Relationship between Vancomycin-Resistant
Staphylococcus aureus
,
Vancomycin-Intermediate
S. aureus
, High Vancomycin MIC, and
Outcome in Serious
S. aureus
Infections
Natasha E. Holmes,a,bPaul D. R. Johnson,a,b,dand Benjamin P. Howdena,c,d,e
Austin Centre for Infection Research (ACIR), Department of Infectious Diseases, Austin Health, Heidelberg, Victoria,a
Department of Medicine, University of Melbourne, Parkville, Victoria,b
Department of Microbiology, Austin Health, Heidelberg, Victoria,c
Department of Microbiology, Monash University, Clayton, Victoria,d
and Department of Microbiology and Immunology, University of Melbourne, Parkville, Victoria, Australiae
Vancomycin has been used successfully for over 50 years for the treatment ofStaphylococcus aureusinfections, particularly those involving methicillin-resistantS. aureus. It has proven remarkably reliable, but its efficacy is now being questioned with the emergence of strains ofS. aureusthat display heteroresistance, intermediate resistance, and, occasionally, complete vanco-mycin resistance. More recently, an association has been established between poor outcome and infections with strains ofS. au-reuswith an elevated vancomycin MIC within the susceptible range. This minireview summarizes the definitions, mechanisms, clinical impact, and laboratory identification of reduced vancomycin susceptibility inS. aureusand discusses practical issues for the diagnostic laboratory in testing and interpreting vancomycin susceptibility forS. aureusinfections.
HISTORY AND DEFINITION OF REDUCED VANCOMYCIN
SUSCEPTIBILITY INSTAPHYLOCOCCUS AUREUS
V
ancomycin, a glycopeptide with activity against a wide range of Gram-positive organisms, was discovered in 1952 and by 1958 was registered by the U.S. Food and Drug Administration for treatment of penicillin-resistant and methicillin-resistant Staphy-lococcus aureus. Unlike the rapid appearance ofS. aureusresistant to penicillin and semisynthetic penicillins, reduced susceptibility or resistance to vancomycin took over 3 decades to emerge. Strains ofS. aureusdisplaying vancomycin heteroresistance (hVISA) and vancomycin intermediate resistance (VISA) were first isolated in Japan in 1996 (8). hVISA strains are phenotypically susceptible using broth microdilution (BMD); however, testing in greater de-tail reveals subpopulations of cells with reduced susceptibility to vancomycin. Vancomycin-resistant S. aureus (VRSA) strains whose resistance is due to acquisition of thevanAresistance de-terminant from enterococci were subsequently reported in the United States, in 2002. VRSA has also been described in Iran and India, although it remains rare worldwide.Differences in vancomycin breakpoints.In the United States, the Clinical and Laboratory Standards Institute (CLSI) reduced the vancomycin MIC susceptibility breakpoint forS. aureusfrom 4g/ml to 2g/ml in 2006 (3). Therefore, any literature pub-lished before this date needs careful appraisal, as the definitions of the susceptible, intermediate, and resistant categories have now changed. VISA and VRSA are currently defined using BMD as exhibiting vancomycin MICs of 4 to 8g/ml andⱖ16g/ml, respectively (3). In contrast, both the European Committee on Antimicrobial Susceptibility Testing (EUCAST) and the British Society for Antimicrobial Chemotherapy simply defineS. aureus
strains as vancomycin susceptible (MICⱕ2g/ml) or resistant (MIC⬎2g/ml) (1,6). The reasons cited for this definition are difficulties in confirming heteroresistance and avoiding confusion for clinicians, because there is a likelihood of clinical treatment failure when vancomycin is used to treat infections where the MIC is above 2g/ml.
Definition of hVISA. Although it is accepted that hVISA strains are phenotypically susceptible to vancomycin by routine laboratory methods but contain vancomycin-intermediate sub-populations on culture, there is no precise definition for hVISA. These subpopulations are typically present at frequencies of 10⫺6
to 10⫺4. Population analysis profile (PAP) testing remains the gold standard for detection of these subpopulations (7,8,33). One example is the modified PAP method by Wootton et al. (33) in which the area under the curve (5) of a PAP test (PAP/AUC) determined in a comparison of a test organism to hVISA reference strain Mu3 (ATCC 700698) is calculated. Using this method, van-comycin-susceptibleS. aureus(VSSA) is defined with a PAP/AUC ratio⬍0.9 and hVISA with a PAP/AUC ratioⱖ0.9.
While earlier studies focused on the role of VISA and hVISA in vancomycin treatment failure, there are now increasing reports of poor clinical outcomes inS. aureusinfections where the vancomy-cin MIC is in the upper end of the susceptible range (ⱕ2g/ml) and hVISA has been excluded (29). The proportion ofS. aureus
isolates that are hVISA increases as the vancomycin MIC in-creases, and the differences between VSSA, hVISA, and VISA are accordingly subtle and may represent a continuum of small incre-mental changes in MIC and other characteristics. In contrast, VRSA is a separate entity, with acquisition of thevanAgene con-ferring complete vancomycin resistance in the majority of re-ported strains.
MECHANISMS OF REDUCED VANCOMYCIN SUSCEPTIBILITY
Cell wall.Sequential mutations in VSSA lead to the emergence of hVISA and ultimately VISA. The hallmark changes are alterations in the bacterial cell wall resulting in reduced autolytic activity and
Published ahead of print16 May 2012
Address correspondence to Benjamin Howden, [email protected].
Copyright © 2012, American Society for Microbiology. All Rights Reserved.
doi:10.1128/JCM.00775-12
on May 16, 2020 by guest
http://jcm.asm.org/
wall thickening. This is thought to result in an impaired ability of vancomycin to reach its binding site and occurs specifically during the cell cycle when the division septum is being formed. These changes are particularly noted after prior exposure to vancomycin (4,13). Multiple genetic mutations have been implicated in the pathogenesis of these cell wall modifications, usually occurring in genes important for cell wall metabolism such asvraRS(15) and
graRS; however, recent attention has focused on the essentialS. aureusregulatorwalKR(14).
Accessory gene regulator locus.Differences in the accessory gene regulator (agr) quorum-sensing-system locus have also been associated with vancomycin heteroresistance.agrtypes I and II have been associated with vancomycin resistance (32), while alteredagr
function leading to reduction in RNA III transcription and delta-hemolysin production has also been linked with resistance (26).
Other changes in hVISA.Often, multiple small sequential changes lead to stepwise generation of hVISA and VISA (12). A number of other changes have been connected with vancomycin heteroresistance, including metabolic changes, altered surface proteins or muropeptides, reduced growth kinetics, and attenu-ated virulence (12,23).
While the genetic determinants of hVISA and VISA are par-tially understood, the relative contributions of these mutations— and of altered cellular processes that contribute to hVISA and VISA—in determining the vancomycin MIC are unknown.
CLINICAL IMPACT OF hVISA, VISA, AND ELEVATED VANCOMYCIN MIC
Clinical features of hVISA and VISA.The spectrum of clinical disease caused by hVISA and VISA is similar to that caused by VSSA, but the prevalence and clinical impact are difficult to de-termine due to the lack of a standardized definition and absence of controlled prospective studies. High-inoculum infections such as bacteremia, endocarditis and osteomyelitis (2,19), and persistent bacteremia (13,16, 19) have been associated with vancomycin heteroresistance, and this may lead to vancomycin treatment fail-ure (2) or other complications (19). However, it is difficult to determine whether hVISA is the cause or corollary of treatment failure in some studies, especially if it is not clear when the hVISA or VISA isolate was detected in the course of the infection. Inter-estingly, one study noted reduced rates of shock in patients with heteroresistant infections compared with VSSA infections (28), possibly demonstrating a clinical correlate of the attenuated viru-lence noted in animal models of VISA infection.
Interestingly, pooled data from a recent meta-analysis demon-strated similar mortality rates for VSSA and hVISA infections; however, treatment failure was more common in the hVISA group (30). Other studies that include infections of lesser severity have reported comparable outcomes and questioned the clinical rele-vance of hVISA (11).
Elevated vancomycin MIC.Clinical factors associated with an elevated vancomycin MIC are similar to those associated with the development of hVISA and include prior vancomycin exposure (18), prior methicillin-resistant S. aureus (MRSA) bacteremia, and increased patient age.
Although rates of hVISA detection by PAP/AUC analysis in-crease as the vancomycin MIC determined by BMD inin-creases (22,
25), increased mortality and treatment failure have also been re-ported in infections with VSSA isolates with an elevated vancomy-cin MIC in the fully susceptible range (10,27–29). Typically, these
isolates have MICs near the susceptibility breakpoint such as 1.5 or 2g/ml, as determined using different MIC methodologies. This has created debate about whether vancomycin susceptibility breakpoints should be reduced further; however, it is difficult to ascertain an appropriate new breakpoint from these studies, as they represent significant heterogeneity in clinical features and infection types, different MIC testing methods, and different MIC values associated with inferior outcomes. In addition, hVISA was not assessed in many of these studies.
The underlying mechanism by which an elevated vancomycin MIC in VSSA causes inferior outcomes has not yet been eluci-dated. It has been suggested that vancomycin treatment be avoided in these situations, as it is presumed that the continuum of changes that lead to reduced vancomycin susceptibility and hVISA is implicated in the development of resistance. In addition, reduced vancomycin bactericidal activity in VSSA isolates with an elevated vancomycin MICin vitrohas been previously noted (27). However, differences in bacterial genotype may be an alterna-tive explanation, with recent publications highlighting associa-tions between genotype and elevated vancomycin MIC. This is particularly relevant, as elevated vancomycin MIC and inferior outcomes in treatment of VSSA infections are not merely confined to MRSA but also occur in cases of methicillin-susceptibleS. au-reus(MSSA) infection (10), including patients receiving beta-lac-tam therapy. An elevated vancomycin MIC may therefore be a surrogate marker for an unknown mechanism leading to treat-ment failure.
LABORATORY IDENTIFICATION OF hVISA, VISA, AND ELEVATED VANCOMYCIN MIC
The lack of a precise definition and standardized testing makes optimum detection of hVISA difficult, as these strains are missed by routine susceptibility tests and relying on vancomycin MIC alone is not sufficient.
Colony morphology.There may be relevant clues when eval-uating growth characteristics on conventional agar plates, as hVISA strains may have altered growth kinetics. Careful observa-tion may reveal smaller-sized colonies or mixed small-colony variants (SCV) among normal colonies in a pure culture, reduced pigmentation and hemolysis, and slower growth (12,20). These changes may be subjective and are not diagnostic, and their obser-vation should not replace confirmatory testing.
Screening tests for hVISA.Due to the low frequency of vanco-mycintermediate subpopulations in hVISA infections, the low in-oculum required for BMD MIC testing is insufficient to detect these subpopulations. Consequently, methods for hVISA detection use a higher inoculum, prolonged incubation (to promote growth of resis-tant subpopulations), or more nutritious agar (12).
The macromethod Etest (MET) is a screening test for hVISA that uses a higher inoculum (2 McFarland standard) and a longer incubation (48 h). A positive test is reported if the teicoplanin MIC isⱖ12g/ml or if the teicoplanin MIC isⱖ8g/ml and the vancomycin MIC is alsoⱖ8g/ml. The actual MIC result cannot be reported, because the method differs from the standard MIC calculation. An alternative screening test is the glycopeptide resis-tance detection (GRD) Etest, which uses a double-ended Etest strip and a standard inoculum (0.5 McFarland) on Mueller-Hin-ton–5% blood agar. A positive GRD result is reported if the van-comycin or teicoplanin MIC isⱖ8g/ml. A number of screening
on May 16, 2020 by guest
http://jcm.asm.org/
agar plates have also been developed; however, the sensitivity has been variable (12).
These Etest screening tests have been compared with the gold standard PAP and shown to have good sensitivity and specificity (34), although a recent report suggested that MET and GRD did not perform as well as expected (31). Ultimately, any screening test should undergo confirmatory testing with PAP/AUC before any positive result is reported.
A novel method for rapid identification of hVISA or VISA from clinical isolates within 4 h using multiplexed automated dig-ital microscopy has recently been described (21). Results were correlated with PAP analysis, and further studies are required to determine its clinical utility.
Confirmatory tests for hVISA. The definitive method for identifying hVISA is the population analysis profile (PAP); how-ever, it is time-consuming, labor-intensive, and difficult to apply in real-time clinical decisionmaking due to delayed test results. The modified PAP/AUC method described by Wootton et al. (33) compares the PAP/AUC of reference hVISA strain Mu3 with that of a test organism, with PAP/AUC values of⬍0.9, 0.9 to 1.3, and
⬎1.3 for VSSA, hVISA, and VISA, respectively.
As the genetic determinants for hVISA are still being delineated and involve different mechanisms, there is no specific molecular assay for diagnosis or detection currently available in either the research or diagnostic laboratory.
VISA and VRSA.Detection of VISA and VRSA is easier, as there are defined CLSI MIC criteria. Note that these have been defined using the reference BMD method. Results determined us-ing other MIC methods should always be confirmed with BMD prior to reporting.
Vancomycin MIC. The reference method for vancomycin MIC is BMD. As this is labor-intensive and time-consuming, many diagnostic laboratories assess vancomycin susceptibility us-ing other methods such as agar dilution, Etest, disc diffusion, and commercial instrument-based assays (for example, Vitek-2, Phoenix, and Microscan). Unfortunately, these methodologies produce subtle differences in MIC results compared with BMD, with Etest results consistently a 1-fold dilution (or 0.5 to 1.5 log2
dilutions) higher than reference BMD results (10,17,24). Note that automated methods are required to align with BMD for U.S. Food and Drug Administration licensing. Many studies that have evaluated vancomycin MIC and treatment outcomes have noted that an elevated Etest MIC predicts poor outcome and the hVISA phenotype better than BMD, often by around 1.5g/ml (consti-tuting a half-dilution step when using traditional BMD) (9,29).
The implications of vancomycin MIC and methodology are relevant and crucial in considering vancomycin pharmacodynam-ics. The area under the curve over 24 h in the steady state divided by the MIC (AUC/MIC ratio) is the best predictor of vancomycin efficacy. Small variations in the MIC therefore lead to significant changes in the AUC/MIC ratio. In addition, the optimal vancomycin AUC/MIC targets were devised using the BMD MIC methodology.
HOW SHOULD THE DIAGNOSTIC LABORATORY TEST AND
INTERPRET VANCOMYCIN SUSCEPTIBILITY INS. AUREUS?
[image:3.585.41.545.77.284.2]Vancomycin MIC.From a practical viewpoint, the relevance of the different vancomycin susceptibility breakpoints according to CLSI, EUCAST, or BSAC adopted by individual laboratories may be less important than other information provided in a laboratory report or by direct liaison with the clinician. The MIC method
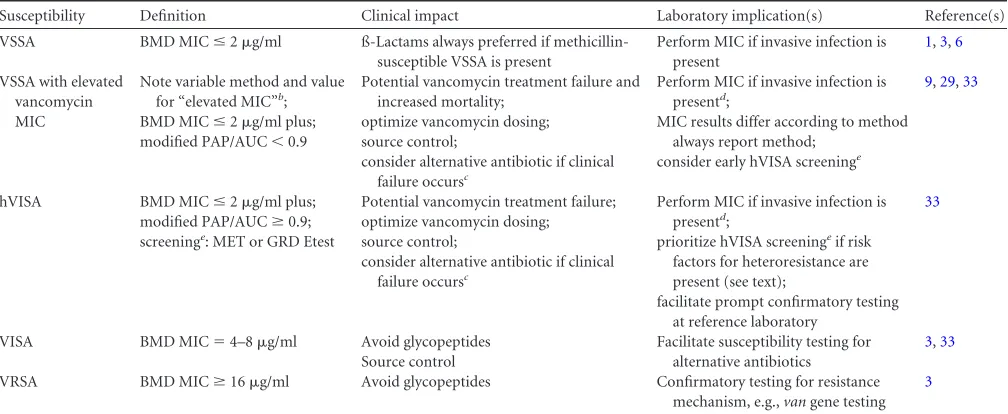
TABLE 1Summary of key points addressing vancomycin susceptibility inS. aureusand implications for the diagnostic laboratorya
Susceptibility Definition Clinical impact Laboratory implication(s) Reference(s)
VSSA BMD MICⱕ2g/ml ß-Lactams always preferred if
methicillin-susceptible VSSA is present
Perform MIC if invasive infection is present
1,3,6
VSSA with elevated vancomycin MIC
Note variable method and value for “elevated MIC”b;
Potential vancomycin treatment failure and increased mortality;
Perform MIC if invasive infection is presentd;
9,29,33
BMD MICⱕ2g/ml plus; optimize vancomycin dosing; MIC results differ according to method
always report method;
modified PAP/AUC⬍0.9 source control;
consider alternative antibiotic if clinical failure occursc
consider early hVISA screeninge
hVISA BMD MICⱕ2g/ml plus; Potential vancomycin treatment failure; Perform MIC if invasive infection is
presentd;
33
modified PAP/AUCⱖ0.9; optimize vancomycin dosing;
screeninge: MET or GRD Etest source control; prioritize hVISA screeningeif risk
consider alternative antibiotic if clinical factors for heteroresistance are
failure occursc present (see text);
facilitate prompt confirmatory testing at reference laboratory
VISA BMD MIC⫽4–8g/ml Avoid glycopeptides Facilitate susceptibility testing for
alternative antibiotics
3,33 Source control
VRSA BMD MICⱖ16g/ml Avoid glycopeptides Confirmatory testing for resistance
mechanism, e.g.,vangene testing 3
aBMD, broth microdilution; PAP/AUC, area under the curve of standard population analysis profile graph; MET, macromethod Etest; GRD, glycopeptide resistance detection;
VSSA, vancomycin-susceptibleS. aureus; hVISA, heterogeneous vancomycin-intermediateS. aureus; VISA, vancomycin-intermediateS. aureus; VRSA, vancomycin-resistantS. aureus.
b
The Etest and a result⬎1g/ml appear to be the MIC method and value most predictive of vancomycin treatment failure and increased mortality, as reported in several publications.
c
There is no standardized definition of clinical failure; however, criteria may include persistent or relapsed bacteremia, development of new hemodynamic instability, or persistent fevers with worsening inflammatory markers.
d
The laboratory report should include MIC method and value with a comment such as “for further information, please discuss this result with the laboratory or with clinical infectious diseases or microbiology staff members.”
e
hVISA screening method dependent on laboratory workflow, preferences, and practices, e.g., Etest-based methods (MET, GRD).
on May 16, 2020 by guest
http://jcm.asm.org/
should always be stated, because clinicians need to be mindful of MIC methodology if using the MIC result for therapeutic deci-sions (for example, pharmacodynamic and dosing consider-ations). As a number of studies have shown that the Etest MIC test seems to predict treatment failure better than BMD testing, this may be a convenient and practical MIC determination method.
Interpretation of susceptibility results should occur in discus-sion with relevant clinical personnel such as infectious-disease pharmacists and physicians, clinical microbiologists, and hospital antimicrobial-committee members. It may be prudent to recom-mend caution about increased risks of vancomycin treatment fail-ure for isolates with MIC⬎1g/ml (regardless of the test method and irrespective of heteroresistance) (9,29). However, it is also important to remember that the clinical context is important, and patients who are responding to vancomycin may not automati-cally need to be switched to an alternative agent merely in response to an elevated vancomycin MIC laboratory result.
hVISA.The ideal manner for detection of vancomycin hetero-resistance is dependent on many factors such as the laboratory workload, number of specimens, capacity to perform more-de-tailed tests, and cost. More importantly, the selection of isolates that undergo hVISA testing must be considered carefully, as it is not feasible to test allS. aureusclinical isolates. Clinically based and laboratory-based algorithms have been proposed to guide the screening and confirmatory testing process (12). Patients at in-creased risk of heteroresistance and vancomycin treatment failure (with risk factors such as older age, prior vancomycin treatment, previous MRSA infection, and high bacterial burden infections) should be prioritized for hVISA screening as early as possible in order to facilitate results being made available in a clinically mean-ingful time frame. Again, the decision to change therapy from vancomycin to alternative agents needs to be based on the clinical context and not purely on laboratory susceptibility results.
Although several screening tests have reasonable sensitivity and specificity and can be helpful in that they may be conducted in a more timely fashion before PAP/AUC determinations are per-formed, a confirmatory test should always be performed on any isolate referred for hVISA testing for a definitive result.Table 1
summarizes some of these key points, including the clinical im-pact of vancomycin susceptibility and implications for the diag-nostic laboratory.
Vancomycin has been the workhorse antibiotic for MRSA in-fections for over 50 years. Although the area of vancomycin het-eroresistance and susceptibility testing has become complicated, rates of VRSA and VISA are still relatively low whereas hVISA is more common. In order to facilitate more-rapid testing for hVISA and VISA, further understanding of the molecular changes asso-ciated with heteroresistance is required. Additional knowledge about the relationship between elevated vancomycin MIC and treatment outcome in cases of VSSA infection is urgently required to clarify the ongoing role of vancomycin in the treatment of se-riousS. aureusinfections.
ACKNOWLEDGMENTS
This work was supported by the National Health and Medical Research Council (NHMRC) of Australia.
REFERENCES
1.British Society for Antimicrobial Chemotherapy (BSAC).2011. BSAC methods for antimicrobial susceptibility testing, version 10.2. British
So-ciety for Antimicrobial Chemotherapy, Birmingham, United Kingdom. http://www.bsac.org.uk/Susceptibility⫹Testing/Breakpoints.
2.Charles PG, Ward PB, Johnson PD, Howden BP, Grayson ML.2004. Clinical features associated with bacteremia due to heterogeneous vanco-mycin-intermediate Staphylococcus aureus. Clin. Infect. Dis.38:448 – 451.
3.Clinical and Laboratory Standards Institute (CLSI).2006. Methods for dilution antimicrobial susceptibility tests for bacteria that grow aerobi-cally; approved standard—seventh edition. CLSI document M07-A7. CLSI, Wayne, Philadelphia, PA.
4.Cui L, Murakami H, Kuwahara-Arai K, Hanaki H, Hiramatsu K.2000. Contribution of a thickened cell wall and its glutamine nonamidated com-ponent to the vancomycin resistance expressed by Staphylococcus aureus Mu50. Antimicrob. Agents Chemother.44:2276 –2285.
5.Elsaghier AA, Aucken HM, Hamilton-Miller JM, Shaw S, Kibbler CC.
2002. Resistance to teicoplanin developing during treatment of methicil-lin-resistant Staphylococcus aureus infection. J. Antimicrob. Chemother.
49:423– 424.
6. European Committee on Antimicrobial Susceptibility Testing (EUCAST).2011. MIC and inhibition zone diameter distributions of mi-croorganisms without and with resistance mechanisms. EUCAST, Växjö, Sweden.http://www.eucast.org/mic_distributions/.
7.Hiramatsu K.2001. Vancomycin-resistant Staphylococcus aureus: a new model of antibiotic resistance. Lancet Infect. Dis.1:147–155.
8.Hiramatsu K, et al.1997. Dissemination in Japanese hospitals of strains of Staphylococcus aureus heterogeneously resistant to vancomycin. Lancet
350:1670 –1673.
9.Holland TL, Fowler VG, Jr. 2011. Vancomycin minimum inhibitory concentration and outcome in patients with Staphylococcus aureus bac-teremia: pearl or pellet? J. Infect. Dis.204:329 –331.
10. Holmes NE, et al.2011. Antibiotic choice may not explain poorer out-comes in patients With Staphylococcus aureus bacteremia and high van-comycin minimum inhibitory concentrations. J. Infect. Dis.204:340 –347. 11. Horne KC, et al.2009. Prospective comparison of the clinical impacts of heterogeneous vancomycin-intermediate methicillin-resistant Staphylo-coccus aureus (MRSA) and vancomycin-susceptible MRSA. Antimicrob. Agents Chemother.53:3447–3452.
12. Howden BP, Davies JK, Johnson PD, Stinear TP, Grayson ML.2010. Reduced vancomycin susceptibility in Staphylococcus aureus, including vancomycin-intermediate and heterogeneous vancomycin-intermediate strains: resistance mechanisms, laboratory detection, and clinical implica-tions. Clin. Microbiol. Rev.23:99 –139.
13. Howden BP, Johnson PD, Ward PB, Stinear TP, Davies JK. 2006. Isolates with low-level vancomycin resistance associated with persistent methicillin-resistant Staphylococcus aureus bacteremia. Antimicrob. Agents Chemother.50:3039 –3047.
14. Howden BP, et al.2011. Evolution of multidrug resistance during Staph-ylococcus aureus infection involves mutation of the essential two
compo-nent regulator WalKR. PLoS Pathog. 7:e1002359. doi:10.1371/
journal.ppat.1002359.
15. Howden BP, et al.2008. Genomic analysis reveals a point mutation in the two-component sensor gene graS that leads to intermediate vancomycin resistance in clinical Staphylococcus aureus. Antimicrob. Agents Che-mother.52:3755–3762.
16. Howden BP, et al. 2004. Treatment outcomes for serious infections caused by methicillin-resistant Staphylococcus aureus with reduced van-comycin susceptibility. Clin. Infect. Dis.38:521–528.
17. Hsu DI, et al.2008. Comparison of method-specific vancomycin mini-mum inhibitory concentration values and their predictability for treat-ment outcome of meticillresistant Staphylococcus aureus (MRSA) in-fections. Int. J. Antimicrob. Agents32:378 –385.
18. Lodise TP, et al.2008. Predictors of high vancomycin MIC values among patients with methicillin-resistant Staphylococcus aureus bacteraemia. J. Antimicrob. Chemother.62:1138 –1141.
19. Maor Y, et al.2009. Clinical features of heteroresistant vancomycin-intermediate Staphylococcus aureus bacteremia versus those of methicil-lin-resistant S. aureus bacteremia. J. Infect. Dis.199:619 – 624.
20. Marlowe EM, Cohen MD, Hindler JF, Ward KW, Bruckner DA.2001. Practical strategies for detecting and confirming vancomycin-intermediate Staphylococcus aureus: a tertiary-care hospital laboratory’s experience. J. Clin. Microbiol.39:2637–2639.
21. Metzger S, Price CS, Dunne WMJ, Howson D.2011. Automated 4-hour detection of heteroresistant vancomycin-intermediate Staphylococcus
on May 16, 2020 by guest
http://jcm.asm.org/
aureus (hVISA), poster 083. Abstr. 111th Gen. Meet. Am. Soc. Microbiol., New Orleans, LA. American Society for Microbiology, Washington, DC. 22. Musta AC, et al.2009. Vancomycin MIC plus heteroresistance and
out-come of methicillin-resistant Staphylococcus aureus bacteremia: trends over 11 years. J. Clin. Microbiol.47:1640 –1644.
23. Peleg AY, et al.2009. Reduced susceptibility to vancomycin influences pathogenicity in Staphylococcus aureus infection. J. Infect. Dis.199:532– 536.
24. Prakash V, Lewis JS II, Jorgensen JH. 2008. Vancomycin MICs for methicillin-resistant Staphylococcus aureus isolates differ based upon the susceptibility test method used. Antimicrob. Agents Chemother.52:4528. doi:10.1128/AAC.00904-08.
25. Rybak MJ, et al.2008. Characterization of vancomycin-heteroresistant Staphylococcus aureus from the metropolitan area of Detroit, Michigan, over a 22-year period (1986 to 2007). J. Clin. Microbiol.46:2950 –2954. 26. Sakoulas G, et al.2002. Accessory gene regulator (agr) locus in
geograph-ically diverse Staphylococcus aureus isolates with reduced susceptibility to vancomycin. Antimicrob. Agents Chemother.46:1492–1502.
27. Sakoulas G, et al.2004. Relationship of MIC and bactericidal activity to efficacy of vancomycin for treatment of methicillin-resistant Staphylococ-cus aureus bacteremia. J. Clin. Microbiol.42:2398 –2402.
28. Soriano A, et al.2008. Influence of vancomycin minimum inhibitory
concentration on the treatment of methicillin-resistant Staphylococcus aureus bacteremia. Clin. Infect. Dis.46:193–200.
29. van Hal SJ, Lodise TP, Paterson DL.2012. The clinical significance of vancomycin minimum inhibitory concentration in Staphylococcus au-reus infections: a systematic review and meta-analysis. Clin. Infect. Dis.
54:755–771.
30. van Hal SJ, Paterson DL.2011. Systematic review and meta-analysis of the significance of heterogeneous vancomycin-intermediate Staphylococ-cus aureus isolates. Antimicrob. Agents Chemother.55:405– 410. 31. van Hal SJ, et al.2011. Performance of various testing methodologies for
detection of heteroresistant vancomycin-intermediate Staphylococcus aureus in bloodstream isolates. J. Clin. Microbiol.49:1489 –1494. 32. Verdier I, et al.2004. Staphylococcus aureus isolates with reduced
sus-ceptibility to glycopeptides belong to accessory gene regulator group I or II. Antimicrob. Agents Chemother.48:1024 –1027.
33. Wootton M, et al.2001. A modified population analysis profile (PAP) method to detect hetero-resistance to vancomycin in Staphylococcus au-reus in a UK hospital. J. Antimicrob. Chemother.47:399 – 403. 34. Yusof A, et al.2008. Evaluation of a new Etest vancomycin-teicoplanin
strip for detection of glycopeptide-intermediate Staphylococcus aureus (GISA), in particular, heterogeneous GISA. J. Clin. Microbiol.46:3042– 3047.