Original Article
Risk factors for persistent diarrhea
Eduardo Sagaro
ABSTRACT
In the last years the literature related to persistent diarrhea (PD) has decreased in a very alarming way. The WHO has called attention to the lack of information on the protracted episodes of diarrhea, and has invited all researchers to obtain and provide information on this problem. PD is one of the diseases that frequently affects morbidity and mortality of children in the world. There are approximately 3 million diarrhea related deaths per year of children less than 5 years old. Forty five percent of these deaths are due to episodes that last more than 14 days. PD represents an important health problem because its magnitude, significance and long duration. A review of the main risk factors for PD is reviewed in this article. Research to identify risk factors for PD is a priority. The identification of such risk factors is basic for the understanding of the pathogenesis and epidemiology of PD. Knowledge of these risk factors in any country is of vital importance for the strategy to prevent and control PD. This strategy must be comprehensive and effective to reduce the rate of mortality related to diarrheal diseases in general and infant mortality in particular. Risk factors for PD are of two kinds: a) Environmental social and b) Host. The most important host related risk factors for PD are: i. age, ii. previous episodes of acute and PD, iii. malnutrition, iv. early introduction of animal milk, v. the use of metronidazol and antibiotics during the acute phase of the disease, and vi. the identification of enteric pathogens.
INTRODUCTION
P
ersistent Diarrhea (PD) is a disease that seriously affects the morbidity and mortality of children in the world.1 PD is not only a disease or affection of the intestinal tract; it is also an important nutritional risk factor for the development and worsening of the vicious circle of diarrhea-malnutrition-infection in our country,2 in the majority of the developing countries,3 and in many developed countries. PD is a chronic disease very easy to diagnose. The interrogation of the mother and the physical examination of the patient make the diagnosis with certainty and confidence. With the current scientific knowledge it is possible to provide therapeutic, nutritional and pharmacological measures that will permit the successful control of the PD and will contribute to avoid the complications that are so frequent in this affection.PD can be classified at the same time as a disease and a nutritional risk factor. It is an important far reaching health problem because of its magnitude (high prevalence in children population), significance (an important cause of infant mortality) and long duration (more than 14 days, that requires medical assistance and control during this time). It is enormous the field for research in PD.
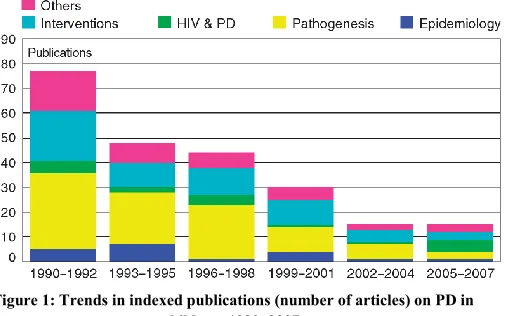
In the last years the literature related to the diagnosis, microbiology and nutritional treatment of PD has decease in a very alarming way. The WHO has called the attention on the lack of information on the protracted episodes of diarrhea, and has invited all researchers to obtain and provide information on the problem4 that is still a main cause of infant mortality in developing countries (Figure 1).
There are approximately 3 million diarrheal related deaths per year of children less than 5 years old. The use of oral rehydration salts has diminished dramatically the mortality by
International Journal of
Gastroenterology, Hepatology,
Transplant & Nutrition
Consultant Professor of Pediatrics, Pediatric Gastroenterologist, Pediatric Hospital “Juan Manuel Marquez”, Havana, Cuba
Address for Correspondence Dr. Eduardo Sagaro
E-mail: [email protected]
Access this article online QR Code
Website: www.journal.pghtn.com
acute diarrhea. The 45% of the deaths related to diarrhea are due to episodes that last more than 14 days.5
Figure 1: Trends in indexed publications (number of articles) on PD in children, 1990–2007.
Prevention has a prominent role in PD. Mothers education and the care that a sick child needs are basic pillars of it. The prevention of PD is only possible if the risk factors are known in detail, and as a consequence, a strategy is planned. The prediction of the risk to PD is also a fascinating chapter in the knowledge of this disease.
DEFINITIONS
As a result of confusion created by multiple classifications, it is important to consider some definitions.
Diarrhea. It is defined as an increase in the volume, in the liquid content and/or the frequency of the stools associated with changes of it consistency. According with the WHO diarrhea is the passage of unusually loose or watery stools, at least three times in a 24 hour period. A diarrheal episode is when the previous criteria is fulfilled and it ends when the last day with diarrhea is followed at least with 48 hours with normal stools.
Persistent diarrhea. It is defined as multiple diarrheal episodes that start acutely, last for 14 days or more and is usually associated with growth faltering. Unlike acute diarrhea, in which dehydration is the chief contributor to mortality, PD has multiple and diverse adverse effects on childhood outcomes, including micronutrient deficiencies,6 stunting, and cognitive impairment. It is an important contributor to morbidity and mortality of other diseases. Operationally persistent diarrhea is a diarrheal episode that lasts 14 days or longer. The main complications are malnutrition and serious non-intestinal infections. Dehydration may also occur.
These criteria identify children with a considerably bigger diarrheal burden and an increase in the rate of deaths related to diarrhea. The etiology of PD is in the majority of the cases of infectious nature and is caused by the same pathogen that originated the acute episode or by another of new acquisition.
The diarrheal episode becomes persistent when it is complicated with sugar or protein intolerance and malnutrition, that most of the time is favored by a inadequate management of the diarrheal episode.7
The majority of the cases with PD in developing countries are of post infectious nature. Children with PD may not represent a different subgroup, but instead they are part of a continuous in the tendency to diarrhea.
PD should be differentiated with other chronic diarrheal syndromes.
In contrast to PD in developing countries that are in the majority of the cases of infectious etiology, some children in developed countries may present severe prolonged diarrhea related mainly with congenital defects of the digestion and absorption or to an inefficient maturing process of intestinal immunity.8
The type of diarrhea that Avery described in 1968 with the term of “protracted diarrhea”,9 and that constitutes the predominant type in developed countries must be specified. The causes of protracted diarrhea are mentioned in table I. Many of these disorders may be seen also in developing countries, even though its prevalence is eclipsed considerably by the cases of post infectious diarrhea. For the diagnosis of PD other chronic diarrheas with or without malabsorption should be ruled out, such as: Celiac Disease, tropical sprue, Cystic Fibrosis, Crohn´s disease, etc.
Table I:
Causes of intractable non infectious diarrhea
Exocrine pancreatic insufficiency
Cystic Fibrosis
Enteropathy
Celiac Disease Autoinmune disorders Allergic enteropathy
Enzimatic defects
Lactase deficiency Enteroquinase deficiency
Transport defects
Glucose-galactose malabsorption
Congenital intractable diarrhea
Micro villi inclusion disease
Short Bowel Syndrome
Intestinal surgery
Blind loop syndrome
chronic enteropathy and PD are common manifestations of the advanced infection by HIV and AIDS.
An important increase in the frequency and mortality by PD in children infected by HIV has been reported.11 The treatment of the diarrhea in patients HIV positive is the same than for HIV negative patients.12 Lactose and monosaccharide intolerance is more frequent in the first group. Tuberculosis and malabsorption may be present. Prolonged diarrheal episodes associated with rare enteric pathogens are common.13 For children with compromised immune system PD is a risk of death.
RISK FACTORS
Research to identify risk factors for PD is a priority. The identification of such risk factors give information on the pathogenesis and epidemiology of PD The knowledge of the risk factors for PD in each country is of a vital importance for the prevention and control of PD. Based on the knowledge of the risk factors a comprehensive and effective strategy should reduce the rate of mortality related to diarrheal diseases. Earlier studies have clearly identified the risk factors for development of PD. However, these studies were conducted nearly two decades ago. Many of the identified risk factors for PD have changed.14
In PD the risk factors are of two kinds: social and those that depend on the host.
Diarrheal diseases are related to the degree of economic development and to the level of sanitation. The alteration of the individual and environmental protective factors; the availability, or not, of the necessary tools to control diarrheal outbreaks and the transmission of the different agents influence the prevalence of PD. The social risk factors are a complex of economic and social facts interrelated between themselves, such as personal and domestic hygiene, water supply, social status, waste disposal and food storage
The risk factors that depend on the host are: age, malnutrition, early introduction of animal milk, cellular immune deficiency, previous episodes of acute and persistent diarrhea, isolation of enteric pathogens and the use of antibiotics and other drugs during the acute phase. These risk factors may act in solitary or mix all together.
The outcome of frequent recurrent episodes of acute diarrhea is a nutritional deterioration that predispose to PD.10 Malnutrition is the sad heritage of sequential diarrheal episodes. Also prolonged episodes of diarrhea lead to a deterioration of the child nutritional status. A vicious circle of diarrhea-malnutrition-infection-diarrhea is established. In the malnourished child more and more severe episodes of diarrhea
may happen and new infections due to a defect in the cellular immunity occur. DP results in a marked shortage of energy, proteins and micronutrients. During the diarrheal episode anorexia, the diminishing of the caloric intake, the malabsorption of different nutrients and a hypercatabolic state along with the increase of the dietary requirements, all in combination, produce a loss of weight and of the growth velocity. The nutritional status is then affected and if there was a previous malnutrition, it is aggravated. It is a fact that malnutrition favors infections, and that infections contribute to malnutrition. Infections and inadequate intake of nutrients prolong all diseases.15 The iron deficiency that goes along with malnutrition diminishes the resistance to infections.
Breast feeding is the natural and better nutrient for infants. The incidence of DP is bigger during weaning. This pattern reflects the combination of the decrease in maternal antibodies, the lack of active immunity in children less than one year old, the introduction of contaminated food and the direct contact with human or animal feces when the infant starts to crawl. Breast fed infants do not get sick as frequently as non breast fed ones. The promotion of breast feeding as an effective way for the nutritional recovery of the infant with PD should be encouraged.16 The WHO considers that more than one million lives of infants could be saved if all the mothers exclusively breast fed their children in the first four months of life. The products of breast milk digestion in the lumen of the intestine enhance the absorption of sodium and water and reduce the frequency and the volume of the stools. The antibodies producing cells from the mother´s intestine migrate to the breast, and secretory antibodies common in the mother and child environment are passively transmitted to the child by his mother´s milk. Secretory IgA helps in the prevention of diarrhea and provides antibodies against the majority of the bacteria responsible for infectious diarrhea. There are also other protective factors in breast milk (lactoperoxidase, Gb3, neuraminic acid, etc). Breast milk is easily digested and acts as a protective factor against diarrhea reducing the exposure to contaminant pathogens. Breast milk stimulates the normal intestinal microbiota and inhibits the growth of several pathogens. It has bacteriostatic, bactericidal, fungicide and antiviral properties. Breast fed babies develop less and less severe infections than those who are not, even in those born from HIV positive mothers. Children without the benefits of breast feeding are 6 times in a bigger risk to die for infectious diseases, including diarrhea, in the first two months of life.17 This protection is more important for children living in places with bad sanitation.
Secretory IgA acts as an immunologic varnish that makes impossible the entrance of macromolecules across the intestine. Animal milk is an important risk factor for PD. Cow´s milk is the first food rich with proteins that an infant receive when is weaned and is the cause of allergic reactions in one fourth of the cases with alimentary allergy, with an incidence of 0.6% to 2% in the first two years of life. It is an important antigenic source in a moment when there is a relative immunologic immaturity. When there is a transitory deficit of IgA, macromolecules flow, being the first step in cow´s milk allergy. In PD there is a bigger permeability of the mucosa, predisposing to the flow across the intestine of macromolecules. Other predisposing factors exist, as for example, family history of atopy, alterations of natural or specific immunity, age of introduction of different foods and maternal immunity. The beginning of the symptoms in Cow´s Milk Protein Intolerance is related to the duration of exclusive breast feeding. The symptoms start after the introduction of cow´s milk alone or in combination with breast milk. Cow´s milk allergy produced by a reaction not mediated by IgE can be a consequence of malnutrition and has a more complicated outcome. The most valuable diagnostic test in alimentary allergy is the challenge with the suspected food. It is more accurate if it is done with a controlled placebo. If it is done periodically it is useful to check the persistence of the symptoms.18 Lactose and protein intolerance are important factors to prolong the diarrhea.
Antibiotics have a direct harmful effect on the intestinal mucosa and at alter the intestinal microbiota. Overgrowth of some microorganism may occur. Most of the children of developing countries with PD admitted to hospitals receive antibiotics during the acute phase of the disease. The use of antibiotics can induce the proliferation of resistant strains of enteric pathogens and may produce prolonged diarrhea. The use of Metronidazol doubles the risk of PD.2 The previous use of other drugs is also associated with the appearance of PD. Antidiarrheal drugs (loperamide, etc) do not have beneficial effects in children with diarrhea. They don’t prevent the dehydration nor improve the nutritional status in children with diarrhea, on the contrary, they have side effects that are dangerous and sometimes may be fatal.19 It is necessary to increase the rational use of antibiotics and other drugs for the treatment of acute diarrhea in children.
The previous episodes of acute and persistent diarrhea are important risk factors for PD. A child with a previous episode of PD has a very high risk for a new episode of PD. The association between previous episodes of acute and persistent diarrhea and PD probably is related to alterations in the epithelial turnover that makes easier the absorption of intact proteins by the damaged mucosa leading to a sensitization of the host to dietetic proteins. A previous episode may influence in
the beginning of PD by interfering with immunologic competence.
Any enteric pathogen capable to produce acute diarrhea can also cause PD. It happens that there is a group of pathogens that have special predilection for PD. We can mention:20
Parasites: Cryptosporidium, Cyclospora, Blastocystis
hominis, Entamoeba histolytica, Giardia, microsporidia Enterocytozoon bieneusi
Bacteria: entero aggregative Escherichia coli,
enteropathogenic E. coli, Campylobacter, Salmonella, Shigella, Plesiomonas.
Virus: norovirus, rotavirus
Cryptosporidium Hominis is highly infectious and an important cause of PD. The 12% of patients with AIDS and diarrhea from developed countries and the 24 % of similar patients in developing countries have Cryptosporidiosis. C. Hominis has been found in the stools of competent persons. In our environment it affects mainly children attending to nurseries. It can be asymptomatic. The majority of patients have watery chronic diarrhea with the loss of weight up to 10%. In Europe epidemic outbreaks associated with contaminated waters have been reported.21
Cyclospora cayetanensis is an emerging pathogen. There is evidence of the relationship of C. cayetanensis and diarrhea in the human being. It is present in adults and children with immune deficiencies or not. The diarrhea produced by C. cayetanens is similar to the diarrhea produced by any other enteric pathogen. It can be associated to steatorrhea and weight loss. C. cayetanensis should be suspected in patients suffering of PD that live or have traveled to tropical countries.22,23
The microsporidia Enterocytozoon bieneusi is an important cause of carbohydrates, fats and other essential nutrients malabsorption as a result of a villous atrophy. The infection by E. bieneusi is frequent in malnourished children with immune defects.24
Giardia Lamblia is frequently asymptomatic but can produce severe diarrhea with malabsorption. The microscopic exam of the feces is a practical and effective method to establish the presence of the infection.25
EPEC is known as efface and attachment (E/A).27 EAEC was found in the feces of patients with diarrhea in which the serology was different to the EPEC group and that were negative for the E/A test. The entero adherence and the production of a potent cytotoxin is the mechanism of production of the diarrhea. The diarrhea is severe, watery, greenish, with mucus, without blood.28 The EHEC produces two toxins (Verotoxin 1 and 2) that are responsible for the hemorrhagic colitis with bloody diarrhea, typical of the disease. There are cases without bloody diarrhea. It is transmitted by bovine meat inadequately cooked, other contaminated foods and by person to person contact.
The enteric Salmonella responsible for gastroenteritis are the Enteritidis, Typhimurium and Choleraesuis serotype. Enteric Salmonella is the most frequent cause of infectious diarrhea in the world. It invades the small intestine mucosa and produces an enterotoxin.29 There is a clear seasonal nature of the infection. It affects mainly children and is a frequent cause of PD.30
There are four groups of Shigella: Shigella disenteriae (group A); Flexneri (group B); Boydii (Group C) y Sonnei (group D). Shigella Flexneri is endemic in our country. Shigella invades superficially the terminal ileum and the colon and is the most important cause of dysentery. The infections by Shigella are significantly related to PD.31
Currently it is accepted that viruses are responsible for an important percentage of gastroenteritis at all ages, from a self limited episode that last less than a week to a prolonged episode with dehydration and substantial risk of death.30 They multiply selectively in the enterocytes destroying the microvilli enhancing the secretion of water and electrolytes and diminishing their absorption. Rotavirus and norovirus are the principal viral agents that produce diarrhea.33,34,35
Figure 2: Odds Ratio
It is important to differentiate between a persistent colonization and a postinfectious enteropathy that fails to repair the intestinal mucosa.36
Figure 3: Previous episode of persistent diarrhea
Figure 4: Malnutrition
We studied 102 patients with acute diarrhea and 85 with PD. All were less than one year old. Information about age, nutritional status, time of breast feeding, previous episodes of acute and persistent diarrhea and the previous use of drugs is registered. Microbiological and parasitological studies were done to identify enteric pathogens. To prove the association of PD and the exposure to different risk factors the statistic method of Chi square (x2) was used and the odds ratio estimated. In order of importance (Figure 2), and according to the OR, the risk factors identified were: previous episodes of PD (Figure 3), Malnutrition (Figure 4), less than one month with breast feeding (Figure 5), the use of metronidazol and antibiotics in the acute phase, multiple infections, previous episodes of acute diarrhea (Figure 6), and the identification of enteric pathogens 20.33
19.49 16.94 13.5 5.66
4.22 1.94
Previous Episode of P.D. Malnutrition Brest Feding ‹ 1 m Medication in Acute Phase Mix Infections Previous Episode of A.D. Isolation of Pathogens
100
2
102 60
25
85
No Yes Total
AD=102 PD
=85
p‹0.001
A.D. P.D.
5 9
88 102
31 26 28
85
‹ 3% 3-10% › 10% Total
AD=102 PD=85
p‹0.0001
(Figure 7). The most frequent pathogen isolated was Salmonella followed by enteropathogenic E. coli.37(Figure 8).
Figure 5: Without breast feeding and introduction of animal milk.
Figure 6: Previous episode of acute diarrhea.
Figure 7: Isolation of Pathogens.
Figure 8: Isolation of Pathogens.
CONCLUSION
PD represents an important health problem. The identification of risk factors for PD is basic for the understanding of the pathogenesis and epidemiology of PD. It is necessary to evaluate the risk factors in each country for the prevention and control of PD and to basic for the understanding of the pathogenesis and epidemiology of PD. It is necessary draw a plan for a comprehensive and effective strategy to reduce the rate of mortality related to diarrheal diseases. In order of importance, and according to the OR, the risk factors identified were: previous episodes of PD, malnutrition, less than one month with breast feeding, the use of metronidazol and antibiotics in the acute phase, multiple infections, previous episodes of acute diarrhea and the identification of enteric pathogens. The most frequent pathogen isolated was Salmonella followed by enteropathogenic E. coli.
REFERENCES
1. Ehsanur Rahman, et al. Childhood diarrhoeal deaths in seven low- and middle-income countries. Bulletin of the World Health Organization. Sep2014, Vol. 92 Issue 9, p 664-671.
2. Ruiz de Villa Martínez Y, et al. Diarrea Persistente. Principales causas y factores asociados en nuestro medio. Acta Pediátrica de México. 2004; 25 (2): 81-84)
3. Robberstad B, et al.Cost effectiveness of zinc as adjunct therapy for acute childhood diarrhea in developing countries. Bulletin of the WHO. 2004; 82 (7): 523-531.
4. World Health Organization: Diarrhoeal Diseases Control Programme Persistent diarrhoea in children in developing countries. WHO/CDD/88/27. 1988, 4-14.
5. Black RE. Persistent Diarrhea in Children in Developing Countries. Pediatric Infectious Disease Journal. 1993; 12: 751-7615.
6. Zea A. y Ochoa T. Diarrea y micronutrientes. Rev Med Hered. 2013; 24: 62-67.
7. Coello-Ramírez P, et al. Diarrea Crónica. Bol Med Hosp Infant Mex. 2001; 58: 491-498.
8. Thapar N, Sanderson IR. Diarrhoea in children: an interface between developing and developed countries. The Lancet, 2004; 363 (9409): 641-653.
9. Avery GB, et al. Intractable Diarrhea in Early Infancy. Pediatrics 1969: 41; 712-722.
10. Partners in Health, The PIH Guide to the Community-Based Treatment of HIV in Resource-Poor Settings (Revised Second Edition), Partners in Health, Boston, 2008.
7 1 5455 3325 8 4 10285
Only Breast Fed ‹ 1 months 1-3 months › 3 months Total
AD=102 PD=85
p₌0.14
A.D. P.D.
65 25 37 60 102 85
No Yes Total
AD=102 PD=85
p‹0.001
A.D. P.D.
71
31
102
46 39 85
No Yes Total
AD
=102 PD=85
p₌0.02
A.D. P.D.
10 2
6 2 1 1
9 2
2 0 0 0
21 8
5 2 2 2 1
2 1 1 1
3
Salmonella EHEC G. Lamblia ETEC Shigella A. Pseudomona
P.D. A.D.
11. Tindyebwa, D., et al., ‘Common Clinical Conditions Associated with HIV’, in: Handbook on Paediatric AIDS in Africa, 2004.
12. Bhutta ZA. Diarrea persistente en países en vías de desarrollo. Ann Nestle (España) 2006; 64: 39-48.
13. Lule, J.R., et al., ‘Effect of Home-Based Water Chlorination and Safe Storage on Diarrhea Among Persons with Human Immunodeficiency Virus in Uganda’, American Journal of Tropical Medicine and Hygiene, 2005; 73(5): 926-933.
14. Kumar Das S, et al. Changing trend of persistent diarrhoea in young children over two decades: observations from a large diarrhoeal disease hospital in Bangladesh. Acta Pædiatrica a2012 Foundation Acta Pædiatrica 2012 101, pp. e452–e457.
15. Suárez Cortina L. Gastroenteritis aguda: rehidratación oral y tratamiento nutricional. ¿Hacemos lo que debemos hacer? An Pediatr (Barc). 2001; 55: 2-4.
16. Jiménez R, Fragoso T, Sagaró E, Bacallao J. Influencia de la lactancia materna en la evolucion nutricional del lactante con diarrea persistente. Acta gastroenterol. latinoam; 25(1): 41-8, 1995.
17. WHO Collaborative Study Team on the Role of Breastfeeding on the Prevention of Infant Mortality, ‘Effect of Breastfeeding on Infant and Child Mortality due to Infectious Diseases in Less Developed Countries: A pooled analysis’, The Lancet, 2000; 355 (9202): 451-455.
18. Fabré D. Alergia Alimentaria. Normas de Pediatría. Programa de Atención Materno Infantil La Habana Cuba. 2012 (En imprenta.)
19. World Health Organization. The Rational Use of Drugs in the Management of Acute Diarrhoea in Children. Geneva, 1990.
20. López Marín D, Sagaró Gonzáles E, Valdés Depena M, Fragoso Arbelo T, Aibizu-Compos JC. Aislamiento de agentes
enteropatógenos en la Diarrea Persistente. Revista de Gastroenterología del Perú - Volumen 16, Nº3 1996.
21. Vergara A, et al. Brote de diarrea y transmisión de Cryptosporidium hominis asociados al uso de pañal en niños Med Clin (Barc) 2006; 127: 653 -656.
22. Gascon J, et al. Ciclosporidiasis: Estudio Clinicoepidemiológico en Viajeros con Cyclospora Cayetanensis Importada.IMed Clin (Barc) 2001; 116: 461-464S.
23. Martínez Silva I1 Ayllón Valdés, y Benítez Padrón X.3 Cyclospora Cayetanansis. Presentación de 20 Casos. Rev Cubana Pediatr 2002; 74(2): 178-81.
24. M Mor S, et al. Microsporidiosis and Malnutrition in Children with Persistent Diarrhea, Uganda. EID Journal. Jan 2009; 15 (1).
25. Medina Claros AF, et al. Parasitosis intestinales. Protocolos Diagnóstico Terapéuticos de la Asociación Española de Pediatría. Infectología Pediátrica. 2008.
26. Rodríguez-Angeles G. Principales características y diagnóstico de los grupos patogenos de Escherichia coli. Salud Publica Mex 2002; 44: 464-475.
27. Knutton S, Lloyd DR, Mc Neish AS. Adhesion of enteropathogenic Escherichia coli to human intestinal enterocytes and cultured human intestinal mucosa. Infect Immun 1987; 55: 69-77.
28. Okhuysen PC, DuPont HL. Enteroaggregative Escherichia coli (EAEC): A Cause of Acute and Persistent Diarrhea of Worldwide Importance. The Journal of Infectious Diseases 2010; 202(4): 503–505.
29. Albarado L, Guzman Y, Guzman M, Betancourt J. Salmonella spp. Y Shigella spp. Asociadas con Síndrome Diarreico Agudo en niños menores de 6 años de edad. Revista Kasmera 2005; 33 (2): 132-141.
30. Herrera D, Sánchez E, Martínez-Navarro F, Pérez-Ciordia, Abadías M, Ferrero M. Enteritis por Salmonella en Huesca. 1996-1999 . Enferm Infecc Microbiol Clin. 2002; 20: 16-21.
31. Ahmed F, Ansaruzzaman M, Haque E, Rao MR, Clemens JD: Epidemiology of postshigellosis persistent diarrhea in young children. Pediatr Infect Dis J 2001; 20: 525–530.
32. Wilhelmi I, Roman E, Sanchez-Fauquier A. Viruses causing gastroenteritis. Clin Microbiol Infect. 2003 4: 47-62.
33. Cáceres DC, Peláez D, Sierra N, Estrada E, y Sánchez L. La carga de la enfermedad por rotavirus en niños menores de cinco años, Colombia, 2004. 2006; Rev Panam Salud Pública. 20: 9–21
34. Kane EM, Turcios RM, Arvay ML, Garcia S, Bresee JS,1 and GlassRI The epidemiology of rotavirus diarrhea in Latin America. Anticipating rotavirus vaccines. Rev Panam Salud Pública. 2004; 16: 371–7.
35. de Rougemont A, Ambert-Balay K, Belliot G, Pothier P. Norovirus infections: an overview. Med Sci (Paris). 2010 Jan;26(1): 73-8.
36. Persistent Diarrhea Working Group. Recent Advances and Evidence Gaps in Persistent Diarrhea. J Pediatr Gastroenterol Nutr, 2008; 47(2): 260-265.
37. Sagaro E, et al. Factores de Riesgo para la Diarrea Persistente. Rev. Gastroent. Perú 1995; 15(3): 231-238.