SUPPLEMENT ARTICLE
Evaluation and Development of Potentially Better
Practices to Improve Pain Management of Neonates
Paul J. Sharek, MD, MPHa, Richard Powers, MDb, Amy Koehn, NNPc, Kanwaljeet J. S. Anand, MBBS, DPhild
aDivision of General Pediatrics, Department of Pediatrics, Stanford University School of Medicine, Lucile Packard Children’s Hospital, Palo Alto, California;bDepartment of
Neonatology, Good Samaritan Hospital, San Jose, California;cDepartment of Pediatrics, Section of Neonatal/Perinatal Medicine, Riley Children’s Hospital, Indianapolis,
Indiana;dDivision of Critical Care Medicine, Department of Pediatrics, University of Arkansas for Medical Sciences, Arkansas Children’s Hospital, Little Rock, Arkansas
The authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
OBJECTIVE.Despite increased knowledge, improved options, and regulatory man-dates, pain management of neonates remains inadequate, promoted by the inef-fective translation of research data into clinical practice. The Neonatal Intensive Care Quality Improvement Collaborative 2002 was created to provide participating NICUs the tools necessary to translate research, related to prevention and treat-ment of neonatal pain, into practice. The objective for this study was to use proven quality improvement methods to develop a process to improve neonatal pain management collaboratively.
METHODS.Twelve members of the Neonatal Intensive Care Quality Improvement Collaborative 2002 formed an exploratory group to improve neonatal pain man-agement. The exploratory group established group and site-specific goals and outcome measures for this project. Group members crafted a list of potentially better practices on the basis of the available literature, encouraged implementation of the potentially better practices at individual sites, developed a database for sharing information, and measured baseline outcomes.
RESULTS.The goal “improve the assessment and management of infants experiencing pain in the NICU” was established. In addition, each site within the group iden-tified local goals for improvement in neonatal pain management. Data from 7 categories of neonates (N⫽277) were collected within 48 hours of NICU admis-sion to establish baseline data for clinical practices. Ten potentially better practices were developed for prioritized pain conditions, and 61 potentially better practices were newly implemented at the 12 participating sites. Various methods were used for pain assessment at the participating centers. At baseline, heel sticks were used more frequently than peripheral intravenous insertions or venipunctures, with substantial variability in the number of avoidable procedures between centers. Pain was assessed in only 17% of procedures, and analgesic interventions were performed in 19% of the procedures at baseline.
www.pediatrics.org/cgi/doi/10.1542/ peds.2006-0913D
doi:10.1542/peds.2006-0913D
Key Words
quality, collaborative, pain management, best practice, NIC/Q 2002
Abbreviations
IFG—I Feel Good
NIC/Q 2002—Neonatal Intensive Care Quality Collaborative 2002 VON—Vermont Oxford Network PBP—potentially better practice PIV—peripheral intravenous ETT— endotracheal tube
Accepted for publication Jul 18, 2006
Address correspondence to Paul J. Sharek, MD, MPH, Department of Pediatrics, 700 Welch Rd, #227, Palo Alto, CA 94304. E-mail: psharek@ lpch.org
CONCLUSIONS.Collaborative use of quality improvement methods resulted in the creation of self-directed, effi-cient, and effective processes to improve neonatal pain management. Group establishment of potentially better practices, collective and site-specific goals, and extensive baseline data resulted in accelerated implementation of clinical practices that would not likely occur outside a collaborative setting.
N
EWBORNS IN THE NICU routinely experience painfrom both acute invasive procedures and surgical procedures.1–3 Evidence suggests that pain, when
unre-lieved, severe, or prolonged, may hamper resolution of underlying disease processes, delay surgical recovery, and result in higher health care costs.4The physiologic
responses to pain include alterations in gastrointestinal and pulmonary function as well as impairment of the immune response.5The neonate exhibits a greater
hor-monal, metabolic, and cardiovascular response to surgi-cal operations when compared with older children. Pre-term and Pre-term neonates experience pain and its consequences much differently than older children and adults and therefore require study and interventions that are tailored to their specific needs.6,7
Despite the knowledge that infants undergo frequent painful procedures, evidence suggests that pain is under-treated in this population.8Several reasons for this
un-dertreatment exist, including a lack of appropriate pain assessment tools, limited therapeutic options, and a lack of knowledge among health care professionals regarding neonatal pain perception and management.9,10
Manage-ment of pain in the newborn also is hampered by a lack of awareness that the neonate is capable of experiencing pain and exaggerated concerns about the adverse effects of analgesic use.7–11
In addition, our internal collaborative survey of clin-ical practices suggests that many evidence-based inter-ventions have not yet been applied effectively in NICUs. A recent report from the Institute of Medicine12noted a
large chasm in many areas of medicine between what we know and what we do. This seems to be true of efforts to improve neonatal pain management as well.
Recent evidence-based guidelines and professional practice standards have described approaches to the pre-vention and management of pain in the newborn.7,13The
“I Feel Good” (IFG) exploratory group, consisting of 12 sites, convened to work collaboratively to improve neo-natal pain management. This exploratory group was a subset of the Neonatal Intensive Care Quality Collabo-rative 2002 (NIC/Q 2002), a 3-year quality improvement collaborative that was overseen by the Vermont Oxford Network (VON).
With the goal of collaboratively improving the quality of pain management in each site’s NICU, IFG partici-pants evaluated, edited, and implemented previously
identified evidence-based potentially better practices (PBPs) related to neonatal pain management. This strat-egy differed from the NIC/Q 2000 collaborative, which required the exploratory groups to create their own list of PBPs on the basis of extensive literature review.14This
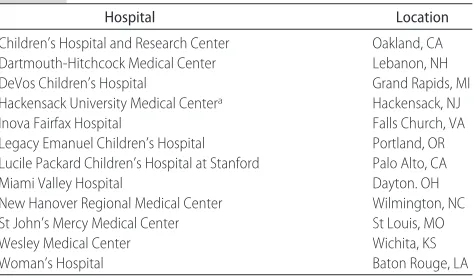
article reviews the strategies that were undertaken by the 12 institutions (Table 1) to improve neonatal pain management, using previously defined PBPs with the guidance of clinical experts.
METHODS
Structure of the Neonatal Pain Management Group
At the first meeting of the neonatal pain management exploratory group (IFG group), an experienced facilita-tor and a content expert were assigned by the VON, and a group leader was chosen. The facilitator advised the group on data-collection tools, measurement strategies, data analysis, and group processes. The content expert provided a list of evidence-based practices, advised the group on the strength of published evidence, and pro-vided real-time expertise for issues related to neonatal pain management. The group leader facilitated discus-sions on the group goals, delegated individual site re-sponsibilities, established time lines and accountability for assigned tasks, led conference call discussions, and corresponded with the leaders of the NIC/Q 2002 project. Each site in the group selected a representative to coordinate individual site efforts.
Establishment of Goals and Outcome Measures
The initial task of the IFG group was to establish primary and secondary goals for the group. Outcome measures were selected to assess the effectiveness of interventions. The primary goal identified was to “improve pain assess-ment and manageassess-ment of infants experiencing pain in the NICU.” Five secondary goals were established (Table 2), with 8 outcome measures and 2 process measures selected (Table 3).
Creation of PBP List
A content expert joined the IFG group and provided a list of evidence-based practices for group review.7Group
TABLE 1 Members of the IFG Exploratory Group
Hospital Location
Children’s Hospital and Research Center Oakland, CA Dartmouth-Hitchcock Medical Center Lebanon, NH DeVos Children’s Hospital Grand Rapids, MI Hackensack University Medical Centera Hackensack, NJ
Inova Fairfax Hospital Falls Church, VA Legacy Emanuel Children’s Hospital Portland, OR Lucile Packard Children’s Hospital at Stanford Palo Alto, CA
Miami Valley Hospital Dayton. OH
New Hanover Regional Medical Center Wilmington, NC St John’s Mercy Medical Center St Louis, MO
Wesley Medical Center Wichita, KS
Woman’s Hospital Baton Rouge, LA
members reviewed these PBPs (Table 4), critically eval-uated the supporting evidence, and determined the rel-evance of each PBP to the defined IFG goals.
Once the final PBP list was created, each PBP was assigned to a subgroup for extensive review and refine-ment. On completion of this process, a PBP tool kit (including a description of the PBP, evidence supporting this PBP, and suggestions for implementation strategies) was created to facilitate implementation. Each partici-pating site then was asked to implement as many of the PBPs as possible, subject to site characteristics and needs.
Database Creation
To determine each site’s pain management practices at baseline, multiple data-collection tools were created (Appendices 1 and 2). Specific data were collected on the following: (1) pain measurement tools used and (2) pain management policies defined. In addition, each site was required to collect data on 5 patients in each of the following categories:
1. ⬍29.0 weeks’ gestational age and on ventilatory sup-port
2. ⬍29.0 weeks’ gestational age and not on ventilatory support
3. From 29.0 to 36.6 weeks’ gestational age and on ventilatory support
4. From 29.0 to 36.6 weeks’ gestational age and not on ventilatory support
5. Term (ⱖ37.0 weeks’ gestational age) and on ventila-tory support
6. Term (ⱖ37.0 weeks’ gestation age) and not on ven-tilatory support
7. All gestational ages in the postoperative period
These data were collected at each site via retrospective chart review for patients who were admitted to the NICU between January 1 and April 15, 2002.
RESULTS
PBPs
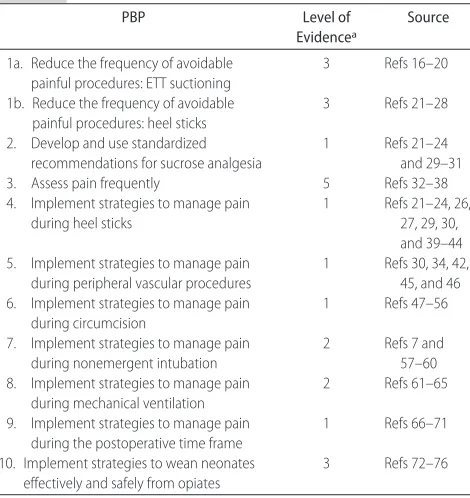
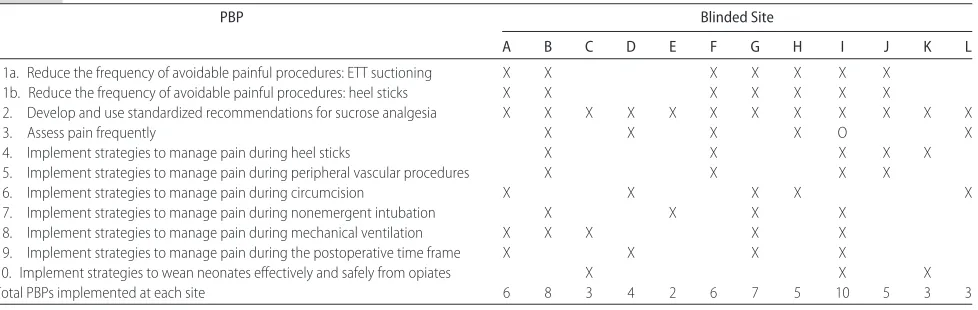
Ten PBPs to improve pain management for infants in the NICU were identified and approved. Following the ter-minology of the NIC/Q collaboratives, these were la-beled as “potentially” better practices because they rep-resented clinical research that may or may not translate into better outcomes if implemented at an individual site. All 10 PBPs (Table 4) were based on published evidence that was available at that time (January 2002). A total of 62 PBPs were implemented by members of the IFG group before (1 PBP) or during (61 PBPs) the NIC/Q 2002 collaborative (Table 5).
TABLE 2 Goals of the IFG Group
Primary goal
Improve pain assessment and management of infants experiencing pain in the NICU
Secondary goals
Reduce the frequency of avoidable painful procedures
Develop and implement a standardized, evidence-based policy regarding sucrose administration for analgesia
Improve the frequency of pain assessment in newborns
Develop recommendations for pain management for specific painful procedures, including heel sticks, peripheral vascular procedures, circumcision, nonemergent intubations, assisted ventilation, and the postoperative period
Develop an evidence-based weaning protocol for opiates
TABLE 3 Outcome and Process Measures for the IFG Group
Outcome measures
Mean number of painful procedures per patient in first 48 h of life Percentage of patients with at least 1 pain assessment in first 48 h of life Mean number of specific procedures in first 48 h of life: heel sticks, PIV
insertions, venipuncture, and ETT suctioning
Percentage of patients with at least 1 occurrence of heel stick, PIV insertion, venipuncture, or ETT suctioning in first 48 h of life
Mean pain scores documented in patients in first 48 h of life
Percentage of patients who received at least 1 pain management intervention during heel sticks, PIV insertions, venipunctures, umbilical arterial catheterizations, nasogastric tube placements, and ETT suctioning Percentage of all defined procedures in which pain scores were documented Percentage of all defined procedures that were treated with a pain
management intervention Process measures
Pain scale(s) used
Presence of protocols for patient groups and specific procedures
TABLE 4 PBPs and Level of Evidence: IFG Group
PBP Level of
Evidencea
Source
1a. Reduce the frequency of avoidable painful procedures: ETT suctioning
3 Refs 16–20
1b. Reduce the frequency of avoidable painful procedures: heel sticks
3 Refs 21–28
2. Develop and use standardized recommendations for sucrose analgesia
1 Refs 21–24 and 29–31 3. Assess pain frequently 5 Refs 32–38 4. Implement strategies to manage pain
during heel sticks
1 Refs 21–24, 26, 27, 29, 30, and 39–44 5. Implement strategies to manage pain
during peripheral vascular procedures
1 Refs 30, 34, 42, 45, and 46 6. Implement strategies to manage pain
during circumcision
1 Refs 47–56
7. Implement strategies to manage pain during nonemergent intubation
2 Refs 7 and 57–60 8. Implement strategies to manage pain
during mechanical ventilation
2 Refs 61–65
9. Implement strategies to manage pain during the postoperative time frame
1 Refs 66–71
10. Implement strategies to wean neonates effectively and safely from opiates
3 Refs 72–76
aMuir Gray Classification System77: level 1, strong evidence from at least 1 systematic review of
multiple well-designed, randomized, controlled trials; level 2, strong evidence from at least 1 properly randomized, controlled trial of appropriate size; level 3, evidence from well-designed trials without randomization, including single group, pre–post, cohort, time series, or matched case controls; level 4, evidence from well-designed nonexperimental studies preferably from
Resource Kit
A resource kit (“tool kit”) was developed by the IFG group and included the 10 PBPs and 20 descriptions of implementation efforts, including common barriers to implementation and strategies to overcome these barri-ers. Four appendices (Suggested Dosing and Administra-tion of Analgesics; Pharmacokinetic and Pharmacody-namic Considerations When Determining Optimal Opiate Dosing for the Neonatal Population; Potential Adverse Effects of Opiates; and A Sample Flowchart for the Administration of Analgesics in Mechanically Venti-lated Infants) and implementation aids such as audit tools, slide presentations, literature references, and site-specific data related to implementation efforts also were included in the IFG tool kit. This resource kit also was distributed to NIC/Q 2002 sites that were not involved in the IFG group to facilitate the implementation of PBPs that were appropriate for non-IFG sites.
Database Creation
Members of the IFG group created a preintervention database to document clinical practices at baseline, which consisted of (1) pain assessment scales that were used and procedure specific guidelines/policies that were available for 11 of the IFG sites (1 site joined after baseline data collection) and (2) invasive procedures that were performed and pain assessment scores on 277 neonatal patients from the 11 initial IFG group members.
The participating sites used various assessment scales (Neonatal Infant Pain Scale; CRIES; Premature Infant Pain Profile; Face, Legs, Arms, Cry, Consolability Pain Scale; and Distress Scale for Ventilated Newborn Infant) to document neonatal pain and distress in the NICU. Invasive procedures were documented during the first 48 hours after NICU admission. From the invasive (skin-breaking) procedures documented, heel sticks for capil-lary blood sampling were used more frequently (on av-erage 2.5–5.3 times per patient among the 7 patient categories studied) than peripheral intravenous (PIV) insertion (on average 0.7–1.9 times per patient among
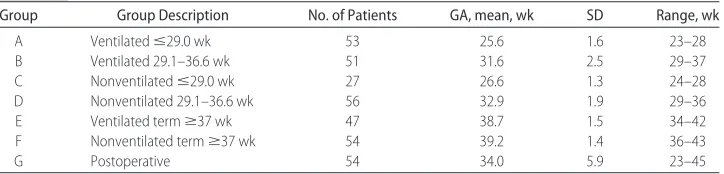
the 7 patient categories) or venipuncture (average 0.3– 1.9 times per patient among the 7 patient categories). The highest frequencies for all 3 invasive procedures occurred among nonventilated infants who were ⬎29 weeks’ gestation (on average, 5.3 heel sticks, 1.9 PIV insertions, and 1.9 venipunctures per patient) and non-ventilated term infants (on average, 4.7 heel sticks, 1.5 PIV insertions, and 1.1 venipunctures per patient) dur-ing the first 48 hours after NICU admission. Greater proportions of the patients in these groups were sub-jected to heel sticks (96% of nonventilated infants who were⬎29 weeks, 91% of nonventilated term neonates), PIV insertion (83% and 86%, respectively), or venipunc-ture (48% and 56%, respectively) as compared with the other patient categories (heel sticks: 37%–70%; PIV in-sertion: 42%– 68%; venipuncture: 16%–24%). Endotra-cheal tube (ETT) suctioning was performed on 77% to 100% of ventilated infants on average 8.5 to 9.3 times per patient during the first 48 hours after NICU admission. Participating sites identified a marked degree of vari-ability in the number of avoidable invasive procedures between centers during the first 48 hours of life (1.0 –9.5 total heel sticks per patient, 0.25–1.9 PIV insertions per patient, 0.14 –1.57 venipunctures per patient, 3.9 –12.4 ETT suctionings per ventilated patient). Relatively few patients received pharmacologic or nonpharmacologic interventions for pain management during these proce-dures (heel sticks: 16%; PIV insertions: 16%; venipunc-tures: 6%; nasogastric tube insertions: 25%; ETT place-ments: 18%). Pain was assessed in 17% of these procedures (133 of 774), and analgesic interventions were provided for 19% of these procedures (148 of 774). Demographic data for the 277 patients are shown in Table 6.
DISCUSSION
The IFG group moved from the creation of a group structure, to the establishment of goals and measures, and finally to the identification of 10 PBPs with imple-mentation of several of these PBPs at each site. The IFG
TABLE 5 PBPs Implemented at Each Participating IFG Site
PBP Blinded Site
A B C D E F G H I J K L
1a. Reduce the frequency of avoidable painful procedures: ETT suctioning X X X X X X X 1b. Reduce the frequency of avoidable painful procedures: heel sticks X X X X X X X
2. Develop and use standardized recommendations for sucrose analgesia X X X X X X X X X X X X
3. Assess pain frequently X X X X O X
4. Implement strategies to manage pain during heel sticks X X X X X
5. Implement strategies to manage pain during peripheral vascular procedures X X X X
6. Implement strategies to manage pain during circumcision X X X X X
7. Implement strategies to manage pain during nonemergent intubation X X X X 8. Implement strategies to manage pain during mechanical ventilation X X X X X 9. Implement strategies to manage pain during the postoperative time frame X X X X
10. Implement strategies to wean neonates effectively and safely from opiates X X X
Total PBPs implemented at each site 6 8 3 4 2 6 7 5 10 5 3 3
group simultaneously developed a database to describe the status of pain assessment and management at base-line to identify and prioritize clinical practice areas that were particularly appropriate for improvement efforts. A secondary purpose was to provide the foundation for subsequent evaluation of clinical outcomes after imple-mentation of the PBPs. Group members acknowledged that these sequential accomplishments could not have occurred by the quality improvement efforts at individ-ual sites alone; rather, they occurred as a direct result of collaboration. Published data also suggest a relatively lower effectiveness of changes in neonatal pain manage-ment at individual institutions.3,8
There are several advantages to collaboration when working to improve quality of patient care. First, the work can be divided among the group members, maxi-mizing the use of available resources while minimaxi-mizing duplication of efforts. Second, the collective enthusiasm that is generated by collaborative work often is difficult to generate and maintain when working at only 1 site. Third, a culture of mutual accountability accelerates the completion of assigned tasks. Fourth, the group provides a rich environment for learning. Site-specific strengths inevitably are discovered and discussed. Topics of mutual interest promote discussion during conference calls and meetings. Finally, data can be shared, creating larger databases for comparisons and combined analyses with larger numbers of patients and the ability to stratify and identify significant trends.
Our experience revealed several essential ingredients for creating an effective collaborative group. Clear, evi-dence-based, and measurable goals are critical to estab-lishing and maintaining an effective exploratory group. An experienced and dedicated leader also is critical, act-ing as a catalyst to move the process forward and main-tain orientation to the assigned tasks. Each participating site must be willing to dedicate time and resources to the project and be willing to forego concerns of confidenti-ality to provide data and candidly discuss care practices. It is important to have frequent contact within the group, using such strategies as conference calls, listservs, and face-to-face meetings. Logical and aggressive time-lines must be established with deadtime-lines for each com-ponent of the process, and a sense of accountability must be instilled into each site to maintain equitable
distribu-tion of work. This accountability stems from the need for a significant return on investment, the peer pressure that is instilled from frequent contact among members, clearly defined expectations, and an established time-line.
Changing practices in large institutions requires en-ergy, flexibility, and risk and rarely occurs without cred-ible support from the literature. Thus, the initial litera-ture review, completed by our content expert and reviewed internally by specific PBP-assigned subgroups, was critical to this process. This literature review and endorsement strategy allowed a comprehensive review of the published data related to neonatal pain manage-ment.
Another advantage of the exploratory group format was that each subgroup chose a single area of expertise, thereby increasing the group’s knowledge base while minimizing the duplication of efforts. This strategy added to the efficiency of the process because clinical practices that lacked supportive data were not pursued. The subgroups’ expertise allowed each recommended PBP to be discussed relative to the strength of the study design and validity of the data. An example of the value of this strategy is reflected in our selection of sucrose use as a PBP for pain prevention in the NICU population. The presence of a single yet influential study suggesting that sucrose use in infants who are⬍31 weeks’ gestation may “put infants at risk for poorer neurobehavioral and physiologic outcomes”15 was evaluated extensively by
the Sucrose subgroup. Intensive review of the sucrose literature, as well as detailed discussion with the lead author of the above mentioned study (C. Celeste John-son, DEd, RN) regarding her data and her study design, reassured the Sucrose subgroup that the benefits out-weighed the risks regarding this recommendation. Fi-nally, the IFG group endorsement of evidence-based PBPs provided the necessary “buy-in” to recommend implementation of these PBPs at their own sites as well as non-IFG sites.
The final component of the IFG group’s project was the patient database. This database eventually will prove to be the most compelling argument for aggressive im-plementation of PBPs. Change concepts can be suggested on the basis of the literature and anecdotal evidence; however, positive results must be achieved, maintained,
TABLE 6 Demographic Data of Baseline Population
Group Group Description No. of Patients GA, mean, wk SD Range, wk
A Ventilatedⱕ29.0 wk 53 25.6 1.6 23–28
B Ventilated 29.1–36.6 wk 51 31.6 2.5 29–37
C Nonventilatedⱕ29.0 wk 27 26.6 1.3 24–28
D Nonventilated 29.1–36.6 wk 56 32.9 1.9 29–36
E Ventilated termⱖ37 wk 47 38.7 1.5 34–42
F Nonventilated termⱖ37 wk 54 39.2 1.4 36–43
G Postoperative 54 34.0 5.9 23–45
and demonstrated for changes in practice to become ingrained and sustained. Without the ability to demon-strate measurable improvement, clinical improvement efforts eventually would be abandoned. Another advan-tage of the database is the ability to monitor and stratify outcomes on the basis of known risk factors such as birth weight, gender, ethnicity, or site of care.
CONCLUSIONS
Collaborative use of quality improvement methods re-sulted in the creation of logical, efficient, and effective processes to improve neonatal pain management. Group identification and endorsement of PBPs and collabora-tive efforts to implement these PBPs resulted in acceler-ated implementation that would be unlikely to occur outside a collaborative setting. Data analysis is under way to determine the effect of this accelerated PBP im-plementation on the primary and secondary outcomes defined.
ACKNOWLEDGMENTS
We thank Jim Handyside, the focus group facilitator, for excellent leadership skills. We also thank the staff at each of the 12 sites for dedication to this study and to improving the quality of care that is provided at their respective institutions.
REFERENCES
1. Barker DP, Rutter N. Exposure to invasive procedures in neo-natal intensive care unit admissions.Arch Dis Child Fetal Neo-natal Ed.1995;72:F47–F48
2. Johnston CC, Collinge JM, Henderson SJ, Anand KJS. A cross-sectional survey of pain and pharmacological analgesia in Ca-nadian neonatal intensive care units. Clin J Pain. 1997;13: 308 –312
3. Porter FL, Anand KJS. Epidemiology of pain in neonates.Res Clin Forums.1998;20:9 –18
4. Acute pain management in infants, children, and adolescents: operative and medical procedures. Agency for Health Care Policy and Research.Clin Pract Guide Quick Ref Guide Clin.1992; (1B):1–22
5. Anand KJS. Clinical importance of pain and stress in preterm newborn infants.Biol Neonate.1998;73:1–9
6. Anand KJS, Brown MJ, Causon RC, Christofides ND, Bloom SR, Aynsley-Green A. Can the human neonate mount an endocrine and metabolic response to surgery?J Pediatr Surg.
1985;20:41– 48
7. Anand KJS. International Evidence-Based Group for Neonatal Pain. Consensus statement for the prevention and manage-ment of pain in the newborn.Arch Pediatr Adolesc Med.2001; 155:173–180
8. Simons SH, van Dijk M, Anand KS, Roofthooft D, van Lingen RA, Tibboel D. Do we still hurt newborn babies? A prospective study of procedural pain and analgesia in neonates.Arch Pediatr Adolesc Med.2003;157:1058 –1064
9. Borakas L. Factors affecting nurses’ decisions to medicate pe-diatric patients after surgery.Heart Lung.1985;4:373–379 10. Purcell-Jones G, Dormon F, Sumner E. Paediatric
anaesthe-tists’ perceptions of neonatal and infant pain.Pain.1988;33: 181–187
11. Jacob E, Puntillo KA. Pain in hospitalized children: pediatric nurses’ beliefs and practices.J Pediatr Nurs.1999;14:379 –391 12. Institute of Medicine.Crossing the Quality Chasm: A New Health
System for the 21st Century. Washington, DC: Institute of Medicine; 2001
13. American Academy of Pediatrics and Canadian Paediatric So-ciety. Prevention and management of pain and stress in the newborn.Pediatrics.2000;105:454 – 461
14. Sharek PJ, Baker R, Litman F, et al. Evaluation and develop-ment of potentially better practices to prevent chronic lung disease and reduce lung injury in neonates. Pediatrics.2003; 111(4). Available at: www.pediatrics.org/cgi/content/full/111/ 4/SE1/e426
15. Johnston CC, Filion F, Snider L, et al. Routine sucrose analge-sia during the first week of life in neonates younger than 31 weeks’ postconceptional age.Pediatrics.2002;110:523–528 16. Durand M, Sangha B, Cabal LA, Hoppenbrouwers T, Hodgman
JE. Cardiopulmonary and intracranial pressure changes related to endotracheal suctioning in preterm infants.Crit Care Med.
1989;17:506 –510
17. Greisen G, Frederiksen PS, Hertel J, Christensen NJ. Catechol-amine response to chest physiotherapy and endotracheal suc-tioning in preterm infants. Acta Paediatr Scand. 1985;74: 525–529
18. Ninan A, O’Donnell M, Hamilton K, Tan L, Sankaran K. Phys-iologic changes induced by endotracheal instillation and suc-tioning in critically ill preterm infants with and without seda-tion.Am J Perinatol.1986;3:94 –97
19. Perlman JM, Volpe JJ. Suctioning in the preterm infant: effects on cerebral blood flow velocity, intracranial pressure, and ar-terial blood pressure.Pediatrics.1983;72:329 –334
20. Skov L, Ryding J, Pryds O, Greisen G. Changes in cerebral oxygenation and cerebral blood volume during endotracheal suctioning in ventilated neonates. Acta Paediatr. 1992;81: 389 –393
21. Larsson BA, Tannfeldt G, Lagercrantz H, Olsson GL. Alleviation of the pain of venipuncture in neonates.Acta Paediatr.1998; 87:774 –779
22. Larsson BA, Tannfeldt G, Lagercrantz H, Olsson GL. Venipunc-ture is more effective and less painful than heel lancing for blood tests in neonates.Pediatrics.1998;101:882– 886 23. Shah V, Ohlsson A. Venipuncture versus heel lance for blood
sampling in term neonates. Cochrane Database Syst Rev.2000: CD001452
24. Shah VS, Taddio A, Bennett S, Speidel BD. Neonatal pain response to heel stick vs venipuncture for routine blood sam-pling.Arch Dis Child Fetal Neonatal Ed.1997;77:F143–F144 25. Acharya AB, Bustani PC, Phillips JD, Taub NA, Beattie RM.
Randomised controlled trial of eutectic mixture of local anaes-thetics cream for venipuncture in healthy preterm infants.Arch Dis Child Fetal Neonatal Ed.1998;78:F138 –F142
26. Larsson BA, Jylli L, Lagercrantz H, Olsson GL. Does a local anaesthetic cream (EMLA) alleviate pain from heel-lancing in neonates?Acta Anaesthesiol Scand.1995;39:1028 –1031 27. McIntosh N, van Veen L, Brameyer H. Alleviation of the pain
of heel prick in preterm infants.Arch Dis Child Fetal Neonatal Ed.
1994;70:F177–F181
28. Stevens B, Johnston C, Taddio A, et al. Management of pain from heel lance with lidocaine-prilocaine (EMLA) cream: is it safe and efficacious in preterm infants? J Dev Behav Pediatr.
1999;20:216 –221
29. Stevens B, Ohlsson A. Sucrose for analgesia in newborn infants undergoing pain procedures.Cochrane Database Syst Rev.2000; (2):CD001069
31. Larsson BA. Strategies to reduce procedural pain in the new-born.Res Clin Forums.1998;20:63–71
32. Franck LS, Boyce WT, Gregory GA, Jemerin J, Levine J, Mias-kowski C. Plasma norepinephrine levels, vagal tone index, and flexor reflex threshold in premature neonates receiving intra-venous morphine during the postoperative period: a pilot study.Clin J Pain.2000;16:95–104
33. Buttner W, Finke W. Analysis of behavioural and physiological parameters for the assessment of postoperative analgesic de-mand in newborns, infants and young children: a comprehen-sive report on seven consecutive studies. Paediatr Anaesth.
2000;10:303–318
34. van Dijk M, de Boer JB, Koot HM, Tibboel D, Passchier J, Duivenvoorden HJ. The reliability and validity of the COM-FORT scale as a postoperative pain instrument in 0 to 3-year-old infants.Pain.2000;84:367–377
35. Stevens B, Johnston C, Petryshen P, Taddio A. Premature Infant Pain Profile: development and initial validation.Clin J Pain.1996;12:13–22
36. Grunau RE, Oberlander TF, Holsti L, Whitfield MF. Bedside application of the Neonatal Facial Coding System in pain as-sessment of premature neonates.Pain.1998;76:277–286 37. Lawrence J, Alcock D, McGrath P, Kay J, MacMurray SB,
Dulberg C. The development of a tool to assess neonatal pain.
Neonatal Netw.1993;12:59 – 66
38. Krechel SW, Bildner J. CRIES: a new neonatal postoperative pain measurement score—initial testing of validity and reliabil-ity.Pediatr Anesth.1995;5:53– 61
39. Bucher HU, Moser T, von Siebenthal K, Keel M, Wolf M, Duc G. Sucrose reduces pain reaction to heel lancing in preterm infants: a placebo-controlled, randomized and masked study.
Pediatr Res.1995;38:332–335
40. Haouari N, Wood C, Griffiths G, Levene M. The analgesic effect of sucrose in full term infants: a randomized controlled trial.
BMJ.1995;310:1498 –1500
41. Johnston CC, Stremler R, Stevens R, Horton L. Effectiveness of oral sucrose and simulated rocking on pain response in pre-term neonates.Pain.1997;72:193–199
42. Corff KE, Seideman R, Venkataraman PS, Lutes L, Yates B. Facilitated tucking: a nonpharmacologic comfort measure for pain in preterm neonates.J Obstet Gynecol Neonatal Nurs.1995; 24:143–147
43. Harpin VA, Rutter N. Making heel pricks less painful.Arch Dis Child.1983;58:226 –228
44. Shah V, Taddio A, Ohlsson A. Randomised controlled trial of paracetamol for heel prick pain in neonates.Arch Dis Child Fetal Neonatal Ed.1998;79:F209 –F211
45. Eichenfield L, Funk A, Fallon-Friedlander S, Cunningham B. A clinical study to evaluate the efficacy of ELA-Max (4% liposo-mal lidocaine) as compared with eutectic mixture of local anesthetics cream for pain reduction of venipuncture in chil-dren.Pediatrics.2002;109:1093–1099
46. Cordero L, Gardner DK, O’Shaughnessy R. Analgesia versus sedation during Broviac catheter placement. Am J Perinatol.
1991;8:284 –287
47. Benini F, Johnston CC, Faucher D, Aranda JV. Topical anes-thesia during circumcision in newborn infants [published cor-rection appears in JAMA. 1994;271:274]. JAMA. 1993;270: 850 – 853
48. Russell CT, Chaseling J. Topical anesthesia in neonatal circumcision: a study of 208 consecutive cases.Aust Fam Phy-sician.1996;(suppl 1):S30 –S34
49. Taddio A, Stevens B, Craig K, et al. Efficacy and safety of lidocaine-prilocaine cream for pain during circumcision.N Engl J Med.1997;336:1197–1201
50. Taddio A, Ohlsson K, Ohlsson A. Lidocaine-prilocaine cream for analgesia during circumcision in newborn boys. Cochrane Database Syst Rev.2000;(2):CD000496
51. Taddio A, Ohlsson A, Einarson TR, Stevens B, Koren G. A systematic review of lidocaine-prilocaine cream (EMLA) in the treatment of acute pain in neonates. Pediatrics.1998;101(3). Available at: www.pediatrics.org/cgi/content/full/101/2/e1 52. Lander J, Brady-Fryer B, Metcalfe JB, Nazarali S, Muttitt S.
Comparison of ring block, dorsal penile nerve block, and top-ical anesthesia for neonatal circumcision: a randomized con-trolled trial.JAMA.1997;278:2157–2162
53. Mohan CG, Risucci DA, Casimir M, Gulrajani-LaCorte M. Comparison of analgesics in ameliorating the pain of circum-cision.J Perinatol.1998;18:13–19
54. Holve RL, Bromberger PJ, Groveman HD, Klauber MR, Dixon SD, Snyder JM. Regional anesthesia during newborn circum-cision. Effect on infant pain response. Clin Pediatr. 1983;22: 813– 818
55. Kurtis PS, DeSilva HN, Bernstein BA, Malakh L, Schechter NL. A comparison of the Mogen and Gomco clamps in combination with dorsal penile nerve block in minimizing the pain of neo-natal circumcision. Pediatrics. 1999;103(2). Available at: www.pediatrics.org/cgi/content/full/103/2/e23
56. Taddio A, Pollock N, Gilbert-MacLeod C, Ohlsson K, Koren G. Combined analgesia and local anesthesia to minimize pain during circumcision. Arch Pediatr Adolesc Med. 2000;154: 620 – 623
57. Cook-Sather SD, Tulloch HV, Cnaan A, et al. A comparison of awake versus paralyzed tracheal intubation for infants with pyloric stenosis.Anesth Analg.1998;86:945–951
58. Millar C, Bissonnette B. Awake intubation increases intracra-nial pressure without affecting cerebral blood flow velocity in infants.Can J Anaesth.1994;41:281–287
59. Pokela ML, Koivisto M. Physiological changes, plasma beta-endorphin and cortisol responses to tracheal intubation in neonates.Acta Paediatr.1994;83:151–156
60. Pokela ML. Pain relief can reduce hypoxemia in distressed neonates during routine treatment procedures.Pediatrics.1994; 93:379 –383
61. Anand KJS, Barton BA, McIntosh N, et al. Analgesia and sedation in preterm neonates who require ventilatory support. results from the NOPAIN trial. Neonatal Outcome and Pro-longed Analgesia in Neonates.Arch Pediatr Adolesc Med.1999; 153:331–338
62. Sabatino G, Quartulli L, Di Fabio S, Ramenghi LA. Hemody-namic effects of intravenous morphine infusion in ventilated preterm babies.Early Hum Dev.1997;47:263–270
63. Quinn MW, Wild J, Dean HG, et al. Randomised double-blind controlled trial of effect of morphine on catecholamine con-centrations in ventilated pre-term babies. Lancet. 1993;342: 324 –327
64. Saarenmaa E, Huttunen P, Leppaluoto J, Meretoja O, Fellman V. Advantages of fentanyl over morphine in analgesia for ventilated newborn infants after birth: a randomized trial.J Pe-diatr.1999;134:144 –150
65. Orsini AJ, Leef KH, Costarino A, Dettorre MD, Stefano JL. Routine use of fentanyl infusions for pain and stress reduction in infants with respiratory distress syndrome.J Pediatr.1996; 129:140 –145
66. Farrington EA, McGuinness GA, Johnson GF, Erenberg A, Leff RD. Continuous intravenous morphine infusion in postopera-tive newborn infants.Am J Perinatol.1993;10:84 – 87 67. Vaughn PR, Townsend SF, Thilo EH, McKenzie S, Morewland
to bolus dosing in neonates after surgery.J Pediatr Surg.1996; 31:1616 –1623
68. Menon G, Anand KJS, McIntosh N. Practical approach to an-algesia and sedation in the neonatal intensive care unit.Semin Perinatol.1998;22:417– 424
69. Campbell NN, Reynolds GJ, Perkins G. Postoperative analgesia in neonates: an Australia-wide survey.Anaesth Intensive Care.
1989;17:487– 491
70. Goldstein RF, Brazy JE. Narcotic sedation stabilizes arterial blood pressure fluctuations in sick premature infants.J Perina-tol.1991;11:365–371
71. van Lingen RA, Deinum JT, Quak JM, et al. Pharmacokinetics and metabolism of rectally administered paracetamol in pre-term neonates. Arch Dis Child Fetal Neonatal Ed. 1999;80: F59 –F63
72. Franck LS, Vilardi J, Durand D, Powers R. Opioid withdrawal in neonates after continuous infusions of morphine or fentanyl
during extracorporeal membrane oxygenation.Am J Crit Care.
1998;7:364 –369
73. Katz R, Kelly HW, Hsi A. Prospective study on the occurrence of withdrawal in critically ill children who receive fentanyl by continuous infusion.Crit Care Med.1994;22:763–767 74. Tobias JD. Tolerance, withdrawal, and physical dependency
after long-term sedation and analgesia of children in the pedi-atric intensive care unit.Crit Care Med.2000;28:2122–2132 75. Anand KJS, Suresh S. Opioid tolerance in neonates: a
state-of-the-art review.Paediatr Anaesth.2001;11:511–521
76. Arnold JH, Truog RD, Orav EJ, Scavone JM, Hershenson MB. Tolerance and dependence in neonates sedated with fentanyl during extracorporeal membrane oxygenation.Anesthesiology.
1990;73:1136 –1140
77. Muir Gray JA.Evidence Based Health Care. How to Make Health Policy and Management Decisions. Edinburgh, Scotland: Churchill Livingstone; 1997:46 –53
APPENDIX 1: DATA-COLLECTION TOOLS FOR DESCRIBING PAIN MANAGEMENT PRACTICES USED BY SITES IN THE IFG GROUP
I. Pain Scale Assessment Which scale(s) do you use? Why did you choose this scale?
Since using this scale what advantages have you observed? Since using this scale what disadvantages have you observed?
II. Guidelines for Pain Scale Use: Indicate in the columns below your center’s protocol for pain scale assessment in the different patient scenarios
APPENDIX 2: DATA-COLLECTION TOOLS OF THE IFG GROUP
Patient Group A: Ventilated Infant⬍29.0 Weeks’ Gestation Center Name:
Instructions: Review at least 5 (1–5) patients during their first 48 h in your NICU. Indicate the total number of pain assessments and the different number of listed procedures the patient experienced during the 48-h period. Use this data sheet for all patients in this category.
Individual Patient Data Sheet for Procedural Interventions Center: Pain Scale Used:
Patient Group:㛭㛭 Patient #㛭㛭 Gest. Age:㛭㛭 Diagnosis:
DOI: 10.1542/peds.2006-0913D
2006;118;S78
Pediatrics
Paul J. Sharek, Richard Powers, Amy Koehn and Kanwaljeet J. S. Anand
Management of Neonates
Evaluation and Development of Potentially Better Practices to Improve Pain
Services
Updated Information &
http://pediatrics.aappublications.org/content/118/Supplement_2/S78
including high resolution figures, can be found at:
References
L
http://pediatrics.aappublications.org/content/118/Supplement_2/S78#BIB
This article cites 71 articles, 15 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/agency_abcs
Agency ABC's
collection(s):
This article, along with others on similar topics, appears in the following
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or in
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2006-0913D
2006;118;S78
Pediatrics
Paul J. Sharek, Richard Powers, Amy Koehn and Kanwaljeet J. S. Anand
Management of Neonates
Evaluation and Development of Potentially Better Practices to Improve Pain
http://pediatrics.aappublications.org/content/118/Supplement_2/S78
on the World Wide Web at:
The online version of this article, along with updated information and services, is located
American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.