Hypothalamic-Pituitary-Adrenal Function and Glucocorticoid Sensitivity
in Atopic Dermatitis
Julie A. Ellison, MRCP*; Leena Patel, MD, FRCPCH*; David W. Ray, MRCP PhD‡; Timothy J. David, MD, FRCPCH*; and Peter E. Clayton, MD, FRCPCH‡
ABSTRACT. Objectives. Topical glucocorticoids (GCs) fail to produce a clinical response in some children with atopic dermatitis (AD), suggesting that GC resistance may be present. To determine whether such resistance is gener-alized or specific to diseased skin, hypothalamic-pituitary-adrenal (HPA) axis function has been assessed in children with moderate to severe AD, who showed a variable re-sponse to treatment with topical GC.
Study Design. Thirty-five patients (.7–18.7 years old; median: 9.3 years) with AD requiring topical GCs from infancy underwent a low-dose adrenocorticotrophin hor-mone (ACTH; Synacthen) test (LDST) (500 ng/1.73 m2 ACTH). Groups 1 (7 patients), 2 (17 patients), and 3 (4 patients) used mild, moderate, or potent/very potent top-ical preparations, respectively. Group 4 (7 boys with se-vere, treatment-resistant disease) had received GC in at least 1 form (inhaledⴞintranasalⴞoral) in addition to varying potencies of topical GC. Fourteen healthy sub-jects (3.8 –17.3 years old) served as control subsub-jects. Group 4 patients had a daytime plasma cortisol profile and 08.00 hours measurement of plasma ACTH and its precursors.
Results. The response to ACTH for groups 1 and 2 did not differ from that of control subjects. Group 3 had lower peak, increment, and area under curve cortisol responses than those in controls, whereas group 4 had lower baseline, peak, and area under curve cortisol re-sponses. Eight patients failed the LDST (peak cortisol <500 nmol/L and increment <200 nmol/L): controls ⴝ 0/14, group 1 ⴝ0/7, group 2ⴝ1/17, group 3 ⴝ4/4, and group 4 ⴝ 3/7. Treatment score (based on GC potency, area treated, and duration) was the only factor to influ-ence peak cortisol response on LDST (r2ⴝ24%). In group 4, only 1 of 7 patients had a cortisol profile within the normal range but he failed the LDST. In the 5 subjects with an 08.00 hours cortisol <300 nmol/L, the matched ACTH level was inappropriately low.
Conclusions. HPA suppression was rarely found in children or adolescents with moderate to severe AD who used mild or moderately potent topical GCs over many years. However, HPA suppression was common in those receiving potent topical GC preparations or a combina-tion of GC routes of administracombina-tion. In those with severe AD, evidence of HPA suppression but lack of clinical response to GC treatment excluded significant general-ized GC resistance. This would suggest that localgeneral-ized resistance to GCs within the diseased skin may be part of
the aetiopathogenesis of severe AD.Pediatrics2000;105: 794 –799;atopic dermatitis, adrenal suppression, glucocor-ticoid sensitivity, glucocorglucocor-ticoid resistance.
ABBREVIATIONS. AD, atopic dermatitis; GC, glucocorticoid; HPA, hypothalamic-pituitary-adrenal; ACTH, adrenocorticotro-phin hormone; LDST, low-dose ACTH (Synacthen) test; IRMA, immunoradiometric assay; AUC, area under curve.
A
topic dermatitis (AD) is an inflammatory skin disorder, characterized by severe pruritis, chronically relapsing course, a typical clinical morphology, and age-related distribution of lesions.1 Treatment of AD is symptomatic and topical glu-cocorticoids (GCs) are the most widely used therapy. However, there is variable clinical response to treat-ment and although some patients improve or remain stable, a minority show little improvement.Generalized and tissue-specific GC resistance is increasingly being recognized and may be inherited or acquired.2Familial syndromes of generalized GC resistance are attributable to mutations in the GC receptor. Acquired GC resistance may result from pathophysiological processes (notably inflamma-tory) and/or may contribute to such processes by not allowing GCs to exert their physiologic effects (eg, antiinflammatory).
Some evidence from patients with asthma who do not respond to GC treatment suggests that GC resis-tance is associated with abnormal GC receptor func-tion.3 Whether acquired GC resistance, possibly in-fluenced by inflammatory mediators (such as interleukin-4), contributes to the pathophysiology of AD in patients who fail to respond to GC treatment has not yet been investigated and the molecular mechanism remains obscure.
Because some patients with severe AD show little improvement with topical GC treatment, we ques-tioned whether they had GC resistance and if so, whether this resistance was generalized or skin-specific. If the GC resistance was generalized, sys-temic effects such as hypothalamic-pituitary-adrenal (HPA) suppression would not occur with topical GC treatment, despite percutaneous absorption and po-tency of topical GC preparation to suppress HPA function. An intact HPA axis in patients on pro-longed systemic GC treatment (which would nor-mally be expected to suppress the HPA axis) would further suggest generalized GC resistance. Therefore, we examined the relationship between HPA function From the *Department of Child Health, and the ‡Endocrine Sciences
Re-search Group, University of Manchester, Manchester, United Kingdom. Received for publication Jul 2, 1999; accepted Oct 28, 1999.
Reprint requests to (J.A.E.) Pediatric Department, Leighton Hospital, Mid-dlewich Rd, Crewe, Cheshire, United Kingdom, CW1 4QJ. E-mail: [email protected]
and GC treatment with topical preparations of dif-ferent potencies as well as systemic preparations. We used the sensitive low-dose adrenocorticotrophin hormone (ACTH; Synacthen) test (LDST; 500 ng/ 1.73 m2 body surface area ACTH)4 to assess HPA function in children and adolescents being treated with topical and systemic GC preparations for AD. Systemic effects of GC were further assessed in a group of patients with severe AD who had shown minimal or no clinical response to topical and oral GC.
METHODS Subjects
Thirty-five patients (26 boys and 9 girls; .7–18.7 years old; median: 9.3; 19 prepubertal and 16 pubertal) with AD (4%– 82% body surface area affected; median: 36%) and who were attending a tertiary referral clinic were studied. All had AD requiring use of topical GC from infancy and were treated with topical GC for a median of 6.9 years (range: .5–17.7). They had a varied clinical response to treatment. Patients were grouped according to their GC use (as defined by the British National Formulary): group 1 (7 patients) only used mildly potent topical GC (1% hydrocortisone), group 2 (17 patients) used moderately potent topical GC (beta-methasone valerate [.025%], clobetasone butyrate [.05%], fluocin-olone acetonide [.00625%], and flurandrenfluocin-olone [.0125%], and group 3 (4 patients) used potent or very potent topical GC prep-arations (betamethasone valerate [.1%], clobetasol propionate [.05%], and hydrocortisone butyrate [.1%]. No patient in groups 1, 2, or 3 had received GC by any other route in the previous 6 months. Group 4 (7 patients) had received GC by⬎1 route: mild, moderate, and potent topical GC (n⫽7); inhaled GC (n⫽7); nasal GC (n⫽3); conjunctival GC (n⫽1); repeated courses of oral GC treatment (1 for asthma, 1 for AD);n⫽2), and long-term oral GC treatment (n⫽2; 1 on daily and 1 on alternate day oral GC; Table 1). All topical preparations were used twice daily but none were used under occlusion. All subjects were free of acute overt infec-tion at assessment.
The severity of AD was assessed on the day of testing, using a previously defined score,5which was obtained from the body
surface area affected, the degree of erythema, and the course of the disease over the past year. A treatment score was obtained from the potency of preparation used, the percentage body surface area treated, and the treatment duration over the past month5(Table 2).
Topical GC dose was assessed in groups 1, 2, and 3 from the reported use of topical GC by the parent: median preparation weight of mildly potent GC was 5.6 g/m2body surface area/day
(range: .3–20.2) and moderately potent GC was 2.6 g/m2body
surface area/day (range: .5–16.4).
Control Subjects
The control group consisted of 14 children (5 boys and 9 girls; 3.8 –17.3 years old; median: 10.3 years; 8 prepubertal and 6 puber-tal) being investigated for short stature. They did not have any identifiable endocrine abnormality, systemic disease, or atopy. They had never received GC by any route.
LDST
A LDST (500 ng/1.73 m2body surface area ACTH) was
per-formed after discontinuing topical GC for 24 hours (normal
re-sponse: peak plasma cortisolⱖ500 nmol/L6,7and/or increment in
plasma cortisolⱖ200 nmol/L.8,9An intravenous cannula was sited
by 10.00 hours, after use of topical anesthetic to minimize discom-fort from cannula insertion. Blood samples were taken between 14.00 hours and 15.00 hours, to coincide with the physiologic daytime low in cortisol. The ACTH test was performed in the afternoon to avoid the possible inhibitory effect of high morning basal cortisol levels on further cortisol release.10The reliability of
the LDST performed in the afternoon has been reported by Dick-stein et al6and Crowley et al.8,9Plasma cortisol samples were taken
immediately before giving the ACTH and then at⫹10, 15, 20, 25, 30, 35, 40, and 60 minutes.
The study was approved by the local research ethics committee. Written consent was obtained from all parents and from those subjects old enough to understand the study.
HPA Axis Assessment in Severe AD
Subjects
The 7 boys in group 4 had further assessment of their HPA axis function. These boys (8.0 –16.5 years old; median: 13.5; 1 prepu-bertal and 6 puprepu-bertal) had severe (severity score: 8 –9; median: 8), persistent (7–15 years; median: 13.3 years), extensive (⬎30% body surface area; median: 40%) AD from infancy. All patients received potent topical GCs at some stage in their treatment (median cur-rent treatment score: 8; range: 8 –9), with minimal or no benefit. Investigations were performed after discontinuing use of all GC preparations for 24 hours. The 7 boys had a daytime plasma cortisol profile with cortisol levels taken at 2 hourly intervals from 08.00 to 18.00 hours (normal: 08.00 hours cortisol⬎300 nmol/L; ratio of 18.00 to 08.00 hours cortisol⬍.66) and measurement of plasma ACTH (normal: .9 –11.3 pmol/L at 08.00 hours) and its precursors, pro-opiomelanocortin and pro-ACTH (normal: ⬍40 pmol/L at 08.00 hours).11Their profiles were compared with a
normal range.12
Plasma cortisol was measured by an in-house immunoradio-metric assay (IRMA) employing a solid phase second antibody separation. The intraassay coefficients of variation were 6.3%, 4.3%, and 3.7% and the interassay coefficients of variation were 8.6%, 5.5%, and 6.5% at plasma cortisol levels of 130, 410, and 750 nmol/L, respectively. ACTH and its precursors (pro-opiomelano-cortin and pro-ACTH) were measured using specific 2-site IRMAs.11,13The intraassay and interassay coefficients of variation
for both IRMAs were⬍10%.
Statistical Analysis
Continuous variables for the groups were compared using the Mann-WhitneyUtest with 95% confidence intervals. Spearman’s rank correlation was used to investigate the relationships between the parameters of the plasma cortisol response to LDST, and between these parameters and variables describing the patients’ disease severity and their treatment. The 1-samplettest was used to compare the ratio of ACTH precursor to ACTH with values for normal adults.
RESULTS Response to LDST
Groups 1 and 2: Using Mild and Moderately Potent Topical GC Preparations
There was no significant difference in the basal, peak, increment, area under curve (AUC), or
time-TABLE 1. Clinical Features for Seven Patients With Severe AD* Patient Oral GC
Treatment
Current Treatment for Asthma
Current Treatment for Allergic Rhinitis
Current Treatment for Allergic Conjunctivitis
1 No Beclomethasone (50g BD) None None
2 No Fluticasone (100g BD) Fluticasone (100g OD) None
3 No Fluticasone (250g QDS) None None
4 Multiple courses Fluticasone (250g BD) None None 5 Multiple courses Fluticasone (500g BD) None None 6 Continuous forⱖ10 y Fluticasone (250g BD) Fluticasone (100g BD) None
to-peak cortisol values for the patients using mild and moderate potency topical GC (groups 1 and 2) compared with the controls (Figs 1 and 2). One pa-tient of 17 in group 2 failed the LDST (plasma cortisol levels: baseline [130 nmol/L], peak [320 nmol/L], and increment [190 nmol/L]). He did not differ clin-ically or in topical GC use from the remainder of the group. No subjects in group 1 or the control group failed the LDST.
Group 3: Using Potent or Very Potent Topical GC Preparations
The peak, increment, and AUC cortisol responses were significantly lower in patients than in controls (P⬍ .03,P⬍.005, and P⬍.04, respectively). There were no differences in the baseline cortisol or time-to-peak cortisol values. All 4 patients failed the LDST.
Group 4: Using Topical and Inhaled⫾Intranasal⫾Oral GC Preparations
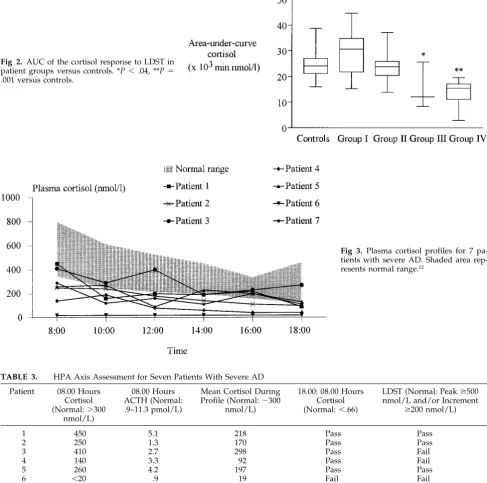
The baseline, peak, and AUC cortisol responses were significantly lower in patients than in controls (P ⫽ .01, P ⬍ .001, and P ⫽ .001, respectively). However, the increment and time-to-peak were not different (P⫽.1,P⫽.8). Three of 7 patients failed the LDST.
Correlations of Cortisol Parameters Between Subject Groups
Baseline plasma cortisol showed a significant cor-relation with both peak cortisol attained (controls:
r ⫽ .81,P ⫽ .001; patients: r⫽ .81,P ⬍ .0001) and with increment ([basal⫹peak]/2 vs increment; con-trols: r⫽ .96,P⬍.001; patients:r⫽.93,P⬍ .0001). There were no correlations between time-to-peak and the other cortisol parameters.
Correlations Between Plasma Cortisol Response to LDST and Severity of AD and Its Treatment
The severity score showed a negative correlation with baseline, peak, and AUC responses (r⫽ ⫺.36,
P⬍.04;r⫽ ⫺.46,P⬍.01; andr⫽ ⫺.36,P⬍.04). The treatment score showed a negative correlation with baseline, peak, increment, and AUC responses (r ⫽
⫺.39,P⬍.05;r⫽ ⫺.57,P⬍.0001;r⫽ ⫺.6,P⬍.0001; and r ⫽ ⫺.49, P ⬍ .01). The cortisol increment showed a weak negative correlation with the body surface area affected by AD (r ⫽ ⫺.34, P ⬍ .05). However the subject’s age, pubertal status, lifetime duration of treatment, and the current dose of mild or moderately potent topical GC showed no signifi-cant correlation with any of the cortisol parameters. In stepwise multiple linear regression, using treat-ment and severity scores, age, pubertal status, and treatment duration as independent variables, the treatment score was the only significant variable in-fluencing peak (r2⫽24%; P⫽.0016) and increment (r2⫽25%; P⫽.0014) cortisol response.
HPA Axis Function in 7 Severely Affected Patients
Cortisol Profiles
Only 2 patients had 08.00 hours cortisol levels above 300 nmol/L and only 1 patient (patient 3) had a cortisol profile within the normal range at all points (Fig 3). Median 08.00 hours plasma cortisol was 260 nmol/L (range:⬍20 – 450). However all but 1 patient had a diurnal pattern (18.00: 08.00 hours cortisol
⬍.66) to their plasma cortisol profile (Table 3). This 1 patient, treated with continuous oral GC, had severe HPA suppression with undetectable plasma cortisol during the profile (cortisol level ⬍20 nmol/L). The remaining 6 patients had a mean cortisol of 190 nmol/L (range: 92–298) during the profile. This was
TABLE 2. Clinical Characteristics of AD Patients and Healthy Control Subjects Group Age (Years)
Median (Range)
Pubertal Status
Disease Severity Score Median (Range)
Treatment Score Median (Range)
1 (n⫽7) 5.2 (4.2–16.9) 4 prepubertal/3 pubertal 6 (5–8) 6 (5–7) 2 (n⫽17) 8.3 (.7–18.7) 11 prepubertal/6 pubertal 7 (5–8) 7 (4–8) 3 (n⫽4) 6.6 (2.6–16.2) 3 prepubertal/1 pubertal 8 (5–9) 9 (9–10) 4 (n⫽7) 13.5 (8.0–16.5) 1 prepubertal/6 pubertal 8 (8–9) 8 (8–9) Controls (n⫽14) 10.3 (3.9–17.3) 8 prepubertal/6 pubertal 0 0
Fig 1. Plasma cortisol (baseline, peak, and increment) in response to LDST in patients versus controls. Data shown as median (horizontal line), 25th to 75th percentiles (box), and range (capped lines). #P⫽.01, ##P⬍.001, *
significantly lower than the mean plasma cortisol for the control group (323 nmol/L;P⫽ .005). The 08.00 hours cortisol correlated with peak (r⫽.79,P⬍.04) but not increment (P⫽ .13) response to the LDST.
ACTH and ACTH Precursors
The median plasma ACTH was 2.7 pmol/L (range: .9 –5.1), all values falling within the normal range. However, 5 of the group had an 08.00 hours cortisol below 300 nmol/L. Therefore, the ACTH values in these 5 subjects were inappropriately low. This was supported by the fact that there was no correlation between 08.00 hours ACTH and either the 08.00 hours cortisol, or peak or increment cortisol response to the LDST. The median 08.00 hours ratio of plasma ACTH precursors to ACTH was 7.8 (standard
devi-ation ⫽ 6), which did not differ from the reported normal adult value of 5.3 (standard deviation⫽.9).14
DISCUSSION
The effects of topical GCs on HPA function have been studied previously using various methods but with contradictory results.15–20 Using the sensitive LDST, we found that long-term use of mild and moderately potent topical GC in prepubertal chil-dren with moderate or severe AD was rarely associ-ated with HPA suppression, confirming the findings of a previous study.5 In addition, we have now shown that this holds for similarly affected pubertal children. Potent/very potent topical GCs reduce the need for oral GC therapy in treatment-resistant AD and are usually used on a short-term basis. In our
Fig 2. AUC of the cortisol response to LDST in patient groups versus controls. *P⬍.04, **P⫽
.001 versus controls.
Fig 3. Plasma cortisol profiles for 7 pa-tients with severe AD. Shaded area rep-resents normal range.12
TABLE 3. HPA Axis Assessment for Seven Patients With Severe AD
Patient 08.00 Hours Cortisol (Normal:⬎300
nmol/L)
08.00 Hours ACTH (Normal: .9–11.3 pmol/L)
Mean Cortisol During Profile (Normal:⬃300
nmol/L)
18.00: 08.00 Hours Cortisol (Normal:⬍.66)
LDST (Normal: Peakⱖ500 nmol/L and/or Increment
ⱖ200 nmol/L)
1 450 5.1 218 Pass Pass
2 250 1.3 170 Pass Pass
3 410 2.7 298 Pass Fail
4 140 3.3 92 Pass Fail
5 260 4.2 197 Pass Pass
6 ⬍20 .9 19 Fail Fail
study, all 4 patients using potent topical GCs (group 3) failed the LDST. Rate of HPA recovery after dis-continuing long-term potent topical treatment was assessed and found to be markedly prolonged in 2 patients.
Our patients reported a wide dose range for topi-cal GC treatment. The poor reliability of the assess-ment of drug use by history is a limitation. Topical GC preparations are categorized into different po-tency groups by the vasoconstrictor (ie, skin blanch-ing) assay. However, this is subjective and does not correlate perfectly with clinical antiinflammatory ef-fects, percutaneous absorption, or propensity for ad-verse effects. Currently, there is no reliable and ac-cessible method available for expressing GC potency in a better way.
Because topical GCs have been shown to impair HPA function, treatment scores might be expected to show an inverse correlation with cortisol responses to LDST, and this was shown in our study. Severity scores also correlated inversely with basal, peak, and AUC cortisol responses.
Of the 7 patients with severe treatment-resistant disease and who were also receiving GC by⬎1 route, those who failed the LDST were not clinically dis-tinct from those who passed. However, all had some evidence of HPA suppression. In addition, all had normal 08.00 hours ACTH levels, but none had a raised level despite low circulating plasma cortisol levels. Because exogenous GCs suppressed both hy-pothalamic corticotrophin-releasing hormone and pituitary ACTH secretion, these inappropriately low ACTH levels suggest central HPA axis suppression. The normal ratio of plasma ACTH precursors to ACTH of patients in this group suggests that ACTH precursor synthesis is impaired in response to GC therapy, implying chronic central HPA axis suppres-sion. These patients have biological evidence of chronic GC excess and so are especially vulnerable to systemic GC side effects. Two patients who used potent topical GCs developed skin atrophy, whereas 1 other subject (patient 6), on continuous oral GC, had cushingoid facies, truncal obesity, skin atrophy, striae, and severe osteoporosis, with a pathologic fracture.
In the severely affected patients in group 4, lack of clinical response in the presence of central HPA axis suppression excludes significant generalized resis-tance to GC and suggests localized resisresis-tance in the skin. Alternatively, it is possible that GC resistance may involve another site. Clayton et al21have shown that patients with AD have reduced GC receptor-binding affinity in peripheral blood mononuclear cells, suggesting that this was an acquired defect that may result from on-going immune activation and increased cytokine generation. Because patients had unremitting disease from infancy, it is likely that the GC-resistant patients were resistant from the incep-tion of their disease. Studies examining the natural history of AD suggest that AD symptoms frequently resolve as the patient gets older.22 Although resis-tance is suggested by failure of AD to resolve with age, it is not possible to predict early in the course of the disorder which patient is likely to have resistant
disease. Both lifetime prevalence and period preva-lence are higher in boys than girls and might explain why there were only males in the most resistant group (group 4). There was no relationship between severe disease and family history of atopy.
This study has demonstrated that mild and mod-erately potent topical GCs very rarely cause adrenal suppression in prepubertal or pubertal subjects with AD. However, impaired function of the HPA axis is common in those receiving potent topical GCs or combinations of GC treatment. Subjects with severe GC-resistant disease have central HPA axis suppres-sion, implying that the GC resistance is specific to their skin disease. This suggests that GC treatment resistance may be part of the aetiopathogenesis of severe AD. Children treated with potent topical GCs or with combination GC therapy should be moni-tored for HPA axis suppression and may require GC replacement, particularly at times of acute stress.
ACKNOWLEDGMENTS
We thank Dr Anne White, School of Biological Sciences, Uni-versity of Manchester, for ACTH and precursor peptide assays; Dr G. M. Addison, Manchester Children’s Hospital Trust, Manches-ter, for cortisol assays; and Drs C. J. De Vile and R. Stanhope, Institute of Child Health, London, for permission to reproduce their normal range data for the cortisol profile.12
REFERENCES
1. Hanifin JM, Rajka G. Diagnostic features of atopic dermatitis.Acta Derm Venereol. 1980;92:44 – 47
2. Ray DW. Molecular mechanisms of glucocorticoid resistance.J Endocri-nol. 1996;149:1–5
3. Barnes PJ, Adcock IM. Steroid resistance in asthma.Q J Med. 1995;88: 455– 468
4. Patel L, Clayton PE. Clinical usefulness of the low dose ACTH test.J Endocrinol Invest. 1999;22:401– 404
5. Patel L, Clayton PE, Addison GM, Price DA, David TJ. Adrenal function following topical steroid treatment in children with atopic dermatitis. Br J Dermatol. 1995;132:950 –955
6. Dickstein G, Shechner C, Nicholson W, Rosner I, Shen-Orr Z, Lahav M. Adrenocorticotropin stimulation test: effects of basal cortisol level, time of day, and suggested new sensitive low dose test.J Clin Endocrinol Metab. 1991;72:773–778
7. Tordjman K, Jaffe A, Grazas N, Apter C, Stern N. The role of the low dose (1g) adrenocorticotropin test in the evaluation of patients with pituitary diseases.J Clin Endocrinol Metab. 1995;80:1301–1305 8. Crowley S, Hindmarsh PC, Holownia P, Honour JW, Brook CGD. The
use of low doses of ACTH in the investigation of adrenal function in man.J Endocrinol. 1991;130:475– 479
9. Crowley S, Hindmarsh PC, Honour JW, Brook CGD. Reproducibility of the cortisol response to stimulation with a low dose of ACTH (1–24): the effect of basal cortisol levels and comparison of low-dose with high-dose secretory dynamics.J Endocrinol. 1993;136:167–172
10. Stewart PM, Corrie J, Seckl JR, et al. A rational approach for assessing the hypothalamic-pituitary-adrenal-axis.Lancet. 1988;1:1208 –1210 11. Crosby SR, Stewart MF, Ratcliffe JG, White A. Direct measurement of
the precursors of adrenocorticotropin in human plasma by two-site immunoradiometric assay.J Clin Endocrinol Metab. 1988;67:1272–1277 12. DeVile CJ, Stanhope R. Hydrocortisone replacement therapy in children
and adolescents with hypopituitarism.Clin Endocrinol. 1997;47:37– 41 13. White A, Smith H, Hoadley M, Dobson SH, Ratcliffe JG. Clinical
eval-uation of a two-site immunoradiometric assay for adrenocorticotrophin in unextracted human blood using monoclonal antibodies.Clin Endo-crinol. 1987;26:41–52
14. Ray DW, Gibson S, Crosby SR, Davies D, Davis JRE, White A. Elevated levels of adrenocorticotropin (ACTH) precursors in post-adrenalectomy Cushing’s disease and their regulation by glucocorticoids.J Clin Endo-crinol Metab. 1995;80:2430 –2436
16. Carr RD, Belcher RW. Adrenocortical suppression with small doses of topical corticosteroids.Acta Derm Venereol. 1969;49:508 –513
17. Feiwel M, James VHT, Barnett ES. Effect of potent topical steroids on plasma cortisol levels of infants and children with eczema.Lancet. 1969;1:485– 487
18. Rasmussen JE. Percutaneous absorption of topically applied triamcin-olone in children.Arch Dermatol. 1978;114:1165–1167
19. Weston WL, Sams JWM, Morris HG, Arthur JM, Blakeman GJ, Andre-sen M. Morning plasma cortisol levels in infants treated with topical fluorinated glucocorticosteroids.Pediatrics. 1980;65:103–106
20. Turpeinen M. Adrenocortical response to adrenocorticotropic hormone in relation to duration of topical therapy and percutaneous absorption of hydrocortisone in children with dermatitis.Eur J Pediatr. 1989;148: 729 –317
21. Clayton MH, Leung DYM, Surs W, Szefler SJ. Altered glucocorticoid receptor binding in atopic dermatitis.J Allergy Clin Immunol. 1995;96: 421– 423
22. Herd RM, Tidman MJ, Prescott RJ, et al. Prevalence of atopic eczema in the community: the Lothian atopic dermatitis study.Br J Dermatol. 1996;135:18 –19
EMINENCE-BASED MEDICINE
The more senior the colleague, the less importance he or she placed on the need for anything as mundane as evidence. Experience, it seems, is worth any amount of evidence. These colleagues have a touching faith in clinical experience, which has been defined as “making the same mistakes with increasing confidence over an impressive number of years.” The eminent physician’s white hair and balding pate are called the “halo” effect.
Isaacs D, Fitzgerald D. Seven alternatives to evidence-based medicine.Br Med J.1999;319:1618
DOI: 10.1542/peds.105.4.794
2000;105;794
Pediatrics
Clayton
Julie A. Ellison, Leena Patel, David W. Ray, PhD?; Timothy J. David and Peter E.
Atopic Dermatitis
Hypothalamic-Pituitary-Adrenal Function and Glucocorticoid Sensitivity in
Services
Updated Information &
http://pediatrics.aappublications.org/content/105/4/794 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/105/4/794#BIBL This article cites 22 articles, 4 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/coding_corner
Coding Corner
http://www.aappublications.org/cgi/collection/dermatology_sub
Dermatology
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.105.4.794
2000;105;794
Pediatrics
Clayton
Julie A. Ellison, Leena Patel, David W. Ray, PhD?; Timothy J. David and Peter E.
Atopic Dermatitis
Hypothalamic-Pituitary-Adrenal Function and Glucocorticoid Sensitivity in
http://pediatrics.aappublications.org/content/105/4/794
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.