Maciej Bagłaj
1, a–d, f, Sylwester Gerus
1, B–d, Urszula dorobisz
2, c, e,
Tadeusz Łukieńczuk
3, c, e, Beata Wikiera
4, c, eThyroidectomy in Children:
Changing Trends and Surgical Strategies
Tyreoidektomia u dzieci: zmieniające się trendy epidemiologiczne
i strategie postępowania chirurgicznego
1 department of Pediatric Surgery and Urology, Wroclaw Medical University, Poland 2 department of Radiology, Wroclaw Medical University, Poland
3 department of General Surgery, Wroclaw Medical University, Poland 4 department of Pediatric endocrinology, Wroclaw Medical University, Poland
A – research concept and design; B – collection and/or assembly of data; C – data analysis and interpretation;
D – writing the article; E – critical revision of the article; F – final approval of article; G – other
Abstract
Background. Surgical thyroid pathology is an uncommon problem in children and due to environmental factors may be locally-specific. Until the mid-90’s, Lower Silesia had been regarded as a region of endemic goiter but since then a better system of iodine prophylaxis has been introduced.
Objectives. To assess changing trends in the epidemiology of surgical thyroid diseases in children and to examine whether they have influenced potential alterations of operative strategies during the study period.
Material and Methods. The medical records of all children operated on for thyroid disease between 1993 and 2010 in the university pediatric surgical center were retrospectively reviewed. The data regarding the indications for thyroidectomy, details of surgical management and outcome were collected and analyzed in three periods of time 1993–1998, 1999–2004 and 2005–2010.
Results. There were 46, 63 and 41 children operated on in the analyzed periods of time, respectively, with no sig-nificant differences regarding their age and gender. Preoperative thyroid ultrasound scan showed nodular lesions within the thyroid gland in 145 children (94.7%). The frequency of unilateral and bilateral nodular lesions was basi-cally similar throughout the whole study. There has been a significant decrease in subtotal resections from around 63% in the first period to less than 16% in the other two periods of the study. The reverse trend can be clearly seen with regard to unilateral total lobectomy. Since 1999, total lobectomy or total thyroidectomy has been performed in more than 80% of the children. Nodular goiter was the most common indication for surgical operation followed by follicular adenoma. Malignant disease was recorded in 7 children (4.6%).
Conclusions. The gradual decrease of the number of children with surgical pathology of the thyroid gland seems to reflect an effective iodine prophylaxis. depending on the extent of thyroid disease, unilateral lobectomy, either alone or coupled with partial or total resection of the contralateral lobe should be a standard surgical procedure in children (Adv Clin Exp Med 2013, 22, 3, 387–393).
Key words: thyroid, children, thyroidectomy, goiter, thyroid nodule.
Streszczenie
Wprowadzenie. chirurgiczne schorzenia tarczycy są rzadkie u dzieci. Na ich występowanie mają wpływ czynniki środowiskowe. do lat 90. XX w. dolny Śląsk był uznawany za obszar endemicznego wola, od tego czasu został jednak wprowadzony lepszy i skuteczniejszy system profilaktyki jodowej.
Cel pracy. Ocena zmiennych trendów epidemiologicznych schorzeń chirurgicznych tarczycy u dzieci oraz wyko-nanie oceny, czy miały one wpływ na zmianę strategii postępowania chirurgicznego.
Materiał i metody. Przeprowadzono retrospektywną analizę dokumentacji medycznej dzieci poddanych leczeniu chirurgicznemu w latach 1993–2010 w referencyjnym ośrodku uniwersyteckim chirurgii dziecięcej. Szczegółowej
adv clin exp Med 2013, 22, 3, 387–393 ISSN 1899–5276
ORIGINaL PaPeRS
ocenie poddano wskazania do zabiegu operacyjnego, szczegóły zabiegu oraz wyniki leczenia. dane były oceniane i analizowane w trzech okresach: 1993–1998, 1999–2004 i 2005–2010.
Wyniki. W analizowanych okresach operowano odpowiednio 46, 63 i 41 dzieci bez istotnych różnic statystycznych w odniesieniu do wieku i płci pacjentów. Zmiany guzkowe wykazano na podstawie przedoperacyjnego badania USG u 145 dzieci (94,7%). częstość występowania zmian obejmujących jeden płat lub oba płaty była zbliżona we wszystkich analizowanych okresach badawczych. Odsetek resekcji subtotalnych bardzo wyraźnie zmniejszył się z 63% w pierwszym okresie do mniej niż 16% w trzecim okresie. Odwrotny trend obserwowano w odniesieniu do jednostronnego usunięcia płata tarczycy. Od 1999 roku całkowite usunięcie co najmniej jednego płata było wyko-nane u ponad 80% dzieci. Najczęstszym wskazaniem do leczenia chirurgicznego było wole guzkowe oraz gruczolak pęcherzykowy. Nowotwory złośliwe odnotowano tylko u 7 dzieci (4,6%).
Wnioski. Stopniowe zmniejszanie częstości występowania schorzeń tarczycy leczonych chirurgicznie u dzieci wydaje się wynikać ze skuteczniejszego programu profilaktyki jodowej na terenie dolnego Śląska. Jednostronna totalna lobektomia uzupełniona o częściowe lub całkowite wycięcie drugiego płata powinna być przyjęta jako stan-dardowy zabieg chirurgiczny u dziecka ze schorzeniem chirurgicznym tarczycy (Adv Clin Exp Med 2013, 22, 3, 387–393).
Słowa kluczowe: tarczyca, dzieci, tyreoidektomia, wole, wole guzkowe.
Surgical thyroid diseases are relatively uncom-mon in children. although the indications for their operative management are predominantly based on a higher risk of malignancy in this age group, strategies applied by pediatric surgeons frequently follow those used in adult patients. a unique fea-ture of thyroid pathology is the fact that due to environmental factors it may be locally-specific. Iodine deficiency must be numbered as one of the most important factors involved in the etiology of diseases of the thyroid gland in the pediatric popu-lation [1, 2]. Until the mid-90’s, Lower Silesia had been regarded as a region of endemic goiter. Since then an effective system of iodine prophylaxis has been introduced in Poland [3]. Taking these facts into consideration, the authors have undertaken a 18-year retrospective review of their experience with thyroidectomy in children. The authors spe-cifically aimed to assess changing trends in the epi-demiology of surgical thyroid diseases in children from Lower Silesia and to examine whether they have influenced potential alterations of operative strategies during the study period.
Material and Methods
The medical files of all children who under-went operative treatment due to disease of the thyroid gland between 1993 and 2010 at the Uni-versity department of Pediatric Surgery in Wro-claw were selected from the hospital database and subjected to a detailed analysis. The department of Pediatric Surgery is the only center offering an operative management of thyroid pathology in children in the south-west region of Poland, which has more than 3.5 million inhabitants. all of the children were referred to the surgical department by a pediatric endocrinologist. Preoperative diag-nosis included hormonal studies, ultrasound scan of the thyroid gland and fine-needle aspiration
biopsy in all patients. Thyroid scintigraphy was part of the routine work-up during the first years of the study period. Later it was ordered routinely in the cases presenting with hyperthyreosis only. Indications for an operative procedure were estab-lished by an endocrinologist and surgeon together. during the first two years of the study period, the operative procedures were performed by or under supervision of the surgeon from the department of General Surgery of the Wroclaw Medical Univer-sity. Since 1995 all operative procedures have been performed by the senior author (MB).
The data regarding the patients’ demograph-ics, previous medical history, clinical presentation of thyroid disease, and the results of hormonal and imaging studies were selected and analyzed in all patients. The details of the surgical procedure were extracted from the operative notes. Three basic categories of thyroidectomy were arbitrarily accepted for the purpose of this study, namely: partial, subtotal and total resection, each referring either to one lobe or to the entire gland. In each case the final diagnosis was made by the patholo-gist examining the resected specimen. In order to comply with the principal aim of the retrospective study, all data was analyzed separately in the three 6-year consecutive periods; 1993–1998, 1999–2004 and 2005–2010.
Statistical significance between frequencies was calculated by the chi-square test χ2
df with Yate’s
correction with a corresponding degree of freedom df (df = (m–1)*(n–1), where m – number of rows, n – number of columns) or if the expected value was less than 5, by a fisher exact test (f).
Results
One hundred and fifty children constituted the study group. Their age ranged from 7 to 18 years (mean 14.8). Three children were operated on twice because of the recurrence of nodular goiter after ini-tial subtotal resection and therefore the total num-ber of operations was 153. There were 116 girls (77.3%). The incidence of surgical thyroid disease among boys in the analyzed periods was 19.6%, 25.3% and 22.5% respectively (p > 0.05). There were no statistical differences when the mean age of the patients in each study period was studied. Preop-erative thyroid ultrasound showed nodular lesions within the thyroid gland in 145 children (94.7%). In 8 children the thyroid gland showed diffuse en-largement of both lobes. Table 1 illustrates the dis-tribution of pathological lesions of the gland in the analyzed patients when assessed by preoperative ultrasound scan. comparing all three studied peri-ods, two trends could be detected, namely decreas-ing number of children with diffuse enlargement of the thyroid gland and slowly increasing incidence of thyroid disease affecting both lobes. Only when
comparing the first and the third period were the differences statistically significant, with a p-value of 0.0172 and x = 13.8.
One hundred eleven children (74%) were eu-thyroid on initial presentation. In thirty-three chil-dren (22%) hormonal studies revealed hyperthy-roid status. Only six children (4%) suffered from hypothyroidism. When this data is analyzed in the three periods of study, the incidence of euthyroid patients rose from 63% to 76.2% between 1999 and 2004 and up to 87.7%. The distribution of patients with hyperthyroidism was 37.2%, 18.75% and 12.2%, respectively.
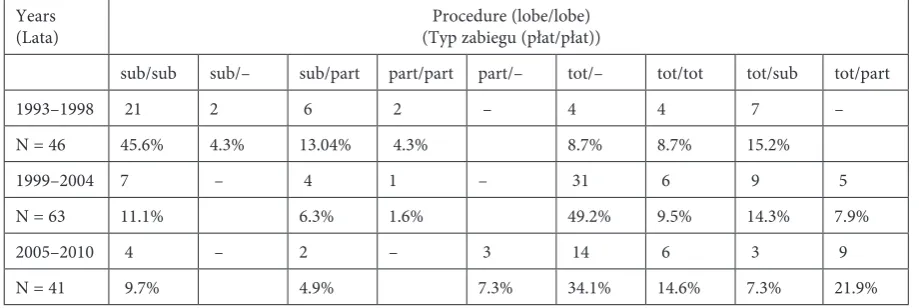
In Table 2, surgical procedures were summa-rized in the three studied periods. during the first years, subtotal resection of the thyroid gland was the preferable operative option regardless of the extension of thyroid disease. This was the prin-ciple applied by the adult surgeons supervising the first procedures performed in the clinic. It had been followed by the authors until around 1998 unless there were indications for another type of thyroid resection. during this period, thyroid scintigraphy was a routine preoperative study. The
Table 1. Pathological anatomy of the thyroid gland assessed on the preoperative ultrasound scan
Tabela 1. Zmiany anatomiczne gruczołu tarczowego ocenione na podstawie przedoperacyjnego badania ultrasonograficznego Years
(Lata) Total (Ogółem) Only one lobe affected (Tylko w jednym płacie) Both lobes affected (Zmiany w obu płatach) diffuse (Zmiany rozsiane) single lesion
(pojedyncza zmiana)
multiple le-sions (mnogie zmiany)
single lesion (pojedyncza zmiana)
multiple lesions (mnogie zmiany)
single lesion (pojedyncza zmiana)
multiple lesions (mnogie zmiany)
enlargement (powiększe-nie)
1993–1998 46 18 (39.1%) 8 (17.4%) 2 (4.3%) – 12 (26%) 6 (13%)
1999–2004 63 29 (46%) 9 (14.2%) 7 (11.1%) 4 (6.3%) 12 (19%) 2 (3.1%)
2005–2010 41 16 (39%) 3 (7.3%) 6 (14.6%) 5 (12.2%) 11 (25.6%) –
Table 2. Surgical procedures performed in the analyzed periods of time (sub – subtotal, part – partial, tot – total lobectomy) Tabela 2. Rodzaj leczenia operacyjnego u dzieci w analizowanych okresach (sub – subototalna resekcja, part – częściowa resekcja plata, tot – calkowite usunięcie płata)
Years
(Lata) (Typ zabiegu (płat/płat))Procedure (lobe/lobe)
sub/sub sub/– sub/part part/part part/– tot/– tot/tot tot/sub tot/part
1993–1998 21 2 6 2 – 4 4 7 –
N = 46 45.6% 4.3% 13.04% 4.3% 8.7% 8.7% 15.2%
1999–2004 7 – 4 1 – 31 6 9 5
N = 63 11.1% 6.3% 1.6% 49.2% 9.5% 14.3% 7.9%
2005–2010 4 – 2 – 3 14 6 3 9
lobe containing cold nodules was routinely sent for intraoperative pathological assessment (frozen sec-tion). Most children operated in the first 2 periods of the study had preoperative fine needle thyroid biopsy performed in the local hospital either by the radiologist or attending pathologist. In cases of suspicion of malignant disease, unilateral lobec-tomy with intraoperative pathology was an initial operative step. Total thyroidectomy was indicated in children with confirmed malignancy. Unfor-tunately, in 3 of the first 5 patients with thyroid carcinoma, the initial cytology was negative and all had subtotal resection of the thyroid gland. These patients underwent reoperation within two weeks of the primary operative procedure with comple-tion of total thyroidectomy and modified bilateral cervical lymphadenectomy. Papillary carcinoma, follicular carcinoma and medullar carcinoma were finally diagnosed in these cases respectively. Since 1999, all patients in whom fNB revealed suspicious cells or raised suspicion of follicular lesion under-went at least unilateral lobectomy. Such strategy was subsequently transferred for patients with uni-lateral pathology of the thyroid gland, even in cases of benign preoperative cytology. Statistical analy-sis has revealed significant differences between the first and other two periods of the study with regard to subtotal and total procedures (p < 0.05). The differences between the two latter periods were not significant (p = 0.127).
Three patients with subtotal resections were re-admitted for surgical management because of the recurrent nodular goiter. The first patient with multiple bilateral nodular lesions underwent total right and subtotal left lobectomy in 1997.
Recur-rence of nodular disease prompted total left lo-bectomy six years later. The second patient had right total and left partial lobectomy in 2001 due to a large single nodule in each lobe. In 2009 she had the left lobe totally excised because of recur-rence of the disease with multiple nodules within the residual thyroid tissue. The last patient had a single large nodule in the left lobe and multiple smaller nodular lesions within the right lobe and subsequently had a total left lobectomy and partial excision of the right lobe. Pathology revealed fol-licular adenoma and nodular goiter. due to recur-rence of multiple nodules in the right lobe, it was subsequently excised in 2008.
The results of pathological examination of the resected specimens of the thyroid gland are pre-sented in Table 3. They include 3 specimens from the re-operated children as well. Statistical analysis did not reveal any significant trend with regards to incidence of particular pathology throughout of the study period.
Discussion
The limited experience of pediatric surgeons in the treatment of thyroid pathology when com-pared to that of general surgeons is well reflected in the medical literature [4, 5]. Because most pe-diatric patients with thyroid pathology are adoles-cents, they are frequently operated on by general surgeons or endocrine surgeons in medical centers for adults as well. The approach varies from coun-try to councoun-try and depends on the general prin-ciples of the medical care system in a given region.
Table 3. Results of pathology reports in the operated children. NG – nodular goiter, fa – follicular adenoma, G-B – Graves-Basedov, SL – lymphatic thyroiditis, hyperplastic – hyperplastic goiter, Inv – involutive goiter, dysh – dyshormonogenetic goiter, ca – thyroid carcinoma, NL – neurilemmoma
Tabela 3. Wyniki badań patologicznych tarczycy u operowanych dzieci. NG – wole guzkowe, fa – gruczolak pęcherzyko-wy, G-B – choroba Graves-Basedowa, SL – limfatyczne zapalenie tarczycy, hyperplastic – wole hyperplastyczne, inv – wole inwolucyjne, dysh – wole dyshormonogenetyczne, ca – rak tarczycy, ML – neurilemmoma
Years
(Lata) Number (Liczba) (Rozpoznanie)diagnosis
NG fa fa
+NG G-B SL hyper-plastic Inv dysh ca cyst NL
1993– 1998 46 18 10 3 4 2 5 – 1 2 – 1
% 39.1 21.7 6.5 8.7 4.3 10.8 – 2.2 4.3 – 2.1
1999– 2004 63 24 16 4 – 4 6 1 1 4 2 1
% 38.1 25.4 6.3 – 6.3 9.4 1.6 1.6 6.3 3.1 1.6
2005–2010 41 20 5 6 1 – 2 4 1 1 1 –
Moreover, thyroid pathology in children reflects more than that in adult patient environmental etiology. Ionizing radiation, either therapeutic or accidental, has for decades been regarded as the most important carcinogenic factor [1]. Iodine de-ficiency is a well known cause of endemic goiter and in the geographic areas with poor iodine sup-plementation, the prevalence of thyroid diseases is still high. all these above mentioned factors indi-cate that the epidemiological and clinical aspects of the surgical diseases of the thyroid gland in chil-dren may vary not only between various countries but may change with time in the same country as well. Present study seems to provide a very good example of such unique features of pediatric thy-roid pathology. The territory of Lower Silesia was known as an endemic goiter region until the late 80’s. a nationwide schedule of iodine salt supple-mentation was introduced in the 90’s [3]. The authors started their program of surgical manage-ment of children with thyroid disease in 1993. Ini-tially, all patients were operated on by a combined team consisting of a general surgeon and pediatric surgeon. Since 1996, all children have been oper-ated on by the same pediatric surgeon with an in-terest in endocrine surgery. The presented series of patients therefore reflects the personal experience of a single surgeon and gives a unique opportunity to objectively assess the changing trends in thyroid surgery during the last two decades. This is one of the largest series of children with surgical thyroid pathology reported in the literature from a single center. Surgeons from Boston reviewed 175 con-secutive children who underwent thyroid surgery but their study period was 35 years [6]. The cana-dian Pediatric Thyroid Nodule Study Group pub-lished the data collected from 9 centers and dur-ing the 6-year period between 2000 and 2005, one hundred and forty-one children underwent sur-gery for thyroid nodules [7]. astl et al. presented 114 children subjected to thyroid surgery between 1991–2000 in Prague. The average number of pa-tients per year is similar to present authors’ but it must be emphasized that the authors represented various departments aimed principally to treat adult patients [8]. The variability of epidemiologi-cal data renders an objective comparative analysis almost impossible. Reviewing their own study, the authors want to stress that the number of patients with surgical pathology has been consistently de-creasing since around 2002, presently less than 10 per year. This trend cannot be proved statistically yet, but it seems obvious that iodine supplementa-tion has played a major role. The low incidence of thyroid cancer in Lower Silesia deserves a separate comment. firstly the authors did not notice any rise in incidence of thyroid pathology in children
with relation to the chernobyl accident. Secondly, a low number of children with cancer of the thy-roid gland seems surprising low when compared to the similar studies from other pediatric surgi-cal centers. The incidence of cancer among the children subjected to surgical management and reported from various centers worldwide ranged from 8% to 43% [7, 9, 10]. Such a difference might result from a much lower number of children with benign nodules among all patients treated opera-tively in these studies. It may well be that some children are operated on by general surgeons and they are simple lost from the pediatric surgical re-cords by changes to their characteristics. Proku-rat et al. presented the results of a collaboProku-rative retrospective study on thyroid cancer in children treated in Poland between 2000–2005. They were able to collect the data of 107 children aged less than 18 years operated on in 14 pediatric surgical centers [11]. It does not seem therefore that the incidence of thyroid cancer in children in Lower Silesia has been underreported.
extent of thyroid resection and the authors have abandoned bilateral subtotal resection. In children with unilateral pathology, total excision of the af-fected lobe is performed while the contralateral lobe remains intact. In children with bilateral benign nodules, one-side lobectomy with partial excision of the contralateral gland is carried out, unless the extent of pathological changes dictates its subtotal or total resection. children with thyroid carcino-ma are scheduled for total thyroidectomy coupled with lymph node dissection and the authors do not offer gland-sparing procedures in cases of ma-lignancy. an analysis of their own results clearly indicates that there has been a significant decrease in subtotal resections from around 63% in the first period to less than 16% in the other two periods of study. The reverse trend can be clearly seen with regard to unilateral total lobectomy. Unfortunate-ly the surgeons from other centers did not present such a comparative analysis of their own results in various periods of time. Scholz et al., reviewing their 35-year experience, noted that 2/3 of children underwent unilateral lobectomy or local excision and subtotal bilateral lobectomy was performed in barely 6.8% of them. It is worth emphasizing that 10 of 52 children with thyroid cancer underwent completion thyroidectomy after the initial unilat-eral lobectomy [6]. In their material 3 of 7 children with thyroid cancer required early re-surgery. The authors believe that even in cases of false-negative preoperative diagnostic studies it is much safer to perform unilateral reoperation than to risk bilater-al injury to vitbilater-al structures. astl et bilater-al. from Prague report an aggressive surgical approach in children with non-malignant disease. The majority of these patients had total thyroidectomy or hemithyroid-ectomy performed [8]. On the other hand it should be emphasized that more than one third of these patients had Graves-Basedov disease or Hashimo-to’s toxicosis. In their surgical material the authors report a very low incidence of such pathology, which again illustrates well a different therapeutic approach to patients with the same pathology ap-plied in various centers. a similar operative strat-egy was presented by surgeons from denver. The children with thyroid nodules had unilateral resec-tion, while in those with suspicion of malignancy, genetic abnormalities, Graves disease or Hashimo-to’s thyroiditis, total resection was performed [4]. In other clinical studies from the last decade, their authors report that total unilateral or bilateral
resection of the thyroid gland were procedures of choice leaving subtotal resections reserved for selected cases only [7, 8, 12]. conversely, in older papers the number of children undergoing less aggressive resection like nodulectomy, partial or subtotal resections is much higher [13, 14].
The introduction of a more aggressive opera-tive policy by the authors does not seem to be linked to changes in thyroid pathology in their patients. Throughout the study, children with nodular goiter and follicular adenoma prevail. a rising incidence of nodular pathology during the last period is ac-companied by a similar decrease in the number of children with follicular adenoma. Interestingly, the number of patients with follicular adenoma associ-ated with nodular goiter increased two fold in the last years. The incidence of other surgical patholo-gies was uniformly low. It is again a locally specific distribution of surgical thyroid diseases in children as other authors present frequently different data. Some of them put the focus on thyroid cancer in children, only omitting benign diseases. In the ca-nadian collaborative study, children with cancer constituted 43% of patients within the whole group. among those with benign disease, patients with follicular adenoma prevailed with a rate of 68% [7]. The rate of nodular goiter of 16.1% was significantly lower compared to present population of patients. Karazugel et al., in their retrospective study of 137 children, showed a similar prevalence to present authors’ of benign pathology of the thyroid gland of 93.6%, but they did not specify the final histological diagnoses in this subset of patients [10]. Hung et al. presented 71 patients with solitary thyroid nodule and found the highest rate of follicular adenoma followed by carcinoma [15].
Summarizing authors’ near 20-year experience, it should be stressed that the introduction of iodine prophylaxis has proved effective and is reflected in the decreasing number of children with surgical thyroid pathology. This trend refers predominantly to children with follicular adenoma. Secondly, ul-trasound scan and fine-needle biopsy have proved to be diagnostic studies of the highest impact on the choice of a surgical approach with cytology aimed at detecting malignancy. Ultrasound dictates the mode of surgical management in children with benign cytology. Regardless of the extent of thy-roid disease, unilateral lobectomy, either alone or coupled with resection of the contralateral lobe has become a standard surgical procedure in children.
References
[1] Koch C, Sarlis N: The spectrum of thyroid diseases in childhood and its evolution during transition to adulthood: Natural history, diagnosis, differential diagnosis and management. J endocrinol Invest 2001, 24, 659–675.
[3] Wasikowa R, Iwanicka Z, Zak T, Barg E, Basiak A, Bieniasz J, Kostecka L, Kotschy B, Maj A, Noczynska A, Sajewicz E, Wikiera B: Goiter prevalence in children in Lower and Middle Silesia. endokrynol Pol 1993, 44, 259–269.
[4] Wood J, Patrick D, Barham H, Bensard D, Travers S, Bruny J, McIntyre R: Pediatric thyroidectomy; a collab-orative surgical approach. J Pediatr Surg 2011, 46, 823–828.
[5] Skrzypek J, Arendt J, Podwiński A: Surgical treatment of goitre in children. ann acad Med Siles 1987, 14–15.
[6] Scholz S, Smith J, Chaignaud B, Shamberger R, Huang S: Thyroid surgery at children’s Hospital Boston; a 35-year single-institution experience. J Pediatr Surg 2011, 46, 437–442.
[7] The canadian Pediatric Thyroid Nodule Study Group: The canadian Pediatric Thyroid nodule study: an evalua-tion of current management practices. J Pediatr Surg 2008, 43, 826–830.
[8] Astl J, Dvorakova M, Vicek P, Vesely D, Matucha P, Betka J: Thyroid surgery in children and adolescents. Int J Pediatr Otorhinol 2004, 68, 1273–1278.
[9] Luco-Vincente H, Ortiz V, Idizarry H, Camps J, Pagan V: Pediatric thyroid nodules: Management in the era of fine needle aspiration. J Pediatr Surg 1998, 33, 1302–1305.
[10] Karaguzel G, Tanyel C, Buyukpamukcu N, Hicsonomez A: Is there any predictive characteristic for malignancy in thyroid enlargements during childhood? eur J Pediatr Surg 1996, 6, 70–74.
[11] Prokurat A, Chrupek M, Pacholska M, Galazka P, Harasymczuk J: diagnosis and treatment of thyroid cancer in children in the multicenter analysis in Poland for PPGGL. endokrynol Pol 2006 (supl a), 775–781.
[12] Raval M, Browne M, Chin A, Zimmerman D, Angelos P, Reynolds M: Total thyroidectomy for benign disease in the pediatric patient – feasible and safe. J Pediatr Surg 2009, 44, 1529–1533.
[13] Desjardines J, Khan A, Montupet P, Collin P, Lebouf G, Polychronakos C, Simard P, Boivert J, Dube J-L:
Management of thyroid nodules in children: a 20-year experience. J Pediatr Surg 1987, 22, 73739.
[14] Raab S, Silverman J, Elsheikh T, Thomas P, Wakely P: Pediatric thyroid nodules: disease demographics and clinical management as determined by fine needle aspiration biopsy. Pediatrics 1995, 95, 46–49.
[15] Hung W, Anderson K, Chandra R, Kapur S, Patterson K, Randolph J, August G: Solitary thyroid nodules in 71 children and adolescents. J Pediatr Surg 1992, 27, 1407–1409.
Address for correspondence:
Maciej Bagłajdepartment of Pediatric Surgery and Urology Wroclaw Medical University
M. Skłodowskiej-curie 52 50-367 Wrocław
Poland
e-mail: [email protected]
conflict of interest: None declared