Serologic Screening for Genital Herpes
An Updated Evidence Report and Systematic Review
for the US Preventive Services Task Force
Cynthia Feltner, MD, MPH; Catherine Grodensky, MPH; Charles Ebel, BA; Jennifer C. Middleton, PhD; Russell P. Harris, MD, MPH; Mahima Ashok, PhD, MS; Daniel E. Jonas, MD, MPH
IMPORTANCEGenital herpes simplex virus (HSV) infection is a prevalent sexually transmitted
infection. Vertical transmission of HSV can lead to fetal morbidity and mortality.
OBJECTIVETo assess the evidence on serologic screening and preventive interventions for genital HSV infection in asymptomatic adults and adolescents to support the US Preventive Services Task Force for an updated recommendation statement.
DATA SOURCESMEDLINE, Cochrane Library, EMBASE, and trial registries through March 31, 2016. Surveillance for new evidence in targeted publications was conducted through October 31, 2016.
STUDY SELECTIONEnglish-language randomized clinical trials (RCTs) comparing screening with no screening in persons without past or current symptoms of genital herpes; studies evaluating accuracy and harms of serologic screening tests for HSV-2; RCTs assessing preventive interventions in asymptomatic persons seropositive for HSV-2.
DATA EXTRACTION AND SYNTHESISDual review of abstracts, full-text articles, and study quality; pooled sensitivities and specificities of screening tests using a hierarchical summary receiver operating characteristic curve analysis when at least 3 similar studies were available.
MAIN OUTCOMES AND MEASURESAccuracy of screening tests, benefits of screening, harms of screening, reduction in genital herpes outbreaks.
RESULTSA total of 17 studies (n = 9736 participants; range, 24-3290) in 19 publications were included. No RCTs compared screening with no screening. Most studies of the accuracy of screening tests were from populations with high HSV-2 prevalence (greater than 40% based on Western blot). Pooled estimates of sensitivity and specificity of the most commonly used test at the manufacturer’s cutpoint were 99% (95% CI, 97%-100%) and 81% (95% CI, 68%-90%), respectively (10 studies; n = 6537). At higher cutpoints, pooled estimates were 95% (95% CI, 91%-97%) and 89% (95% CI, 82%-93%), respectively (7 studies; n = 5516). Use of this test at the manufacturer’s cutpoint in a population of 100 000 with a prevalence of HSV-2 of 16% (the seroprevalence in US adults with unknown symptom status) would result in 15 840 true-positive results and 15 960 false-positive results (positive predictive value, 50%). Serologic screening for genital herpes was associated with psychosocial harms, including distress and anxiety related to positive test results. Four RCTs compared preventive medications with placebo, 2 in nonpregnant asymptomatic adults who were HSV-2
seropositive and 2 in HSV-2–serodiscordant couples. Results in both populations were heterogeneous and inconsistent.
CONCLUSIONS AND RELEVANCESerologic screening for genital herpes is associated with a high rate of false-positive test results and potential psychosocial harms. Evidence from RCTs does not establish whether preventive antiviral medication for asymptomatic HSV-2 infection has benefit.
JAMA. 2016;316(23):2531-2543. doi:10.1001/jama.2016.17138
Editorialpage 2493
Related articlepage 2525
Supplemental content
CME Quizat jamanetworkcme.com
Related articleat jamadermatology.com
Author Affiliations:RTI
International–University of North Carolina at Chapel Hill Evidence-based Practice Center (Feltner, Grodensky, Middleton, Harris, Ashok, Jonas); Cecil G. Sheps Center for Health Services Research, University of North Carolina at Chapel Hill (Feltner, Middleton, Harris, Jonas); Department of Medicine, University of North Carolina at Chapel Hill (Feltner, Harris, Jonas); RTI International, Research Triangle Park, North Carolina (Ebel, Ashok).
Corresponding Author:Cynthia
G
enital herpes is a sexually transmitted infection (STI) caused by herpes simplex virus (HSV) type 1 or type 2. Many pa-tients experience signs and symptoms during primary in-fection and recurrences, but some may have mild or no symptoms.1 Episodic subclinical viral shedding leads to the potential for trans-mission in the absence of symptoms.2,3HSV-2 accounts for most prevalent genital herpes cases and is more likely to cause frequent symptomatic recurrences than HSV-1 (which is most commonly ac-quired in childhood and associated with orofacial infection).4-6 Genital HSV infection during pregnancy poses a risk of neonatal trans-mission during delivery, particularly among women who acquire HSV near the time of delivery.1,7
The true prevalence of asymptomatic HSV-2 infection is un-known; prevalence estimates rely on serologic test results and are not confirmed with Western blot. The estimated seroprevalence of HSV-2 in the United States was 16% in 2005-2010; only 14% of se-ropositive persons reported having been diagnosed with genital herpes.6
It is unclear what proportion of HSV-2–seropositive par-ticipants with no prior diagnosis of genital herpes had true asymp-tomatic (or unrecognized) infection vs a false-positive test result.
In theory, screening to identify unrecognized HSV-2 infection followed by counseling, antiviral treatment (episodic or sup-pressive), or both could prevent transmission and reduce symp-toms and shedding. Several US Food and Drug Administration (FDA)–approved type-specific HSV serologic tests are available.8 Since HSV-2 rarely causes infection outside the anogenital region, HSV-2 antibodies can be interpreted as an indicator of genital infection.
In 2005, the US Preventive Services Task Force (USPSTF) rec-ommended against routine serologic screening for HSV in asymp-tomatic adolescents, adults, and pregnant women (grade D recommendation).9
To inform an updated recommendation, we re-viewed the evidence on benefits and harms of serologic screening for HSV-2, screening test accuracy, and benefits and harms of anti-viral treatment in populations relevant to US primary care.
Methods
Scope of Review
Detailed methods are available in the full evidence report at https://www.uspreventiveservicestaskforce.org/Page/Document /final-evidence-review/genital-herpes-screening1.The full evi-dence report also provides additional information about the pro-posed methods for key question (KQ) 7 (focused on the association between subclinical genital HSV-2 viral shedding and health out-comes), additional background and contextual information about genital herpes in the United States, and a list of studies that were excluded during the full-text review phase of the literature search. Figure 1shows the analytic framework and KQs that guided the review.
Data Sources and Searches
PubMed/MEDLINE, the Cochrane Library, and EMBASE were searched for English-language articles published through March 31, 2016. Search strategies are listed in eMethods in the Supple-ment. We searched for unpublished literature in ClinicalTrials.gov and the World Health Organization’s International Clinical Trials
Registry Platform. To supplement electronic searches, reference lists of pertinent articles and suggested citations from reviewers were reviewed. We conducted ongoing surveillance after March 2016 through article alerts and targeted searches of high-impact journals to identify major studies published in the interim that may affect the conclusions or understanding of the evidence and related USPSTF recommendation. The last surveillance was con-ducted on October 31, 2016.
Study Selection
Two investigators independently reviewed titles, abstracts, and full-text articles to determine eligibility using prespecified criteria (eTable 1 in theSupplement). Disagreements were resolved by dis-cussion. English-language studies of immunocompetent adults or adolescents, including pregnant women, were included. Only stud-ies rated as good or fair quality were included. For all KQs, studstud-ies of persons without symptoms or a clinical history of genital herpes were eligible, as were studies of asymptomatic partners of persons with known genital herpes (ie, discordant couples). For the over-arching question on direct evidence that screening improves health outcomes (KQ1), only randomized clinical trials (RCTs) comparing groups that were screened with groups that were not screened were included.
For KQ2 (accuracy of serologic tests), we included studies of FDA-approved serologic tests for HSV-2 that reported accuracy com-pared with the Western blot, which has been used as a reference standard in studies assessing commercially available serologic tests in the United States. Eligible populations could be symptomatic, asymptomatic, or a combination of both.
For KQ3 (harms of screening), we included trials, systematic re-views, and observational studies assessing the harms of screening in asymptomatic populations with no prior diagnosis of genital her-pes, with or without a comparison group.
For studies assessing benefits or harms of preventive medica-tions in asymptomatic populamedica-tions (KQ4 through KQ6), RCTs comparing FDA-approved oral antiviral medications for the sup-pression of recurrent genital herpes (acyclovir, famciclovir, or valacyclovir) with placebo were eligible. RCTs of behavioral coun-seling interventions (eg, education or councoun-seling; partner notifi-cation; barrier protection; or combinations of these components) were also eligible. For studies assessing the harms of antiviral medications in pregnant women (KQ6b), multi-institution antivi-ral medication pregnancy exposure registries were eligible. Eli-gible outcomes included reduced rates of symptomatic episodes and transmission (including measures of HSV-2 seroconversion). For KQ5b (effectiveness of interventions in pregnant women), eli-gible outcomes also included rates of neonatal HSV infection and reduced rates of symptomatic genital herpes at delivery. For KQ4 (effects of antiviral medication on subclinical HSV-2 shedding), we included any outcome measure of subclinical HSV-2 shedding (eg, percentage of days with any shedding detected).
Data Extraction and Quality Assessment
the USPSTF and adapted for this topic (eTables 2-3 in the Supple-ment). Individual study quality ratings are provided in the Supplement(eTables 4-7).
Data Synthesis and Analysis
Findings for each question were summarized in tabular and narra-tive form. To determine whether meta-analyses were appropriate, the clinical and methodological heterogeneity of the studies was
assessed following established guidance.11
To do this, we qualita-tively assessed the similarities and differences in populations, tests, treatments, comparators, outcomes, and designs. For KQ2 (the only KQ with sufficient numbers of similar studies for quanti-tative syntheses), pooled sensitivities and specificities for each type of serologic test were calculated using a hierarchical sum-mary receiver operating characteristic (HSROC) curve analysis when at least 3 similar studies were available. Separate models Figure 1. Analytic Framework and Key Questions
Key questions
5 a. How effective are preventive medications and behavioral counseling interventions in reducing future symptomatic episodes and transmissions of genital herpes in asymptomatic nonpregnant adults and adolescents?
b. How effective are preventive medications and behavioral counseling interventions in reducing neonatal HSV infection and symptomatic episodes of genital herpes at delivery in pregnant women?
6 a. What are the harms of preventive medications and behavioral counseling interventions for reducing future symptomatic episodes and transmission of genital herpes in asymptomatic nonpregnant adults and adolescents?
b. What are the harms of preventive medications and behavioral counseling interventions for reducing neonatal HSV infection and symptomatic episodes of genital herpes at delivery in asymptomatic pregnant women?
1 a. Does serologic screening for herpes simplex virus type 2 (HSV-2) or combined testing for herpes simplex virus type 1 (HSV-1) and 2 in asymptomatic nonpregnant adults and adolescents reduce future symptomatic episodes and transmission of genital herpes?
b. Does serologic screening for HSV-2 or combined testing for HSV-1 and HSV-2 in pregnant women reduce neonatal HSV infection and symptomatic episodes of genital herpes at delivery?
3 a. What are the harms of serologic screening for HSV-2 or combined testing for HSV-1 and HSV-2 in asymptomatic nonpregnant adolescents and adults?
b. What are the harms of serologic screening for HSV-2 or combined testing for HSV-1 and HSV-2 in asymptomatic pregnant women? What is the accuracy of serologic screening for HSV-2 in asymptomatic adults, adolescents, and pregnant women?
2
What is the evidence supporting an association between subclinical HSV-2 viral shedding and health outcomes in asymptomatic adults, adolescents, and pregnant women who are seropostive for HSV-2?
7
How effective are oral antiviral medications in reducing genital HSV-2 viral shedding in asymptomatic adolescents, adults, and pregnant women? 4
Harms of screening
3
HSV serologic screening a
Preventive medications and behavioral counseling
Health outcomes
Genital herpes symptoms Transmission of genital herpes Neonatal HSV infection 1
5
Asymptomatic sexually active adults, adolescents, and pregnant women with no clinical history of genital herpes
2
Harms of interventions
6 4
HSV status Genital HSV-2
viral shedding 7
b
Evidence reviews for the US Preventive Services Task Force (USPSTF) use an analytic framework to visually display the key questions that the review will address to allow the USPSTF to evaluate the effectiveness and safety of a preventive service. The questions are depicted by linkages that relate interventions and outcomes. A dashed line indicates health outcomes that follow an intermediate outcome. HSV indicates herpes simplex virus. Further details are available from the USPSTF procedure manual.10
a
Studies that screen using an HSV-2 serologic test alone or a paired (HSV-1 and HSV-2) serologic test will be included if they meet other eligibility criteria; however, only the accuracy of test characteristics related to HSV-2 serologic tests will be evaluated.
bKey question 7 will be addressed only if there is insufficient literature for key
were developed for each type of serologic test, and separate analyses were conducted for HerpeSelect using the manufacturer-recommended cutpoint for test positivity and for higher cutpoints reported in the literature to determine whether accuracy is improved with using higher cutpoints. The metandi program in Stata version 1412
was used to conduct all quantitative analyses.
Results
Seventeen included studies with a total of 9736 participants (range, 24-3290) and reported in 19 publications were identified (Figure 2).13-29
Benefits of Screening
Key Question 1a.Does serologic screening for HSV-2 or combined testing for HSV-1 and HSV-2 in asymptomatic nonpregnant adults and adolescents reduce future symptomatic episodes and transmis-sion of genital herpes?
Key Question 1b.Does serologic screening for HSV-2 or combined testing for HSV-1 and HSV-2 in pregnant women reduce neonatal HSV infection and symptomatic episodes of genital herpes at delivery?
No eligible studies were identified.
Accuracy of HSV-2 Serologic Screening Tests
Key Question 2.What is the accuracy of serologic screening for HSV-2 in asymptomatic adults, adolescents, and pregnant women?
We included 11 good- or fair-quality studies (n = 7129; range, 61-3290) assessing the accuracy of 1 or more type-specific HSV-2 serologic tests compared with Western blot.13-23
All 11 studies enrolled adults and none enrolled pregnant women. Most studies (8) enrolled a population with HSV-2 prevalence greater than 40% based on Western blot (range, 41%-70%). Two included studies described whether participants had current or prior symp-toms consistent with genital herpes17,30
; 1 study enrolled US col-lege students with no current or previous symptoms consistent with genital herpes,30
and the other enrolled men seeking care at US STI clinics (17% were later diagnosed with genital herpes).17
In the 9 other studies, the proportion of participants who had cur-rent or past symptoms of genital herpes was not described. Most studies enrolled participants from 1 or more African countries; 3 were set in the United States,13,17,18
and 1 enrolled participants from multiple countries (Argentina, Costa Rica, Korea, Mexico, Nigeria, Thailand, and Vietnam).14
All 11 studies compared the Focus HerpeSelect HSV-2 enzyme-linked immunosorbent assay with Western blot and used a test cut-point value of 1.1 to define a positive test result (current manufac-turer’s cutpoint). Seven studies also assessed higher test cutpoints to boost specificity (ranging from 2.1 to 3.5).14-16,19,21-23
Four stud-ies also assessed accuracy of the biokit HSV-2 Rapid Test.18,20-22 Fur-ther study characteristics are shown inTable 1.
Ten studies (n = 6537 participants analyzed; range, 89-3290) provided sufficient data to estimate sensitivity and specificity of HerpeSelect using a cutpoint value of 1.113-16,18-23
; individual study Figure 2. Summary of Evidence Search and Selection
270Excluded
63Ineligible population
36Ineligible comparator
31Ineligible intervention
21Ineligible study design
18Ineligible screening test
10Poor quality study
4Non–English-language
50Ineligible outcome
37Not original research
3001Excluded after review of titles and abstracts
11Studies included for KQ2 (10 studies for quantitative analysis)
1Study included for KQ6
4Studies included for KQ5
2Studies included for KQ4
2Studies included for KQ3
0Studies included for KQ1
289Full-text articles assessed for eligibility
3290Records screened
3213Records identified through database searching (after duplicates removed)
77Records identified through other sources
17Fair- or good-quality studies (from 19 articles) included
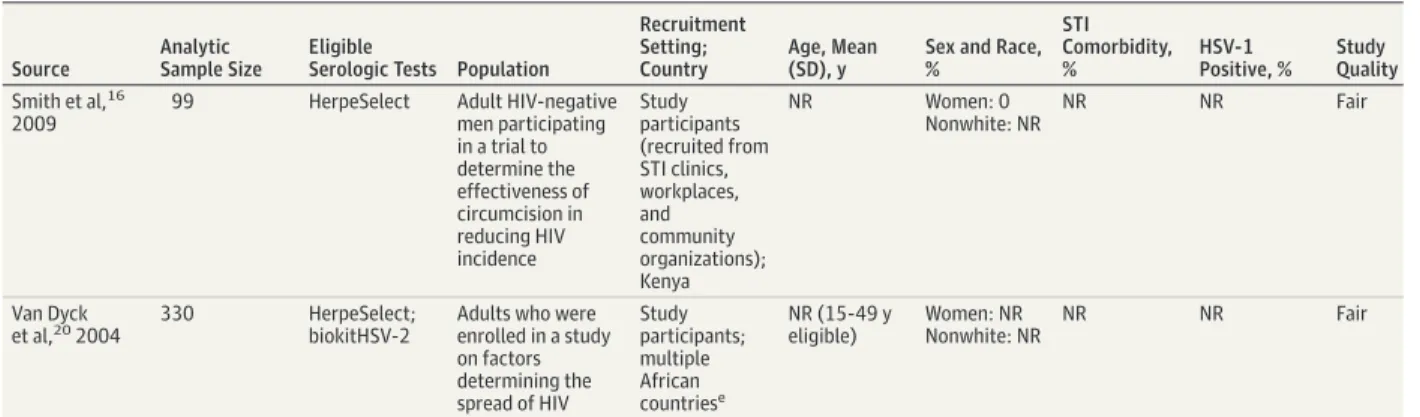
Table 1. Characteristics of Included Studies Assessing the Accuracy of Serologic Screening Tests for HSV-2 (Key Question 2)
Source
Analytic Sample Size
Eligible
Serologic Tests Population
Recruitment Setting; Country
Age, Mean (SD), y
Sex and Race, %
STI Comorbidity, %
HSV-1 Positive, %
Study Quality
Ashley-Morrow et al,142004
675 HerpeSelect Women aged ≥15 y participating in an HSV seroprevalence study
Study participants; multinationala
NR Women: 100
Nonwhite: NR
NR 93-99 (by
WB)
Fair
Delany-Moretlwe et al,232010
98 HerpeSelect Adult women with unknown HSV-2 serostatus
Family planning clinics; South Africa
26 (range, 18-46)
Women: 100 Nonwhite: NR
52 (HIV-1) NR Fair
Golden et al,17 2005
61 HerpeSelect Men who had been tested for HSV at an STI clinic between 2001-2002
2 county STI clinics; United States
Median, 35 (range, 18-73)
Women: 0 Nonwhite: 23
1 56 (by WB) Fair
Hogrefe
et al,192002 776 HerpeSelect Adults, varied bylocation; Kenya: women enrolled in a vitamin A study; Uganda: (1) serologic samples from participants in an HIV seroprevalence study, (2) samples from HIV-negative women South Africa and Namibia: samples initially collected for HIV screenings from healthy, primarily middle-income individuals
Varied by location— primarily study participants; multiple African countriesb
NR Women: NR
Nonwhite: NR
NR 89-100 (by
WB)
Fair
Lingappa et al,212010
467 HerpeSelect; biokit HSV-2
Adults participating in a study of genital herpes
seroprevalence and incidence
Study participants; Uganda
NR Women: NR
Nonwhite: NR
12 (HIV-1) NR Good
Mark et al,13 2007; Mark et al,302008
89 HerpeSelect Urban university students with no history of genital herpes or genital sores who reported being sexually active within the past 6 mo
Recruited by flyers, announce-ments, and online/ newspaper advertisements at 1 university; United States
25 (4.4) Women: 64 Nonwhite: 31
NR 9 (by
HerpeSelect); 3 (by WB)
Good
Morrow et al,18 2005
782 HerpeSelect; biokit HSV-2
Two populations enrolled: (1) adult MSM screened for enrollment in a clinical trial assessing acyclovir to reduce HIV transmission and (2) consecutive serologic samples submitted for HSV WB testing
Study participants and serologic samples sent to the University of Washington Virology Laboratory during a 4-wk period; United States
NR Women: 0
Nonwhite: NR
NR 64 (by WB) Fair
Mujugira et al,152011
3290 HerpeSelect HIV-negative adult men and women participating in the Partners in Prevention HSV/HIV Transmission Studyc
Study participants; multiple African Countriesd
Median, 34 Women: 33 Nonwhite: NR
NR NR Good
Ng’ayo et al,22 2010
233 HerpeSelect; biokit HSV-2
Adult men who worked in the fishing industry who reported being sexually active in the previous 2 wk
Community (beaches along Lake Victoria); Kenya
NR (≥18 y eligible)
Women: 0 Nonwhite: NR
NR NR Fair
results are shown in eTable 8 in theSupplement. Pooled estimates of sensitivity and specificity were 99% (95% CI, 97%-100%) and 81% (95% CI, 68%-90%), respectively (Table 2). eFigure 1 in the Supplementshows the HSROC with 95% confidence ellipse using pairs of sensitivity and specificity. Estimates for specificity were highly variable, ranging from 41% to 97.5%. Studies handled equivocal (or indeterminate) test results in various ways, which may contribute to heterogeneity in estimates of test accuracy (eTable 8 in theSupplement). Five studies (n = 1840; range, 61-776) reported a positive predictive value using the manufactur-er’s cutpoint; estimates ranged from 37.5 to 86.0.13,14,17,18,22
Four studies (n = 1779; range, 89-776) reported negative predictive val-ues; estimates ranged from 96.5 to 100.13,14,18,22
Seven studies (n = 5516 participants analyzed; range, 99-3290) assessed higher cutpoints for a positive test result than those recommended by the manufacturer (ranging from 2.2 to 3.5) (eTable 8 in theSupplement).14-16,19,21-23
Estimates of specificity were gen-erally higher at cutpoints greater than 2.2. The pooled estimates of sensitivity and specificity were 95% (95% CI, 91%-97%) and 89% (95% CI, 82%-93%), respectively (Table 2). eFigure 2 in the Supplementshows the HSROC with 95% confidence ellipse using pairs of sensitivity and specificity.
Four studies (n = 1512 participants analyzed; range, 98-782) re-ported on the sensitivity and specificity of the biokit HSV-2 Rapid Test (eTable 9 in theSupplement).18,20-22
The pooled estimates of
sensitivity and specificity were 84% (95% CI, 73%-91%) and 95% (95% CI, 93%-97%), respectively (Table 2). eFigure 3 in the Supplementshows the HSROC with 95% confidence ellipse using pairs of sensitivity and specificity.
Harms of HSV-2 Serologic Screening in Asymptomatic Populations
Key Question 3a.What are the harms of serologic screening for HSV-2 or combined testing for HSV-1 and HSV-2 in asymptomatic nonpreg-nant adolescents and adults?
Key Question 3b.What are the harms of serologic screening for HSV-2 or combined testing for HSV-1 and HSV-2 in asymptomatic pregnant women?
Characteristics and outcomes of the 2 included fair-quality stud-ies are shown in eTable 10 in theSupplement.24,25
Both studies were set in the United States and assessed the effect of a positive HSV-2 serologic test result on psychosocial outcomes among people who reported no history of genital herpes.
The first study (n = 24) was a qualitative assessment of the psychosocial effects of receiving an HSV-2 diagnosis based on serologic testing.24
Investigators recruited 24 adult participants reporting no history of genital herpes who tested HSV-2 seroposi-tive by Western blot. Participants were recruited from clinical set-tings (STI, maternal and infant care, family medicine, and research clinics) and completed in-depth interviews on their experience of Table 2. Accuracy of Serologic Screening Tests for HSV-2 Compared With Western Blot (Key Question 2)a
HerpeSelect
biokit HSV-2 1.1 Cutpoint 2.2-3.5 Cutpoint
Studies, No. 10 7 4
Participants, No. 6537 5516 1512
Sensitivity (95% CI), % 99 (97-100) 95 (91-97) 84 (73-91)
Specificity (95% CI), % 81 (68-90) 89 (82-93) 95 (93-97)
Likelihood ratio (95% CI)
Positive 5 (3-10) 8 (5-13) 17 (11-29)
Negative 0.01 (0.003-0.04) 0.06 (0.036-0.099) 0.16 (0.92-0.30)
Abbreviation: HSV-2, herpes simplex virus type 2.
a
Values summarize the pooled estimates of sensitivity and specificity based on hierarchical summary receiver operating characteristic curve and bivariate analyses.
Table 1. Characteristics of Included Studies Assessing the Accuracy of Serologic Screening Tests for HSV-2 (Key Question 2) (continued)
Source
Analytic Sample Size
Eligible
Serologic Tests Population
Recruitment Setting; Country
Age, Mean (SD), y
Sex and Race, %
STI Comorbidity, %
HSV-1 Positive, %
Study Quality
Smith et al,16 2009
99 HerpeSelect Adult HIV-negative men participating in a trial to determine the effectiveness of circumcision in reducing HIV incidence
Study participants (recruited from STI clinics, workplaces, and community organizations); Kenya
NR Women: 0
Nonwhite: NR
NR NR Fair
Van Dyck
et al,202004 330 HerpeSelect;biokitHSV-2 Adults who wereenrolled in a study on factors determining the spread of HIV
Study participants; multiple African countriese
NR (15-49 y eligible)
Women: NR Nonwhite: NR
NR NR Fair
Abbreviations: HIV, human immunodeficiency virus; HSV, herpes simplex virus; MSM, men who have sex with men; NR, not reported; STI, sexually transmitted infection; WB, Western blot.
a
Argentina, Costa Rica, Korea, Mexico, Nigeria, Thailand, Vietnam.
bKenya, Uganda, South Africa, Namibia.
c
Randomized trial of acyclovir (for HSV-2 suppressive therapy) to reduce HIV-1 transmission.
dKenya, Rwanda, Tanzania, Uganda, Botswana, South Africa, Zambia. e
HSV-2 diagnosis. The qualitative analysis identified 3 categories of themes: (1) short-term, emotional responses that included surprise, denial, confusion, distress, sadness, disappointment, and relief to know; (2) short-term, psychological responses that included fear of telling sex partners, anger at the source partner, guilt about acquir-ing or transmittacquir-ing, and concern about transmittacquir-ing to a child; and (3) perceived ongoing responses that included fear of telling future partners, concern about transmitting to a sex partner, feeling sexu-ally undesirable, feeling socisexu-ally stigmatized, feeling like “damaged goods,” sex avoidance because of social responsibility, fear of trans-mitting to a newborn child, and relationship concerns relating to the diagnosis. The authors concluded that participants exhibited strong emotional and psychological responses to their serologic diagnoses of HSV-2, while observing that some of these responses were time limited.24
The second study (n = 33) enrolled individuals aged 14 to 30 years from an urban university setting and various clinical settings, including STI, primary care, and adolescent clinics.25
Of the 1190 en-rolled, 820 (68%) had serologic testing (type of test not de-scribed) and 149 (18%) were HSV-2–positive. Of those participants who screened positive for HSV-2, 93 (62%) returned for their initial test results and 33 returned for the 3-month follow-up. At 3 months, participants completed the herpes Health-Related Quality of Life Questionnaire (HRQOLQ).31
Participants responded to each item using a 4-point scale that ranged from “very” to “not at all.” For in-dividual-item analysis, answers of “very” or “quite” were consid-ered indicative of endorsing the experience.25
A number of indi-vidual HRQOLQ items were endorsed frequently as “very” or “quite,” including the following: “It is difficult to forget that I have herpes” (63%); “I worry about giving herpes to someone” (56%); and “I worry about people finding out I have herpes” (48%).25
Other items from the HRQOLQ endorsed less frequently are shown in eTable 10 in the Supplement.
Effectiveness of Preventive Interventions
for Asymptomatic HSV-2–Seropositive Populations
Key Question 4.How effective are oral antiviral medications in re-ducing genital HSV-2 viral shedding in asymptomatic adolescents, adults, and pregnant women?
We included 2 fair-quality RCTs (n = 129; range, 63-66) that com-pared daily preventive antiviral medication with placebo over 6 to 8 weeks (Table 3).26,27
One study did not describe how symptoms of genital herpes were ascertained27
; the other reported that par-ticipants had undergone HSV serologic testing as part of their clini-cal care but reported no current or prior symptoms consistent with genital herpes.26
One RCT (n = 63) assessed valacyclovir (1 g daily)26 and the other (n = 66) assessed famciclovir (250 mg twice daily).27 In both studies, participants were educated on performing self-administered swabs of the anogenital area, which they completed once daily during the treatment period. Study characteristics are shown in Table 3.
One RCT reported a statistically significant reduction in viral shedding outcomes, and the other did not (Table 3). In the RCT assessing valacyclovir (n = 63), valacyclovir treatment significantly reduced subclinical days with HSV-2 shedding compared with pla-cebo (1.5% vs 5.1%,P< .001) and also resulted in a greater propor-tion of participants experiencing no days with shedding (84% vs 54%,P= .001; between-group difference, 30% [95% CI,
15%-46%]).26
In the RCT comparing famciclovir (250 mg twice daily) with placebo (n = 66), participants in both groups did not have a significantly different risk of subclinical viral shedding; poly-merase chain reaction samples were positive on 5.0% and 5.7% of subclinical days, respectively (relative risk [RR], 0.8 [95% CI, 0.41-1.56];P= .52).27
Quality limitations across both trials included attrition (23%-29% of participants) and unclear handling of missing data. In addi-tion, the validity and reliability of daily self-swab to ascertain viral shedding is unclear, potentially contributing to measurement bias. Key Question 5a.How effective are preventive medications and be-havioral counseling interventions in reducing future symptomatic episodes and transmission of genital herpes in asymptomatic non-pregnant adults and adolescents?
Key Question 5b.How effective are preventive medications and be-havioral counseling interventions in reducing neonatal HSV infec-tion and symptomatic episodes of genital herpes at delivery in preg-nant women?
We included 4 fair-quality RCTs (n = 2550; range, 63-1484) evaluating antiviral medications (Table 3).26-29
Two focused on pre-venting transmission and enrolled adult heterosexual couples who were serologically discordant for HSV-2 infection (ie, one partner had known genital herpes and the other partner had no prior diagnosis and was also HSV-2 seronegative),28,29
and 2 enrolled asymptom-atic adults with no history of genital herpes who were seropositive for HSV-2 infection.26,27
Two RCTs comparing daily suppressive antiviral medication with placebo also reported viral shedding outcomes and were de-scribed in KQ4. Both reported on incidence of genital herpes symp-toms (Table 3). In the RCT assessing valacyclovir (n = 63), partici-pants were educated on signs and symptoms of genital herpes and instructed to return to the clinic any time they suspected an out-break. At 2 months, fewer participants in the valacyclovir group re-ported symptoms of genital herpes than in the placebo group (12% vs 23%, respectively). The authors report that the treatment effect was significant (P= .033, controlling for the crossover effect); how-ever, the arithmetic mean of the difference between groups was not significant (11% [95% CI, −0.6% to 22%]).26
In the RCT assessing fam-ciclovir (n = 66), the incidence of genital herpes symptoms was simi-lar in the famciclovir and placebo groups at 6 weeks (17.5% and 17.2%, respectively;Pvalue not reported).27
Quality limitations across both trials included attrition (23%-29% of participants), unclear handling of missing data, and risk of measurement bias. Symptoms were ascertained by self-report (not using a validated questionnaire) over a relatively short dura-tion (6-8 weeks). One study enrolled participants who had HSV serologic testing as part of their clinical care26
; results may not be applicable to those who screen positive but are not seeking test-ing for HSV infection.
Two RCTs compared the benefit of daily suppressive antiviral medication with placebo for preventing genital herpes transmis-sion between HSV-2–serodiscordant heterosexual couples; one mea-sured outcomes at 8 months28,29
and the other at 12 to 24 months (Table 3).32
One RCT enrolled immunocompetent couples,28,29 while the other was a substudy of HIV-1–serodiscordant couples in which the HIV-1–negative partner was also susceptible to HSV-2.32
One RCT (n = 1484 couples) assessed valacyclovir (500 mg daily),28,29
T able 3 .Char ac teris tic s and R e sults of R andomiz ed Clinical T rials Asse ssin g Antivir al Medications in A dults (K e y Que stions 4 and 5 ) a Source Population R ecruitment Setting; Countr y Group Information T reatment Dur ation, wk HSV -2 T est Age, Mean (SD), y S e x and Race, % HSV -1 Positiv e, % Vir al Shedding Outcome Measure, R esults S
ymptomatic Episodes
Outcome Measure R esults HSV -2 T ransmission Outcome Measure R esults Leone et al , 27 2007 Adults ≥18 y seropositiv e for HSV -2 with no histor y o f symptomatic genital herpes 7 centers (not other wise specified); United States T otal (66) Group 1: famciclo vir (250 mg twice daily) first (NR) Group 2: placebo first (NR) 6 W estern blot Median, 38 (r ange, 18-68) W o men: 64 Nonwhite: 35 55 Par ticipants with any shedding, No . (%), Group 1 : 27 (42.9) Group 2 : 29 (50.0) P =N R Days with any subclinical vir a l shedding, mean (%), Group 1 : 114/2277 (5.0) Group 2 : 122/2141 (5.7) P < .52 R eduction in subclinical shedding risk, group 1 vs group 2: RR, 0.80 (95% C I, 0.41-1.56) Par ticipants repor ting genital lesions, No . (%), Group 1: 11 (17.5) Group 2: 10 (17.2) P =N R NR Sperling et al , 26 2008 Adults ≥18 y seropositiv e for HSV -2 with no activ e lesions or symptoms consistent with genital herpes and no histor y o f recurrent or
undiagnosed symptoms consistent
with genital herpes 13 clinical settings (STI clinics, primar y care clinics, and
gynecology practices); United
T able 3 .Char ac teris tic s and R e sults of R andomiz ed Clinical T rials Asse ssin g Antivir al Medications in A dults (K e y Que stions 4 and 5 ) a(continued) Source Population R ecruitment Setting; Countr y Group Information T reatment Dur ation, wk HSV -2 T est Age, Mean (SD), y S e x and Race, % HSV -1 Positiv e, % Vir al Shedding Outcome Measure, R esults S
ymptomatic Episodes
Outcome Measure R esults HSV -2 T ransmission Outcome Measure R esults Corey et al , 28 2004 Kim et al , 29 2008 Adult (≥18 y) HSV -2 serodiscordant heterose xual couples 96 study sites (not other wise specified); United States, Canada, E urope, Latin America, Austr alia T otal (1484 couples) Group 1: v alacy clo vir (500 mg once daily) (743 couples) Group 2: placebo (741 couples) 32 W estern blot Median, 34-34 (r ange, 18-76) W o men: 33 Nonwhite: 10-11 70 NR NR HSV -2 seroconv ersions, No . (%), Group 1: 14 (1.9) Group 2: 27 (3.6) HR, 0.52 (95% CI,
0.27-0.99) P=
.04 Incidence of symptomatic genital herpes, No . (%), Group 1: 4 (0.5) Group 2, 16 (2.2) HR, 0.25 (95% CI,
0.08-0.75) P=
.008 Mujugir a et al , 32 2013 HSV -2 serodiscordant heterose xual couples enrolled into the Par tners in Pre v ention HSV /HIV T ransmission study 33 ; couples w ere also serodiscordant for HIV (HSV -2–infected par tners w ere also infected with HIV ) 14 study sites (not specified); K eny a, R w anda, T anzania, Uganda, B otsw ana, South Africa, Zambia T otal (937 couples) Group 1: acy clo vir (400 mg twice daily) (458 couples) Group 2: placebo (453 couples) 78 HerpeSelect f Median, 31 (IQR, 27-38) W o men: 12 Nonwhite: NR ≥99 N R N R HSV -2 seroconv ersions, No ., Group 1: 40 Group 2: 28 HSV -2 incidence, HR, 1.35 (95% CI,
0.83-2.20) P=
both studies, antiviral medication was provided to the infected partner.32
Both studies were conducted in multiple countries; one enrolled from 96 study sites in the United States, Canada, Europe, Latin America, and Australia,28,29
and one was conducted in 7 sub-Saharan African countries.32
The 2 trials found conflicting results (Table 3). In the RCT assessing valacyclovir, fewer HSV-2–susceptible partners in the valacyclovir group had symptomatic HSV-2 infection than partners randomized to placebo over 8 months (0.5% vs 2.2%, respec-tively; hazard ratio, 0.25 [95% CI, 0.08-0.75]); similarly, fewer HSV-2–suceptible partners in the valacyclovir group seroconverted to HSV-2 than those in the placebo group (1.9% vs 3.6%, respec-tively;P= .04; hazard ratio, 0.52 [95% CI, 0.27-0.99]).28,29 In contrast, the RCT assessing acyclovir use among HIV-1– serodiscordant couples did not find a reduction in transmission. At follow-up (median, 18 months), the number of susceptible part-ners with seroconversions was not statistically different between the acyclovir group (40) and placebo group (28), which indicated seroincidence of 5.9 and 4.3 cases per 100 person-years, respec-tively (hazard ratio, 1.35 [95% CI, 0.83-2.20];P= .22).32
Key limitations across both trials included high attrition; 22% of couples withdrew from one trial,28,29
and the overall attrition was 66% in the other trial.32
Harms of Preventive Interventions
for Asymptomatic HSV-2–Seropositive Populations
Key Question 6a.What are the harms of preventive medications and behavioral counseling interventions for reducing future sympto-matic episodes and transmission of genital herpes in asymptom-atic nonpregnant adults and adolescents?
Key Question 6b.What are the harms of preventive medications and behavioral counseling interventions for reducing neonatal HSV in-fection and symptomatic episodes of genital herpes at delivery in asymptomatic pregnant women?
One RCT (n = 63) included in KQ4 and KQ5 reported on harms.26 Rates of reported adverse events were similar among groups ran-domized to valacyclovir and placebo, including dizziness, head-ache, and nausea (eTable 11 in theSupplement).26
Discussion
This review did not identify any eligible studies directly assessing the benefits or harms of serologic screening for HSV-2 compared with no screening. Therefore, the literature that might establish an indi-rect chain of evidence from multiple questions that link screening to health outcomes (KQ2 through KQ7) was reviewed.
Table 4provides a summary of findings in this evidence review. Estimates for specificity varied and were imprecise, with-out a clear explanation for the observed heterogeneity. Potential explanations for false-positive serologic test results include cross-reactivity with HSV-1 (or other viruses), recent seroconversion, geographic variability in HSV-2 strain variants, and laboratory error. At higher cutpoints, estimates of sensitivity and specificity from 8 studies in Africa were still imprecise. There was evidence from 2 uncontrolled observational studies that detection of unex-pected HSV-2 by screening is associated with potential psychoso-cial harms, including anxiety, worry, and distress. Other potential
harms of serologic screening include false-positive results that lead to psychosocial distress and costs of confirmatory testing.
The estimates of the accuracy of serologic tests are generally applicable to populations with a higher prevalence of HSV-2 infec-tion than general primary care populainfec-tions in the United States. The majority of studies assessing the accuracy of HerpeSelect enrolled a population with HSV-2 prevalence greater than 40% based on Western blot. Use of HerpeSelect in a population with lower prevalence, similar to that of US adults, would greatly increase the number of false-positive test results. For example, in a hypothetical population of 100 000 persons with a prevalence of asymptomatic HSV-2 of 50% (similar to the prevalence in included studies), with test sensitivity of 99% and specificity of 81%, there would be an estimated 49 500 true-positive results and 9500 false-positive results (positive predictive value, 84%). If the preva-lence instead were 16% (similar to the seroprevapreva-lence in the gen-eral US adult population among people with unknown symptom status), the number of true-positive results would be estimated at 15 840, and the number of false-positive results would be esti-mated at 15 960 (positive predictive value, 50%). True-positive results would decrease further, and false-positive results would increase further if the prevalence were less than 16%.
If sensitivity were unchanged, screening a lower-prevalence population would reduce the number of false-negative test results, although the negative predictive value would change little. It is pos-sible, however, that the sensitivity of the screening tests could be lower in a lower-prevalence population, owing to such factors as lower antibody levels, thus increasing the number of false-negative results per 1000 persons tested. The direction of these changes with prevalence would be similar regardless of which cut-points were used.
There was limited evidence evaluating preventive interven-tions for asymptomatic adults who screen positive for HSV-2. No studies enrolled pregnant women or adolescents, and none assessed behavioral counseling interventions. Two RCTs (total of 129 participants) assessed the benefit of preventive antiviral medi-cations for reducing HSV-2 viral shedding and symptomatic occur-rences among adults seropositive for HSV-2 who reported no prior genital herpes symptoms. Evidence from these 2 trials does not allow an accurate estimate of the benefit of preventive antiviral medications for improving health outcomes. The 2 trials differed in several ways. They assessed different medications (valacyclovir and acyclovir), recruited from different sources, and used different tests to establish HSV-2 infection. Both assessed outcomes over a short time (6-8 weeks) and relied on self-report to ascertain symp-tom occurrence. This duration is likely inadequate to evaluate whether antiviral medications reduce symptom incidence among populations who have been asymptomatic. Results were inconsis-tent and imprecise; 1 trial found benefit for valacyclovir compared with placebo for reducing viral shedding and symptom oc-currences,26
and the other found no statistically significant differ-ences between groups.27
Similarly, the 2 RCTs assessing preventive antiviral medica-tions for reducing HSV-2 transmission between serodiscordant part-ners were heterogeneous and found inconsistent results. One en-rolled immunocompetent couples from primarily industrialized countries,28
Table 4. Summary of Evidence: Serologic Screening for Genital Herpesa
Key Question Topic
No. of Studies
No. of
Participants Study Design
Summary of Findings (Including
Consistency and Precision) Applicability
Limitations (Including Reporting Bias)
Key question 1: Benefits of screening
0 NA NA No studies were identified that directly evaluated the benefits of screening compared with no screening.
NA NA
Key question 2: Accuracy of serologic screening tests
11 Total: 7129; pooled analyses: 6537 (HerpeSelect, 1.1 cutpoint); 5516 (HerpeSelect, 2.2-3.5 cutpoint); 1512 (biokit HSV-2)
Cross-sectional Pooled sensitivity for detecting HSV-2 with HerpeSelect (1.1 cutpoint) was 99% (95% CI, 97%-100%) and slightly lower (95%) at higher cutpoints. Pooled sensitivity of biokit HSV-2 was 84% (95% CI, 73%-91%). Pooled specificity for detecting HSV-2 with HerpeSelect (at manufacturer’s cutpoint) was 81% (95% CI, 68%-90%) and slightly higher (89%) at higher cutpoints. Pooled specificity of biokit HSV-2 was 95% (95% CI, 93%-97%).
Overall, findings were consistent but imprecise.
Populations from African countries that have a high prevalence of HSV-2 infection (>50%)
Evidence identified for only 2 FDA-approved HSV-2 serologic tests; most studies excluded equivocal test results from calculations of test accuracy (or did not describe the handling of missing data).
Key question 3: Harms of screening
2 57 Qualitative
study; cohort study
The qualitative study found that participants with a new HSV-2 diagnosis had short-term emotional responses (eg, distress, sadness), short-term
psychological responses (eg, fear of telling sex partners), and perceived ongoing responses (eg, feeling sexually undesirable). The cohort study found that individual items frequently reported as interfering in daily life on the herpes HRQOLQ included “It is difficult to forget I have herpes” (63%); “I worry about giving herpes to someone” (56%); “I worry about people finding out I have herpes” (48%); and others. Findings were consistent but imprecise.
Asymptomatic persons with no known history of genital herpes
Studies are uncontrolled; due to study design and outcome measures, estimating magnitude of effect or assessing precision is not possible.
Key question 4: Benefits of treatment: shedding
2 129 Crossover RCTs The valacyclovir trial found that those taking valacyclovir (1 g daily) had fewer subclinical days with any genital HSV-2 viral shedding detected over 6-8 wk than those taking placebo (1.5% vs 5.1%, respectively,P< .001). The famciclovir trial found that those taking famciclovir (250 mg twice daily) had fewer subclinical days with any genital HSV-2 viral shedding detected over 6-8 wk than placebo (5.7% vs 5.0%, respectively; RR, 0.8 [95% CI, 0.41-1.56];P= .52). Findings were inconsistent and imprecise.
Asymptomatic adults with HSV-2 infection diagnosed (or confirmed) by Western blot
Studies assessed different medications over a short duration; sample sizes were small, and overall attrition was >20% in both trials.
Key question 5: Benefits of treatment for asymptomatic adults
2 129 Crossover RCTs The valacyclovir trial found that those taking valacyclovir (1 g daily) had lower incidence of self-reported genital herpes symptoms at 6-8 wk than placebo (12% vs 23%, respectively;P= .033). The famciclovir trial found that those taking famciclovir (250 mg twice daily) had lower incidence of self-reported genital herpes symptoms at 6-8 wk than those taking placebo (17.5% vs 17.2%, respectively;P
value NR). Findings were inconsistent and imprecise.
Asymptomatic adults with HSV-2 infection diagnosed (or confirmed) by Western blot
Incidence was self-reported; outcomes were measured over a relatively short duration; sample sizes were small, and overall attrition was >20% in both trials.
Key question 5: Benefits of treatment for serodiscordant couples
2 2421 RCTs The valacyclovir trial found that participants whose partners took valacyclovir (1 g daily) had lower incidence of HSV-2 seroconversion at 32 wk than those whose partners took placebo (HR, 0.52 [95% CI, 0.27-0.99];P= .04). The acyclovir trial found that participants whose partners took acyclovir had no difference in incidence of HSV-2 seroconversion at 78 wk compared with those whose partners took placebo (HR, 1.35 [95% CI, 0.83-2.20];P= .220). Findings were inconsistent and imprecise.
Asymptomatic adults with known, ongoing exposure to genital herpes from a partner
Studies assessed different medications over different durations in populations that were heterogeneous.
Key question 6: Harms of treatment
1 62 RCT Incidence of self-reported adverse events were similar between groups (headache, nausea). Findings were imprecise; consistency NA.
Generally healthy asymptomatic nonpregnant adults
Unclear if adverse events were prespecified.
Abbreviations: FDA, US Food and Drug Administration; HR, hazard ratio; HRQOLQ, Health-Related Quality of Life Questionnaire; HSV, herpes simplex virus; NA, not applicable; NR, not reported; RCT, randomized clinical trial; RR, relative risk.
a
The trials assessed different medications (valacylovir and acyclo-vir) and over different durations (8 months and a median of 18 months). One trial found benefit for valacyclovir compared with pla-cebo for reducing symptomatic HSV-2 infection and HSV-2 serocon-version in the susceptible partner; however, the magnitude of ben-efit for symptom reduction was modest, and results were imprecise (0.5% vs 2.2%, respectively; hazard ratio, 0.25 [95% CI, 0.08-0.75]).
One trial assessed harms of medications; adverse events were similar between groups randomized to valacyclovir and placebo.26 Other review studies have concluded that there are few harms in nonpregnant adults.34
This review had limitations. Studies were required to com-pare an FDA-approved currently available serologic screening test with Western blot. We did not evaluate other comparisons, such as a serologic test compared with a viral polymerase chain reac-tion swab or culture or with another commercially available sero-logic test, to determine concordance. We limited the assessment to studies enrolling people with no current or prior symptoms and found only 2 trials. For people with frequent symptomatic recur-rences of genital herpes (more than 4 episodes per year), antiviral medications have been shown to reduce the frequency of
recur-rences; however, the magnitude of effect is uncertain, and the quality of evidence is low. A Cochrane review published in 2014 evaluated the efficacy of antiviral medications (acyclovir, famci-clovir, and valacyclovir) to suppress genital herpes outbreaks in nonpregnant adults34
; 22 trials were included, and the risk of bias was considered high for half of the studies and unclear for the other half. The authors concluded that there was low-quality evi-dence that the risk of having at least 1 clinical recurrence was reduced with acyclovir (9 parallel-group trials, n = 2049; RR, 0.48 [95% CI, 0.39-0.58]), valacyclovir (4 trials, n = 1788; RR, 0.41 [95% CI, 0.24-0.69]), or famciclovir (2 trials, n = 732; pooled RR, 0.57 [95% CI, 0.50-0.64]).34
It is unclear whether these results would apply to people who have less frequent recurrences (or who are asymptomatic).
Conclusions
Serologic screening for genital herpes is associated with a high rate of false-positive test results and potential psychosocial harms. Evi-dence from RCTs does not establish whether preventive antiviral medication for asymptomatic HSV-2 infection has benefit.
ARTICLE INFORMATION
Author Contributions:Dr Feltner had full access to
all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Concept and design:Feltner, Grodensky, Ebel, Ashok, Jonas.
Acquisition, analysis, or interpretation of data: Feltner, Grodensky, Ebel, Middleton, Harris, Ashok, Jonas.
Drafting of the manuscript:Feltner, Grodensky, Ebel, Middleton, Ashok, Jonas.
Critical revision of the manuscript for important intellectual content:Feltner, Grodensky, Ebel, Harris, Ashok, Jonas.
Statistical analysis:Feltner. Obtained funding:Feltner, Jonas.
Administrative, technical, or material support: Grodensky, Ebel, Middleton, Jonas. Supervision:Feltner, Jonas.
Conflict of Interest Disclosures:All authors have
completed and submitted ICMJE Form for Disclosure of Potential Conflicts of Interest and none were reported.
Funding/Support:This research was funded
under contract HHSA-290-2012-00015-I, Task Order No. 6, from the Agency for Healthcare Research and Quality (AHRQ), US Department of Health and Human Services, under a contract to support the USPSTF.
Role of the Funder/Sponsor:Investigators worked
with USPSTF members and AHRQ staff to develop the scope, analytic framework, and key questions for this review. AHRQ had no role in study selection, quality assessment, or synthesis. AHRQ staff provided project oversight; reviewed the report to ensure that the analysis met methodological standards, and distributed the draft for peer review. Otherwise, AHRQ had no role in the conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript findings. The
opinions expressed in this document are those of the authors and do not reflect the official position of AHRQ or the US Department of Health and Human Services.
Additional Contributions:We gratefully acknowledge the following individuals for their contributions to this project: David Meyers, MD (AHRQ), Evelyn Whitlock, MD, MPH (Kaiser Permanente Research Affiliates EPC), and Meera Viswanathan, PhD; Carol Woodell, BSPH; Rachel Weber, PhD; Christiane Voisin, MSLS; Sharon Barrell, MA; and Loraine Monroe (RTI International–University of North Carolina EPC).
Additional Information:A draft version of the full evidence report underwent external peer review from 4 content experts (Rhoda A. Morrow, PhD, University of Washington, Seattle; David Kimberlin, MD, University of Alabama at Birmingham; Jeffrey Peipert, MD, MPH, MHA, Washington University, St Louis, MO; and 1 anonymous content expert) and 4 partner reviewers from the Eunice Kennedy Shriver National Institute of Child Health and Human Development; National Institute of Allergy and Infectious Diseases; National Center for HIV, Hepatitis, STD, and TB Prevention (Centers for Disease Control and Prevention); and Office of the Surgeon General, G-3/5/7, Health and Wellness. Comments from reviewers were presented to the USPSTF during its deliberation of the evidence and were considered in preparing the final evidence review.
Editorial Disclaimer:This evidence report is presented as a document in support of the accompanying USPSTF Recommendation Statement. It did not undergo additional peer review after submission toJAMA.
REFERENCES
1. Patel R, Rompalo A. Genital herpes infections. In: Zenilman JM, Shahmanesh M, eds.Sexually Transmitted Infections: Diagnosis, Management,
and Treatment. Sudbury, MA: Jones & Bartlett Learning; 2009:165-176.
2. Wald A, Zeh J, Selke S, et al. Reactivation of genital herpes simplex virus type 2 infection in asymptomatic seropositive persons.N Engl J Med. 2000;342(12):844-850.
3. Sacks SL. Famciclovir suppression of asymptomatic and symptomatic recurrent anogenital herpes simplex virus shedding in women: a randomized, double-blind,
double-dummy, placebo-controlled, parallel-group, single-center trial.J Infect Dis. 2004;189(8):1341-1347.
4. Whitley RJ, Kimberlin DW, Roizman B. Herpes simplex viruses.Clin Infect Dis. 1998;26(3):541-553.
5. Workowski KA. Centers for Disease Control and Prevention sexually transmitted diseases treatment guidelines.Clin Infect Dis. 2015;61(suppl 8):S759-S762.
6. Bradley H, Markowitz LE, Gibson T, McQuillan GM. Seroprevalence of herpes simplex virus types 1 and 2—United States, 1999-2010. J Infect Dis. 2014;209(3):325-333.
7. Brown ZA, Wald A, Morrow RA, Selke S, Zeh J, Corey L. Effect of serologic status and cesarean delivery on transmission rates of herpes simplex virus from mother to infant.JAMA. 2003;289(2): 203-209.
8. LeGoff J, Péré H, Bélec L. Diagnosis of genital herpes simplex virus infection in the clinical laboratory.Virol J. 2014;11:83.
9. US Preventive Services Task Force. Screening for genital herpes: recommendation statement.Am Fam Physician. 2005;72(8):1557-1561.http://www
.aafp.org/afp/2005/1015/p1557.html.Accessed
November 16, 2016.
10. US Preventive Services Task Force. Methods and Processes: section 3: topic work plan development.https://www
.uspreventiveservicestaskforce.org/Page/Name
/methods-and-processes.Updated August 2016.
11. West SL, Gartlehner G, Mansfield AJ, et al. Comparative Effectiveness Review Methods: Clinical Heterogeneity. Rockville, MD: Agency for Healthcare Research and Quality; 2010.
12. StataCorp.Stata Statistical Software: Release 14.0. College Station, TX: StataCorp LP; 2015.
13. Mark HD, Nanda JP, Roberts J, Rompalo A, Melendez JH, Zenilman J. Performance of focus ELISA tests for HSV-1 and HSV-2 antibodies among university students with no history of genital herpes.Sex Transm Dis. 2007;34(9):681-685.
14. Ashley-Morrow R, Nollkamper J, Robinson NJ, Bishop N, Smith J. Performance of focus ELISA tests for herpes simplex virus type 1 (HSV-1) and HSV-2 antibodies among women in ten diverse geographical locations.Clin Microbiol Infect. 2004; 10(6):530-536.
15. Mujugira A, Morrow RA, Celum C, et al; Partners in Prevention HSV/HIV Transmission Study Team. Performance of the Focus HerpeSelect-2 enzyme immunoassay for the detection of herpes simplex virus type 2 antibodies in seven African countries. Sex Transm Infect. 2011;87(3):238-241.
16. Smith JS, Bailey RC, Westreich DJ, et al. Herpes simplex virus type 2 antibody detection performance in Kisumu, Kenya, using the Herpeselect ELISA, Kalon ELISA, Western blot and inhibition testing.Sex Transm Infect. 2009;85(2): 92-96.
17. Golden MR, Ashley-Morrow R, Swenson P, Hogrefe WR, Handsfield HH, Wald A. Herpes simplex virus type 2 (HSV-2) Western blot confirmatory testing among men testing positive for HSV-2 using the Focus enzyme-linked immunosorbent assay in a sexually transmitted disease clinic.Sex Transm Dis. 2005;32(12):771-777.
18. Morrow RA, Friedrich D, Meier A, Corey L. Use of “biokit HSV-2 Rapid Assay” to improve the positive predictive value of Focus HerpeSelect HSV-2 ELISA.BMC Infect Dis. 2005;5:84.
19. Hogrefe W, Su X, Song J, Ashley R, Kong L. Detection of herpes simplex virus type 2–specific immunoglobulin G antibodies in African sera by using recombinant gG2, Western blotting, and gG2 inhibition.J Clin Microbiol. 2002;40(10):3635-3640.
20. van Dyck E, Buvé A, Weiss HA, et al. Performance of commercially available enzyme immunoassays for detection of antibodies against herpes simplex virus type 2 in African populations. J Clin Microbiol. 2004;42(7):2961-2965.
21. Lingappa J, Nakku-Joloba E, Magaret A, et al. Sensitivity and specificity of herpes simplex virus-2 serological assays among HIV-infected and uninfected urban Ugandans.Int J STD AIDS. 2010;21 (9):611-616.
22. Ng’ayo MO, Friedrich D, Holmes KK, Bukusi E, Morrow RA. Performance of HSV-2 type specific serological tests in men in Kenya.J Virol Methods. 2010;163(2):276-281.
23. Delany-Moretlwe S, Jentsch U, Weiss H, et al. Comparison of Focus HerpesSelect and Kalon HSV-2 gG2 ELISA serological assays to detect herpes simplex virus type 2 antibodies in a South African population.Sex Transm Infect. 2010;86(1):46-50.
24. Melville J, Sniffen S, Crosby R, et al. Psychosocial impact of serological diagnosis of herpes simplex virus type 2: a qualitative assessment.Sex Transm Infect. 2003;79(4):280-285.
25. Rosenthal SL, Zimet GD, Leichliter JS, et al. The psychosocial impact of serological diagnosis of asymptomatic herpes simplex virus type 2 infection.Sex Transm Infect. 2006;82(2):154-157.
26. Sperling RS, Fife KH, Warren TJ, Dix LP, Brennan CA. The effect of daily valacyclovir suppression on herpes simplex virus type 2 viral shedding in HSV-2 seropositive subjects without a history of genital herpes.Sex Transm Dis. 2008;35 (3):286-290.
27. Leone P, Warren T, Hamed K, Fife K, Wald A. Famciclovir reduces viral mucosal shedding in HSV-seropositive persons.Sex Transm Dis. 2007;34
(11):900-907.
28. Corey L, Wald A, Patel R, et al; Valacyclovir HSV Transmission Study Group. Once-daily valacyclovir to reduce the risk of transmission of genital herpes. N Engl J Med. 2004;350(1):11-20.
29. Kim HN, Wald A, Harris J, Almekinder J, Heitman C, Corey L. Does frequency of genital herpes recurrences predict risk of transmission? further analysis of the valacyclovir transmission study.Sex Transm Dis. 2008;35(2):124-128.
30. Mark H, Nanda JP, Joffe A, et al. Serologic screening for herpes simplex virus among university students: a pilot study.J Am Coll Health. 2008;57 (3):291-296.
31. Wild D, Patrick D, Johnson E, Berzon R, Wald A. Measuring health-related quality of life in persons with genital herpes.Qual Life Res. 1995;4(6):532-539.
32. Mujugira A, Magaret AS, Celum C, et al; Partners in Prevention HSV/HIV Transmission Study Team. Daily acyclovir to decrease herpes simplex virus type 2 (HSV-2) transmission from HSV-2/HIV-1 coinfected persons: a randomized controlled trial. J Infect Dis. 2013;208(9):1366-1374.
33. Celum C, Wald A, Lingappa JR, et al; Partners in Prevention HSV/HIV Transmission Study Team. Acyclovir and transmission of HIV-1 from persons infected with HIV-1 and HSV-2.N Engl J Med. 2010; 362(5):427-439.