0095-1137/10/$12.00 doi:10.1128/JCM.01801-09
Copyright © 2010, American Society for Microbiology. All Rights Reserved.
Clostridium difficile
Testing in the Clinical Laboratory
by Use of Multiple Testing Algorithms
䌤
Susan M. Novak-Weekley,
1* Elizabeth M. Marlowe,
1John M. Miller,
1Joven Cumpio,
1Jim H. Nomura,
2Paula H. Vance,
3and Alice Weissfeld
3Southern California Permanente Medical Group, North Hollywood,1and Southern California Permanente Medical Group,
Los Angeles,2California, and Microbiology Specialists Inc., Houston, Texas3
Received 12 September 2009/Returned for modification 5 November 2009/Accepted 5 January 2010
The incidence ofClostridium difficileinfection (CDI) has risen almost 3-fold in the United States over the past decade, emphasizing the need for rapid and accurate tests for CDI. The Cepheid XpertC. difficileassay is an integrated, closed, nucleic acid amplification system that automates sample preparation and real-time PCR detection of the toxin B gene (tcdB). A total of 432 stool specimens from symptomatic patients were tested by a glutamate dehydrogenase (GDH) assay, a toxin A and B enzyme immunoassay (EIA), the XpertC. difficile
assay, and a cell culture cytotoxicity neutralization assay (CCCN). The results of these methods, used individually and in combination, were compared to those of toxigenic culture. Results for the XpertC. difficile
assay alone showed a sensitivity, specificity, positive predictive value, and negative predictive value (NPV) of 94.4, 96.3, 84.0, and 98.8%, while the EIA alone gave corresponding values of 58.3, 94.7, 68.9, and 91.9%, respectively. An algorithm using the GDH assay and the EIA (plus the CCCN if the EIA was negative) showed corresponding values of 83.1, 96.7, 83.1, and 96.1%. The XpertC. difficileassay was statistically superior to the EIA (P, <0.001 by Fisher’s exact test) and to the GDH-EIA-CCCN algorithm (P, 0.0363). Combining the GDH and XpertC. difficileassays lowered both the sensitivity and the NPV of the Xpert assay. The GDH-EIA-CCCN procedure required, on average, 2 days to complete testing on GDH-positive results, while testing by the Xpert
C. difficile assay was completed, on average, in less than 1 h. Xpert C. difficile testing yielded the highest
sensitivity and NPV, in the least amount of time, of the individual- and multiple-test algorithms evaluated in this study.
Clostridium difficile is the main cause of infectious health
care-associated diarrhea in the United States and around the world.C. difficileinfections (CDI) can vary from a mild diar-rhea to the potentially fatal pseudomembranous colitis, toxic megacolon, and sepsis (7, 19).C. difficilecolonization of the bowel often follows disruption of normal flora after the patient receives antimicrobial therapy. The incidence and severity of
C. difficilehas increased in both hospital and long-term care
settings, due in part to the emergence of several novel strains, including the epidemic J strain described by Johnson et al. and the hypervirulent NAP1/027/BI strain (16, 19). Strain NAP1/ 027/BI produces high quantities of spores, which disseminate easily in the hospital environment, and is associated with high mortality rates (1, 5, 9, 11, 17, 32).
Historically, the cell culture cytotoxicity neutralization assay (CCCN), which detects cytotoxin production in monolayers of cells, such as human diploid fibroblasts, has been the gold standard forC. difficile detection in the laboratory. However, cell culture is labor-intensive, and many laboratories have adopted other testing methods, such as enzyme immunoassays (EIAs) for toxins A and B, which are easier and faster to perform than CCCN (22, 27, 33). However, recent reports have highlighted the lack of sensitivity of the toxin A/B EIAs, which
show sensitivities as low as 48% (2, 28). Although toxigenic culture of the organism has now been reaccepted as the true gold standard (25), this method requires substantial laboratory resources, and results are not available in a short enough time frame to be clinically useful (18, 24, 28). Thus, other ap-proaches to improving both the sensitivity and the cost-effec-tiveness of C. difficile testing have been introduced (2, 22). Testing algorithms using a glutamate dehydrogenase (GDH) assay (which has presumptively higher sensitivity but lacks specificity) to screen forC. difficilein stool samples, with reflex testing using a more specific assay, such as a toxin A/B EIA or the CCCN, have been proposed (26, 29, 31). GDH assays detect antigen present in both toxigenic and nontoxigenic strains ofC. difficiledirectly in stool samples. The time neces-sary to perform the GDH assay with EIA or CCCN confirma-tion can be as long as 3 days (34). Gilligan noted that EIAs often lack sufficient sensitivity for confirmation of positive GDH assay results (14). In this algorithm, the need to confirm GDH-positive specimens increases the turnaround time (TAT) for positive results, delaying the notification of the physician ordering the test. PCR assays for various targets have been developed as a potential replacement for the less-sensitive (EIA) and less-specific (GDH) assays forC. difficiledetection (3, 4, 6, 23, 30). Such assays include both “home brew” PCR assays and FDA-cleared commercial assays (15, 20, 28, 30). Cepheid (Sunnyvale, CA) has recently developed a GeneXpert cartridge-based assay for detection of the C. difficiletoxin B gene (tcdB) directly from stool. In this study, we compared the sensitivity and specificity of the XpertC. difficilePCR assay to
* Corresponding author. Mailing address: Kaiser Permanente, SCPMG Regional Reference Labs, 11668 Sherman Way, North Hol-lywood, CA 91605. Phone: (818) 503-6884. Fax: (818) 503-6866. E-mail: [email protected].
䌤Published ahead of print on 13 January 2010.
889
on May 16, 2020 by guest
http://jcm.asm.org/
those of the GDH assay and the EIA, individually and within specific testing algorithms, using toxigenic culture as the gold standard for a positive specimen.
(This work was previously presented as a poster at the 109th General Meeting of the American Society for Microbiology, 2009.)
MATERIALS AND METHODS
Study population and sample collection.This was a prospective study con-ducted at the Southern California Permanente Medical Group Regional Refer-ence Laboratories. Eligible patients included those with suspected CDI for whom toxin EIAs from unformed stool were ordered forC. difficiletesting according to the institution’s standard practices. All specimens enrolled and tested in this study represented excess, leftover stool, and therefore, informed consent was waived by the Institutional Review Board. Duplicate specimens from the same patient and patients under the age of 2 years were excluded.
Upon the establishment of eligibility and following standard testing at the institution, excess unformed stool specimen was placed in a sterile container. A portion of the specimen was shipped to a single central laboratory for reference culture. The remaining unformed stool was used for testing by the EIA, the GDH assay, and the XpertC. difficileassay on site. Those specimens that were negative forC. difficileby the EIA but positive by the GDH assay were further tested for cytotoxin B by the CCCN.
Enzyme immunoassay.Toxin testing was performed using the Premier Toxins A & B microwell EIA (Meridian Bioscience, Inc., Cincinnati, OH). The assay was performed on previously frozen stool specimens according to the manufac-turer’s instructions. Positive results for the Premier Toxins A & B EIA are indicated by optical densities at 450 and 630 nm (OD450/630) ofⱖ0.100, and negative results are indicated by OD450/630of⬍0.100.
Glutamate dehydrogenase. Specimens were tested for GDH using the TechLabC.DIFFCHEK-60 EIA (distributed by Inverness Medical Innovations, Inc., Princeton, NJ). Testing was performed on previously frozen stool specimens according to the manufacturer’s recommendations. Negative results for GDH antigen are indicated by OD450/630of⬍0.80, and positive results are indicated by OD450/630ofⱖ0.80. Specimens that were positive for GDH were tested by EIA. GDH-positive, EIA-positive specimens were considered positive for toxin B-producingC. difficile. Those specimens that were GDH positive and EIA nega-tive were tested by the CCCN. GDH-posinega-tive, EIA-neganega-tive, CCCN-posinega-tive specimens were considered positive for toxin B-producingC. difficile.
Xpert C. difficile PCR assay.The XpertC. difficile PCR assay (Cepheid, Sunnyvale, CA) was performed according to the manufacturer’s instructions. Briefly, a swab was dipped into the unformed stool specimen container. The swab was placed in sample reagent and capped. The specimen was vortexed for 10 s, and all the liquid from the sample reagent was transferred to the “S” chamber of the cartridge using a large transfer pipette. Next, reagent 1 was added to chamber 1 of the test cartridge. Finally, reagent 2 was added to chamber 2 of the test cartridge, and the lid was closed. The cartridge barcode was scanned and placed in the GeneXpert instrument. Any XpertC. difficileassay not yielding a result on the first attempt was repeated using new reagents and a new cartridge. If no result was obtained upon retesting, the specimen was reported as unresolved.
Cell culture cytotoxicity neutralization assay.Approximately 1 ml of fecal material was transferred to M4 transport medium, centrifuged at 2,500 rpm for 15 min, and filtered with a 0.45-m-pore-size Millex-HA filter unit. Next, 250l of filtered stool was inoculated into two tubes of Vero cells (Diagnostic Hybrids, Inc., Athens, OH). Simultaneously, a preincubated filtrate antitoxin mixture (TechLab, Blacksburg, VA) was inoculated into the second tube. Tubes were incubated at 35⫾2°C for 3 days. Cells were observed daily for cytopathic effect in the first tube and neutralization (no toxic effect) in the second tube, using an inverted microscope at a total magnification of⫻63. Specimens that were neg-ative forC. difficiletoxin (CDT) showed cells that remained normal in appear-ance, while specimens positive for CDT demonstrated cytotoxicity. The lack of specific cytopathic effect in the antitoxin-neutralized well confirms CDT.
Reference culture methods.All bacterial cultures were performed at a single centralized reference laboratory that was blinded to the other test results. An aliquot of the unformed stool specimen was shipped on ice packs in anaerobic transport medium (Anaerobe Systems, Morgan Hill, CA). Toxigenic culture was initiated within 2 days of sample receipt; all manipulations took place under an anaerobic atmosphere. Stool was inoculated into prereduced cycloserine-cefox-itin-fructose direct agar (CCFA-D) and cycloserine-cefoxitin-mannitol broth with taurocholate lysozyme cysteine (CCMB-TAL) (Anaerobe Systems). The CCFA-D plate was incubated at 35°C to 37°C for 48 h; CCMB-TAL was
incu-bated at 35°C to 37°C for 24 h. CCMB-TAL was subcultured at 24 h to a second CCFA plate (CCFA-E [enriched]). If the CCFA-D plate was positive forC. difficile(see the testing protocol below), the CCFA-E plate was discarded. If the CCFA-D plate was negative forC. difficile, the CCFA-E plate was considered as described below.
Aerotolerance testing was performed from the CCFA plate. The appearance of large Gram-positive rods that were obligate anaerobes from CCFA and were susceptible to 5g of vancomycin was considered presumptive evidence ofC. difficile. These isolates were subcultured, using approximately 2 to 4 colonies, to chopped meat broth with carbohydrates (CMC) and were incubated for 2 days. The presence of iso acids as an end product of glucose fermentation by gas-liquid chromatography served as confirmation of identification. A cell-free supernatant was then tested by a cytotoxin assay similar to that described above (instead using tube cultures of human foreskin fibroblasts; Diagnostic Hybrids, Inc.) to detect
C. difficiletoxin B. AC. difficileantitoxin was used to demonstrate the specificity of the tissue culture reaction by neutralizing the cytotoxin present in the super-natant.
Analysis.A sample was considered to contain toxigenicC. difficileif the CCCN for cytotoxin B from a culture supernatant was positive. Performance character-istics were calculated for the GDH assay, the EIA, and the XpertC. difficileassay relative to the toxigenic culture result. Accuracy is defined as the percentage of overall agreement between the two tests or algorithms being compared. Perfor-mance was further investigated by considering the results of the GDH assay and EIA combined versus toxigenic culture; the GDH and XpertC. difficileassays combined versus toxigenic culture; and GDH, EIA, and CCCN testing combined versus toxigenic culture.
Statistical methods.This study was conducted in order to compare several different methods/algorithms for detectingC. difficile. The equivalency of these platforms/algorithms was categorically analyzed with 2⫻5 tables using the chi-square test and Fisher’s exact test under the Freq procedure in the SAS system, version 9. Fisher’s exact test calculates the actual (nonasymptotic) prob-ability of observing the actual results (or something more extreme) given that the different methods are in fact equivalent. APvalue of⬎0.05 by Fisher’s exact test indicates that the categories are statistically equivalent. The chi-square test gives an asymptotic probability for the same data. ThePvalue is the probability of obtaining the observed result, or something more extreme, given that all the tests are in fact equivalent. This gives the statistical significance of the test and is used to test the null hypothesis of no difference between the different methods.
RESULTS
Clinical performance.The performances of the GDH assay, EIA, and XpertC. difficileassay as individual indicators and as parts of testing algorithms for the presence of toxin
B-produc-ingC. difficilewere assessed for 432 stool samples; the results
of each assay were compared to the results of toxigenic culture. In this study, both direct toxigenic and enriched toxigenic cul-tures were performed. If the direct toxigenic culture was neg-ative, then the results of the enriched toxigenic culture were evaluated. Four specimens failed to yield a valid PCR result by use of the XpertC. difficileassay (n⫽ 428). For the GDH-EIA-CCCN algorithm, one cytotoxin specimen gave no result, due to bacterial contamination (n⫽431). Only four samples yielded nontoxigenicC. difficileisolates. Relative to toxigenic culture, the XpertC. difficileassay demonstrated a sensitivity, a specificity, and positive and negative predictive values of 94.4, 96.3, 84.0, and 98.8%, respectively, while the EIA dem-onstrated a sensitivity, a specificity, and positive and negative predictive values of 58.3, 94.7, 68.9, and 91.9%, respectively (Table 1).
Compared to toxigenic culture, the algorithm of the GDH assay and the EIA yielded a sensitivity, a specificity, and pos-itive and negative predictive values of 55.6, 98.3, 87.0, and 91.7%, respectively, and the algorithm of the GDH assay com-bined with the toxin EIA and the CCCN (if the confirmation EIA gave a negative result) demonstrated values of 83.1, 96.7, 83.1, and 96.7%, respectively (Table 1). The GDH assay
on May 16, 2020 by guest
http://jcm.asm.org/
bined with the XpertC. difficilePCR assay demonstrated both lower sensitivity (86.1%) and a lower negative predictive value (97.8%) than the XpertC. difficileassay alone (Table 1). The addition of the GDH screening test increased the turnaround time for most results. The GDH-EIA-CCCN results were available, on average, in 48 h, while the results of the XpertC.
difficileassay were available, on average, in less than 1 h.
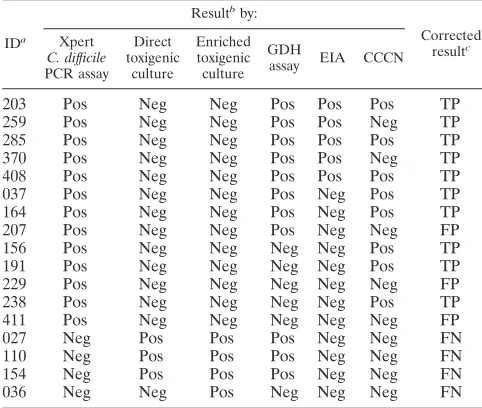
Of the 13 patient specimens that were positive by the Xpert
C. difficilePCR assay and negative by toxigenic culture, three
specimens were positive by the GDH assay, the EIA, and the CCCN; two specimens were GDH positive, EIA positive, and CCCN negative; two specimens were GDH positive, EIA neg-ative, and CCCN positive; one specimen was GDH positive, EIA negative, and CCCN negative; three specimens were GDH negative, EIA negative, and CCCN positive; and two specimens were negative by the GDH assay, the EIA, and the CCCN (Table 2). Of the four specimens that were negative by the Xpert C. difficile assay but culture positive, three were
GDH positive, EIA negative, and CCCN negative (Table 2). Eleven of the 17 specimens for which discrepant results were obtained came from patients with histories ofC. difficile infec-tion.
The results of a categorical analysis of the data across the different methods showed that the methods gave statistically different results for sensitivity (P,ⱕ0.001 [P,⬍0.0001 both by Fisher’s exact test and by the chi-square test]). However, theP
value for specificity wasⱖ0.05 (P, 0.0657 by Fisher’s exact test and 0.0603 by the chi-square test), indicating that the different methods are statistically equivalent for specificity, although the lower specificity of the EIA approached significance (data not shown). There was no statistical difference between the sensi-tivity result for the toxin EIA (58.3%) and that for the combi-nation of the GDH assay and the toxin EIA (55.6%) (P, 0.8664 by Fisher’s exact test) or between the sensitivity result for the XpertC. difficileassay (94.4%) and that for the GDH assay– XpertC. difficileassay algorithm (86.1%) (P⫽0.1578), which was surprising given the large gap between the sensitivities, although the lack of significant difference may have been due to the relatively small number of positive samples in this study. There were, however, statistically significant differences be-tween the sensitivity result for the XpertC. difficileassay alone and that for the toxin EIA alone (P⬍0.001) and between the sensitivity result for the XpertC. difficileassay alone and that for the GDH-EIA-CCCN three-test algorithm (P⫽0.0363).
DISCUSSION
CDI is a major medical and infection control problem in many health care facilities, including hospitals, long-term care facilities, and nursing homes around the world (8, 20). Accu-rate and timely diagnosis is necessary both for appropriate clinical management of the patient and for the timely imple-mentation of infection control and pharmacy measures (13, 21). Many hospitals are now required to report health care-associated transmission of pathogens, includingC. difficile, to public health departments. Thus, it is imperative that the di-agnosis of CDI be rapid and accurate.
Due to the poor sensitivity of the toxin A/B EIAs, patients with negative toxin EIA results who are still suspected of hav-ing CDI are often subjected to additional testhav-ing and proce-dures, adding substantial costs to hospitalization (14, 19).
Per-TABLE 1. Summary of algorithm versus stand-alone testing options compared to direct/enriched toxigenic culture
Parametera Test(s)
EIA only GDH⫹EIA GDH⫹EIA⫹cytotoxinb
GDH⫹Xpertc
Xpert onlyd
No. of specimens 432 432 431 432 428
Sensitivity 58.3 (42/72) 55.6 (40/72) 83.1 (59/71) 86.1 (62/72) 94.4% (68/72)
Specificity 94.7 (341/360) 98.3 (354/360) 96.7 (348/360) 97.8 (352/360) 96.3 (343/356) Accuracy 88.7 (383/432) 91.2 (394/432) 94.4 (407/431) 95.8 (414/432) 96.0 (411/428)
PPV 68.9 (42/61) 87.0 (40/46) 83.1 (59/71) 88.6 (62/70) 84.0 (68/81)
NPV 91.9 (341/371) 91.7 (354/386) 96.7 (348/360) 97.2 (352/362) 98.8 (343/347)
a
Sensitivity, specificity, accuracy, positive predictive value (PPV), and negative predictive value (NPV) are expressed as percentages followed by fractions in parentheses as follows: sensitivity, (number of true-positive results)/(sum of true-positive and false-negative results); specificity, (number of true-negative results)/(sum of true-negative and false-positive results); accuracy, (number of true results)/(total results); PPV, (number of true-positive results)/(sum of true-positive and false-positive results); NPV, (number of true-negative results)/(sum of true-negative and false-negative results).
b
Cytotoxin assay results were not available for one specimen. c
The four specimens with no Xpert results were GDH negative, so according to the algorithm, no Xpert test was needed. d
[image:3.585.44.542.80.170.2]Xpert results were not available for four specimens.
TABLE 2. Characterization of specimens with discrepant results by the XpertC. difficileassay versus toxigenic culture
IDa
Resultbby:
Corrected resultc Xpert
C. difficile
PCR assay Direct toxigenic
culture
Enriched toxigenic culture
GDH
assay EIA CCCN
203 Pos Neg Neg Pos Pos Pos TP
259 Pos Neg Neg Pos Pos Neg TP
285 Pos Neg Neg Pos Pos Pos TP
370 Pos Neg Neg Pos Pos Neg TP
408 Pos Neg Neg Pos Pos Pos TP
037 Pos Neg Neg Pos Neg Pos TP
164 Pos Neg Neg Pos Neg Pos TP
207 Pos Neg Neg Pos Neg Neg FP
156 Pos Neg Neg Neg Neg Pos TP
191 Pos Neg Neg Neg Neg Pos TP
229 Pos Neg Neg Neg Neg Neg FP
238 Pos Neg Neg Neg Neg Pos TP
411 Pos Neg Neg Neg Neg Neg FP
027 Neg Pos Pos Pos Neg Neg FN
110 Neg Pos Pos Pos Neg Neg FN
154 Neg Pos Pos Pos Neg Neg FN
036 Neg Neg Pos Neg Neg Neg FN
a
ID, specimen identification number. b
Pos, positive; Neg, negative. c
TP, true positive; FP, false positive; FN, false negative.
on May 16, 2020 by guest
http://jcm.asm.org/
[image:3.585.42.283.495.699.2]haps more importantly, a significant number of active C.
difficilecarriers are undiagnosed, leading to unmitigated
trans-mission in health care settings. Often one or more stool spec-imens are collected following the first EIA-negative result if the suspicion of CDI is high (10, 20). Algorithms forC. difficile
testing in the hospital setting have evolved due to the need for more-accurate assays to better detect those patients with CDI (26, 31). Algorithms that appear to be more sensitive than testing by the toxin A/B EIA alone have been implemented in laboratories (26, 29, 31). These algorithms use the GDH assay as a screen and confirm GDH-positive results with the toxin A/B EIA, or with either culture or the CCCN. In previously published data, the GDH assay appeared to have good sensi-tivity in detecting C. difficile-positive specimens but lacked specificity (29). Two recent studies evaluated a multistep ap-proach with the GDH assay as a screening assay and found that as many as 23 to 24% of the positive specimens were missed by using this algorithm (i.e., sensitivity was approximately 76%) (26, 28). In our study, using a multistep approach, we achieved a sensitivity of 83.1% compared to toxigenic culture by using the GDH assay as the initial screen. These results are slightly lower than those reported by Eastwood et al. (12), who noted a GDH assay sensitivity of 87.6% compared to toxigenic cul-ture in their study.
Although these multitest algorithms improve the specificity of the GDH test, they delay the reporting of the results to the ordering physician (14). Multitest algorithms often require 2 or more days to validate a positive screening result, particularly if the CCCN is used for confirmation. Although many physicians start empirical therapy when a patient is suspected of having CDI, others wait for the results of the diagnostic tests to con-firm the diagnosis of CDI before stopping other antibiotics and initiating specific CDI therapy. This delay, especially in com-bination with the low sensitivity of the EIA, can facilitate the spread ofC. difficileto other patients and further contamina-tion of the environment, in addicontamina-tion to increasing the potential for the patient to develop more-severe disease (21).
Our data demonstrate that the sensitivity and negative pre-dictive value of the XpertC. difficileassay exceed those of the other individual assays and testing algorithms, specifically the GDH-EIA-CCCN algorithm (P, 0.0363), which is superior to the GDH-EIA algorithm in terms of sensitivity (83.1% versus 55.6%, respectively). This study confirms other published data demonstrating that the sensitivity of the EIAs currently mar-keted is very limited; thus, they should not be considered reliable for the detection of CDI. A review of the other testing results for specimens that were positive by the XpertC. difficile
assay but negative by reference toxigenic culture shows that 7 of 13 specimens appear to be true-positive specimens, given the positive GDH, EIA, and/or CCCN results (Table 2). The corrected sensitivity and specificity of the PCR assay would be 95.1% and 99.4%, respectively. Negative results by reference toxigenic culture could be due to several factors, such as pa-tients’ receipt of antimicrobial agents at the time of specimen collection, the lag time between specimen collection and test-ing, or the presence of nonviable organisms in the sample. Lack of either heat or alcohol shock for spore enrichment in the culture protocol may also have contributed to these seem-ingly false-negative culture results. Conversely, three of the four specimens that were negative by the XpertC. difficileassay
but positive by reference toxigenic culture were positive by the GDH assay but both EIA negative and CCCN negative (Table 2), which may be explained by a sampling problem due to low concentrations of organisms in very heterogeneous samples. Taken together, however, these data suggest that the sensitivity and specificity of the XpertC. difficileassay would allow the laboratory not only to enhance and speed up the detection of toxigenicC. difficilebeyond that with EIAs and GDH assay-based algorithms but also to have even more confidence in an initially negative result based on one test only. Further studies will be needed to determine the significance of PCR-positive results for patients who test negative by other conventional methods.
Two other PCR assays for C. difficile have recently been cleared by the FDA for use in U.S. laboratories. The results of those FDA-cleared assays were compared to the results of the CCCN rather than to the results of toxigenic culture in the clinical trials used for FDA clearance (30). Compared to the CCCN, these assays performed well. However, Stamper et al. compared the GeneOhm assay from Becton Dickinson & Company (BD) to toxigenic culture and demonstrated a sen-sitivity of 83.6%, which was lower than stated in the package insert for the BD product (30). Eastwood et al. (12) reported a somewhat higher sensitivity (88.5%) for the BD assay com-pared to toxigenic culture. Gluck et al. (15) comcom-pared the Prodesse proGASTROC. difficilePCR assay to toxigenic cul-ture and reported a sensitivity of 73.3% and a specificity of 99.2%. Since toxigenic culture has better sensitivity than the CCCN alone for detectingC. difficile, it is not surprising that the sensitivities reported by Stamper et al. and Gluck et al. when comparing the assays to the gold standard are lower than those reported in the package inserts (30). The sensitivity of the Xpert C. difficile assay was determined in this study by comparing the results to those of enriched toxigenic culture. A study comparing the results of all three commercial PCR meth-ods for the same stool specimen to those of enriched toxigenic culture would be of interest.
The cost-benefit ratio of the PCR-based assays, which will be more expensive than the GDH-EIA-CCCN algorithm, needs to be determined. Due to the improved sensitivity that PCR assays provide, theoretically, physicians would be able to order fewerC. difficiletests in order to obtain an accurate diagnosis (25). This potentially offsets some of the increased cost of the newer PCR assays. Hospitals need to consider what TAT is needed forC. difficileresults, as well as the impact of TAT on the risk of transmission. Patient outcome should be considered in addition to other data in determining what approach toC.
difficiletesting is required in the laboratory setting. We
con-clude that when the various algorithms are compared, the XpertC. difficileassay, both with regard to sensitivity and with regard to the negative predictive value, exceeds the perfor-mance levels of the individual tests and the GDH-EIA-CCCN algorithm and may also be able to reduce the practice of multiple test ordering, which has become commonplace in many hospitals.
ACKNOWLEDGMENT
Financial support for this study was provided by Cepheid, Inc.
on May 16, 2020 by guest
http://jcm.asm.org/
REFERENCES
1.Akerlund, T., I. Persson, M. Unemo, T. Noren, B. Svenungsson, M. Wullt, and L. G. Burman.2008. Increased sporulation rate of epidemicClostridium difficiletype 027/NAP1. J. Clin. Microbiol.46:1530–1533.
2.Alcala´, L., L. Sanchez-Cambronero, M. P. Catalan, M. Sanchez-Somolinos, M. T. Pelaez, M. Marin, and E. Bouza.2008. Comparison of three commer-cial methods for rapid detection ofClostridium difficiletoxins A and B from fecal specimens. J. Clin. Microbiol.46:3833–3835.
3.Alonso, R., C. Mun˜oz, S. Gros, D. García de Viedma, T. Pela´ez, and E. Bouza.1999. Rapid detection of toxigenicClostridium difficilefrom stool samples by a nested PCR of toxin B gene. J. Hosp. Infect.41:145–149. 4.Arzese, A., G. Trani, L. Riul, and G. A. Botta.1995. Rapid polymerase chain
reaction method for specific detection of toxigenicClostridium difficile. Eur. J. Clin. Microbiol. Infect. Dis.14:716–719.
5.Bacci, S., G. St-Martin, B. Olesen, B. Bruun, K. E. Olsen, E. M. Nielsen, and K. Molbak.2009. Outbreak ofClostridium difficile027 in North Zealand, Denmark, 2008–2009. Euro Surveill.14:19183.
6.Barbut, F., M. Braun, B. Burghoffer, V. Lalande, and C. Eckert.2009. Rapid detection of toxigenic strains ofClostridium difficilein diarrheal stools by real-time PCR. J. Clin. Microbiol.47:1276–1277.
7.Bartlett, J. G.2006. Narrative review: the new epidemic of Clostridium difficile-associated enteric disease. Ann. Intern. Med.145:758–764. 8.Bartlett, J. G., and T. M. Perl.2005. The newClostridium difficile—what does
it mean? N. Engl. J. Med.353:2503–2505.
9.Brazier, J. S., B. Patel, and A. Pearson.2007. Distribution ofClostridium difficilePCR ribotype 027 in British hospitals. Euro Surveill.12:E070426. 10.Cardona, D. M., and K. H. Rand.2008. Evaluation of repeatClostridium
difficileenzyme immunoassay testing. J. Clin. Microbiol.46:3686–3689. 11.Coignard, B., F. Barbut, K. Blanckaert, J. M. Thiolet, I. Poujol, A.
Car-bonne, J. C. Petit, and J. C. Desenclos.2006. Emergence ofClostridium difficiletoxinotype III, PCR-ribotype 027-associated disease, France, 2006. Euro Surveill.11:E060914.
12.Eastwood, K., P. Else, A. Charlett, and M. Wilcox.2009. Comparison of nine commercially availableClostridium difficiletoxin detection assays, a real-time PCR assay forC. difficile tcdB, and a glutamate dehydrogenase detection assay to cytotoxin testing and cytotoxigenic culture methods. J. Clin. Micro-biol.47:3211–3217.
13.Gerding, D. N., C. A. Muto, and R. C. Owens, Jr.2008. Measures to control and preventClostridium difficileinfection. Clin. Infect. Dis.46(Suppl. 1):S43– S49.
14.Gilligan, P. H.2008. Is a two-step glutamate dehydrogenase antigen-cyto-toxicity neutralization assay algorithm superior to the premier toxin A and B enzyme immunoassay for laboratory detection of Clostridium difficile? J. Clin. Microbiol.46:1523–1525.
15.Gluck, L., J. Wehrlin, P. D. Stamper, W. Babiker, R. Alcabasa, D. Aird, I. Ikpeama, and K. C. Carroll.2009. Comparison of the Prodesse ProGastro Cd real-time PCR to a commercial cytotoxin assay, abstr. S87. Poster Abstr. 25th Clin. Virol. Symp. Ann. Meet. Pan Am. Soc. Clin. Virol.
16.Johnson, S., M. H. Samore, K. A. Farrow, G. E. Killgore, F. C. Tenover, D. Lyras, J. I. Rood, P. DeGirolami, A. L. Baltch, M. E. Rafferty, S. M. Pear, and D. N. Gerding.1999. Epidemics of diarrhea caused by a clindamycin-resistant strain ofClostridium difficilein four hospitals. N. Engl. J. Med.
341:1645–1651.
17.Loo, V. G., L. Poirier, M. A. Miller, M. Oughton, M. D. Libman, S. Michaud, A. M. Bourgault, T. Nguyen, C. Frenette, M. Kelly, A. Vibien, P. Brassard, S. Fenn, K. Dewar, T. J. Hudson, R. Horn, P. Rene, Y. Monczak, and A. Dascal.2005. A predominantly clonal multi-institutional outbreak of Clos-tridium difficile-associated diarrhea with high morbidity and mortality. N. Engl. J. Med.353:2442–2449.
18.McFarland, L. V.2009. Renewed interest in a difficult disease:Clostridium difficile infections—epidemiology and current treatment strategies. Curr. Opin. Gastroenterol.25:24–35.
19.Monaghan, T., T. Boswell, and Y. R. Mahida.2008. Recent advances in
Clostridium difficile-associated disease. Gut57:850–860.
20.Murabata, M., H. Kato, H. Yano, M. Ogura, J. Shibayama, Y. Wakimoto, Y. Arakawa, and M. Mizokami.2008. Intestinal colonization and nosocomial spread ofClostridium difficilein pediatric cancer patients under long-term hospitalization. Kansenshogaku Zasshi82:419–426.
21.Muto, C. A., M. K. Blank, J. W. Marsh, E. N. Vergis, M. M. O’Leary, K. A. Shutt, A. W. Pasculle, M. Pokrywka, J. G. Garcia, K. Posey, T. L. Roberts, B. A. Potoski, G. E. Blank, R. L. Simmons, P. Veldkamp, L. H. Harrison, and D. L. Paterson.2007. Control of an outbreak of infection with the hyper-virulentClostridium difficileBI strain in a university hospital using a com-prehensive “bundle” approach. Clin. Infect. Dis.45:1266–1273.
22.Novak-Weekley, S. M., and M. H. Hollingsworth.2008. Comparison of the premier toxin A and B assay and the TOX A/B II assay for diagnosis of
Clostridium difficileinfection. Clin. Vaccine Immunol.15:575–578. 23.Peterson, L. R., R. U. Manson, S. M. Paule, D. M. Hacek, A. Robicsek, R. B.
Thomson, Jr., and K. L. Kaul. 2007. Detection of toxigenicClostridium difficilein stool samples by real-time polymerase chain reaction for the diagnosis ofC. difficile-associated diarrhea. Clin. Infect. Dis.45:1152–1160. 24.Peterson, L. R., M. M. Olson, C. J. Shanholtzer, and D. N. Gerding.1988. Results of a prospective, 18-month clinical evaluation of culture, cytotoxin testing, and culturette brand (CDT) latex testing in the diagnosis of Clos-tridium difficile-associated diarrhea. Diagn. Microbiol. Infect. Dis.10:85–91. 25.Peterson, L. R., and A. Robicsek.2009. Does my patient haveClostridium
difficileinfection? Ann. Intern. Med.151:176–179.
26.Reller, M. E., C. A. Lema, T. M. Perl, M. Cai, T. L. Ross, K. A. Speck, and K. C. Carroll.2007. Yield of stool culture with isolate toxin testing versus a two-step algorithm including stool toxin testing for detection of toxigenic
Clostridium difficile. J. Clin. Microbiol.45:3601–3605.
27.Shin, B. M., S. J. Yoo, and H. J. Oh.2009. Comparison of two enzyme immunoassays for detection ofClostridium difficile toxin A and toxin B. Korean J. Lab. Med.29:122–126. (In Korean.)
28.Sloan, L. M., B. J. Duresko, D. R. Gustafson, and J. E. Rosenblatt.2008. Comparison of real-time PCR for detection of thetcdCgene with four toxin immunoassays and culture in diagnosis of Clostridium difficile infection. J. Clin. Microbiol.46:1996–2001.
29.Snell, H., M. Ramos, S. Longo, M. John, and Z. Hussain.2004. Performance of the TechLabC. DIFFCHEK-60 enzyme immunoassay (EIA) in combi-nation with the.C. difficileTox A/B II EIA kit, the TriageC. difficilepanel immunoassay, and a cytotoxin assay for diagnosis ofClostridium difficile -associated diarrhea. J. Clin. Microbiol.42:4863–4865.
30.Stamper, P. D., R. Alcabasa, D. Aird, W. Babiker, J. Wehrlin, I. Ikpeama, and K. C. Carroll.2009. Comparison of a commercial real-time PCR assay fortcdBdetection to a cell culture cytotoxicity assay and toxigenic culture for direct detection of toxin-producingClostridium difficilein clinical samples. J. Clin. Microbiol.47:373–378.
31.Ticehurst, J. R., D. Z. Aird, L. M. Dam, A. P. Borek, J. T. Hargrove, and K. C. Carroll.2006. Effective detection of toxigenicClostridium difficileby a two-step algorithm including tests for antigen and cytotoxin. J. Clin. Micro-biol.44:1145–1149.
32.Warny, M., J. Pepin, A. Fang, G. Killgore, A. Thompson, J. Brazier, E. Frost, and L. C. McDonald.2005. Toxin production by an emerging strain of
Clostridium difficileassociated with outbreaks of severe disease in North America and Europe. Lancet366:1079–1084.
33.Yoo, S. J., J. O. Kang, H. J. Oh, and B. M. Shin.2006. Comparison of two enzyme immunoassays forClostridium difficiletoxin A. Korean J. Lab. Med.
26:408–411. (In Korean.)
34.Zheng, L., S. F. Keller, D. M. Lyerly, R. J. Carman, C. W. Genheimer, C. A. Gleaves, S. J. Kohlhepp, S. Young, S. Perez, and K. Ye.2004. Multicenter evaluation of a new screening test that detectsClostridium difficilein fecal specimens. J. Clin. Microbiol.42:3837–3840.