Petra Ratka-Kr
uger
€
Hans-J
urgen Wenz
€
Unsplinted implants and teeth
supporting maxillary removable partial
dentures retained by telescopic crowns:
a retrospective study with
>
6 years
of follow-up
Authors’ affiliations:
Eberhard Frisch,Oral Surgery and Periodontology, Northern Hessia Implant Center, Hofgeismar, Germany
Petra Ratka-Kr€uger,Periodontology, Periodontology Section, Department of Operative Dentistry and Periodontology, University of Freiburg, Freiburg, Germany
Hans-J€urgen Wenz,Prosthodontics, Clinic of Prosthodontics, Propaedeutics and Dental Materials, Christian-Albrechts University, Kiel, Germany
Corresponding author: DMD Eberhard Frisch, MSc Markt 3, Hofgeismar 34369, Germany Tel.: +49 5671 925029
Fax: +49 5671 925027 e-mail: [email protected]
Key words: double crown, implant, long-term results, maintenance, peri-implantitis, retro-spective study, success, telescopic crown
Abstract
Objectives: Data regarding tooth- and implant-supported maxillary removable partial dentures (TIRPDs) are scarce. The objective of this research was to perform a retrospective evaluation of the clinical long-term outcome of maxillary TIRPDs rigidly retained via telescopic crowns in patients undergoing supportive post-implant therapy (SIT).
Material and Methods: The inclusion criteria were met by 26 patients restored with maxillary TIRPDs between 1997 and 2011 in a private practice. Primary crowns (Marburg double crowns, MDCs) on teeth were cemented, whereas those on implants were screw-retained. Using patient records and data from a cross-sectional clinical examination in 2013, the survival rates of the teeth, implants and prostheses, together with the biological and technical complications, were analyzed.
Results: After 6.123.80 (range: 2 16) years of loading, 23 non-smoking patients with 23 dentures supported by 60 implants and 66 teeth were available for assessment. Nine teeth (survival rate: 86.36%) were lost, whereas 1 implant (survival rate: 98.36%) failed because of
peri-implantitis. Although 30 implants (50%) in 16 patients (69.57%) showed bleeding on probing (BOP+), no further peri-implantitis was observed. The mean peri-implant probing depth (PPD) was 3.680.71 mm. All dentures were functional and required technical maintenance efforts amounting to 0.128 treatments per patient per year (T/P/Y).
Conclusions: Within the limitations of this study, we conclude that TIRPDs retained via MDCs may represent a viable treatment option for patients with residual maxillary teeth.
Implant-supported fixed prostheses or remov-able partial dentures (IRPDs), mostly using bars or ball attachments for retention on den-tal implants, have been increasingly used over the past several decades for the rehabili-tation of edentulous maxillae. In the litera-ture, data on implant-supported double crowns have been scarce. These restorations were first proposed as conical crowns (Besimo & Kempf 1995) and later as resilient (Heck-mann et al. 2004; Krennmair et al. 2007) and non-resilient (Eitner et al. 2008; Krennmair et al. 2012; Frisch et al. 2013b) telescopic crowns. Restorations utilizing this principle have yielded good long-term results (Wenz et al. 2001; Andreiotelli et al. 2010; Frisch et al. 2013a; Frisch et al. 2013b) and have been proposed for the implant-supported rehabilitation of partially dentate patients
(Mengel et al. 2002) who may experience an improvement in their oral-health-related quality of life by additional, strategic implant placement (Wolfart et al. 2013).
Such IRPDs provide secure function, can be easily repaired and offer good access for oral hygiene measurements (Budtz-Jorgensen€
1996; Bergman et al. 1997; Wagner & Kern 2000). It has been noted that accessibility of these designs to hygiene instruments is help-ful in preventing periodontitis (Wenz & Lehmann 1998). Implant planning based on the use of double crowns offers several advanta-ges, such as the option of utilizing residual teeth, relatively large freedom of anatomical abutment positioning and an opportunity to provide structures resembling fixed prosthe-ses while allowing added soft tissue support and the closure of interproximal spaces for
Date:
Accepted 18 March 2014 To cite this article:
Frisch E, Ratka-Kr€uger P, Wenz H-J. Unsplinted implants and teeth supporting maxillary removable partial dentures retained by telescopic crowns: a retrospective study with
>6 years of follow-up.
Clin. Oral Impl. Res.00, 2014, 1–7 doi: 10.1111/clr.12407
enhanced esthetics and phonetics. Fixed pros-theses supported by tooth–implant combina-tions are relatively well documented (Lang et al. 2004; Nickenig et al. 2006, 2008; Pjetursson & Lang 2008). By contrast, few investigations of removable partial dentures supported by tooth–implant combinations (TIRPDs) are available, and the evidence they have produced is scanty (Hug et al. 2006; Ka-ufmann et al. 2009; Bernhart et al. 2012). Only one study of tooth/implant-borne, dou-ble-crown-retained dentures in maxillae (Krennmair et al. 2007) was listed in a sys-tematic review by Koller et al. (2011). There is currently a lack of data concerning clinical studies and long-term results, especially those collected in the private practice setting. The Marburg double crown (MDC) (Wenz & Lehmann 1998) uses a clearance fit with no friction or wedging of the primary and secondary crown during insertion and removal. To achieve retention, additional attachments are used (TK-Snap, Si-Tec GmbH, Herdecke, Germany). These attach-ments consist of an elastic resin body holding a titanium ball, which in the terminal posi-tion snaps into a corresponding hollow in the parallel surface of the inner crown (Fig. 1). All metal components are produced from a single cobalt–chromium–molybdenum alloy, and the framework (including outer crowns) is cast in one piece. Therefore, the complete inner and outer crowns and framework can be produced from base metal alloys rather than the noble alloys typically used for indi-vidually milled telescopic and conical crowns (Wenz et al. 2001).
This study was performed to investigate patients with residual maxillary teeth who had been provided with telescopic crown-retained TIRPDs in a private dental practice. The purpose of this study was the retrospec-tive, long-term evaluation of the survival/ success rates of implants and dentures, along with their biological/technical complication rates.
Material and methods
This retrospective clinical study was con-ducted in a private practice specializing in implants (Northern Hessia Implant Center, Hofgeismar, Germany). A retrospective non-interventional study design was used, based on the analysis of primary patient data that had been extracted from the patients’ records. We evaluated the clinical outcomes of TIR-PDs rigidly retained via MDCs in maxillae with residual teeth. This study was reviewed and authorized by the Ethics Commission of the Albert-Ludwigs University Freiburg, Germany (application no. 46/10-120329). The recommendations for strengthening the reporting of observational studies in epidemi-ology (STROBE) were followed (von Elm et al. 2008).
Study population
Patients who were provided with maxillary double-crown-retained TIRPDs according to the MDC technique during the period between January 1997 and December 2011 and who were attending a post-implant main-tenance program were identified. These patients were approached during the annual maintenance appointments and were asked to participate in the study after having received written information regarding the aims and course of the investigation. Patients who provided written informed consent and met the following inclusion criteria were included:
Age≥18 years.
Having received surgical and prosthetic treatment in the study center.
Regular (at least annual) prophylaxis/sup-portive therapy in the study center. Retention of the denture by at least four double-crown attachments according to the MDC technique.
Double crowns exclusively screwed onto the implants and cemented on the teeth. Functional period of the final restoration >2 years.
Availability of the complete medical his-tory, including the following potential
risk factors: medication (immune suppres-sion and bisphosphonate), diabetes, cardio-vascular disease and rheumatoid arthritis, in addition to smoking habits.
The following exclusion criteria were applied:
Tobacco smoking
Use of implant designs other than the An-kylos (Dentsply Friadent, Mannheim, Ger-many) system.
Use of designs other than the MDC tech-nique for telescopic crowns on the teeth and implants.
Non-compliance with the post-implant maintenance program (minimum 19/ year).
Treatment course
The treatment planning aimed at achieving at least two supporting units (implants and/ or natural teeth) on each side of the maxilla. Edentulous sides were usually provided with 2 (and not more than 3) implants. Surgical treatment was performed under local anes-thesia and followed the manufacturer’s proto-col. All clinical procedures were performed by the same experienced clinician (EF). Anti-biotics were given 1 h before and continued for 1 week after the surgery (amoxicillin 1000 391/day). Wound assessment was per-formed after 7 days (suture removal) and 28 days. Second-stage surgery was performed after a healing period of 3 months.
Prosthodontic treatment (Figs 2–5) was conducted according to the Marburg double-crown (MDC) technique, with a clearance fit (Wenz & Lehmann 1998) and additional attachments (TK-Snap, Si-tec GmbH, Herdecke, Germany). The secondary struc-tures of all TIRPDs were cast in one piece and included no solder or welding joints. The primary telescopes were either screwed to the implants or cemented to the residual teeth.
Fig. 1. Schematic drawing of the Marburg double-crown system: (a) During insertion of the prosthesis, the resin body of the snap attachment undergoes elastic deforma-tion. (b) In the final position, the titanium ball of the attachment snaps into the corresponding hollow of the inner crown to provide retention.
Fig. 2. Internal view of the Marburg double crown with an additional retention element TK-Snap.
Following delivery of the TIRPDs, oral hygiene instructions were given to all patients. Subsequently, the patients were scheduled for a supportive post-implant hygiene therapy program (SIT) with tri-monthly visits. These sessions included an evaluation of peri-implant tissue status using the Quigley-Hein plaque index (QHI) (Quigley & Hein 1962) and measurement of peri-implant probing depths (PPDs) using a milli-meter-scaled periodontal probe (PCP 15; Hu-Friedy, Chicago, IL, USA) at four locations per implant (buccal, disto-buccal, mesio-oral, disto-oral). Any bleeding upon probing (BOP; 30 s following the probing) was noted,
and radiographs for implants with a positive BOP and a PPD≥5 mm were performed using the long-cone parallel technique. All follow-up sessions included reinforcement of patient motivation and repeated instruction regarding at-home plaque control. Finally, all implants and teeth were professionally cleaned using a polishing paste and a rubber cup (FSI Slimline, De Trey GmbH, Konstanz, Germany). During the complete study period, prosthesis design, material selection, surgical/technical proce-dures and SIT remained unchanged.
Data collection
Between January 1, 2013 and December 1, 2013, the patients in our study were evalu-ated according to the following parameters using patient records: age and gender, medi-cal history, smoking habits, anatomical position of the implants (according to the Federation Dentaire Internationale [FDI] scheme), number of implants, loss of implants, time of denture placement, oppos-ing dentition and the period of observation. Moreover, during the last SIT appointment, the subjects were clinically examined by an EF, who evaluated the following biological and technical complications of the teeth/ implants and removable dentures: screw loos-ening, material fractures, loss of retention, changing retention elements, relinings, secondary caries (teeth) or peri-implantitis (implants). A periodontal examination (including PPD and BOP) was performed for all implants. To confirm the diagnosis of peri-implant disease in implants with a posi-tive BOP and PPD≥5 mm, radiographs were taken to measure the extent of peri-implant bone loss with respect to the baseline radio-graph (prosthetic delivery). To assess the peri-implant bone level, intra-oral radiographs were taken using the parallel technique.
Diagnostic criteria and statistical analysis
Survival was defined as the continued pres-ence of the implant or prosthetic reconstruc-tion in the mouth, independent of biological and/or technical complications (Rinke et al. 2011; Frisch et al. 2013a). Any technical complication related to the overdenture or the implant abutment (e.g., abutment screw loosening, fracture of the abutment, fracture of the denture base or denture teeth, loss of retention or defects in the attachments) was recorded. Incidence rates for technical com-plications were calculated based on the num-ber of treatments occurring per patient per year (T/P/Y).
Every recorded BOP incident was defined as peri-implant mucositis (Fransson et al.
2008). No true endpoints have been identified to diagnose peri-implantitis (Lee 2011; Klinge et al. 2012, Mombelli et al. 2012). Therefore, the following surrogate endpoints were used: positive BOP, PPD≥5 mm and a maximum bone loss of ≥3.5 mm (Rinke et al. 2011; Frisch et al. 2013a). Because of the small sample size, no meaningful statistical analy-sis of potential factors influencing the treat-ment outcome was possible. Therefore, only descriptive statistics (no statistical test or confidence interval) were applied.
Results
Patients
In total, 26 patients met the inclusion crite-ria. Because one patient moved out of the area and two patients changed their dental provider, the dropout rate was 11.54%. Therefore, 23 non-smoking patients aged 71.668.04 (range: 52.29 86.39) years were available for the study. All patients attended 1–4 SIT appointments/year. Of these patients, 15 were female (65.22%) and 8 were male (34.78%). The medical histories revealed car-diovascular disease in 11 (47.83%) patients. No patient suffered from diabetes. The mean follow-up was 6.123.80 years, and the median follow-up was 5.03 (range: 2.01 15.95) years. Table 1 summarizes the pertinent patient data.
Implant treatment
In total, 61 implants with a Morse taper con-nection (Ankylos, Dentsply Friadent, Mann-heim, Germany) were provided with unsplinted telescopic crowns according to the MDC technique. The mean implant length was 11.291.46 (range: 9.5–14) mm. Table 2 summarizes the distribution of implants and teeth using the FDI numbering system. One implant was lost within the observation per-iod after 5 years of intra-oral service as a result of peri-implantitis (implant survival rate: 98.36%).
Tooth treatment
In total, 66 teeth were provided with tele-scopic crowns according to the MDC tech-nique. Within the observation period, we observed the loss of nine teeth (13.64%) in seven patients (30.43%) after a mean of 5.58 (range: 2.78 10.75) years. Hence, the cumula-tive survival rate of telescope-fitted teeth was 86.36% after a mean of 6.12 years. Reasons for tooth loss were caries (seven teeth), failed endodontic treatment (two teeth) and one crown fracture. No cases of tooth intrusion or periodontal disease were observed. Tables 3
Fig. 3. Maxilla with two residual teeth and three addi-tional implants prepared for restoration.
Fig. 4. Primary telescopes cemented to the teeth and screwed to the implants.
Fig. 5. Intra-oral view of the tooth- and implant-sup-ported MDC-RPD.
and 4 summarize the results obtained for the clinical parameters related to the teeth and implants.
Dentures
Each of the 23 included patients had received a removable telescopic denture supported by a combination of teeth (n=66) and implants (n=61). All TIRPDs were fabricated by one-piece casting of the secondary structure and were retained via MDCs. All dentures were found to be functional at the time of investi-gation, and none had been renewed; there-fore, the survival probability for the TIRPDs in our study was 100% after a mean observa-tion period of 6.12 years. The opposing denti-tion consisted of teeth or a fixed restoradenti-tion in 13 cases (56.52%), and 10 patients were restored with a removable partial denture (43.48%); no patient had full dentures (Table 1).
Technical maintenance requirements
In addition to treatments necessitated by tooth loss, the patients required 18 visits to
address technical requirements, for a total incidence of 0.128 treatments per patient per year (T/P/Y). No case of abutment loosening occurred. Screw loosening (primary crowns were screwed onto the abutments) was found seven times, which resulted in an incidence of 0.05 T/P/Y. Within the observation period, one “TK-Snap” retaining element of a Marburg double crown had to be replaced (0.007 T/P/Y). Furthermore, eight treatments were necessary to address prosthetic require-ments (i.e., relining or veneer fracture) (0.057 T/P/Y). Table 5 presents an overview of the technical complications and prosthetic main-tenance requirements.
Peri-implant mucositis/peri-implantitis
The mean plaque index (mod. QHI) was 0.270.45 (median 0), with 43 implants (71.67%) exhibiting no plaque and 17 implants (28.33%) rated as 1. The mean peri-implant probing depth was 3.680.71 (2.25 6) mm, with a median value of 3.75 mm. Bleeding on probing (peri-implant mucositis) was observed in 30 implants (50%) and 16 patients (69.57%). BOP+ and PPD≥5 mm were exhibited by two implants (3.33%), but no implant pre-sented a mean bone loss≥3.5 mm; therefore, we determined no diagnosis of peri-implanti-tis according to the selected criteria.
Discussion
The goal of this study was to present long-term data on the clinical outcomes of maxil-lary MDC-retained TIRPDs in patients attending a SIT program in a private practice. The study revealed a limited incidence of biological and technical complications over a
>6-year period of intra-oral service.
In interpreting our results, it should be considered that only a small number of patients could be presented and that only 23 of 26 patients in whom dentures were placed could be followed for the complete observa-tion period. Furthermore, a control group with fixed or exclusively implant-supported restorations matched to the study group could not be presented. The provision of all
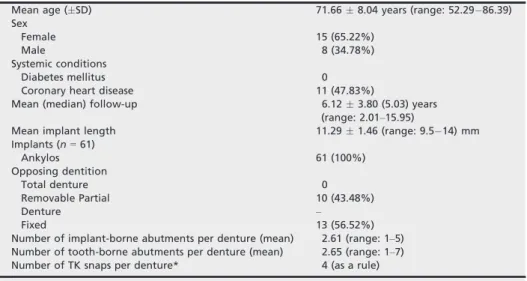
Table 1. Pertinent data for the patients and dentures (n=23)
Mean age (SD) 71.668.04 years (range: 52.29 86.39)
Sex
Female 15 (65.22%)
Male 8 (34.78%)
Systemic conditions
Diabetes mellitus 0
Coronary heart disease 11 (47.83%)
Mean (median) follow-up 6.123.80 (5.03) years
(range: 2.01–15.95)
Mean implant length 11.291.46 (range: 9.5 14) mm
Implants (n=61) Ankylos 61 (100%) Opposing dentition Total denture 0 Removable Partial 10 (43.48%) Denture – Fixed 13 (56.52%)
Number of implant-borne abutments per denture (mean) 2.61 (range: 1–5) Number of tooth-borne abutments per denture (mean) 2.65 (range: 1–7)
Number of TK snaps per denture* 4 (as a rule)
*Additional retaining elements of the Marburg double crowns.
Table 2. Distribution of the maxillary implants (n=61) and teeth (n=66)
Tooth position (FDI) 18 17 16 15 14 13 12 11 21 22 23 24 25 26 27 28
Implants (n) 1 0 3 11 10 6 3 1 1 3 7 6 5 4 0 0
Teeth (n) 0 2 0 0 1 10 4 7 7 5 9 5 7 4 5 0
Federation Dentaire Internationale (FDI).
Table 4. Outcomes of the implants (n=60) and TIRPDs (n=23) after a mean follow-up of 6.12 years
Mean probing depth 3.680.76 (range: 2 6) mm Bleeding on probing (peri-implant mucositis) 30 (50%) mod. QHI Median 0 Grade 0 43 (71.67%) Grade 1 17 (28.33%) Grade≥2 0 Implants lost 1 (1.64%) Peri-implantitis 0*
Implant survival rate 60 (98.36%) Implant success rate* 60 (98.36%) TIRPD survival rate 23 (100%) mod. QHI, mean plaque index. *The one implant with peri-implantitis was lost. Table 3. Outcomes of the teeth (n=66)
n %
Survival 57 86.36
Loss 9 13.64
Loss resulting from
Caries 6 9.09
Periodontitis 0 0
Intrusion 0 0
Endodontic complications 2 3.03
Fracture 1 1.52
Table 5. Prosthetic maintenance requirements of maxillary dentures (n=23) retained on 66 teeth and 61 implants by Marburg double crowns (mean follow-up: 6.12 years)
Total Abutment loosening Screw loosening TK-Snap* renewal RCMT† Denture repair Number of treatments (n) 18 0 7 1 2 8 Number of treatments (%) 100 0 39 6 11 44 Treatments/P/Y‡ 0.128 0 0.05 0.007 0.014 0.057
*Additional retaining elements of the Marburg double crowns;†re-cementation (primary telescope to the tooth);‡per patient per year.
treatments by a single provider represents another limitation. Because of the retrospec-tive nature of the study, the observation per-iod ranged from a minimum of 2 years up to 16 years.
The investigated implant system (Anky-losâ) offers a platform switch. Recent literature indicates that this characteristic may reduce peri-implant bone loss (Al-Nsour et al. 2012). Furthermore, the possible influences of a platform switch, different implant designs or abutment necks on bio-logical width formation and on pocket depths has not been clarified. These factors should be considered in the interpretation of the present results.
Despite these limitations, the present study is one of the first investigations focused on double-crown-retained TIRPDs in maxillae with residual teeth. This investiga-tion may contribute to further evaluainvestiga-tion of the long-term performance of TIRPDs because of the comparably long observational period of>6 years and the fact that non-resil-ient telescopic crowns were assessed. In pre-vious studies, different types of double crowns, often using resilient crowns, were investigated. The present clinical data were generated under the typical conditions of a private practice, whereas previous clinical studies of telescopic crown-retained overden-tures were predominantly conducted in uni-versity settings.
The tooth survival rate of 85.25% in our study fell into the lower range of similar studies of exclusively tooth-supported double-crown restorations (Wagner & Kern 2000; Verma et al. 2013). The 6-year observa-tion period of the present study appears par-ticularly relevant with regard to tooth loss because these events occurred after a mean of 5.62.4 years. Previous studies typically did not cover this observation period, which may emphasize the relevance of clinical long-term studies.
Implant survival rates of 95 100% have been described for removable implant-sup-ported dentures in edentulous mandibles fea-turing bars or ball attachments for retention (Bergendal & Engquist 1998; Gotfredsen & Holm 2000; Oetterli et al. 2001; Naert et al. 2004). The limited published data regarding double-crown-retained IODs in edentulous jaws (Koller et al. 2011; Krennmair et al. 2012) reveal success rates of 97%–100% for implants and 95–100% for overdentures. The implant survival rate of 98.36% and the TIR-PD survival rate of 100% after 6 years found in our study were comparable to those of pre-vious studies, that is, to the rates observed
for solely double-crown-retained IODs and other implant-supported retention systems.
In the literature, available data for tooth-and implant-supported RPDs have been rare, and most of the observation periods covered by these data are relatively short. Hug et al. (2006) monitored eight patients with eight maxillary dentures supported by tooth–
implant combinations over 2 years, mostly using ball attachments, but including≤5 con-ical crowns.
Krennmair et al. (2007) reported implant and tooth survival rates of 100% each and a 5% incidence of screw loosening in 22 patients with 60 maxillary implants followed for a mean of 3.2 years.
Nickenig et al. (2008) did not observe any differences in complication rates between implant-supported fixed prostheses and tele-scopic removable dentures in 224 patients.
Kaufmann et al. (2009) inserted removable dentures in 65 partially dentate jaws, mostly using root caps and ball attachments for anchorage. They included only seven tooth-supported and eight implant-tooth-supported tele-scopes in their study and indicated observa-tion periods≥3 years for 31 implants. No data were specifically given for the telescopes.
Bernhart et al. (2012) analyzed 16 patients with maxillary (n=14) and mandibular (n=2) restorations supported by 40 implants and 44 teeth over 2 years and reported 100% survival and success rates for both teeth and implants, with one case of screw loosening and two veneer fractures.
Schwarz et al. (2012) reported on double-crown-retained dentures after a mean obser-vation period of 3.4 years. Thirty-six TIRPDs (24 maxillary) supported by 80 implants and 102 teeth and 30 IODs supported by 129 implants were investigated. The survival rate of the TIRPDs was 100%.
The risk of tooth-supported telescopic den-tures undergoing loss of function was consid-erably reduced by instituting a systematic recall program with professional maintenance (W€ostmann et al. 2007). Our results support this finding for telescopic crown-retained TIRPDs, as the denture survival rates were found to be considerably higher than those reported for tooth-supported double-crown dentures and were similar to those offered by purely implant-supported double-crown den-tures (Koller et al. 2011; Frisch et al. 2013a). Presumably, the high-implant survival rate and the low prevalence of peri-implant dis-ease (mucositis and peri-implantitis) can be explained, at least partially, by excellent access to the abutments for oral hygiene and a high degree of patient compliance in our
SIT program (with its comparatively exten-sive schedule of trimonthly visits).
Prosthetic maintenance requirement values are an important factor in evaluating restor-ative treatment concepts. Published data on technical complications of IRPDs have been scarce; the maintenance requirements vary between 0.27 and 4.03 treatments per patient per year (T/P/Y) (Rentsch-Kollar et al. 2010; Weinl€ander et al. 2010; Mackie et al. 2011; Krennmair et al. 2012). In a prospective study assessing four interforaminal implants in the mandible and covering 3 years of follow-up, the requirement for prosthetic maintenance was 0.41 treatments per patient per year (T/ P/Y) with bar structures, compared with 0.45 T/P/Y for telescopic restorations (Krennmair et al. 2012). Another 5-year study of edentu-lous mandibles revealed 0.37 T/P/Y for milled bars supported by four implants, 1.2 T/P/Y for egg-shaped bars supported by four implants and 1.04 T/P/Y for ovoid transversal bars supported by two implants (Weinl€ander et al. 2010). Maintenance requirements vary-ing from 1.09 to 4.03 T/P/Y were observed in an 8-year comparative study of various implant systems used with ball attachments on two interforaminal implants (Mackie et al. 2011). A 10-year study of cases predom-inantly involving two interforaminal implants resulted in 0.25 T/P/Y for bars and 0.37 T/P/Y for ball attachments (Rentsch-Kollar et al. 2010). Our finding of 0.114 T/P/ Y confirms the relatively low-maintenance requirements for the implant-supported tele-scopic designs that were used (i.e., dentures fabricated by 1-piece casting of the secondary structure and retained by MDCs). Of these visits, 44% were exclusively devoted to the dentures themselves (i.e., relining or resin fractures). In another 11%, it was necessary to re-cement the tooth-retained telescopes, whereas only 45% of visits were related to the technology connecting the implants to the IODs.
Fixed dentures supported by tooth–implant combinations and featuring non-rigid connec-tions were previously found to intrude in approximately 5% of the natural teeth involved (Lang et al. 2004). The present find-ings for removable double-crown-retained res-torations revealed no intrusion of teeth.
The Consensus of the 7th European Work-shop on Periodontology describes peri-implant mucositis as a host response to the presence of bacterial biofilms and as a phase preliminary to peri-implantitis (Lang & Berglundh 2011). With a prevalence of 48% for mucositis and no cases of peri-implanti-tis, the data from the present study reveal
lower rates for peri-implant disease than those reported by Lindhe & Meyle (2008), who found mucositis and peri-implantitis, respectively, in 50% and 22–43% of the implant sites studied. Recent studies have yielded lower peri-implantitis rates of 18%, 11.2% and 9.1%, respectively, among indi-viduals attending professional SIT programs (Rinke et al. 2011; Costa et al. 2012; Frisch et al. 2013a). The results of our study appear to support these findings. It should be men-tioned that soft tissue quality (keratinzed mucosa width) and soft tissue level (mucosal recession) were not evaluated in our study. Therefore, not all peri-implant tissue changes could be included and the dimen-sion of attachment loss might be underesti-mated.
According to the literature, different types of double crowns have successfully been used for teeth and implants, but data comparing different double-crown systems are scarce. All of these studies reveal the same advanta-ges with regard to accessibility for oral hygiene measurements. Therefore, we hypothesize that comparable data concerning biological complications may be obtained for each type. However, our results may not be applicable to other double-crown systems,
because they include differences from the MDC system. IRPDs based on the MDC technique are cost-effective because noble alloys can currently be avoided. These resto-rations are well suited for double-crown-retained overdentures on both implants and teeth and therefore may be recommended for clinical use.
Implications for dental practice
1. The reported treatment concept of rigidlyretained TIRPDs may be well suited for patients with few remaining maxillary teeth. Based on the rates of implant and denture survival, in addition to biological and technical complications, this tech-nique is comparable to the alternative retention concepts and may be utilized clinically.
2. Patients with maxillary TIRPD restora-tions and compliance with a SIT program demonstrated a low risk for peri-implan-titis. The present data may lead clini-cians to reconsider the importance of implant accessibility for hygiene instru-ments. Easy access should be prioritized, especially in elderly patients.
3. The reported design of the dentures (one-piece casting of the secondary structure and retention by MDCs) showed no increased risk for technical complica-tions, even over extended periods.
Conclusion
In summary, our study revealed comparably high success rates and low rates of biological and technical complications for implants and dentures over a >6-year period for maxillary TIRPDs in patients attending supportive post-implant therapy (SIT) in a private prac-tice. Overdentures supported by teeth and implants and rigidly retained by MDCs appear to be well suited for rehabilitating maxillae with residual teeth. Further prospec-tive studies with more patients are necessary to validate the present results and to compare this treatment concept with alternative con-cepts of retaining RPDs and with alternative types of double crowns.
Disclaimer
The authors report no conflicts of interest or third-party funding of the study.
References
Al-Nsour, M.M., Chan, H.L. & Wang, H.L. (2012) Effect of the platform-switching technique on preservation of peri-implant marginal bone: a sys-tematic review.International Journal of Oral and Maxillofacial Implants27: 138–145.
Andreiotelli, M., Att, W. & Strub, J.R. (2010) Prosthodontic complications with implant overdentures: a systematic literature review. International Journal of Prosthodontics23: 195– 203.
Bergendal, T. & Engquist, B. (1998) Implant-sup-ported overdentures: a longitudinal prospective study.International Journal of Oral and Maxillo-facial Implants13: 253–262.
Bergman, B., Ericson, A. & Molin, M. (1997) Long-term clinical results after treatment with conical crown-retained dentures.International Journal of Prosthodontics10: 149–155.
Bernhart, G., Koob, A., Schmitter, M., Gabbert, O., Stober, T. & Rammelsberg, P. (2012) Clinical suc-cess of implant-supported and tooth– implant-sup-ported double crown-retained dentures. Clinical Oral Investigations16: 1031–1037.
Besimo, C. & Kempf, B. (1995)In vitro investiga-tion of various attachments for overdentures on osseointegrated implants. Journal of Oral Reha-bilitation22: 691–698.
Budtz-J€orgensen, E. (1996) Restoration of the par-tially edentulous mouth–a comparison of over-dentures, removable partial over-dentures, fixed partial
dentures and implant treatment.Journal of Den-tistry24: 237–244.
Costa, F.O., Takenaka-Martinez, S., Cota, L.O., Ferreira, S.D., Silva, G.L. & Costa, J.E. (2012) Peri-implant disease in subjects with and without preventive maintenance: a 5-year follow-up. Jour-nal of Clinical Periodontology39: 173–181. Eitner, S., Schlegel, A., Emeka, N., Holst, S., Will,
J. & Hamel, J. (2008) Comparing bar and double-crown attachments in implant-retained prosthetic reconstruction: a follow-up investigation.Clinical Oral Implants Research5: 530–537.
von Elm, E., Altman, D.G., Egger, M., Pocock, S.J., Gøtzsche, P.C. & Vandenbroucke, J.P. (2008) STROBE initiative. The strengthening the report-ing of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Journal of Clinical Epide-miology61: 344–349.
Fransson, C., Wennstrom, J. & Berglundh, T. (2008)€
Clinical characteristics at implants with a history of progressive bone loss.Clinical Oral Implants Research19: 142–147.
Frisch, E., Ziebolz, D. & Rinke, S. (2013a) Long-term results of implant-supported over-dentures retained by double crowns: a practice-based retro-spective study after minimally 10 years follow-up. Clinical Oral Implants Research12: 1281–1287. Frisch, E., Ziebolz, D., Ratka-Kruger, P. & Rinke, S.€
(2013b) Double crown-retained maxillary
overden-tures: 5-Year follow-up.Clinical Implant Dentis-try and Related Research. doi:10.1111/cid.12087. [Epub ahead of print].
Gotfredsen, K. & Holm, B. (2000) Implant-supported mandibular overdentures retained with ball or bar attachments: a randomized prospective 5-year study.International Journal of Prosthodontics13: 125–130.
Heckmann, S.M., Schrott, A., Graef, F., Wichmann, M.G. & Weber, H.P. (2004) Mandibular two-implant telescopic overdentures. Clinical Oral Implants Research5: 560–569.
Hug, S., Mantokoudis, D. & Mericske-Stern, R. (2006) Clinical evaluation of 3 overdenture con-cepts with tooth roots and implants: 2-year results. International Journal of Prosthodontics19: 236–243. Kaufmann, R., Friedli, M., Hug, S. & Mericske-Stern, R. (2009) Removable dentures with implant support in strategic positions followed for up to 8 years. International Journal of Prosthodontics
22: 233–241.
Klinge, B., Meyle, J. & Working Group 2 (2012) Peri-implant tissue destruction. The Third EAO Consensus Conference 2012. Clinical Oral Implants Research23: 108–110.
Koller, B., Att, W. & Strub, J. (2011) Survival rates of teeth, implants, and double crown-retained removable dental prostheses: a systematic litera-ture review.International Journal of Prosthodon-tics2: 109–117.
Krennmair, G., Krainh€ofner, M., Waldenberger, O. & Piehslinger, E. (2007) Dental implants as stra-tegic supplementary abutments for implant-tooth-supported telescopic crown-retained maxil-lary dentures: a retrospective follow-up study for up to 9 years. International Journal of Prostho-dontics20: 617–622.
Krennmair, G., Sut€€o, D., Seemann, R. & Piehsling-er, E. (2012) Removable four implant-supported mandibular overdentures rigidly retained with telescopic crowns or milled bars: a 3-year pro-spective study. Clinical Oral Implants Research
23: 481–488.
Lang, N.P. & Berglundh, T. (2011) Peri-implant dis-eases: where are we now? Consensus of the sev-enth European workshop on periodontology. Journal of Clinical Periodontology38(Suppl.): 11. Lang, N.P., Pjetursson, B.E., Tan, K., Br€agger, U.,
Egger, M. & Zwahlen, M. (2004) A systematic review of the survival and complication rates of fixed partial dentures (FPDs) after an observation period of at least 5 years. II. Combined tooth– implant-supported FPDs. Clinical Oral Implants Research15: 643–653.
Lee, D.W. (2011) Validated surrogate endpoints needed for peri-implantitis.Evidence-Based Den-tistry1: 7.
Lindhe, J. & Meyle, J. (2008) Peri-implant diseases: consensus report of the sixth European workshop on periodontology.Journal of Clinical Periodon-tology35(Suppl. 8): 282–285.
Mackie, A., Lyons, K., Thomson, W.M. & Payne, A.G. (2011) Mandibular two-implant overden-tures: prosthodontic maintenance using different loading protocols and attachment systems. International Journal of Prosthodontics 24: 405–416.
Mengel, R., Lehmann, K.M., Metke, W., Wolf, J. & Flores-de-Jacoby, L. (2002) A telescopic crown concept for the restoration of partially edentulous patients with aggressive generalized periodontitis: two case reports. International Journal of Periodontics and Restorative Dentistry 22: 129–137.
Mombelli, A., M€uller, N. & Cionca, N. (2012) The epidemiology of peri-implantitis. Clinical Oral Implants Research23: 67–76.
Naert, I., Alsaadi, G., van Steenberghe, D. & Quiry-nen, M. (2004) A 10-year randomized clinical trial on the influence of splinted and unsplinted oral implants retaining mandibular overdentures: peri-implant outcome. International Journal of Oral and Maxillofacial Implants19: 695–702. Nickenig, H.J., Sch€afer, C. & Spiekermann, H.
(2006) Survival and complication rates of com-bined tooth-implant-supported fixed partial den-tures.Clinical Oral Implants Research17: 506– 511.
Nickenig, H.J., Spiekermann, H., Wichmann, M., Andreas, S.K. & Eitner, S. (2008) Survival and complication rates of combined tooth-implant-supported fixed and removable partial dentures. International Journal of Prosthodontics21: 131– 137.
Oetterli, M., Kiener, P. & Mericske-Stern, R. (2001) A longitudinal study on mandibular implants supporting an overdenture: the influence of reten-tion mechanism and anatomic-prosthetic vari-ables on periimplant parameters. International Journal of Prosthodontics14: 536–542.
Pjetursson, B.E. & Lang, N.P. (2008) Prosthetic treatment planning on the basis of scientific evi-dence. Journal of Oral Rehabilitation 35(Suppl. 1): 72–79.
Quigley, G.A. & Hein, J.W. (1962) Comparative cleansing efficiency of a manual and power brushing.Journal of the American Dental Associ-ation65: 26–29.
Rentsch-Kollar, A., Huber, S. & Mericske-Stern, R. (2010) Mandibular implant overdentures followed for over 10 years: patient compliance and pros-thetic maintenance. International Journal of Prosthodontics23: 91–98.
Rinke, S., Ohl, S., Ziebolz, D., Lange, K. & Eick-holz, P. (2011) Prevalence of periimplant disease in partially edentulous patients: a practice-based cross-sectional study. Clinical Oral Implants Research22: 826–833.
Schwarz, S., Bernhart, G., Hassel, A.J. & Rammels-berg, P. (2012) Survival of double-crown-retained dentures either tooth-implant or solely implant-supported: an 8-year retrospective study.Clinical Implant Dentistry and Related Researchdoi: 10. 1111/cid.12023. [Epub ahead of print].
Verma, R., Joda, T., Br€agger, U. & Wittneben, J.G. (2013) A systematic review of the clinical perfor-mance of tooth-retained and implant-retained dou-ble crown prostheses with a follow-up of≥3 years. Journal of Prosthodontics1: 2–12.
Wagner, B. & Kern, M. (2000) Clinical evaluation of removable partial dentures 10 years after inser-tion. Success rates, hygienical problems and technical failures.Clinical Oral Investigations4: 74–80.
Weinl€ander, M., Piehslinger, E. & Krennmair, G. (2010) Removable implant-prosthodontic rehabili-tation of the edentulous mandible: five-year results of different prosthetic anchorage concepts. International Journal of Oral and Maxillofacial Implants25: 589–597.
Wenz, H.J., Hertrampf, K. & Lehmann, K.M. (2001) Clinical longevity of removable partial dentures retained by telescopic crowns: outcome of the double crown with clearance fit. International Journal of Prosthodontics14: 207–213.
Wenz, H.J. & Lehmann, K.M. (1998) A telescopic crown concept for the restoration of the partially edentulous arch: the Marburg Double Crown sys-tem.International Journal of Prosthodontics 11: 541–550.
Wolfart, S., Moll, D., Hilgers, R.D., Wolfart, M. & Kern, M. (2013) Implant placement under existing removable dental prostheses and its effect on oral health-related quality of life. Clinical Oral Implants Research24: 1354–1359.
Wostmann, B., Balkenhol, M., Weber, A., Ferger, P.€
& Rehmann, P. (2007) Long-term analysis of tele-scopic crown retained removable partial dentures: survival and need for maintenance. Journal of Dentistry35: 939–945.