Joanna Rymaszewska
1, Justyna Mazurek
2The Social and Occupational Functioning of Outpatients
from Mental Health Services*
Funkcjonowanie społeczne i zawodowe pacjentów
ambulatoryjnej opieki psychiatrycznej
1 Department of Psychiatry, Wroclaw Medical University, Poland 2 Academic Hospital, Wroclaw, Poland
Abstract
Background. Many authors stress the important correlation between disorders and social disability.
Objectives. The aim of the project was the assessment of the occupational and relational social functioning of persons who suffer from different mental disorders.
Material and Methods. During the 15 months of the project, enrollment was conducted among patients calling in to three outpatient psychiatric clinics in the Lower Silesia region in Poland. The study included persons (n = 185) at the age of 18–54 from five diagnostic groups, according to ICD-10: psychotic disorders (F2), affective disorders (F3), anxiety disorders (F4), eating disorders (F5) and personality disorders (F6). Functioning was evaluated using the Groningen Social Disabilities Schedule (GSDS II), the Social and Occupational Functioning Assessment Scale (SOFAS) and the Global Assessment of Relational Functioning (GARF).
Results. The group which had the highest level of functioning with a disability consisted of persons with the F2 diagnosis (1.42, SD = 0.63), whereas persons with anxiety disorders had the lowest disability (0.72, SD = 0.59). The severity of psychopathological symptoms was indeed related to social functioning. There was a significant correlation between general social functioning (the overall GSDS score) and the number of episodes (cor = 0.289; p = 0.001), hospitalizations (cor = 0.352; p < 0.001) and days on leave (cor = 0.393; p < 0.001) for the sample as a whole.
Conclusions. The functional disabilities indicated within the majority of patients give strong arguments for intro-ducing the diagnosis and therapy of these disabilities and implementation of them to the standards of psychiatric treatment (Adv Clin Exp Med 2012, 21, 2, 215–223).
Key words: social disability, functioning, mental disorders, outpatient clinics.
Streszczenie
Wprowadzenie. Wielu autorów podkreśla istotną korelację między zaburzeniem psychicznym a niesprawnością społeczną.
Cel pracy. Ocena poziomu niesprawności społecznej i zawodowej wśród osób z różnymi rozpoznaniami psychia-trycznymi.
Materiał i metody. Badanie przeprowadzono w ciągu 15 miesięcy wśród pacjentów zgłaszających się do trzech poradni zdrowia psychicznego na Dolnym Śląsku w Polsce. Do badania zostały włączone osoby (n = 185) w wieku 18–54 lat z pięciu grup diagnostycznych według ICD-10: zaburzeń schizofrenicznych (F2), zaburzeń afektyw-nych (F3), zaburzeń nerwicowych, związaafektyw-nych ze stresem i pod postacią somatyczną (F4), zaburzeń odżywiania (F5) i zaburzeń osobowości (F6). Funkcjonowanie oceniano za pomocą Formularza Niesprawności Społecznej Groningen (GSDS II), Skali Oceny Funkcjonowania Społeczno-Zawodowego (SOFAS) oraz Skali Globalnej Oceny Funkcjonowania w Związkach (GARF).
Wyniki. Osoby z zaburzeniami schizofrenicznymi (F2) odznaczały się najwyższym poziomem niesprawności spo-łecznej (1,42, SD = 0,63), a pacjenci z zaburzeniami nerwicowymi, związanymi ze stresem i pod postacią soma-tyczną – najniższym (0,72; SD = 0,59). Nasilenie objawów psychopatologicznych w sposób istotny było związane z funkcjonowaniem społecznym. Stwierdzono istotną korelację między ogólnym poziomem niesprawności
spo-Adv Clin Exp Med 2012, 21, 2, 215–223 ISSN 1899–5276
ORIGINAL PAPERS
© Copyright by Wroclaw Medical University
łecznej oraz liczbą epizodów (cor = 0,289; p = 0,001), hospitalizacji (cor = 0,352; p < 0,001) oraz dni na urlopie (cor = 0,393; p < 0,001) dla całej grupy pacjentów.
Wnioski. Stwierdzone u większości badanych zaburzenia funkcjonowania społecznego uzasadniają wprowadzenie terapii tych zaburzeń do standardów leczenia psychiatrycznego (Adv Clin Exp Med 2012, 21, 2, 215–223).
Słowa kluczowe: niesprawność społeczna, funkcjonowanie, zaburzenia psychiczne, pacjenci leczeni ambulatoryjnie.
Research results confirm that in social dis-ability, the mental factor often plays a much larger role than the somatic factor. Disability caused by mental disorders is considered equal to or even larger than in chronic, serious physical illnesses [4, 13]. The occurrence of a mental disorder, even at a subliminal level, is connected to an aggravation of social life [29]. Furthermore, unemployed per-sons suffer from mental disorders twice as often as those employed [11]. It is believed that work, for many of the mentally ill, constitutes an important mechanism for coping and enables them to main-tain social contacts [18]. Experience from practice proves beyond doubt the need for assessment and the taking into account of changes in the patients’ functioning during the therapy.
The problem of social disability has been un-dertaken using cases of patients that had different mental diagnoses, e.g. schizophrenia or with anxi-ety, mood, personality or eating disorders [6, 22, 28]. Studies have been conducted on patients with depression [2, 4, 20], persons with depression and a chronic somatic illness [28] and with subdepres-sive symptoms [12]. There are also studies on the disability of persons with personality and eating disorders [8, 22, 27], who, before having treatment in a hospital, function worse than persons suffer-ing from anxiety disorders [26]. The influence of socio-demographic parameters (e.g. age, gender, family situation, occupational status and marital status) on the severity of disorders in social func-tioning were also verified [1, 27]. Many authors stress the important correlation between disorders and social disability [2, 21]. Also, the connection between social malfunction and the general num-ber of requirements of patients with mental diag-noses has been examined [15, 23].
The aim of the project was the assessment of the occupational and relational social functioning of persons who have different mental disorders and its predictors.
Material and Methods
During the first 15 months of the project, enrollment was conducted within patients call-ing in to the outpatient psychiatric clinic of the Academic Specialist Health Center and the men-tal hospimen-tals in Wroclaw, Swidnica and Zabkowice
Slaskie in the Lower Silesia region of Poland. The study included persons at the age of 18–54 from five diagnostic groups according to ICD-10: psy-chotic disorders, incl. schizophrenia (F2), affec-tive disorders (F3), neurotic, stress-related and
somatoform disorders (F4), eating disorders (F5)
and personality disorders (F6). The inclusion cri-teria was the lack of a stated inability to work and written consent.
The criteria for exclusion from the study were: addiction to alcohol or other psychoactive sub-stances, dementia, serious, chronic somatic dis-eases and the inability to give conscious agreement to participate in the study.
Instruments
Social disability was assessed using the Gron-ingen Social Disabilities Schedule (GSDS II), which is a semi-structuralized interview used for evaluation of disorders in social functioning in several social roles (self-care, family, kinship, part-ner, citizen, social and occupational) both in non-psychiatric and non-psychiatric patients, irrespectively of the total of their psychopathological symptom-atology. The sum score was based on overall role ratings. The higher score in GSDS II, the worse the social functioning.
Occupational functioning was evaluated by the Social and Occupational Functioning Assessment Scale (SOFAS), that focuses exclusively on the in-dividual’s level of occupational functioning and is not directly influenced by the overall severity of the individual’s psychological symptoms.
The Global Assessment of Relational Func-tioning (GARF) was used to indicate an overall judgment of the functioning of a family or other ongoing relationship. SOFAS and GARF are one-dimensional scales (0–100 points) which are based on DSM-IV. They are helpful in the assessment of social, occupational and relational (family, part-ner) functioning irrespectively of the patient’s di-agnosis.
The Brief Psychiatric Rating Scale was used
of psychopathological symptoms, which consists of 24 positions and enables a quick assessment of the main symptoms of mental illnesses (depres-sion, anxiety, hallucinations, delusions, activity, suicidality, hostility, guilt, elevated mood, bizarre behavior, self-neglect, etc.) and also the dynamics of their changes over time.
Statistical Methods
The research material gathered was analyzed, taking into account its diversity, using the pro-gram R package 2.4.1. The data was divided into the following parameters: dependent variables, which included the overall scores of the GSDS II, SOFAS and GARF scales, and independent variables such as socio-demographic and clinical parameters (age, gender, education, occupational category, marital status and diagnostic group), clinic diagnosis in accordance to ICD-10 and the overall score of the BPRS scale. A Pearson’s test was used to compare qualitative attributes be-tween diagnosis groups and within these groups due to other factors. This was verified with the Monte Carlo method. A Spearman’s rank corre-lation coefficient was used to define the strength of the connection between continuous variables. A basic comparison of two tests was conducted using a Student’s t-test and its non-parametric equivalent, the Mann-Whitney test. Test statis-tics were verified using a two-tailed test, at the significance level of 0.05. The overall scores of the scales and subscales for all patients and diagno-sis groups were counted as an arithmetic mean. Missing observations and cases in which patients refused to answer the question were not taken into account in stating the arithmetic means. Regression analysis, including stepwise multiple block regression and two step multiple regres-sion, was constructed to examine the relation of a dependent variable to specified independent variables.
The study was approved by the Commission of Bioethics at Wroclaw Medical University. All participants provided written informed consent to participate in the study.
Results
Group Description
The average age (n = 185) was 34.8 (SD = 11.3), Table 1. The examined patients were grouped into diagnostic categories in accordance with the main psychiatric diagnosis according to ICD-10 classifica-tion. Among all patients, the majority were persons whose main diagnosis was recognized as neurotic,
stress-related and somatoform disorders (F4, n =
58). The subsequent groups, in respect to quantity, consisted of persons with affective disorders (F3, n = 44), personality disorders (F6, n = 36), and schizo-phrenic disorders (F2, n = 32). The smallest group consisted of patients with diagnosed eating disor-ders (F5, n = 16). Essential statistical differences be-tween diagnosis groups (p < 0.001) were indicated. Patients from group F5, with eating disorders, have the lowest age average (23.7) comparing to the rest of the patients, and the highest ages correspond to patients from group F4, with neurotic,
stress-relat-ed and somatoform disorders (38.8), and F3, with
affective disorders (38.7). In all the tested groups there were more women (n = 132, 71%) than men, Table 2. The exception was eating disorders, from which only women suffered (n = 16). Among the patients described, the most had secondary educa-tion (n = 96, 51.9%) and the least had only com-pleted their education at a primary level (n = 16, 8.6%). Particular diagnostic groups did not differ significantly with respect to the level of education. Nearly two thirds of those tested were workers (n = 116, 63%). 74 persons (40%) remained in a for-mal relationship, the least of the patients were in the group widow/widower (n = 6, 3.3%) and only a few lived alone (n = 13, 7%).
Table 1. Mean age in the diagnostic groups
Tabela 1. Średnia wieku w grupach diagnostycznych
Min. 1st Qu. Median. Mean 3rd Qu. Max Std NA’s
F2 19.00 23.00 29.00 30.26 32.50 54.00 10.15 1.00
F3 19.00 30.00 36.00 37.36 47.00 55.00 11.27 2.00
F4 20.00 29.50 41.00 38.03 48.00 57.00 10.64 1.00
F5 19.00 20.00 23.00 24.54 27.00 32.00 4.72 1.00
The Severity of
Psycho-pathological Symptoms (BPRS)
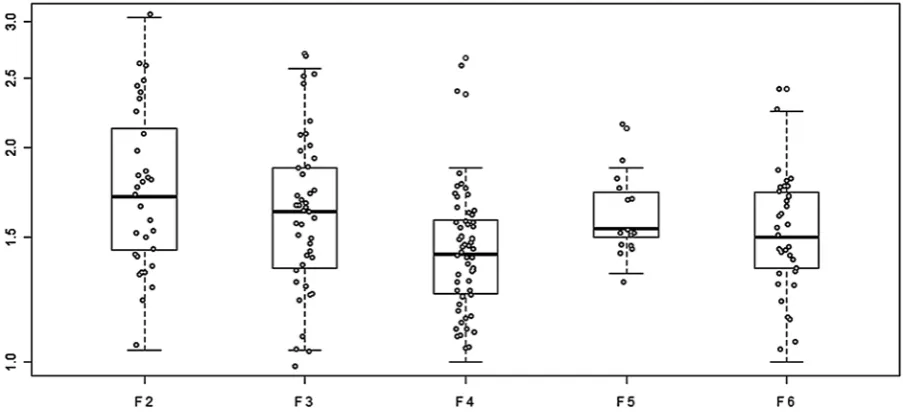
The studied group of patients obtained an overall score of approximately 1.61 (SD = 0.38). For half of the patients, the results were in the range of 1.38–1.7 5. The differences between di-agnostic groups were statistically significant (p = 0.001). Persons with schizophrenic disorders had the highest average BPRS result (1.80, SD = 0.48), and patients with neurotic, stress-related and
so-matoform disorders had the lowest results (1.45,
SD = 0.29), Figure 1.
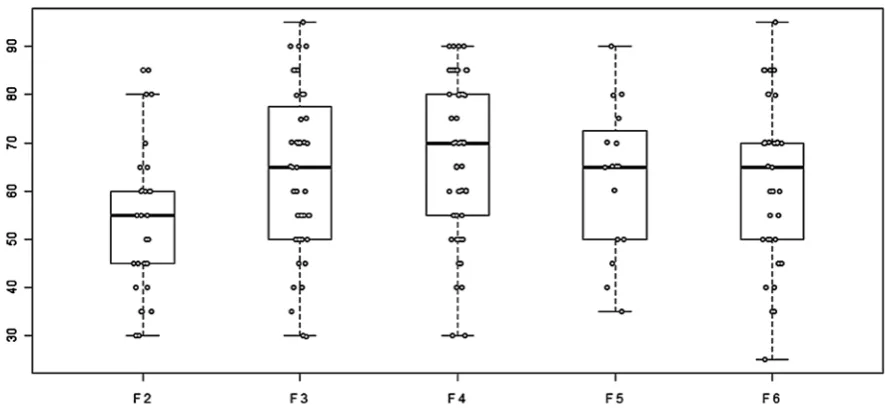
Relational Functioning (GARF)
On the Global Assessment of Relational Func-tioning Scale the examined patients obtained a mean result of 61.67 (SD = 16.32). Significant statistical differences between the diagnostic groups were observed (p < 0.001). Persons from diagnostic group F2 (53.59, SD = 13.93) obtained the lowest result in the scale, and persons from group F4 (68.71, SD = 14.16) the highest. A nega-tive, directly proportional correlation between overall scores of the GSDS II and GARF scales (r =
-0.695; p < 0.001) was observed. According to sta-tistics, patients with higher social disability in fact also functioned worse in relations, Figure 2.
Social and Occupational
Functioning Assessment Scale
(SOFAS)
The examined patients obtained an average re-sult of 63.92 (SD = 17.43). Significant differences be-tween diagnostic groups (p < 0.01) were noted. As in the case of the GARF scale, the largest dispropor-tions concerned patients with a main diagnosis F4 or F2 (p = 0.0013). Indeed, patients with neurotic,
Table 2. Gender in the diagnostic groups
Tabela 2. Płeć w grupach diagnostycznych
F2 F3 F4 F5 F6
Female (Żeńska) 15 26 30 13 16 Male (Męska) 8 8 9 0 13
Fig. 1. The results of BPRS in diagnostic groups
Ryc. 1. Wyniki BPRS w grupach diagnostycznych
Fig. 2. Overall score of GSDS II in respect to overall GARF score
stress-related and somatoform disorders (67.81, SD = 16.28) had the highest average results and persons with schizophrenic disorders – the lowest (53.44, SD = 14.39), which is presented in Figure 3. Similarly, as in the relation between GSDS II and GARF, here also a negative, directly proportional correlation between overall scores of GSDS II and SOFAS (r = -0.759; p < 0.001) was observed. The lower the GSDS II result, the higher the SOFAS result, Figure 4.
Social Functioning (GSDS II)
The studied group obtained an average result of 1.06 (SD = 0.66), which corresponds to a func-tioning disorder at a low rate. Half of the examined
obtained results from 0.57 to 1.50. Results signifi-cantly varied between patients from different di-agnostic groups (p < 0.001). The group which had the highest level of functioning disorder consisted of persons with the F2 diagnosis (1.42, SD = 0.63). Patients from groups F5 (1.09, SD = 0.56) and F3 (1.09, SD = 0.73) functioned at a similar level as persons from group F3 (1.03, SD = 0.55), whereas persons diagnosed as F4 showed disability of so-cial functioning at the level 0.72 (SD = 0.59). The particular statistical parameters are presented in Table 1.
The analyses showed significantly statistical differences in the overall scores of GSDS II be-tween persons in a formal relationship and single persons (p = 0.0086) and between people in infor-mal relationships and single persons (p = 0.0012). Patients with a marital status defined as single had significantly higher GSDS II results (worse social functioning) than patients remaining in a formal or informal relationship.
A significant difference between persons living alone and people living with others were indicated (p < 0.01). Persons living alone had a significantly lower overall GSDS II scale score (better social functioning).
The overall GSDS II score for persons with higher education was considerably lower than for persons with primary education (p < 0.01).
No correlation between the overall GSDS II score and age (p < 0.05), gender (p < 0.05) or oc-cupation category (p < 0.05) was noted.
There was a significant correlation between the overall GSDS score and the number of: pre-vious episodes (r = 0.289; p = 0.001), psychiatric hospitalizations (r = 0.352; p < 0.001) and days
Fig. 3. Overall score of SOFAS in respect to overall score of BPRS
Ryc. 3. Ogólny wynik SOFAS w odniesieniu do ogólnego wyniku BPRS
Fig. 4. Overall score of GSDS II in respect to overall SOFAS score
on leave (r = 0.393; p < 0.001) for the sample as a whole.
A positive, directly proportional correlation between overall scores of the GSDS II and BPRS scales (r = -0.684; p < 0.001) was observed. Indeed, patients with larger social disability had more se-vere psychopathological symptoms, Figure 5.
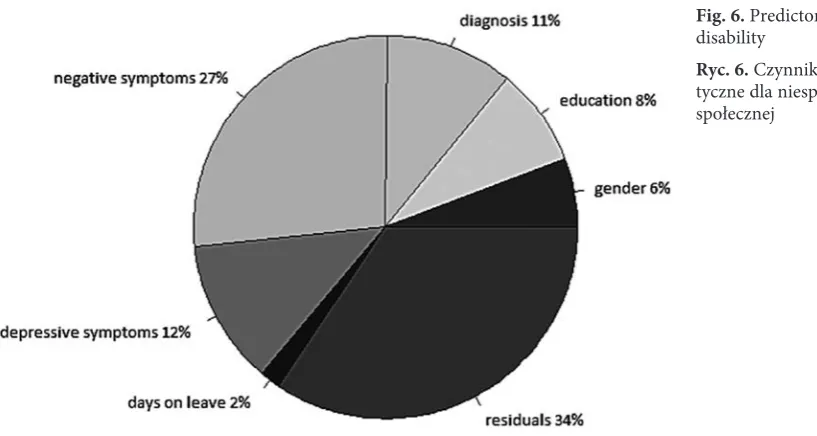
Considering regression analyses, a high level of negative symptoms appeared as the strongest pre-dictor of social disability. Depressive symptoms, main diagnosis, education and gender were other important predictors which all together explained 66% of the variance, Figure 6.
Discussion
The social functioning of persons from four different diagnostic groups was compared taking into account the connections of different factors. On the basis of comparison of the overall GSDS II
score between diagnostic groups, it was stated that patients with neurotic, stress-related and soma-toform disorders had statistically the lowest level of social disability in comparison to the examined patients with affective, schizophrenic, personality and eating disorders. In this study, the social dis-ability differences between persons with affective, eating and personality disorders have not been in-dicated. These results partially confirm the results obtained in previous research conducted in several European centers (n = 969) [26], where during the period of severity of symptoms, persons with eat-ing, personality and schizophrenic disorders func-tioned worse than persons with affective and neu-rotic disorders. In population studies conducted in Belgium, France, Germany, Italy, Holland and Spain (n > 21,000) which assessed the correlation between mental and physical disorders and dif-ferent areas of functioning, Biust-Bouwman and co-authors stated that the largest connection with disability is among anxiety disorders, which are followed by mood disorders and those related to alcohol [4]. Other authors confirm a direct con-nection between the level of disability and diag-nostic category. Sanderson and Andrews showed that the greatest disability is found among patients with affective and anxiety disorders [27] and Rie and co-authors have proven that social disabil-ity is higher among persons with personaldisabil-ity and eating disorders than among persons with fear or mood symptoms [22]. In Bij and Ravelli’s re-search, the level of social disability was different depending on the main psychiatric diagnosis, and the highest degree of disability was found among persons with affective disorders [2]. Simon stated that functioning got worse in the case of persons with affective disorders [28], whereas in Bilder’s and Mechanic’s research, patients with the same diagnosis functioned worse in all the areas of the Functional Status Questionaire, in comparison to general population [3]. According to Judd and co-authors, it is the subdepressive state that can be linked with psycho-social disability [12]. However, the conclusion of a significant correlation between
Table 3. The results of GSDS II in diagnostic groups
Tabela 3. Wyniki GSDS II w grupach diagnostycznych
Min. 1st Qu. Median Mean 3rd Qu. Max. SD Missing F 2 0.43 1.09 1.29 1.42 1.78 2.71 0.63 0.00 F 3 0.00 0.57 1.00 1.09 1.57 2.57 0.72 0.00 F 4 0.00 0.26 0.62 0.72 0.97 2.50 0.59 0.00 F 5 0.29 0.82 1.00 1.09 1.31 2.29 0.56 0.00 F 6 0.00 0.71 1.00 1.03 1.43 2.12 0.55 0.00
Fig. 5. Overall score of GSDS II in respect to the over-all BPRS score
psychiatric diagnosis and functioning hasn’t been confirmed unanimously. Some authors have prov-en a lack of direct connection betweprov-en the level of occupational skills and diagnostic category [1, 10]. Detailed comparisons are impossible due to meth-odological differences.
The severity of psychopathological symptoms was indeed related to social functioning: patients with more intensified mental disorder functioned much worse. This conclusion has been confirmed in many studies [2, 19] and some authors have stressed that the severity of psychopathological symptoms has more importance for the level of so-cial disability than the type of diagnosis [24, 25].
Neither the age nor gender nor occupational category have any significant influence on social functioning within the examined group. Among researchers, there is lack of agreement whether there is an influence of gender on social function-ing within patients with different diagnostic cat-egories. Sanderson and Andrews obtained different results, in which functioning was different between men and women suffering from mental illnesses, finding it advantageous to women [27]. Melle and co-authors proved that, among those suffering from schizophrenia, the male gender and higher educa-tion were connected to better funceduca-tioning [16], whereas Wiersma and co-authors confirmed the lack of influence of gender on disability amongst patients with the same diagnosis [30].
Górna and Rybakowski proved the lack of es-sential significance of marital status with social functioning among persons receiving outpatient
treatment [9]. However in the present study, per-sons with a marital status defined as single func-tioned much worse than persons remaining in formal or informal relationships.
The comparison of the level of social disabil-ity among persons from different diagnostic cat-egories made it possible to come to the following conclusions.
Among patients from outpatient psychiatric clinics, persons with schizophrenic disorders (F2) functioned relatively the worst and patients with neurotic, stress-related and somatoform disorders (F4) the best. A similar level of disability was char-acteristic for patients with eating, affective and personality disorders.
Among the rest of the independent variables, severity of psychopathological symptoms, marital status, residence and education were significant for the level of social disability. The higher the social disability, the worse the social-occupational and relational functioning. The more intensified the psychopathological symptoms, the higher the social disability.
The level of social efficiency didn’t differ among patients based on age, gender and occupa-tional category.
Negative symptoms, depressive symptoms, main diagnosis, education and gender were sig-nificant predictors of social disability.
The social functioning disabilities indicated within the majority of patients give reason to in-troduce the diagnosis and therapy of these disabil-ities to the standards of psychiatric treatment.
Fig. 6. Predictors of social disability
References
[1] Bell MD, Lysaker PH: Clinical benefits of paid work activity in schizophrenia: 1-year followup. Schizophr Bull 1999, 23(2), 317–128.
[2] Bijl RV, Ravelli A: Current and residual functional disability associated with psychopathology: findings from the Netherlands Mental Health Survey and Incidence Study (NEMESIS). Psychol Med 2000, 30(3), 657–668.
[3] Bilder S, Mechanic D: Navigating the disability process: persons with mental disorders applying for and receiving disability benefits. Milbank Q 2003, 81(1), 75–106.
[4] Buist-Bouwman MA, De Graaf R, Vollebergh WAM, Alonso J, Bruffaerts R, Ormel J, and the ESEMeD/ AHEDAE 2000 investigators: Functional disability of mental disorders and comparison with physical disorders: a study among the general population of six European countries. Acta Psychiatr Scand 2006, 113, 492–500. [5] Buist-Bouwman MA, de Graaf R, Ormel J, Vollebergh WA: Functioning after a major depressive episode:
com-plete or incomcom-plete recovery? J Affect Disord 2004, 82(3), 363–371.
[6] Druss BG, Marcus SC, Rosenheck RA, Olfson M, Tanielian T, Pincus HA: Understanding disability in mental and general medical conditions. Am J Psychiatry 2000, 9, 1485–1491.
[7] Faulkner A, Layzell S: Strategies for Living. A report of user-led research into people’s strategies for living with mental distress. London: The Mental Health Foundation 2000.
[8] Flament MF: Predictive factors of social disability in patients with eating disorders. Eat Weight Disord 2001, 6, 99–106.
[9] Górna K, Rybakowski J: Social functioning of patients with schizophrenia: a follow-up study. Psychiatr Pol 1995, 29(5), 619–129.
[10] Gureje O, Herrman H, Harvey C, Morgan W, Jablensky A: The Australian National Survey of Psychotic Disorders: profile of psychosocial disability and its risk factors. Psychol Med 2002, 32, 639–648.
[11] Jenkins R, Bebingron P, Brugha TS, Farrell M, Lewis G, Meltzer H: British Psychiatric Morbidity. Br J Psychiatry 1998, 173, 4–7.
[12] Judd LL, Akiskal HS, Zeller PJ, Paulus M, Leon AC, Maser JD, Endicott J, Coryell W, Kunovac JL, Mueller TI, Rice JP, Keller MB: Psychosocial disability during the long-term course of unipolar major depressive disorder. Arch Gen Psychiatry 2000, 57(4), 375–380.
[13] LaPlante MP, Carlson D: Disability in the United States: Prevalence and causes, 1992. Disability Statistics Report, 7. Washington D.C: U.S. Department of Education. National Institute on Disability and Rehabilitation Research 1996. [14] Lehtinen V, Riikonen E, Lahtinen E: Promotion of mental health on European Area. STAKES National Research
and Development Center for Welfare and Health 1998.
[15] Middleboe T, Bengtsson-Tops A, Bjarnason O, Dybbro J, Karlsson H, Hansson L, Mackeprang T, Nilsson LL, Sandlund M, Sorgaard KW, Werdelin G: The Nordic study on schizophrenic patients living in the community. Subjective needs and perceived help. Eur Psychiatry 2001, 16, 201–215.
[16] Melle I, Friis S, Hauff E, Vaglum P: Social functioning of patients with schizophrenia in high-income welfare societies. Psychiatr Serv 2000, 51(2), 223–228.
[17] Mykletun A, Overland S, Dahl AlvA, Krokstad S, Bjerkest O, Glozier N, Aaro LE, Prince M: A Population-Based Cohort Study of the Effect of Common Mental Disorders on Disability Pension Award. Am J Psychiatry 2006, 163, 1412–1418.
[18] Noble JH: Policy reform dilemmas in promoting employment of persons with severe mental illnesses. Psychiatr Serv 1998, 4, 775–781.
[19] Olfson M, Lewis-Fernandez R, Weissman MM, Feder A, Gameroff MJ, Pilowsky D, Fuentes M: Psychotic symptoms in an urban general medicine practice. Am J Psychiatry 2002, 159(8), 1412–1419.
[20] Ormel J, Oldenhinkel AJ, Simon G, Tiemans BG, Ustun TB, Vonkorff M: Onset of disability in depressed and non-depressed primary care patients. Psychol Med 1999, 29(4), 847–853.
[21] Ormel J, Brilman E, Katon W, Oldenhinkel T, Van den Brink W, Von Korff M: Depression, anxiety and social disability show synchrony of change in primary care patients. Am J Publ Health 1993, 83(3), 385–390.
[22] Rie S, Noordenbos G, Donker M, Furth E: The patient’s view on quality of life and eating disorders. Int J Eat Disord 2007, 40(1), 13–20.
[23] Ruggeri M, Bonizzato P, Fontecedro L, Leese M, Slade M, Tansella M: Demographic, clinical, social and ser-vice variables associated with higher needs for care in community psychiatric serser-vice patients. The South Verona Outcome Project 8. Soc Psychiatry Psychiatr Epidemiol 2004, 39, 60–68.
[24] Rymaszewska J, Kiejna A, Jarosz-Nowak J, Kallert T, Nawka P, Priebe S, Raboch J: Social disability among mentally ill from different European countries. Acta Psychiatr Scand 2004a, 421, 25.
[25] Rymaszewska J, Kiejna A, Kallert T, Nawka P, Priebe S, Raboch J: Work and severe mental disorders in five European countries. Eur Psychiatry 2004b, 19 suppl 1, 84.
[26] Rymaszewska J, Jarosz-Nowak J, Kiejna A, Kallert T, Schutzwohl M, Priebe S, Wright D, Nawka P, Raboch J:
Social disability in different mental disorders. Eur Psychiatr 2007, 22, 160–166.
[27] Sanderson K, Andrews G: Prevalence and severity of mental health-related disability and relationship to diagno-sis. Psychiatr Serv 2002, 53(1), 80–86.
[28] Simon GE: Social and economic burden of mood disorders. Biol Psychiatry 2003, 54, 208–215.
[30] Wiersma D, Wanderling J, Dragomirecka E, Ganev K, Harrison G, An Der Heiden W, Nienhuis FJ, Walsh D:
Social disability in schizophrenia: its development and prediction over 15 years in incidence cohorts in six European centers. Psychol Med 2000, 30(5): 1155–1167.
Address for correspondence:
Justyna Mazurek Faculty of Physiotherapy
Wroclaw University of Physical Education Łęczycka 11/4
53-632 Wrocław Poland
Tel.: +48 695 18 09 84
E-mail: [email protected]
Conflict of interest: None declared