APPENDIX 1: DETAILS OF EXTERNAL INSPECTION OUTCOMES
JANUARY 2014 CQC
Leeds Donor Centre and East Team Meets requirements
Edgware Donor Centre Meets requirements
Sheffield Cathedral Court Donor Centre Meets requirements
Bristol Donor Centre Meets requirements
Birmingham Donor Centre Meets requirements
Bristol North Team Meets requirements
Liverpool StS Meets requirements
Oxford Donor Centre and StS Meets requirements
FEBRUARY 2014 CQC
Plymouth Donor Centre and Team mobile Meets requirements
Oxford Apheresis Clinic and Team Meets requirements
Lancaster Apheresis Static Site Meets requirements
Cambridge Apheresis Clinic Meets requirements
Southampton Donor Suite Meets requirements
Brentwood Apheresis Cinic Meets requirements
Newcastle MHRA: February 2014 2 Majors;
QM sampling operator working with four units rather than one at a time
Temperature Validation and monitoring - Hot and cold spot criteria definition, probe positioning, poor data interpretation, lack of seasonal mapping in team stores, lack of temp limits in H&I, failed mapping risk assessments weak, mapping probes not in worst case positions.
10 Others 2 Comments MARCH 2014 CQC
Tooting Donor Clinic Meets requirements OCTOBER to DECEMBER 2013
Birmingham MHRA - November 2013 1 Major
Document control and documentation practice was found to be poor across a number of departments
8 Others 2 Comments
Leeds HTA - November 2013 4 Advice & Guidance Sheffield MHRA - October 2013 2 Majors
Information was provided to the inspectors which was misleading in relation to process programme settings for the Optipress equipment in POD 3.
Quality Management System and associated documentation was weak in the following areas; Control of process deviations (PDVs), Impact and Risk Assessment Processes and Qualification & Validation Documentation 6 Others
Business Continuity (ISO22301) All Depts November 2013 (Manchester, Tooting, Brentwood, Filton, Plymouth)
No issues raised
JACIE Yorkshire Blood & Bone marrow Transplant Service Including StS and CMT Leeds - October 2013
5 minor deficiencies noted for StS and CMT
HTA - Tissue Services Satellite Site Friarage Hospital October 2013 No shortfalls reported
JULY 2013 to SEPTEMBER 2013
HTA - Tissue Services Satellite Site Bradford Royal Infirmary August 2013 No shortfalls reported
5 items of advice and guidance Oxford MHRA - August
6 Others Filton MHRA - July 2 Majors
Equipment management is deficient with respect to the validation scripts and the use of validation in change control
Training issues were identified which included Records for contract staff not being maintained. Staff training was not commenced or completed prior to the issue of SOPs in some instances. Task Based Training Records to several documents were not available at the time of the audit.
8 Others
Tooting MHRA - July 5 Others: 2 Comments:
JACIE Birmingham - July
Positive feedback received and no non-conformances reported. HTA ODT - July
3 items of advice and guidance. APRIL 2013 to JUNE 2013
HTA - Tissue Services Satellite Site Aintree Hospital June 2013 No shortfalls reported
Plymouth MHRA June 2013 4 Others
10 Comments
Additionally a letter was received warning that further breaches of procedure re. inadequate spacing of screening booths will result in a Major non-conformance. Oxford MHRA July 2013
6 Others 7 Comments
Cambridge MHRA - May 2013 3 Other
3 Comments, including;
It was a pleasure (as usual) to inspect your site at Cambridge. Please pass on my regards to your team for the professional way they conducted themselves.
Manchester/Lancaster MHRA April 2013 1 Major
Issues in facilities and equipment management with regard to the management of TABs requests and the fabric of the Lancaster Stock Holding Unit. Temperature mapping and monitoring and the history of some equipment not being available. 6 Others
8/9 Comments
Clinical Biotechnology Centre MHRA April 2013 3 Majors
Company practices were not minimising the risk of potential contamination. Aseptic Practices were deficient including poor gowning techniques, poor environmental monitoring, jewellery being worn in the clean rooms. Autoclave was not in compliance with current EU GMP requirements. 3 Others
3 Comments
Birmingham HTA (SCI) - April 2013 1 Other
Oxford HTA April 2013
APPENDIX 2: SCHEDULED AND ANTICIPATED EXTERNAL INSPECTIONS 2014/15
Apr-14 May-14
Jun-14
Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Apr-15
Leeds JACIE(i) MHRA CPA(RCI)
Liverpool MHRA
HTA UL
CPA(RCI) JACIE(i)
Liverpool ATU MHRA
Manchester/Lancaster MHRA Newcastle EFI CPA(RCI)
Sheffield CPA(RCI)
HTA Brentwood MHRA Cambridge Colindale MHRA EFI CPA(RCI)
HTA CPA (NTMRL)
Tooting EFI CPA(RCI)
Birmingham EFI CPA(RCI)
HTA Filton CPA(IBGRL) CPA(RCI)
HTA Oxford HTA JACIE Plymouth Southampton
MHRA HTA JACIE (i)
Cord Blood bank
(Colindale and Filton) CBC MHRA Wolfson Business Continuity BSI ODT
APPENDIX 3: DETAILS OF MHRA SABRE REPORTABLE EVENTS
JANUARY 2014 to MARCH 2014
Birmingham - Transport Courier - Directed platelet for a named patient was delivered directly to Queen Elizabeth Hospital Birmingham instead of to Birmingham Hospital Services for irradiation then issue to the hospital. Unit was not issued as a clinical concession (unit was out of NHSBT control while at the hospital and had been removed from container and placed in platelet incubator before being returned for irradiation).
Manchester - Clinical Support Team were contacted by Manchester Donor Centre with the information that they had received a platelet sample from this donor and had noticed that NCC had placed a malaria travel deferral in July 2013 which lapsed in December 2013. Despite this there was no Discretionary Test incident for malaria travel on her last donation. Initial
investigation has shown that unit tested negative for Malaria so there was no direct risk to patient safety in this instance.
Colindale. Hospital Services. BactAlert recall was not performed and no action taken for implicated components, Apheresis platelets pack 1 and pack 2. Colindale Hospital Services notified by Alarm point at 16:37 on 25/01/14 for recall W004766. Pack 1 transfused at UCH on 26/01/14 at 17:45. Pack 2 in stock at Brentwood.
Sheffield - H&I. Incorrect HLA typing report issued to hospital. DNA had been switched during the typing process leading to the wrong type being assigned to a patient. This led to the incorrect HLA type being assigned to the patient who required HLA matched platelets. The impact appears to have been minimal: the patient received HLA matched platelets and gained some increments. Manchester - Bacterial Screening. Platelets could not be validated at normal time. Results resolved at 20.00 as problem was not picked up until this time as it was out of hours. National IT reported that the Message Client on the Data Manager was closed. This program links the Data Manager to Pulse. During this time it appears a bottle became positive at 15.55 but no automatic alarmpoint recall was sent and so there was a 4 hour delay in initiating the recall. Pack 2 of the apheresis platelet associated with this recall was transfused at Royal Oldham Hospital but testing concluded indeterminate negative and no patient reaction was reported.
Manchester - Bacterial Screening. 20 anaerobic bottles found to be anonymous on the BactAlert system. Bottles were sampled and loaded and were incubating for four days. All 20 products had an initial negative in Pulse hence there was no risk to patients.
Tooting - Tunbridge Wells. Possible that donor arm was not cleaned before venepuncture. An unused chloraprep wand was found in one of the empty pack boxes indicating the possibility that a donor arm was not cleaned before venepuncture. As the implicated donation could not be identified 24 donations were discarded.
OCTOBER to DECEMBER 2014
Filton - Testing virology. On 20/11/13 it was noted that the updated Aurora software retest function does not identify the sample status until later in the process than the previous system. This is being investigated by Abbott/Stratec and as part of INC45489 they have performed a search of the database to determine if samples have been loaded more than once on an Prism. Eleven samples were found from 23/09/13. These samples had valid HIV results in PULSE with initial reactive results and one negative retest, the negative retest was reported from aurora before the initial reactive result.
Manchester - Testing - Donor identified as a DV (RhD positive) in partial D kit. Banked as RhD negative on 21/07/13. Donors historical RHGRP blood characteristic had been blanked down with DBAs by Savant on two occasions. Two other donations had been banked as RhD negative prior to DV status being confirmed, hence transfused product labelled as D negative which should have been labelled D positive.
National - A number of failures to recall components within the required timelines has prompted a review of current procedures. Full review of Recall Process ongoing. Immediate action being taken on where recalls are handled as hand offs have caused issues. Immediate clarification of record keeping and hospital contact requirements. Clarified timescales for Bact Screening recalls for MHRA.
Colindale - Hospital Services - Recall not performed for Packs 1 & 3.
Colindale - Manufacturing - white lumps in CD Platelet pack returned to NHSBT and unit credited. No units transfused. QA initiated recall for pack 2 and associated pack 1 at Hammersmith for NBL and Manufacturing to investigate.
Colindale - Manufacturing. 173 units not manufactured in a timely manner.
Filton - Hospital Services - Bacterial positive recall was not communicated to hospital in the half hour limit.
JULY to SEPTEMBER 2013
Colindale - Hospital Services - Recall not performed for Packs 1 & 3.
Colindale Hospital Services Recall: Confirmation received from hospital that a recalled component was transfused after the hospital had been contacted (recall was not sent to hospital within one hour), there was a delay of 3 hours by Hospital Services in contacting the Hospital. Tooting - Hither Green 2 (mobile). Likely contaminated pack not reported at the time of donation, was reported the following morning. Staff member reported withdrawing the needle without closing the clamps, therefore air was possibly introduced to the pack.
NQI - Current version of DAT341 and the extended criteria data sheet DAT2334 were incorrect. While both list Sardinia as Malaria and Chick V zero risk (correctly) they however do not highlight it as WNV risk. The risk is that donors may have been bled within 28 days of visiting Sardinia and not had the discretionary sample taken, nor have been questioned about any flu/cold like illness they may have had whilst there or since their return.
Colindale - Hospital Services. Recall not performed for Packs 1 & 3. Recall instruction was to recall all 3 components but recall was run for only 1. New recall performed but receiving Hospital reported both components transfused; it was concluded that at least 1 of these transfusions could have been avoided if the full recall had been undertaken initially.
Conlindale - Hospital Services - Recall confirmation received from hospital that a recalled component was transfused after the hospital had been contacted. Paperwork for Watford hospital not immediately available so hospital contacted by phone and given details of unit to be quarantined pending further contact. Verbal confirmation received from hospital that component (Platelet pool) had been transfused (approx. 3 hours after initial contact made by Hospital Services Colindale). Risk: High - Unit appears to have been transfused after the hospital were contacted to quarantine implicated component. Hospital confirmed: Patient did not have a transfusion reaction.
APRIL to JUNE 2013
Newcastle - A chloroprep wand was found in the bedside tray following completion of donation. Staff were unsure if donors arms had been cleaned on Session.
Newcastle -174 units of Red Cells were not stored at the required temperature (2-6°C). The units were being transported from Processing to Hospital Services and during the transfer 10 crates of red cells (one trolley) was not placed into the fridge but left next to the fridge door. The trolley was discovered by Hospital Services the next day.
APPENDIX 4: DETAILS OF HTA REPORTABLE EVENTS JANUARY 2014 to MARCH 2014
None reported.
OCTOBER to DECEMBER 2014
Leeds - SCI Leeds Hospital notified by the Anthony Nolan that a bone marrow donation was growing streptococcus viridans. At this point the bone marrow donation had already been infused. The patient had developed signs of infection and had had central and peripheral blood cultures done. These grew a gram negative organism, but did not grow streptococcus viridans. Patient has improved rapidly on treatment for the gram negative organism. This was reported to HTA by the Anthony Nolan.
Filton - Cord Blood. Patient was infused with a double cord transplant, the cord units were frozen and from Cord banks coordinated through the National Marrow Donor Program (NMDP). - 2 cord units via the NMDP. The patient had a reaction during the infusion of the second bag of 3. The patient experienced severe abdominal pain and required morphine bolus. Third and final bag of the infusion was delayed 1hour and 50 minutes, the third bag appears to have been infused with no event. INC44896 had already been raised and closed due to damage to the line of one of the bags on receipt from the Cord Bank.
Liverpool - Tissues Customer Care - Supplier - Ramsey Fitzwilliam Hospital in Peterborough called to check their 'before 09:00' delivery of tissue was on its way. TNT said there had been some sorting issues at the depot and that the ETA had changed to 10:30. TNT then called to say the delivery would be even later, ETA 11:00. The tissue was delivered to the hospital at 11:10. However the way it was delivered was also cause for concern. The van had a very shabby appearance and was described as having the look of a maintenance van. The floor of the van had old bits of plaster on it. The boxes within the van were tumbled all over it. Although the driver was apologetic he had no idea what he was looking for or where it was in the van. It was clear he didn't know he was delivering human tissue. A member of hospital staff had to climb into the van and look for the box and when found it was wet. The biggest concern for the Theatre Manager was that because of the lateness of the delivery the Surgeon had to change the procedure whilst in the middle of surgery. He was forced to take the bone graft from the patients tibia and he felt the patient was put at risk. The tissue from NHSBT was also used when it eventually arrived. JULY to SEPTEMBER 2013
Leeds - SCI - PAE. Patient received a double cord transplant at St James. One of the cords was a red cell replete. The clinicians were informed of this. The SCI lab received an IAIR stating that the patient had symptoms that were "suspicious of intravascular haemolysis". The patient was treated with supportive care. The symptoms started during the infusion of the red cell replete unit. Patient
had hypoxia, hypotension, abdominal pain and acute kidney injury. Both Cord blood units provided through the Nolan Registry who have been asked to investigate by the HTA. Reaction thought to be due to excess red cells in one of the units supplied by an Italian Cord Blood bank. Oxford - SCI. The 2G 30 day engraftment form was received from the Churchill Hospital informing the lab that a patient with Myelofibrosis had primary graft failure following a cryopreserved sibling transplant.
National - Hematos - Bug identified in Hematos v3.5.2.2 whereby the bacteriology results for the previous / historical donation is reported if a bacteriology result for the current donation is not available. This may give rise to an incorrect bacteriology result being reported to a Transplant Centre. This impacts several SCI Transplant Summary Request Reports that have been printed since v3.5.2.2 go-live. No other reports or Departments are impacted by this bug.
APRIL to JUNE 2013
Leeds - SCI -Leeds General Infirmary (LGI) - Late collection of Directed Cord Blood collection (DCB). 2 hours post delivery. Risk: Insufficient stem cells collected for therapeutic use Impact: Low, The cord was not a match for the intended recipient. Event raised against supplier (LGI). Event raised as major on advice of LQS because event is to be notified to HTA by LGI.
Filton - BBMR - Donor requested for confirmatory typing for German patient. DHC returned by donor to BBMR. Donor answered question A6 (MSM) as Yes. The response was not questioned or followed up by BBMR Stem Cell Co-ordinator. Consultant authorising the final donor clearance requested sight of DHC completed by donor and noted the answer to Question A6.
Filton - BBMR - Healthcare at Home (HaH) home administration team failed to administer Day 1 and Day 2 G-CSF injections to the donor. The service by HaH is made up of 2 components, a Pharmacy service to supply G-CSF for 4 days prior to the first apheresis day and a nurse to administer the drug to the donor at home for the first 3 days. The 4th day injection is administered at the STS unit. The donor would attend the STS unit as planned to determine if they had mobilized sufficiently to commence the apheresis procedure. The CD34+ cell count in the blood was 2 x 10^3/µl, insufficient to commence the first apheresis. TC were informed of the possibility of a delay of ~24 hours in the availability of the cells for infusion. The TC was in Bordeaux, France. The delay in G-CSF administration resulted in a revision to the apheresis schedule. The transport of the cells may have been delayed by 24 hours and therefore impact on the intended infusion date.
APPENDIX 5: CURRENT DOCUMENTS OVERDUE REVIEW Quarter 4 2013/14
Owner
Directorate Document Count Overdue review
% Overdue BD 650 11 1.7 BTS 428 69 16.2 CLINICAL 631 8 1.3 CPA 3 3 100 Logistics 476 1 0.2 Emergency Planning Service 153 11 7.1 FIN 125 14 11.2 HR 177 1 0.7 ODT 562 20 0.2 PS 2171 5 0.2 QA 344 2 0.3 DTS 4876 47 0.0 Total 10596 192 1.8
Percentage of documents overdue review
0 0.5 1 1.5 2 2.5 3 3.5 4 0 1 /0 4 /1 3 0 1 /0 5 /1 3 0 1 /0 6 /1 3 0 1 /0 7 /1 3 0 1 /0 8 /1 3 0 1 /0 9 /1 3 0 1 /1 0 /1 3 0 1 /1 1 /1 3 0 1 /1 2 /1 3 0 1 /0 1 /1 4 0 1 /0 2 /1 4 0 1 /0 3 /1 4 0 1 /0 4 /1 4
APPENDIX 6: BENCHMARKING DATA SABRE REPORTS
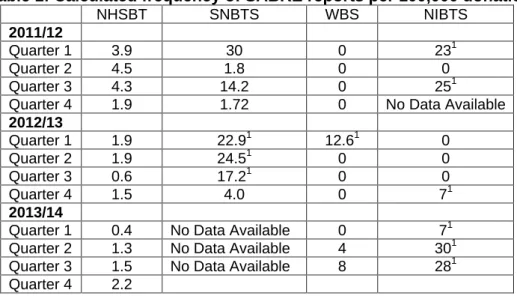
Table 1: Calculated frequency of SABRE reports per 100,000 donations NHSBT SNBTS WBS NIBTS
2011/12
Quarter 1 3.9 30 0 231
Quarter 2 4.5 1.8 0 0
Quarter 3 4.3 14.2 0 251 Quarter 4 1.9 1.72 0 No Data Available
2012/13 Quarter 1 1.9 22.91 12.61 0 Quarter 2 1.9 24.51 0 0 Quarter 3 0.6 17.21 0 0 Quarter 4 1.5 4.0 0 71 2013/14
Quarter 1 0.4 No Data Available 0 71 Quarter 2 1.3 No Data Available 4 301 Quarter 3 1.5 No Data Available 8 281 Quarter 4 2.2
1
relatively small numbers donated by comparison to NHSBT throughput mean that a small number of reports in a quarter have a big impact on the calculated frequency.
SAED REPORTS
Table 2: Calculated frequency of SAEDs reports per 100,000 donations
NHSBT SNBTS WBS NIBTS 2012/13 Quarter 1 1.5 0 0 0 Quarter 2 1.1 0 0 0 Quarter 3 2.3 0 4.32 0 Quarter 4 1.3 1 0 0 2013/14
Quarter 1 3.3 No Data Available 0 0 Quarter 2 2.2 No Data Available 0 0 Quarter 3 2.0 No Data Available 0 0 Quarter 4 1.1
1 2010/2011 data
2
relatively small numbers donated by comparison to NHSBT throughput mean that a small number of reports in a quarter have a big impact on the calculated frequency
Table 3: Bacterial Screening Initial Reactive Rates (%)
NHSBT SNBTS WBS 1 NIBTS 2012/13 Quarter 1 0.18 0.34 0.1 0.26 Quarter 2 0.18 0.10 0.1 0.38 Quarter 3 0.19 0.07 0.4 0.3 Quarter 4 0.14 0.20 0.1 0.91 2013/14
Quarter 1 0.13 No Data Available 0.49 0* Quarter 2 0.27 No Data Available 0.13 0.44 Quarter 3 0.21 No Data Available 0.04 0.56 Quarter 4 0.15
*No bacteriology screening of platelets in May and June due to validation of industry bottles (only 75 platelets screened).