ISSN Print: 2164-5329
DOI: 10.4236/wjcd.2019.95028 May 16, 2019 324 World Journal of Cardiovascular Diseases
Development of SIMS (Simple Indigenous
Metallic Stabilizer) for OPCAB
Murali P. Vettath, Kannan Arunachalam Venkatachalam, Nitin Gangadharan,
Madhu Ravisankar, Smera Koroth, Gopalakrishnan Raman
Meitra Hospital, Kozhikode, India
Abstract
Development of a simple, reusable stabilizer for beating heart surgery has been long overdue. Every time a disposable stabilizer is used and discarded, we add to the carbon footprint we leave behind. We had been working on developing such a stabilizer, and had finally come up with a simple indigen-ous (reusable) metallic stabilizer (SIMS). We have used it for over 600 con-secutive off pump coronary artery bypass (OPCAB) with excellent results. The anatomy of the stabilizer is described here along with a comparison of this stabilizer with the commercially available one.
Keywords
SIMS, OPCAB
1. Introduction
OPCAB (off pump coronary artery bypass) has been the standard of care in a few centers around the world. We have been performing the same for over two decades. As one of the pioneers of this technique, we have fabricated, developed, innovated and re-engineered this technique to perform OPCAB in all patients needing CABG (coronary artery bypass grafting) [1]-[7]. We herewith present our recent innovation—A simple indigenous metallic stabilizer (SIMS) which we have used for the past three years. We have compared this with a similar number of OPCABs done using the commercially available stabilizer in the market.
Since the arrival of the first Octopus stabilizer in the market in the late nine-ties, we have been using them to perform OPCAB. In our country, these stabi-lizers have been reused by ethylene oxide sterilization, at an average of about ten times each so that the cost of surgery comes down.
As only 10% - 15% of our population has medical insurance the cost of
sur-How to cite this paper: Vettath, M.P., Venkatachalam, K.A., Gangadharan, N., Ravisankar, M., Koroth, S. and Raman, G. (2019) Development of SIMS (Simple In-digenous Metallic Stabilizer) for OPCAB. World Journal of Cardiovascular Diseases, 9, 324-330.
https://doi.org/10.4236/wjcd.2019.95028
Received: April 11, 2019 Accepted: May 13, 2019 Published: May 16, 2019
Copyright © 2019 by author(s) and Scientific Research Publishing Inc. This work is licensed under the Creative Commons Attribution International License (CC BY 4.0).
DOI: 10.4236/wjcd.2019.95028 325 World Journal of Cardiovascular Diseases
gery is usually borne by the individual. Hence bypass surgeries becomes in af-fordable unless the cost is contained. It has been our endeavor to bring down the cost of cardiac surgery to the minimum, and the development of SIMS has defi-nitely made it possible in a big way.
2. Materials and Method
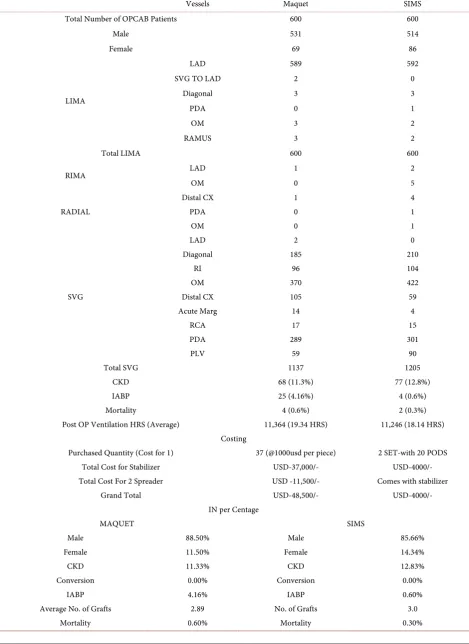
Since 2015, we had started using our SIMS and by the end of 2018 we have used them in over 600 OPCABs. We have compared this with a similar 600 OPCABs performed using the commercially available Maquet stabilizers which we have been using for the last ten years. We have compared the ability of these two sta-bilizers in performing anastomosis in all the walls of the heart and to perform the grafts on all the coronary arteries we needed to graft. The comparative chart is provided in Table 1. We have noticed that both the stabilizers have been pro-ficient in stabilizing in every region of the heart and once we started off with us-ing SIMS, we have never ever had to go back on to these commercially available stabilizers ever again. The way to use this stabilizer is shown in the link provided in the last paragraph.
The interesting aspect is that we have used only two sets of SIMS stabilizers all through to perform these 600 OPCABs, without any need to replace them, and that its still being used. The only part that has to be changed every 5 to 10 cases was the stabilizer pods (Photo 1).
SIMS (simple indigenous metallic stabilizer)
DOI: 10.4236/wjcd.2019.95028 326 World Journal of Cardiovascular Diseases
Table 1. Showing comparison of maquet stabilizer with SIMS.
Vessels Maquet SIMS
Total Number of OPCAB Patients 600 600
Male 531 514
Female 69 86
LIMA
LAD 589 592
SVG TO LAD 2 0
Diagonal 3 3
PDA 0 1
OM 3 2
RAMUS 3 2
Total LIMA 600 600
RIMA LAD 1 2
OM 0 5
RADIAL
Distal CX 1 4
PDA 0 1
OM 0 1
SVG
LAD 2 0
Diagonal 185 210
RI 96 104
OM 370 422
Distal CX 105 59
Acute Marg 14 4
RCA 17 15
PDA 289 301
PLV 59 90
Total SVG 1137 1205
CKD 68 (11.3%) 77 (12.8%)
IABP 25 (4.16%) 4 (0.6%)
Mortality 4 (0.6%) 2 (0.3%)
Post OP Ventilation HRS (Average) 11,364 (19.34 HRS) 11,246 (18.14 HRS)
Costing
Purchased Quantity (Cost for 1) 37 (@1000usd per piece) 2 SET-with 20 PODS
Total Cost for Stabilizer USD-37,000/- USD-4000/-
Total Cost For 2 Spreader USD -11,500/- Comes with stabilizer
Grand Total USD-48,500/- USD-4000/-
IN per Centage
MAQUET SIMS
Male 88.50% Male 85.66%
Female 11.50% Female 14.34%
CKD 11.33% CKD 12.83%
Conversion 0.00% Conversion 0.00%
IABP 4.16% IABP 0.60%
Average No. of Grafts 2.89 No. of Grafts 3.0
DOI: 10.4236/wjcd.2019.95028 327 World Journal of Cardiovascular Diseases
Photo 1. SIMS (simple indigenous metallic stabilizer).
Photo 2. SIMS, a combo device.
DOI: 10.4236/wjcd.2019.95028 328 World Journal of Cardiovascular Diseases
Photo 4. Vertical two inch metallic rod.
Photo 5. The stabilizer rod.
conventional stabilizers, which could be attached to the suction apparatus and used as suction stabilizer as well. Over time, once we get used to the stabilizer we can avoid the suction unless it is absolutely needed.
3. Results
DOI: 10.4236/wjcd.2019.95028 329 World Journal of Cardiovascular Diseases
converted on to the heart lung machine. In fact we had published our last data on our OPCABs which showed that over the last ten years we have had no con-versions on to the Cardio-pulmonary bypass so far [8].
4. Discussion
OPCAB surgery started in the early nineties after Buffalo (1985) and Benetti (1991) reported their individual papers on how they had been able to perform coronary bypass surgery without going on the heart lung machine [9] [10]. These publications stimulated our group to start performing OPCABs in all pa-tients who had to undergo CABG. The Utrecht group published (1996) their se-minal article after which the name Octopus became a name synonymous with beating heart surgery [11]. This was the first commercially available stabilizer that was available to perform OPCAB in all the coronary arteries around the heart. After that many disposable stabilizers came into the market and have re-mained so far. But the need to be able to reuse and recycle these stabilizers made us research for developing an indigenous reusable metallic stabilizer which could be used as any surgical steel instrument [12].
Development of this stabilizer actually brought down our carbon foot print significantly that the last 600 odd patients could undergo OPCAB with the same device and only the pods have been changed frequently. Hence apart from saving on cost incurred per patient, it has also improved our expertise to perform such surgeries. Hence with increasing expertise in OPCAB surgery, we hope that this type of instrumentation would be able to make inroads into developing this specialty and that after a decade on pump CABG would be a thing of the past.
We have also uploaded videos which how SIMS has been used by us in differ-ent positions of the heart in youtube. That can be seen on clicking this link or copy pasting this. The youtube link is
https://www.youtube.com/playlist?list=PLmvb6npEfabinhlatq8IYLBz8WlHo8bu1.
Acknowledgements
We would like to acknowledge the work done by Mr. Arun, who had diligently provided the data work and Mr Bipin, who, worked on the page setting and the photograph. Mr Gopalakrishnan of G&S industries has been the man who made the first Prototype and now the final version on which the stabilizer is now ready for manufacturing. Would like to acknowledge him for his perseverance and hard work, without which this SIMS would not have materialized. Also ac-knowledging the input of Mr Saiju, our surgical asst. and Mr Jayaprakash, our chief perfusionist, who has spend time with us in developing this product.
Conflicts of Interest
DOI: 10.4236/wjcd.2019.95028 330 World Journal of Cardiovascular Diseases
References
[1] Vettath, M.P. (2003) Vettath’s Anastomotic Obturator: A Simple Proximal Anas-tomotic Device. The Heart Surgery Forum, 6.
[2] Vettath, M.P., Kannan, A.V., Sheen Peecheeyen, C.S., Baburajan, A.K., Vahab, A. and Sujith, M.P. (2004) Vettath’s Anastomotic Obturator—Our Experience of 269 Proximal Anastamosis. Heart Lung and Circulation, 13, 288-290.
https://doi.org/10.1016/j.hlc.2004.02.019
[3] Prabhu, A.D., Karim, R.A., Rajendran, S., Thazhkuni, I.E., Thamaran, R.A., Vella-chami, K.A. and Vettath, M.P. (2008) Vettath’s Technique of Long Mammary Patch Reconstruction of a Diffusely Diseased Left Anterior Descending Coronary Artery without Endarterectomy on the Beating Heart. The Heart Surgery Forum, 11, 64-67.
https://doi.org/10.1532/HSF98.20071155
[4] Prabhu, A.D., Thazhkuni, I.E., Rajendran, S., Thamaran, R.A., Vellachamy, K.A. and Vettath, M.P. (2008) Mammary Patch Reconstruction of Left Anterior De-scending Coronary Artery. Asian Cardiovascular and Thoracic Annals, 16, 313-317.
https://doi.org/10.1177/021849230801600412
[5] Vettath, M.P., Ismail, E., Kannan, A. and Murali, A. (2012) Re-Engineering in OPCAB Surgery, Special Topics in Cardiac Surgery, Narin, C., Ed.
http://www.intechopen.com/articles/show/title/re-engineering-in-opcab-off-pump-coronary-artery-bypass-surgery
[6] Vettath, M.P., Ismail, E. and Kannan, A. (2013) Re-Engineering in OPCAB—A Vettath’s Perspective. World Journal of Cardiovascular Disease, 3, 33-44.
https://doi.org/10.4236/wjcd.2013.34A006
[7] Vettath, M., et al. (2016) Role of Intra Aortic Balloon Pump in off Pump Coronary Artery Bypass—A Vettath Modification. World Journal of Cardiovascular Disease, 6, 188-195. https://doi.org/10.4236/wjcd.2016.66020
[8] Vettath, M.P., Ravisankar, M., Kopjar, T., Kannan, A.V. and Gangadharan, N. (2018) The Heart Su Off-Pump Coronary Artery Bypass Grafting Improves Early Clinical Outcomes Including Operative Mortality. The Heart Surgery Forum, 21.
https://doi.org/10.1532/hsf.2007
[9] Buffolo, E., Andrade, J.C.S., Succi, J.E., et al. (1985) Direct Myocardial Revasculari-zation without Cardiopulmonary Bypass. The Thoracic and Cardiovascular Sur-geon, 33, 26-29. https://doi.org/10.1055/s-2007-1014076
[10] Benetti, F.J., Naselli, C., Wood, M. and Geffner, L. (1991) Direct Myocardial Revas-cularization without Extracorporeal Circulation. Experience in 700 Patients. Chest, 100, 312-316. https://doi.org/10.1378/chest.100.2.312
[11] Borst, C., Jansen, E.W., Tulleken, C.A., et al. (1996) Coronary Artery Bypass Graft-ing without Cardiopulmonary Bypass and without Interruption of Native Coronary Flow Using a Novel Anastomosis Site Restraining Device (“Octopus”). Journal of the American College of Cardiology, 27, 1356-1364.
https://doi.org/10.1016/0735-1097(96)00039-3