively new shift to single-cup coffee brewing presents a solution. Keurig introduced the first single cup coffee brewer in 1998, and is self-reportedly North America’s most popular single cup brewing system today.22 With identical pods that, when placed
in the machine, produce identical cups of coffee, caffeine content in each cup is standardized, allowing expectant mothers to know the exact amount of caffeine they are consuming. And, since in 2011, “one out of every four home coffee makers sold in the United States was a Keurig,”23 the widespread use of single cup brewing
systems as a way to standardize caffeine content may not be too far from realistic. Coming to definitive conclusions on coffee consumption is challenging due to limited methods of data collection and conflicting results. It is so important, especially when pertaining to the lives of unborn children and their mothers, to be extremely cautious in recommendations issued. The medical community should accept the ACOG’s conservative recommendation of a 200 mg maximum daily dose of caffeine. This needs to be taken even further, however: it is essential that women know precisely how to translate the 200 mg recommendation to their daily routine. A general guideline of 1-2 cups of coffee is simply too vague. With a trend of single-cup home brewing systems emerging, it is now possible to recommend that women prepare their coffee beverages in these systems, where exact caffeine content can be monitored.
Acknowledgements
I would like to thank Dr. Cary Moskovitz and Dr. Barbara Goodman for their stimulating insight and critique, as well as my Writing 101 peers for their valuable input.
Average Amount of Caffeine in Drinks and Food
Brewed Coffee (8 oz) 137 mg
Instant Coffee (8 oz) 76 mg
Brewed Tea (8 oz) 48 mg
Instant Tea (8 oz) 26 to 36 mg
Soft Drinks, such as cola (12 oz) 37 mg
Hot Cocoa (3 tsp or 1 envelope) 8 to 12 mg
Chocolate Milk (8 oz) 5 to 8 mg
Dark Chocolate (1.45 oz bar) 30 mg
Milk Chocolate (1.55 oz bar) 11 mg
Chocolate Syrup (2 tbsp) 3 mg
Coffee Ice Cream/Frozen Yogurt (4 oz) 2 mg
1. US Food and Drug Administration. CFR - Code of Federal Regulations Title 21. Available at: http:// www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?fr=182.1 180 Accessed: April 2, 2013. 2. Nolen GA. The effect of brewed and instant coffee on reproduction and teratogenesis in the rat, Toxicology and Applied Pharmacology, 1981;58(2):171-183. http://www.sciencedirect.com/science/ article/pii/0041008X8190421X#
3. Burros, M. The caffeine conflict - where does it stand? The New York Times. April 21, 1982. http://www. nytimes.com/1982/04/21/garden/the-caffeine-conflict- where-does-it-stand.html. Accessed: April 2, 2013. 4. Perez MG. Coffee consumption increases in U.S., association survey shows. Bloomberg News. http:// www.bloomberg.com/news/2013-03-22/coffee-consumption-increases-in-u-s-association-survey-shows.html Accessed April 22, 2013.
5. Babycenter. Caffeine during pregnancy. http://www.babycenter.com/caffeine-during-pregnancy. Accessed April 17, 2013.
6. Punam S, Patel BG, Patel BK. Drug use in pregnancy; a point to ponder! Indian J Pharm Sci. 2009;71(1):1–7. doi:10.4103/0250-474X.51941.
7. Belonwu, S. Coffee during pregnancy? It’s complicated... Writing 101. Duke University, Spring 2013. 8. National Institutes of Health. Vasoconstriction. MedlinePlus Encyclopedia.
http://www.nlm.nih.gov/medlineplus/ency/article/002338.htm Accessed April 20, 2013
9. Infante-Rivard C, Fernández A, Gauthier R, David M, Rivard G. Fetal loss associated with caffeine intake before and during pregnancy. JAMA. 1993;270(24):2940-2943. doi:10.1001/ jama.1993.03510240052031.
10. Bech BH, Nohr EA, Vaeth M, Henriksen TB, Olsen J. Coffee and fetal death: A cohort study with prospective data. Am. J. Epidemiol. 2005;162(10):983- 990. doi: 10.1093/aje/kwi317.
11. Mills JL, Holmes LB, Aarons JH, et al. Moderate caffeine use and the risk of spontaneous abortion and intrauterine growth retardation. JAMA. 1993;269(5):593-597. doi:10.1001/ jama.1993.03500050071028.
12. Savitz DA, Chan RL, Herring AH, Howards PP, Hartmann KE. Caffeine and miscarriage risk. Epidemiology 2008;19(1):55–62. doi:10.1097/EDE.0b013e31815c09b9`.
13. The American College of Obstetricians and Gynecologists. Moderate caffeine consumption during pregnancy. Committee opinion no. 462. American College of Obstetricians and Gynecologists. Obstet Gynecol 2010;116:467–8. http://www.acog.org/Resources_And_Publications/Committee_Opinions/ Committee_on_Obstetric_Practice/Moderate_Caffeine_Consumption_During_Pregnancy.
14. Eskenazi B, Stapleton AL, Kharrazi M, Chee WY. Associations between maternal decaffeinated and caffeinated coffee consumption and fetal growth and gestational duration. Epidemiology. 1999;10(3):242-9. http://superfund.berkeley.edu/pdf/317.pdf.
15. Bech BH, Obel C, Henriksen TB, Olsen J. Effect of reducing caffeine intake on birth weight and length of gestation: randomised controlled trial. BMJ 2007;334(7590):409. doi: 10.1136/ bmj.39062.520648.BE.
16. Jahanfar S, Jaafar SH. Effects of restricted caffeine intake by mother on fetal, neonatal and pregnancy outcome. Cochrane Database of Systematic Reviews 2009;2(1-14). Art. No. CD006965. doi:10.1002/14651858.CD006965.pub3.
17. Center for Science in the Public Interest. Caffeine content of food and drugs. http://www.cspinet.org/new/cafchart.htm. Accessed April 21, 2013.
18. Chang L, Warner J. Decaf coffee isn’t caffeine-free. WebMD. http://www.webmd.com/diet/ news/20061011/decaf-coffee-isnt-caffeine-free. Accessed April 23, 2013.
19. Barth WH. The American College of Obstetricians and Gynecologists. No Link Between Mod-erate Caffeine Consumption and Miscarriage. http://www.acog.org/About_ACOG/News_Room/ News_Releases/2010/No_Link_Between_Moderate_Caffeine_Consumption_and_Miscarriage. Ac-cessed April 17, 2013.
20. Mann D, Martin LJ. Moderate coffee drinking OK in pregnancy: New guidelines say moder-ate amounts of caffeine won’t increase miscarriage risk. WedMD. http://www.webmd.com/baby/ news/20100721/moderate-coffee-drinking-ok-in- pregnancy. Accessed April 22, 2013.
21. March of Dimes. Caffeine in pregnancy. http://www.marchofdimes.com/pregnancy/nutrition_ caffeine.html. Accessed April 22, 2013.
22. Keurig. The Keurig Story. http://www.keurig.com/the-keurig-story Accessed April 23, 2013. 23. McGinn D. The Buzz Machine: The inside story of Keurig’s rise -- a tale unlikely, ultra-caffeinated, and sometimes explosive. The Boston Globe. August 7, 2011. http://www.boston.com/business/ articles/2011/08/07/the_inside_story_of_keurig_rise_to_a_billion_dollar_coffee_empire/ Accessed April 22, 2013.
References
For more information on
using this article or others to teach and learn about effective writing, visit http://twp.duke.edu/deliberations.