A Model of Interpersonal Trust, Credibility, and
Relationship Maintenance
Bryan Sisk, MD,aJustin N. Baker, MDb
I wasn’t upset by my child’s bad reaction to the treatment. I was upset because no one told me it was a possibility beforehand.
I don’t think our doctor looked at us during the entire visit. She just kept typing away.
I couldn’t get in touch with my child’s medical team for three days after the scans. I just had to sit around and worry until the nursefinally returned my calls.
Trust is essential to the clinician-family relationship in pediatrics, and it is affected by the actions or inactions of clinicians. High levels of trust can support confidence, peace of mind, and a sense of security. Broken trust can lead to anxiety, second-guessing, and frustration. In these opening statements, parents describe lapses in clinicians’honesty,fidelity, and caring that impaired their trust. Mounting evidence suggests that the US health care system is entering into a crisis of trust, with Americans reporting decreased trust in physicians and the health care system over the last half century.1
In 2014, a report found that only 58% of American patients agreed that doctors could be trusted, ranking 24th among all countries surveyed.1Lee et al2argued that this erosion of trust has resulted from the
deprioritization of relationships in modern US health care, and they recommended a framework for increasing trust between patients and health care organizations or health care teams. Although this
organizational trust is important, we argue that interpersonal trust in pediatrics between each family and clinician is paramount. Every clinician has an opportunity to reinforce or hinder the family’s trust in the clinician, the hospital, and the greater health care system.
Interpersonal trust is a complex topic that is understudied in the medical literature, and this work is almost absent from the pediatric literature. Understanding trust in the pediatric setting is even more challenging given the triadic nature of communication between child, parent, and clinician. As children and adolescents develop autonomy, supporting their voice becomes even more important to developing a trusting relationship. Although many studies have used“trust in the physician”as an outcome measure, few studies have evaluated the determinants, outcomes, and evolution of interpersonal trust between clinicians and patients. In this
aDivision of Hematology and Oncology, Department of Pediatrics,
School of Medicine, Washington University, St Louis, Missouri; and
bDivision of Quality of Life and Palliative Care, Department of Oncology,
St. Jude Children’s Research Hospital, Memphis, Tennessee
Drs Sisk and Baker both conceptualized, drafted and revised, and approved thefinal manuscript as submitted.
DOI:https://doi.org/10.1542/peds.2019-1319 Accepted for publication May 23, 2019
Address correspondence to Bryan Sisk, MD, Department of Pediatrics, Washington University School of Medicine, 4523 Clayton Ave, Campus Box 8005, St Louis, MO 63110. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2019 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE:The authors have indicated they have nofinancial relationships relevant to this article to disclose.
FUNDING:Supported in part by the National Center For Advancing Translational Sciences of the National Institutes of Health under award number UL1 TR002345 (Dr Sisk). Funded by the National Institutes of Health (NIH).
POTENTIAL CONFLICT OF INTEREST:The authors have indicated they have no potential conflicts of interest to disclose.
To cite:Sisk B and Baker JN. A Model of Interpersonal Trust, Credibility, and Relationship Maintenance.
Pediatrics. 2019;144(6):e20191319
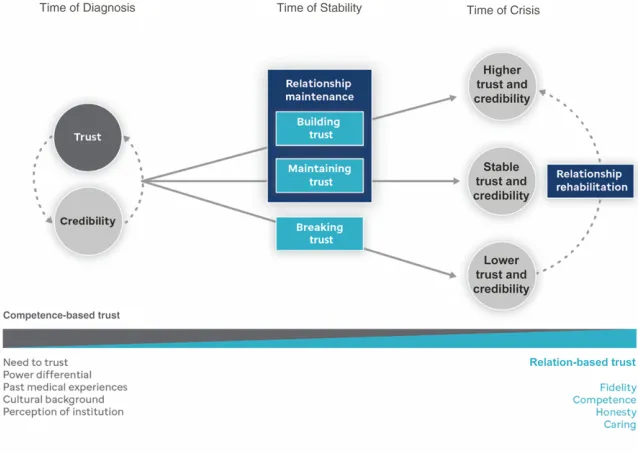
limited literature, most studies have been focused on trust during times of crisis rather than times of stability, and none have been focused on pediatrics. However, we argue that trust is more impactful if established and maintained before times of crisis. As such, we propose a model of trust evolution in the clinical relationship, a model that calls for increased attention to relationship maintenance over time (Fig 1). This model was informed by currentfindings from the trust literature and clinical
experiences.
We consider trust to have the following features: (1) making a prediction about future behaviors of others, (2) holding positive
expectations that the trustee will perform a valued behavior, (3) being vulnerable to the actions of the trustee.3In pediatrics, the family develops some level of trust in the clinician, and the clinician
demonstrates credibility or trustworthiness over time through actions. The family’s interpretation of the clinician’s actions modulates this level of trust in a continuing cycle.
When a familyfirst encounters a clinician, their level of trust is based largely on preconceived assumptions about the clinician’s competence, so called competence-based trust.4
Contributors to this initial
competence-based trust can include the family’s need to trust the clinician due to lack of other options and the inherent power differential in the relationship, as well as the family’s cultural background, past experiences within the health care system, perceptions of the particular institution, and personal biases. As such, clinicians have little active role in determining their initial credibility with the family, but their actions will determine the
longitudinal trajectory of this trust and credibility.
Families test their clinicians over time against their expectations of what clinicians should do.5As the clinical relationship develops, the family’s trust becomes increasingly contingent on the clinician’s demonstrated actions, which we call relation-based trust. Studies suggest that relation-based trust is supported by
demonstrations of caring,fidelity, honesty, and competence.4
In this model, we hypothesize that relationship maintenance is integral to maintaining and building trust over time. By relationship
maintenance, we mean consistently acting in ways that demonstrate caring,fidelity, honesty, and competence, thus demonstrating credibility and further supporting trust. However, the natural history of trust and credibility has not been
firmly established in pediatrics nor is there evidence to support specific relationship maintenance practices. Common sense suggests that the following efforts might have sustaining effects on trust. Visiting a family when their child is
hospitalized, personally and promptly calling with imaging results, or visiting briefly during follow-up appointments even if they are being seen by a different clinician might signal caring. Following through on promises from the previous clinic visit (eg,“I will type up a treatment summary”or“I will contact your primary pediatrician”) might demonstratefidelity. Providing truthful prognostic information in a sensitive manner can demonstrate honesty. Demonstrating knowledge and communicating in
understandable words and phrases can signal competence. Attention to a respectful and thorough physical examination might demonstrate caring and competence.
These are simple (but not easy) approaches. Although none will be a panacea, together, such approaches might show that the clinician respects the patient and family and will provide safe and effective care. Yet, the success of these interventions hinges on the clinician’s awareness of the patient’s and family’s needs and commitment to addressing them.
Despite good intentions, sometimes trust can break. This break might result from insufficient relationship
FIGURE 1
Model of trust and relationship maintenance. For most families, a time of crisis will transition (at least temporarily) to a time of stability. Thisfigure represents 1 iteration of this cycle.
maintenance, medical or communication errors, adverse events, or (often) some combination of these contributors. When trust is diminished or broken, the clinician should take steps to re-establish credibility and rehabilitate the relationship. Again, these efforts would ideally take place before crises, but breaks in trust might not become apparent until the relationship is strained by clinical circumstances. Clinicians in this situation can borrow concepts from the conflict resolution literature to realign with the family. This literature suggests that communication efforts should be focused on identifying the family’s underlying interests, seeking their truth, and recognizing anger as a reactive emotion.6Although this approach was developed for ethics consultations, we have found these approaches to be effective in the clinical setting when trust has been damaged. This type of communication is often uncomfortable for clinicians and requires preparation and practice. An apology can also help to defuse situations and humanize the clinician but only if sincere. Additionally, clinicians
should recognize that trust from the parents does not necessarily indicate trust from the pediatric patient and vice versa. Clinicians interested in bolstering their communication skills might consider online courses or modules, such as VitalTalk, DocCom, or I*CARE, among others.
Without trust, relationships languish, and clinicians cannot provide all the care that patients and families need. Our model of trust evolution proposes that contributors to trust change over time, and necessary interventions to bolster trust must also vary by time and context. However, too much of this critical process relies on common sense rather than evidence, especially in pediatrics. More work is needed to understand how clinicians can affect this process positively and negatively. Future research should aim to characterize the inputs and outcomes of relationship maintenance and relationship rehabilitation. In the meantime, clinicians should reflect on their clinical experiences (and perhaps their own experiences as
patients) to identify ways to demonstrate their caring,fidelity, honesty, and competence to patients and families.
REFERENCES
1. Blendon RJ, Benson JM, Hero JO. Public trust in physicians--U.S. medicine in international perspective.N Engl J Med. 2014;371(17):1570–1572
2. Lee TH, McGlynn EA, Safran DG. A framework for increasing trust between patients and the organizations that care for them.JAMA. 2019;321(6): 539–540
3. Hillen MA, de Haes HC, Smets EM. Cancer patients’trust in their physician-a review.Psychooncology. 2011;20(3):227–241
4. Hillen MA, Onderwater AT, van Zwieten MC, de Haes HC, Smets EM.
Disentangling cancer patients’trust in their oncologist: a qualitative study.
Psychooncology. 2012;21(4):392–399
5. Mechanic D, Meyer S. Concepts of trust among patients with serious illness.
Soc Sci Med. 2000;51(5):657–668
6. Fiester A. Contentious conversations: using mediation techniques in difficult clinical ethics consultations.J Clin Ethics. 2015;26(4):324–330
DOI: 10.1542/peds.2019-1319 originally published online November 13, 2019;
2019;144;
Pediatrics
Bryan Sisk and Justin N. Baker
A Model of Interpersonal Trust, Credibility, and Relationship Maintenance
Services
Updated Information &
http://pediatrics.aappublications.org/content/144/6/e20191319 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/144/6/e20191319#BIBL This article cites 6 articles, 0 of which you can access for free at:
Subspecialty Collections
dicine_sub
http://www.aappublications.org/cgi/collection/hospice:palliative_me Hospice/Palliative Medicine
http://www.aappublications.org/cgi/collection/ethics:bioethics_sub Ethics/Bioethics
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml Information about ordering reprints can be found online:
at Viet Nam:AAP Sponsored on August 28, 2020
www.aappublications.org/news
DOI: 10.1542/peds.2019-1319 originally published online November 13, 2019;
2019;144;
Pediatrics
Bryan Sisk and Justin N. Baker
A Model of Interpersonal Trust, Credibility, and Relationship Maintenance
http://pediatrics.aappublications.org/content/144/6/e20191319
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2019 has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
at Viet Nam:AAP Sponsored on August 28, 2020
www.aappublications.org/news