PLEASE SCROLL DOWN FOR ARTICLE
On: 18 February 2010
Access details: Access Details: [subscription number 908990998] Publisher Routledge
Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Journal of Social Work in End-Of-Life & Palliative Care
Publication details, including instructions for authors and subscription information:http://www.informaworld.com/smpp/title~content=t792322386
Preparing Family Caregivers for the Death of a Loved One: Implications
for Hospital Social Workers
Randy S. Hebert a; Valire C. Copeland b; Richard Schulz c; Charlene A. Amato d; Robert M. Arnold e a Forbes Hospice, Pittsburgh, Pennsylvania b School of Social Work, University of Pittsburgh in Pittsburgh, Pennsylvania c University Center for Social and Urban Research, University of Pittsburgh in Pittsburgh, Pennsylvania d Case Management Department, UPMC Presbyterian Hospital in Pittsburgh, Pennsylvania e Division of General Internal Medicine, Section of Palliative Care and Medical Ethics, University of Pittsburgh School of Medicine in Pittsburgh, Pennsylvania
To cite this Article Hebert, Randy S., Copeland, Valire C., Schulz, Richard, Amato, Charlene A. and Arnold, Robert M.(2008) 'Preparing Family Caregivers for the Death of a Loved One: Implications for Hospital Social Workers', Journal of Social Work in End-Of-Life & Palliative Care, 4: 4, 269 — 285
To link to this Article: DOI: 10.1080/15524250903081533 URL: http://dx.doi.org/10.1080/15524250903081533
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article may be used for research, teaching and private study purposes. Any substantial or systematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply or distribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.
PEER-REVIEWED ARTICLES
Preparing Family Caregivers for the
Death of a Loved One: Implications
for Hospital Social Workers
Randy S. Hebert Valire C. Copeland
Richard Schulz Charlene A. Amato
Robert M. Arnold
Preparation of this manuscript was supported by grants from the NIMH (1K23 MH074963–01) and the Cancer and Aging Program at the University of Pittsburgh in Pittsburgh, Pennsylvania (P20 CA103730).
Randy S. Hebert, MD, MPH, is Medical Director at Forbes Hospice in Pittsburgh, Pennsylvania. Valire C. Copeland, PhD, MPH, is an Associate Professor in the School of Social Work at the University of Pittsburgh in Pittsburgh, Pennsylvania. Richard Schulz, PhD, is a Professor of Psychiatry and Director of the University Center for Social and Urban Research at the University of Pittsburgh in Pittsburgh, Pennsylvania. Charlene A. Amato, MSW, BCD, LCSW, is a Palliative Care Social Worker in the Case Management Department at UPMC Presbyterian Hospital in Pittsburgh, Pennsylvania. Robert M. Arnold, MD, is a Professor in the Division of Gen-eral Internal Medicine, Section of Palliative Care and Medical Ethics at the University of Pittsburgh School of Medicine in Pittsburgh, Pennsylvania.
Address correspondence to Randy S. Hebert, Medical Director, Forbes Hospice, 115 South Neville Street, Pittsburgh, PA 15213. E-mail: rhebert@ wpahs.org
Journal of Social Work in End-of-Life & Palliative Care, Vol. 4(4) 2008
#2008 by Taylor & Francis Group, LLC. All rights reserved.
doi: 10.1080/15524250903081533 269
ABSTRACT. Providing care to a seriously ill loved one at end of life is very difficult. Many family caregivers, however, are not prepared for the death and may suffer more psychological morbidity as a result. Although the scope of social workers’ practice makes them ideal professionals to work with caregivers, there is little research about the role they play in preparing caregivers for the death. Focus groups and semistructured interviews conducted with caregivers of terminally ill patients revealed that hospital social workers were not generally perceived as helpful in preparing them for the death. Caregivers reported many unmet needs for which social workers’ expertise would have been invaluable—i.e., needs for better com-munication with health care providers, psychosocial support, and accessing resources. Future work should be directed to verifying our findings and determining how to overcome barriers that prevent hospital social workers from preparing caregivers for the death of a loved one.
KEYWORDS. Bereavement, caregivers, palliative care, social work, terminally ill
BACKGROUND
Providing care to a family member or loved one with terminal illness can be very stressful, as family and friends provide personal and medical (e.g., administering medications, changing dressings) care while balancing home and work responsibilities. In fact, care-givers spend an average of more than 100 hours a week with these tasks when patients are at end of life (Haley, LaMonde, Han, Narramore, & Schonwetter, 2001). Despite the intense nature of the care provided, however, many caregivers perceive themselves as unprepared for the death. For example, in one national sample, 23% of approximately 1600 decedents reported that the death was ‘‘extremely’’ unexpected (Teno et al., 2004). In another study, 25% of bereaved caregivers thought that health care providers should have done more to prepare them (Barry & Prigerson, 2002). Being un-prepared for the death is not without consequence. Caregivers who perceived themselves as unprepared suffer from more depression, anxiety, and complicated grief (Barry, Kasl, & Prigerson, 2002; Hebert, Dang, & Schulz, 2006). The scope of this problem is tremendous when one considers that of the 2.4 million deaths a year
in the United States, the great majority are preceded by a period of family caregiving (Emanuel et al., 1999; National Center for Health Statistics, 2007).
Preparedness has been a focus of recent investigation. For example, several studies have demonstrated that preparing for the death of a loved one has medical, practical, psychosocial, and religious or spiritual components (Clayton, Butow, Arnold, & Tattersall, 2005; Steinhauser et al., 2001). Caregivers, therefore, often need more than prognostic information in order to prepare. They may also need information about financial, family, or spiritual con-cerns (Hebert, Schulz, Copeland, & Arnold, 2008). Preparedness also depends on getting consistent, accurate information from credible authorities, including the various health care providers involved in the patient’s care. Credible authorities help prepare caregivers by pro-viding reliable information and demonstrating empathic behaviors such as acknowledging caregivers’ emotions, listening, providing emotional support, and eliciting questions (Parker et al., 2007). Unfortunately, many health care providers do not use or possess these skills. They feel uncomfortable discussing death and dying, use ambiguous language, answer caregivers’ questions inappropri-ately, provide conflicting information, or adopt strategies that block caregivers’ emotional reactions (Fallowfield, Jenkins, & Beveridge, 2002; Maguire, 1985). As a result, although preparing caregivers for the death of a loved one is a key task for health care providers who provide care to dying patients, caregivers report that this compo-nent of end-of-life care is often neglected (Hanson, Danis, & Garrett, 1997; Russ & Kaufman, 2005).
The education and training of social workers makes them ideal professionals to help address this deficiency in end-of-life care (Bern-Klug, Gessert, & Forbes, 2001; Kovacs, Bellin, & Fauri, 2006). Social worker competencies linked to preparedness include knowledge of the biopsychosocial aspects of death and dying and expertise with the practical, informational, and spiritual needs of family caregivers (Gwyther et al., 2005). By explaining the process of dying, supporting the family before and after the death, and pro-viding caregivers with access to community resources, social workers are uniquely qualified to prepare families for death and bereavement (Bern-Klug, Kramer, & Linder, 2005; Quinn, 1998). Social workers have in fact been described as the ‘‘glue’’ that links palliative care patients and families to needed health, economic, and social systems
(Berzoff et al., 2006). By counseling families and providing them with adaptive coping strategies, social workers can also assist grieving family members manage emotions which could otherwise limit their ability to process information (Kissane, Bloch, McKenzie, McDowall, & Nitzan, 1998; Roberts, Baile, & Bassett, 1999). Finally, because poor communication with members of the health care team can hinder preparation for the death, social workers can help better prepare caregivers by fostering effective communication between members of the interdisciplinary team, patients, and families (Gwyther et al., 2005). In summary, the scope of social work practice allows social workers to use their expertise in counseling, family systems, bereavement, and interdisciplinary communication to imp-rove the care of family members of terminally ill patients (Rose & Shelton, 2006; Zittle, Lawrence, & Wodarski, 2002).
Although social workers can play a vital role in palliative care, there is, however, little research about the role they play in preparing caregivers for the death of a loved one. The goal of this article is to describe family caregivers’ experiences with hospital social workers as they were preparing for the death of their loved one.
METHODS Study Design
The data reported below were collected as part of larger data set describing the factors caregivers believe are important to prepare for death and bereavement (Hebert, Schulz, Copeland, & Arnold, 2009).
Sample
As is standard in qualitative research, we recruited a purposeful sample, or one expected to provide in-depth information about an issue about which little is known (Patton, 2002). Current caregivers were English-speaking adults involved in the care of a patient with a life expectancy of less than 6 months and receiving care from a university-based palliative care consult service or community-based hospice. Bereaved caregivers were those whose family member was deceased for less than 12 months. This sample was chosen for several
reasons. First, current caregivers were likely to have considered the possibility of their loved one’s death. Second, bereaved caregivers were interviewed because current caregivers are sometimes so engrossed with providing care that they may have difficulty reflecting on their needs (Rabow, Hauser, & Adams, 2004). Finally, unlike hospice, the consult service sees patients who are receiving care with life-prolonging intent. Interviewing caregivers from both settings allowed us to obtain broader insights on preparedness.
Data Collection
We planned focus groups for six to eight caregivers, the ideal number to ensure meaningful dialogue without hindering partici-pation (Carey, 1995). However, cancellations reduced the first two groups to only three and five participants, respectively. Because several caregivers commented on the emotional difficulty of being interviewed at the hospital where their loved one died, the format was therefore changed to ethnographic interviews held at the hospital or in caregivers’ homes. A moderator guide was used to structure the interviews. Interviews were conducted by an experienced moderator, audiotaped, and transcribed. A research assistant took notes. Data collection and data analyses were iterative and interviews were conducted to the point of redundancy, or until no additional topics were raised.
Data Analysis
Data were analyzed using the constant comparative method (Patton, 2002). Two investigators read all transcripts independently to generate a list of preliminary codes, met regularly to refine the coding structure, and developed a codebook used to structure data analyses (MacQueen, McLellan, Kay, & Milstein, 1998). Any men-tion of the words social worker or social workers was noted. Transcripts were then independently coded by two coders who were not members of the study team. Coders met regularly with the moderator to discuss the utility of codes, the consistency of code application, and to resolve inconsistencies. This iterative coding process continued until consensus was reached. The ATLAS software program (ATLAS.ti 5.0 Scientific Software Development, Berlin, Germany) was used to manage data. Steps used to ensure reliability
and validity included comparing the accuracy of all audiotapes with written notes, independent coding of data in a standardized manner, and review of the data analyses by the study team consisting of individuals with complimentary areas of expertise in social work, palliative care, qualitative methods, end-of-life communication, cultural competence, and caregiving.
Study procedures were approved by the University of Pittsburgh Institutional Review Board.
RESULTS
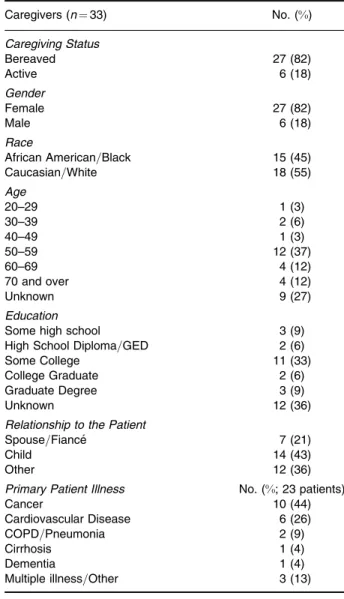
Caregivers were predominantly female, adult children, and providing care to loved ones with cancer or cardiopulmonary disease (Table 1). Table 2 provides a list of the main questions asked of caregivers. With no prompting by the moderator, seven (21%) of the caregivers discussed their interactions with hospital social workers. The major finding was that none of these caregivers thought that social workers were helpful in preparing them for the death of their love one. Rather, the comments were negative in nature.
The most common comments referred to the perception that social workers were more interesting in discharging patients, or ‘‘shipping them out,’’ than addressing families’ questions.
They (doctors) were talking about how we were to meet the social worker, saying ‘‘Someone will come in and talk to you.’’. . .Next thing I know the social worker is shipping me out of the hospital. Nobody communicated with me. I just had no idea what I was going to do. . .I didn’t know what was going on. (Bereaved, Caucasian, sister of patient)
The following caregiver, a nurse, describes her experience trying to have her mother-in-law transferred to hospice rather than a nursing home.
They were ready to get her (mother-in-law) out of the hospital. They wanted her out. . .so the social worker told me, ‘‘She doesn’t go to a hospice facility. She has to go to ____ (the nursing home).’’ I had to fight to get her out of ____ (the nursing home) and into a hospice. I don’t think you should have
to fight for those kinds of things. And I wouldn’t even have known to ask for that (hospice) had I not been a nurse and knew a little bit about that. . .That was the most overwhelming experience. . .you’re so vulnerable at that time and you’re so dependent upon them to help you. . .She (social worker) was
TABLE 1. Characteristics of Study Participants
Caregivers (n¼33) No. (%) Caregiving Status Bereaved 27 (82) Active 6 (18) Gender Female 27 (82) Male 6 (18) Race
African American=Black 15 (45) Caucasian=White 18 (55) Age 20–29 1 (3) 30–39 2 (6) 40–49 1 (3) 50–59 12 (37) 60–69 4 (12) 70 and over 4 (12) Unknown 9 (27) Education
Some high school 3 (9) High School Diploma=GED 2 (6) Some College 11 (33) College Graduate 2 (6) Graduate Degree 3 (9)
Unknown 12 (36)
Relationship to the Patient
Spouse=Fiance´ 7 (21)
Child 14 (43)
Other 12 (36)
Primary Patient Illness No. (%; 23 patients)
Cancer 10 (44)
Cardiovascular Disease 6 (26) COPD=Pneumonia 2 (9)
Cirrhosis 1 (4)
Dementia 1 (4)
Multiple illness=Other 3 (13)
more interested in getting her to go to a nursing home. . .
(Bereaved, Caucasian, sister-in-law of patient)
The following two caregivers reported that social workers were unhelpful in helping them access resources that would have allowed them to better care for their loved one at home prior to the death.
What started out as a job (caregiving) to keep me occupied for a couple of hours a day became a fulltime necessity. . .That’s where the social workers failed me. . .I had no one to help me (care for the patient at home). . .(Bereaved, Caucasian, wife)
The social worker kept telling me what to do but didn’t give me a means to do it. We didn’t have no money. Instead of saying ‘‘I know of resources. . .’’ he kept saying ‘‘Can’t you just do this?’’ He was all talk and no action. (Bereaved, African American, mother)
The following woman had years of experience caring for her husband who had multiple hospital admissions for diabetes, renal insufficiency, and severe congestive heart failure.
What I need is an advocate. I need somebody that’s going to be there. . . I’ve been going crazy trying to get these stupid forms (insurance) filled out. These forms are a nightmare. . .they (social workers) don’t give enough information. . .we found things out by accident. . .I need a person to serve as an advocate and help me gather resources as needed so I don’t have to try to figure out who to contact, how to get them, how to pull it all together, and all the questions I need to ask and keep pounding, pound, pounding. . .In the old days I thought that’s what a
TABLE 2. Moderator Guide for Interviews
1. Please tell us a little bit about your loved one’s illness.
2. Think back to when you first realized that your loved one’s illness was progressing or was not curable, what questions came to mind?
3. How do=did you prepare for the future?
4. What is=was important to you in preparing for your loved one’s death? 5. How can health care providershelp caregivers prepare?
Note.We defined health care providers for participants as doctors, nurses, social workers,
therapists, clergy, or others involved in the care of their loved one.
social worker was supposed to help you with, but that doesn’t seem to be the case anymore. In fact, you don’t even hear from them. (Current, Caucasian, wife)
More disturbingly, when caregivers were asked, ‘‘How can health care providers help caregivers prepare?’’ (Table 2, Question #5), caregivers’ recommendations focused on what physicians, nurses, and clergy can do to help prepare them for the death of their loved one. No caregivers included social workers in their recommendations. The fact that social workers were not included in the recommenda-tions should not be taken to imply that caregivers had no needs that social workers could help address. On the contrary, caregivers needed help with several issues for which social workers’ assistance would have been invaluable. A common need was the need for better com-munication with health care providers. This caregiver described her frustration in attempting to get answers from the multiple health care providers involved in her mother’s care. She had no clear idea who was coordinating the care or to whom she should turn to for questions.
I could never get in touch with the doctor associated with her personal care home. They had other doctors associated with the hospital attending her. . .you’ve got 100 people (health care providers) to see. . .It looks like a phone book. . .Where do I start?. . .So I try to talk to one person, she can’t talk. . .the nurses don’t really want to talk to you so they push you off on a doctor. . .and it wasn’t the doctor who took care of her (patient) at the personal care home. . .and they are unable to reach him. He never calls back. . .so now I’m talking to a doctor I don’t know and he doesn’t know her (patient). . .it’s just a lack of communication. (Bereaved, African American, daughter) Social workers could also have been helpful in addressing caregivers’ unmet psychosocial and practical needs. The following caregiver, whose loved one died of chronic obstructive pulmonary disease after a long illness, had few close family or friends.
I wish somebody could help me cope with a lot of things like with him passing and not being here. . .(I wish I could have had help) coping with grief. . .Like I said, I had already started grieving and missing him before he was even gone. . .after he
passed and I was here (home), I thought he’s never going to be here again. (Bereaved, Caucasian, wife)
Several caregivers were distressed by disrupted family dynamics or family conflict as a result of the illness.
I didn’t feel right bringing it (the conflict between the caregiver’s husband and sister-in-law) up. My husband is very private. I think if he (the social worker) had said to us, ‘‘Has there been family conflict because of the death of your mother?’’ I think that my husband might have opened up to him. (Bereaved, Caucasian, sister-in-law)
Finally, some would have liked more help with practical matters such as making funeral arrangements and estate planning.
We had to decide which funeral she (the patient) wanted. . .We had to get a funeral home. . .We also started looking into insurance policies. . .We knew that we had to take care of it. . .But we couldn’t do it (make funeral arrangements and estate planning) while she (patient) was there (in the hospi-tal). . .We knew this (the death) was coming. . .We should have prepared for this but nobody brought it (making funeral arrangements and estate planning) up. . .I wasn’t thinking about what to do next. (Bereaved, African American, niece)
DISCUSSION
Preparing for the death of a loved one is important to family caregivers of terminally ill patients. Among the factors that are important to preparing include receiving medical, practical, psycho-social, religious, or spiritual information, being provided with clear and accurate communication from credible health care providers, and having access to resources that allow one to complete tasks such as estate planning, funeral arrangements, etc. Although social workers clearly have expertise in each of these areas, we found that caregivers did not generally perceive hospital social workers as helpful in preparing them for the death. In addition, when asked what
health care providers could do to help better prepare them for the death, caregivers did not mention social workers, possibly implying that social workers did not have a role in or did not identify themselves as interested in preparing them for the death. Finally, despite not mentioning social workers, caregivers discussed several areas in with social workers could be helpful—areas such as facilitat-ing communication between health care providers and the family, counseling=providing support, conflict resolution, and helping access community resources. Although these skills are acquired as part of social work education, our caregivers did not connect them with hospital social workers.
Our findings that hospital social workers were not perceived as helpful to caregivers of terminally ill patients are in stark contrast to their historical role as advocates for families (Massachusetts General Hospital Social Work, (n.d.); Taylor-Brown & Sormanti, 2004). Because preparing families for the death remains an integral dimension hospital social work, a discussion of the barriers that social workers face is in order (Sheldon, 2000). It deserves mention that social workers’ attitudes about preparing caregivers are likely not the primary barriers. On the contrary, social workers perceive preparing caregivers as very important (Lord & Pockett, 1998; Luptak, 2004; Sheldon). Despite positive attitudes, however, social workers are constrained from preparing caregivers because of factors beyond their immediate control. The current health care environment is not very conducive to preparing caregivers (Colone, 1993). Traditionally, physicians and nurses relied on social workers to address the interrelationships between the physical, emotional, and social factors in disease. The push to control and decrease health care costs, however, has moved the role of the social worker away from psychosocial assessment and made discharge planning a major part of their practice (Holliman, Dziegielewski, & Datta, 2001). In fact, physicians now utilize social workers not for counseling but for assistance with patient discharges from the hospital or to obtain resources needed for care after discharge (Cowles & Lefcowitz, 1995; Mizrahi & Abramson, 2000). Economic realities have also led to larger caseloads which limit the number of psychosocial-oriented visits possible (Parker Oliver & Peck, 2006). Therefore, in busy, short-staffed, acute care units, social workers may not have the requi-site time to prepare caregivers. Second, role ambiguity may be a problem. More than ever, the social work role is blurring with that
of nurse case managers, which may in turn lead to competition for turf and autonomy (Ben-Sira & Szyf, 1992; Keigher, 1997; Mizrahi & Abramson). Physicians and social workers also sometimes disagree about who should best coordinate the care of patients and families (Abramson & Mizrahi, 2003). As a result, social workers may marginalize their role and defer to physicians for end-of-life com-munication (Back, 2000). Third, it is possible that hospital social workers may be involved too late in the end-of-life trajectory to prop-erly prepare caregivers for the death. Health care providers involved in discharge planning generally characterize palliative care as end-of-life or hospice care that is initiated after the decision to limit curative treatment is made (Rodriguez, Barnato, & Arnold, 2007). If palliative care is initiated very late in the illness trajectory, social work involve-ment with family caregivers may be limited. Finally, several studies have demonstrated that social workers receive very little exposure to palliative care during their training (Christ & Sormanti, 1999). A study of hospice social workers in two Southeastern states reported that more than 90% received less than 6 hours of formal education in palliative care (Arnold, Artin, Griffith, Person, & Graham, 2006). The training is often uneven and not sufficiently integrated into the broader social work education.
What can be done to overcome these barriers? The economic pres-sures that hinder social workers from preparing caregivers are not likely to go away. Nonetheless, given the important role that social workers can play in preparing caregivers for the death of a loved one, we believe social workers need to better advocate for expanding their role. A necessary step is for social work education to focus more specifically on the care of the dying and their families. Without better education, hospital social workers will lack role models who can lay the foundation for future training, leadership development, and advocacy. Next, preparing family caregivers for the death of a loved one is best done using the combined expertise of social workers, phy-sicians, nurses, clergy, etc. (Hebert, Prigerson, Schulz, & Arnold, 2006). Unlike many colleagues from these other disciplines, social workers are well versed in the intricacies of interdisciplinary teams. As such, they should take the lead in educating their colleagues about the benefits of interdisciplinary collaboration; many health care professionals are unaware of the expertise that social workers can bring to end-of-life care (Leipzig et al., 2002). Finally, one of the most convincing arguments that social workers can use for expanding their
role in end-of-life care is to demonstrate improved clinical outcomes or reduced costs because of their involvement (Clark, Rubenach, & Winsor, 2003; Miller et al., 2007).
Our findings should be placed in the context of several study limitations. First, our data was obtained from caregivers of patients seen at one university-based hospital and community-based hospice. With one exception, all patients had received care from the same hos-pital system. Social workers work in many other settings (e.g., nurs-ing homes, community, prisons, and pediatric hospitals) that care for terminally ill patients. Each has its own culture and regulations that may impact how social workers prepare caregivers. For example, the concept of family-centered care provided by social workers may be more established in pediatric hospitals than in adult hospitals (Gilmer, 2002). While the focus on hospital-based social work is certainly a limitation to the generalizabilty of our findings, we believe that it is a reasonable place to begin investigation as approximately 50% of all deaths in the United States occur in hospitals (National Center for Health Statistics, 2009). Nonetheless, it would be impor-tant to verify our findings in other hospitals and settings. In addition, approximately 80% of our sample was bereaved. Although caregivers perceived social workers as generally unhelpful, we have no data on what social workers actually did or did not do in regards to preparing caregivers. It is possible that caregivers’ perceptions of the helpfulness of social workers were negatively affected by the death itself. Finally, our study was not designed specifically to explore caregivers’ perceptions of social workers. Rather, the data was abstracted from data obtained from a larger project designed to explore the factors caregivers believe are important for preparing for the death of a loved one. Future work should be geared specifically to exploring this topic in more detail.
Implications for Practice
Family caregivers are invaluable to the care of patients with serious illness. Despite providing intense care, sometimes for years, many caregivers are not prepared for the death and may suffer more psychological morbidity as a result. The scope of social work training and practice makes social workers ideal professionals to help address this deficiency in end-of-life care. Addressing caregivers’ unmet needs are among the skills and competencies basic to the education
and training of social workers. Through this training, the expertise necessary to provide psychosocial support, facilitate communication between members of the interdisciplinary health care team, patients, and caregivers, and help caregivers access needed material, psycho-social, and spiritual resources is gained. The need for more social work intervention is clear from our sample. Our data demonstrate that hospital social workers may not be adequately preparing family caregivers. Future work should be directed to verifying our findings and determining how best to overcome the barriers that prevent hospital social workers from preparing caregivers for the death of a loved one.
REFERENCES
Abramson, J. S., & Mizrahi, T. (2003). Understanding collaboration between social workers and physicians: Application of a typology.Social Work in Health Care, 37(2), 71–100.
Arnold, E. M., Artin, K. A., Griffith, D., Person, J. L., & Graham, K. G. (2006). Unmet needs at the end of life: Perceptions of hospice social workers.Journal of Social Work in End-of-Life & Palliative Care,2(4), 61–83.
Back, A. (2000). Communication between professions: Doctors are from mars, social workers are from venus.Journal of Palliative Medicine,3(2), 221–222.
Barry, L. C., Kasl, S. V., & Prigerson, H. G. (2002). Psychiatric disorders among bereaved persons: The role of perceived circumstances of death and preparedness for death.American Journal of Geriatric Psychiatry,10(4), 447–457.
Barry, L. C., & Prigerson, H. G. (2002). Perspectives on preparedness for a death among bereaved persons.Connecticut Medicine,66(11), 691–696.
Ben-Sira, Z., & Szyf, M. (1992). Status inequality in the social worker-nurse collaboration in hospitals.Social Science and Medicine,34(4), 365–374.
Bern-Klug, M., Gessert, C., & Forbes, S. (2001). The need to revise assumptions about the end of life: Implications for social work practice.Health & Social Work, 26(1), 38–48.
Bern-Klug, M., Kramer, B. J., & Linder, J. F. (2005). All aboard: Advancing the social work research agenda in end-of-life and palliative care.Journal of Social Work in End-of-Life & Palliative Care,1(2), 71–86.
Berzoff, J., Lucas, G., Deluca, D., Gerbino, S., Browning, D., Foster, Z., et al. (2006). Clinical social work education in palliative and end-of-life care: Relational approaches for advanced practitioners. Journal of Social Work in End-of-Life & Palliative Care,2(2), 45–63.
Carey, M. (1995). Concerns in the analysis of focus group data.Qualitative Health Research,5(4), 487–495.
Christ, G. H., & Sormanti, M. (1999). Advancing social work practice in end-of-life care.Social Work in Health Care,30(2), 81–99.
Clark, M. S., Rubenach, S., Winsor, A. (2003). A randomized controlled trial of an education and counseling intervention for families after stroke. Clinical Rehabilitation,17(7), 703–712.
Clayton, J. M., Butow, P. N., Arnold, R. M., & Tattersall, M. H. (2005). Discussing end-of-life issues with terminally ill cancer patients and their carers: A qualitative study.Support Care and Cancer,13(8), 589–599.
Colone, M. (1993). Case management and managed care. Balancing quality and cost control.Social Work Administration,19(1), 7–10.
Cowles, L. A., & Lefcowitz, M. J. (1995). Interdisciplinary expectations of the medical social worker in the hospital setting: Part 2. Health & Social Work, 20(4), 279–286.
Emanuel, E. J., Fairclough, D. L., Slutsman, J., Alpert, H., Baldwin, D., & Emanuel, L. L. (1999). Assistance from family members, friends, paid care givers, and volunteers in the care of terminally ill patients.New England Journal of Medicine, 341(13), 956–963.
Fallowfield, L. J., Jenkins, V. A., & Beveridge, H. A. (2002). Truth may hurt but deceit hurts more: Communication in palliative care. Palliative Medicine,16(4), 297–303.
Gilmer, M. J. (2002). Pediatric palliative care: A family-centered model for critical care.Critical Care Nursing Clinics of North America,14(2), 207–214.
Gwyther, L. P., Altilio, T., Blacker, S., Christ, G., Csikai, E. L., Hooyman, N., et al. (2005). Social work competencies in palliative and end-of-life care. Journal of Social Work in End-of-Life & Palliative Care,1(1), 87–120.
Haley, W. E., LaMonde, L. A., Han, B., Narramore, S., & Schonwetter, R. (2001). Family caregiving in hospice: Effects on psychological and health functioning among spousal caregivers of hospice patients with lung cancer or dementia. Hospice Journal,15(4), 1–18.
Hanson, L. C., Danis, M., & Garrett, J. (1997). What is wrong with end-of-life care? Opinions of bereaved family members.Journal of the American Geriatrics Society, 45(11), 1339–1344.
Hebert, R. S., Dang, Q., & Schulz, R. (2006). Preparedness for the death of a loved one and mental health in bereaved caregivers of patients with dementia: Findings from the REACH study.Journal of Palliative Medicine,9(3), 683–693.
Hebert, R. S., Schulz, R., Copeland, V. C., & Arnold, R. M. (2008). What questions do family caregivers want to discuss with healthcare providers in order to prepare for the death of a loved one? An ethnographic study of caregivers of patients at end of life.Journal of Palliative Medicine,11(3): 476–483.
Hebert, R. S., Schulz, R., Copeland, V. C., & Arnold, R. M. (2009). Preparing family caregivers for death and bereavement. Insights from caregivers of terminally ill patients.Journal of Pain and Symptom Management,37(1), 3–12.
Hebert, R. S., Prigerson, H. G., Schulz, R., & Arnold, R. M. (2006). Preparing caregivers for the death of a loved one: A theoretical framework and suggestions for future research.Journal of Palliative Medicine,9(5), 1164–1171.
Holliman, D. C., Dziegielewski, S. F., & Datta, P. (2001). Discharge planning and social work practice.Social Work in Health Care,32(3), 1–19.
Keigher, S. M. (1997). What role for social work in the new health care practice paradigm?Health & Social Work,22(2), 149–155.
Kissane, D. W., Bloch, S., McKenzie, M., McDowall, A. C., & Nitzan, R. (1998). Family grief therapy: A preliminary account of a new model to promote healthy family functioning during palliative care and bereavement. Psycho-Oncology, 7(1), 14–25.
Kovacs, P. J., Bellin, M. H., & Fauri, D. P. (2006). Family-centered care: A resource for social work in end-of-life and palliative care.Journal of Social Work in End-of-Life & Palliative Care,2(1), 13–27.
Leipzig, R. M., Hyer, K., Ek, K., Wallenstein, S., Vezina, M. L., Fairchild, S., et al. (2002). Attitudes toward working on interdisciplinary healthcare teams: A comparison by discipline. Journal of the American Geriatrics Society, 50(6), 1141–1148.
Lord, B., & Pockett, R. (1998). Perceptions of social work intervention with bereaved clients: Some implications for hospital social work practice.Social Work & Health Care,27(1), 51–66.
Luptak, M. (2004). Social work and end-of-life care for older people: A historical perspective.Health & Social Work,29(1), 7–15.
MacQueen, K. M., McLellan, E., Kay, K., & Milstein, B. (1998). Codebook development for team-based qualitative analysis.Cultural Anthropology Methods, 10(2), 31–36.
Maguire, P. (1985). Barriers to psychological care of the dying. British Medical Journal (Clinical Research Edition),291(6510), 1711–1713.
Massachusetts General Hospital Social Work. (n.d.).Social work history.Retrieved November 22, 2007, from http://www.mghsocialwork.org/history.html
Miller, J. J., Frost, M. H., Rummans, T. A., Huschka, M., Atherton, P., Brown, P. et al. (2007). Role of a medical social worker in improving quality of life for patients with advanced cancer with a structured multidisciplinary intervention. Journal of Psychosocial Oncology,25(4), 105–119.
Mizrahi, T., & Abramson, J. S. (2000). Collaboration between social workers and physicians: Perspectives on a shared case.Social Work in Health Care,31(3), 1–24. National Center for Health Statistics. (2007).Deaths by place of death, age, race, and sex: United States, 1999–2004. Retrieved November 22, 2007, from http:// www.cdc.gov/nchs/data/dvs/MortFinal2004_Worktable309.pdf
National Center for Health Statistics. (2009).Faststats A to Z. Death and mortality 2004. Retrieved November 22, 2007, from http://www.cdc.gov/nchs/fastats/ deaths.htm
Parker, S. M., Clayton, J. M., Hancock, K., Walder, S., Butow, P. N., Carrick, S., et al. (2007). A systematic review of prognostic=end-of-life communication with adults in the advanced stages of a life-limiting illness: Patient=caregiver preferences for the content, style, and timing of information.Journal of Pain and Symptom Management, 34(1), 81–93.
Parker Oliver, D., & Peck, M. (2006). Inside the interdisciplinary team experiences of hospice social workers.Journal of Social Work in End-of-Life & Palliative Care, 2(3), 7–21.
Patton, M. Q. (2002).Qualitative research & evaluation methods. Thousand Oaks, CA: Sage Publications, Inc.
Quinn, A. (1998). Learning from palliative care: Concepts to underpin the transfer of knowledge for specialist palliative care to mainstream social work settings.Social Work Education,17(1), 9–20.
Rabow, M. W., Hauser, J. M., & Adams, J. (2004). Supporting family caregivers at the end of life: ‘‘They don’t know what they don’t know.’’Journal of the American Medical Association,291(4), 483–491.
Roberts, C. S., Baile, W. F., & Bassett, J. D. (1999). When the care giver needs care. Social Work in Health Care,30(2), 65–80.
Rodriguez, K. L., Barnato, A. E., & Arnold, R. M. (2007). Perceptions and utilization of palliative care services in acute care hospitals.Journal of Palliative Medicine,10(1), 99–110.
Rose, S. L., & Shelton, W. (2006). The role of social work in the ICU: Reducing family distress and facilitating end-of-life decision-making.Journal of Social Work in End-of-Life & Palliative Care,2(2), 3–23.
Russ, A. J., & Kaufman, S. R. (2005). Family perceptions of prognosis, silence, and the ‘‘suddenness’’ of death.Culture, Medicine and Psychiatry,29(1), 103–123. Sheldon, F. M. (2000). Dimensions of the role of the social worker in palliative care.
Palliative Medicine,14(6), 491–498.
Steinhauser, K. E., Christakis, N. A., Clipp, E. C., McNeilly, M., Grambow, S., Parker, J., et al. (2001). Preparing for the end of life: Preferences of patients, families, physicians, and other care providers. Journal of Pain and Symptom Management,22(3), 727–737.
Taylor-Brown, S., & Sormanti, M. (2004). End-of-life care.Health & Social Work, 29(1), 3–5.
Teno, J. M., Clarridge, B. R., Casey, V., Welch, L. C., Wetle, T., Shield, R., et al. (2004). Family perspectives on end-of-life care at the last place of care.Journal of the American Medical Association,291(1), 88–93.
Zittle, K. M., Lawrence, S., & Wodarski, J. S. (2002). Biopsychosocial model of health and healing: Implications for health social work practice.Journal of Human Behavior in the Social Environment,5(1), 19–33.
Date Received: 12/04/07 Date Revised: 02/03/08 Date Accepted: 02/18/08