OSTEOGENIC ACTIVITY ASSOCIATED WITH DENTAL IMPLANT PLACEMENT IN PATIENTS WITH TYPE 2 DIABETES MELLITUS AS COMPARED TO HEALTHY
INDIVIDUALS
Acela A. Martinez Luna
A thesis submitted to the faculty of the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for the degree of Master of Science in the Department of
Periodontology in the School of Dentistry.
Chapel Hill 2015
ii © 2015
iii ABSTRACT
Acela A. Martínez Luna: Osteogenic activity associated with dental implant placement in patients with type 2 diabetes mellitus as compared to healthy individuals.
(Under the direction of Steven Offenbacher)
iv
TABLE OF CONTENTS
LIST OF TABLES …...……….………..…………..……...v
LIST OF FIGURES……….……...vi
LIST OF ABBREVATIONS……….……....vii
CHAPTER I Review: Dental implant therapy in patients with diabetes mellitus.……...………..…..1
Introduction………..………….….1
Effect of diabetes mellitus on wound healing…..…………...….………….….2
Impact of diabetes mellitus on dental implant therapy..………..………….….5
Statement of purpose, hypothesis and specific aims………...12
References……….…...14
II Osteogenic activity associated with dental implant placement in patients with diabetes as compared to healthy individuals………..……..22
Introduction……….…...22
Materials and methods……….……25
Results……….…...28
Discussion………...……….……30
Tables………...38
Figures………..43
v
LIST OF TABLES
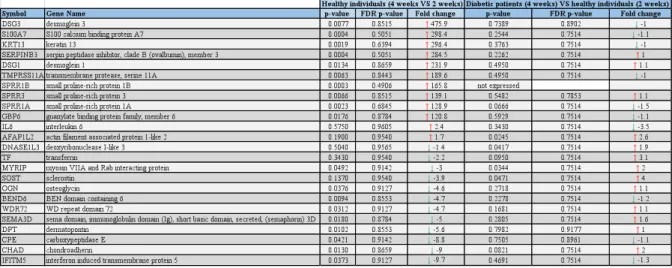
Table 1. Demographic information of the study participants….………..……….…38 Table 2. Expression of top molecules in healthy individuals at 4 weeks as compared to 2
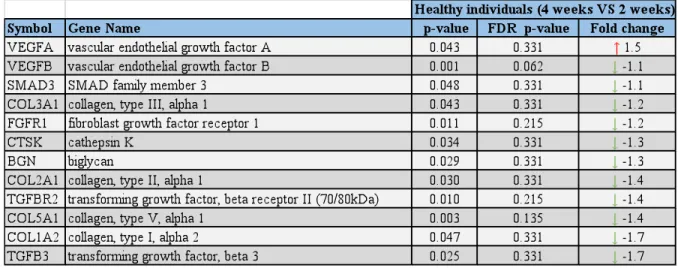
weeks and patients with T2DM at 4 weeks as compared to healthy individuals at 2 weeks…….38 Table 3. Gene expression of human osteogenesis genes at 4 weeks as compared to 2 weeks in healthy individuals……….39 Table 4. Gene expression of human osteogenesis genes comparing patients with T2DM at 4 weeks versus healthy individuals at 2 weeks……….39 Table 5. Gene expression of human osteogenesis genes comparing patients with T2DM
versus healthy individuals at 2 weeks………40 Table 6. Gene expression of human osteogenesis genes comparing patients with T2DM
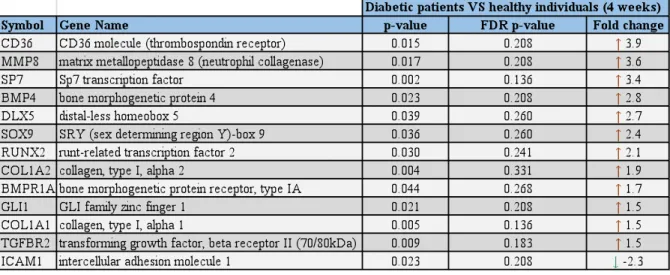
versus healthy individuals at 4 weeks………40 Table 7. Contingency table: patients wth T2DM versus healthy individuals at 4 weeks as
compared to healthy individuals at 4 weeks versus 2 weeks……….41 Table 8. Contingency table: patients wth T2DM versus healthy individuals at 4 weeks as
compared to patients with T2DM at 4 weeks versus healthy individuals at 2 weeks………41 Table 9. Contingency table patients wth T2DM versus healthy individuals at 4 weeks as
vi
LIST OF FIGURES
Figure 1. Human osteogenesis genes and associated canonical pathways (gene expression at 4 weeks as compared to 2 weeks in healthy individuals)………..43 Figure 2. Human osteogenesis genes and associated canonical pathways (gene expression
at 4 weeks in patients with T2DM as compared to healthy individuals at 2 weeks)………….…43 Figure 3. Human osteogenesis genes and associated canonical pathways (gene expression
in patients with T2DM as compared to healthy individuals at 2 weeks)………...44 Figure 4. Human osteogenesis genes and associated canonical pathways (gene expression
vii
LIST OF ABBREVIATIONS AGEs Advanced glycation end products CBCT Cone beam computed tomography DM Diabetes Mellitus
ECM Extracellular matrix FGF Fibroblast growth factor GK Goto-Kazizaki
IGF-1 Insulin-like growth factor 1 IL-1β Interleukin-1 beta
IL-6 Interleukin-6
MMPs Matrix metalloproteinases MMP13 Matrix metallopeptidase 13 MSCs Mesenchymal stem cells NFk-B Nuclear factorkappa B OCN Osteocalcin
OPN Osteoprotegerin
PDGF Platelet derived growth factor
RAGEs Receptors for AGEs
T1DM Type 1 Diabetes Mellitus T2DM Type 2 Diabetes Mellitus
TGF-β1 Transforming growth factor beta 1
1
CHAPTER 1: REVIEW OF DENTAL IMPLANTS IN PATIENTS WITH DIABETES MELLITUS
Introduction
Diabetes mellitus (DM) is a chronic metabolic disorder characterized by hyperglycemia due to impaired insulin secretion, insufficient insulin action or both.1 Type 1 Diabetes Mellitus (T1DM) is characterized by an absolute insulin deficiency and accounts for only 5 to 10% of all patients with DM. Type 2 diabetes mellitus (T2DM) is characterized by impaired insulin function and accounts for 90% to 95% of all patients with DM.2 Patients with DM represent a significant portion of the population. In 2012, 29.1 million Americans, or 9.3% of the population had diabetes. Of the 29.1 million, 21.0 million were diagnosed, and 8.1 million were undiagnosed.3
The number of individuals with DM will continue to increase as the population ages. In this aging population, in which both tooth loss and DM coexist, the need for implant therapy may be the greatest, and they can benefit from an implant-based oral rehabilitation to enhance their well being.4
2
Several studies have demonstrated that successful osseointegration of dental implants could be achieved in diabetic patients with well-controlled glycemic level.7-18 However, other studies, most of which are experimental, have reported that DM could negatively affect the osseointegration of dental implants.19-25
The effect of diabetes mellitus on wound healing
3
collagen in bone resorption is not clear, some studies have shown an increase in osteoclasts and resorptive markers.29,40-42 In contrast, other studies have reported that decreased bone resorption may occur.43-45 Therefore, the role of AGEs on bone resorption are likely most relevant to the inflammatory response.29 Other collagen abnormalities that predispose patients with DM to impaired wound healing have been recognized, including a decrease in collagen synthesis and solubility in gingiva and bone, and an increment in the urinary excretion of hyrdoxyproline, which is a marker of collagen degradation.28
4
5
osseous formation.60,61 Several studies conducted on diabetic animal models to assess fracture healing have reported decreased expression of important mitogenic factors for MSCs during osseous healing such as fibroblast growth factor (FGF)62 and platelet derived growth factor (PDGF),60 and other important growth factors for osteogenesis including transforming growth factor βI (TGF-β1), insulin-like growth factor-1 (IGF-1) and vascular endothelial growth factor (VEGF) at fracture sites.60,61 Another possible explanation of the impaired osseous healing observed in diabetes due to suppressed osteoblastic activity is supported by studies that have reported a decrease in collagen content63,64 and a reduced mRNA expression of OCN,58 which is an important noncollagenous bone matrix protein secreted by osteoblasts. With regard to intramembranous ossification, which is the ossification process seen in the mandible, histological and histomorphometric studies have demonstrated that experimental diabetes impaired the intramembranous bone potential mainly after the first and during the second week of osseous healing.59 Furthermore, experimental diabetes models have demonstrated an alteration of mineral homeostasis and a decrease in osteoid production and bone formation.65-67 Bone turnover is reduced as measured by the percentage of osteoclasts, osteoblats, osteoid surface present, failure to uptake tetracycline labeling and decreases in osteocalcin synthesis.68 Histomorphometry studies have reported diminished bone mineral apposition, osteoid formation and matrix volume.65,69 These studies have also demonstrated impaired microarchitectural bone quality due to poor trabecular connectivity, increased porosity, and lower bone spicule/marrow space ratio.70,71
Impact of diabetes mellitus on dental implant therapy
6
7
8
group as compared with non-diabetic controls.86 Siqueira et al. reported that bone growth area and bone-to-implant contact were not statistically different between the insulin-treated and control groups.75 These studies have demonstrated that the use of insulin around implants may reduce the deleterious effects of diabetes on osseous healing.72
9
10
cytokines act on mesenchymal progenitors by stimulating cell proliferation and inhibiting differentiation. This study proposed that changes in the signaling milieu, might affect the proliferation and differentiation of mesenchymal progenitor cells during the osseointegration phase.93
Pertaining to clinical studies; it has been concluded from retrospective13,14,16 and prospective studies12,15,17,19 that high survival rates may be obtained in patients with diabetes, given that patients present an adequate glycemic control. A retrospective study by Fiorellini et al. showed that implant survival rate was lower in well-controlled diabetic patients as compared to non-diabetic individuals; however there was still a reasonable success rate.94 Oates reported that there are no clear clinical data supporting increased implant failures for patients lacking good glycemic control and, in fact, more recent studies support the used of dental implant therapy for patients in the absence of good glycemic control with appropriate accommodations for delays in implant integration.4
11
rate increased after one year of loading.17 Other than failure rates and implant survival, outcomes of dental implants placed in patients with diabetes have not been studied extensively. According to a meta-analysis by Chrcanovic et al, concerning maginal bone loss, there was a statistically significant difference between diabetic and non-diabetic patients, favoring non-diabetic patients.94 In regard to post-operative infections, few studies have provided information, and therefore a meta-analysis was not possible. 94
The clinical applicability and predictability of dental implants in the healthy patients has been studied and confirmed extensively. Long-term success has been shown utilizing endosseous implants and their predictability relies on successful osseointegration formed during the healing period.6 While experimental models have provided evidence that DM affects the process of ossointegration, the applicability to dental implants placed in human subjects requires caution. Furthermore, the bone formation disturbance reported systemically and locally to the periodontium cannot be assumed to apply to endosseous implants.6 Succesful treatment of patients with diabetes is well documented. However, the impact of DM on osseous healing around dental implants placed on human subjects is unclear. To the best of our knowledge, there are no controlled human studies examining the effects of DM on the implant-bone interphase and early phases of osseointegration.Insufficient information is available to determine how DM affects the process of osseointegration in human subjects. It will be important to examine the molecular pathways that may affect osseointegration,6 in both health and disease.
12
One of the scientific merits of this study is to understand early osseous healing around dental implants at a molecular level in terms of gene expression in human subjects. Furthermore, this study could help understand differences in osseous healing in diabetic patients as compared to healthy individuals. Unraveling the pathways of osseointegration around dental implants will lead to improved treatment strategies to optimize the outcomes, specially in a population that represent the most prevalent diabetes type for which dental therapy is considered. In addition, understanding the systemic conditions that place the patient at a higher risk of implant complications and failure will allow the clinician to make informed decisions and improve the treatment modalities.95
Statements of purpose, hypothesis and specific Aims:
The process of early osseous healing around dental implants in patients with T2DM has not been explored. Previous experimental and clinical studies have shown that DM could affect the stages osseous healing. However, due the heterogeneity of clinical studies and the inability to extrapolate findings from experimental studies, there is not sufficient and conclusive information to understand osseous healing. We are seeking to understand the gene expression and molecular pathways that modulate osseous healing since they are crucial for implant osseointegration and treatment outcomes, and could possible explain the delayed osseous healing observed in patients with diabetes as well as the early or late failures that have been reported in the literature. Two specific aims are developed to test our hypothesis that during the initial phase of wound healing and osseointegration of endosseous dental implants, patients with T2DM will present with delayed osseous healing in comparison to healthy subjects.
13
In this aim, we will first identify differentially expressed genes and those molecular pathways that modulate osseous healing at two and four weeks after implant placement by placing titanium test cylinders that permit vascular and osseous ingrowth in patients with diabetes and healthy subjects. A biological sample obtained from each test cylinder will be processed for RNA extraction and gene expression profiling using Affymetrix (Affymetrix Inc., Santa Clara, CA) recommended procedure and analyzed using Partek and IPA software. Gene expression data seen on the Affymetrix array will be confirmed by PCR array method (SABioscences) for human osteogenesis panel. Patterns in gene expression will help to have an insight into the dynamics of osseous healing response around dental implants.
Aim 2: to compare the differences in the gene expression at two and four weeks after implant placement in patients with T2DM and healthy individuals.
14
REFERENCES
1. King GL. The role of inflammatory cytokines in diabetes and its complications. J Periodontol 2008; 79 Suppl 8:1527-1534.
2. American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2005;28:S37-S-42
3. National Diabetes Statistics Report. 2014 Retrieved from:
http://www.cdc.gov/diabetes/pubs/statsreport14/national-diabetes-report-web.pdf
4. Oates T, Huynh-Ba G, Vargas A, Alexander P, Feine J. A critical review of diabetes, glycemic control, and dental implant therapy. Clin Oral Implants Res 2013;24(2):117-27.
5. Javed F, Romanos GE. Impact of diabetes mellitus and glycemic control on the osseointegration of dental implants: a systematic literature review. J Periodontol 2009;80(11):1719-30.
6. Fiorellini JP, Nevins ML. Dental implant considerations in the diabetic patient. Periodontol 2000 2000;23:73-7.
7. Tawil G, Younan R, Azar P, Sleilati G. Conventional and advanced implant treatment in the type II diabetic patient: surgical protocol and long-term clinical results. Int J Oral Maxillofac
Implants 2008;23(4):744-52.
8. Casap N, Nimri S, Ziv E, Sela J, Samuni Y. Type 2 diabetes has minimal effect on osseointegration of titanium implants in Psammomys obesus. Clin Oral Implants Res 2008;19(5):458-64.
9. Balshi SF, Wolfinger GJ, Balshi TJ. An examination of immediately loaded dental implant stability in the diabetic patient using resonance frequency analysis (RFA). Quintessence Int 2007;38(4):271-9.
10. Kwon PT, Rahman SS, Kim DM, Kopman JA, Karimbux NY, Fiorellini JP. Maintenance of osseointegration utilizing insulin therapy in a diabetic rat model. J Periodontol 2005;76(4):621-6.
11. Siqueira JT, Cavalher-Machado SC, Arana-Chavez VE, Sannomiya P. Bone formation around titanium implants in the rat tibia: role of insulin. Implant Dent 2003;12(3):242-51.
12. Peled M, Ardekian L, Tagger-Green N, Gutmacher Z, Machtei EE. Dental implants in patients with type 2 diabetes mellitus: A clinical study. Implant Dent 2003;12:116-122.
15
14. Abdulwassie H, Dhanrajani PJ. Diabetes mellitus and dental implants: A clinical study.
Implant Dent 2002;11:83-86.
15. Olson JW, Shernoff AF, Tarlow JL, Colwell JA, Scheetz JP, Bingham SF. Dental endosseous implant assessments in a type 2 diabetic population: A prospective study. Int J Oral Maxillofac
Implants 2000;15:811-818.
16. Balshi TJ, Wolfinger GJ. Dental implants in the diabetic patient: A retrospective study.
Implant Dent 1999;8:355-359.
17. Shernoff AF, Colwell JA, Bingham SF. Implants for type II diabetic patients: Interim report. VA Implants in Diabetes Study Group. Implant Dent 1994;3:183-185.
18. Ferreira SD, Silva GL, Cortelli JR, Costa JE, Costa FO. Prevalence and risk variables for peri-implant disease in Brazilian subjects. J Clin Periodontol 2006;33:929-935.
19. Morris HF, Ochi S, Winkler S. Implant survival in patients with type 2 diabetes. Ann
Periodontol 2000;5(1):157-65.
20. Messer RL, Tackas G, Mickalonis J, Brown Y, Lewis JB, Wataha JC. Corrosion of machined titanium dental implants under inflammatory conditions. J Biomed Mater Res B Appl Biomater 2009;88:474-481.
21. Hasegawa H, Ozawa S, Hashimoto K, Takeichi T, Ogawa T. Type 2 diabetes impairs implant osseointegration capacity in rats. Int J Oral Maxillofac Implants 2008;23:237-246.
22. Alsaadi G, Quirynen M, Komárek A, van Steenberghe D. Impact of local and systemic factors on the incidence of oral implant failures, up to abutment connection. J Clin Periodontol 2007;34:610-617.
23. McCracken MS, Aponte-Wesson R, Chavali R, Lemons JE. Bone associated with implants in diabetic and insulin-treated rats. Clin Oral Implants Res 2006;17:495-500.
24. Kopman JA, Kim DM, Rahman SS, Arandia JA, Karimbux NY, Fiorellini JP. Modulating the effects of diabetes on osseointegration with aminoguanidine and doxycycline. J Periodontol 2005;76:614-620.
16
27. Buccala R, Makita Z, Kochisnky T, Cerami A, Vlassara H. Lipid advanced glycosylation: pathway for lipid oxidation in vivo. Proc Natl Acad Sci U S A 1993;90:6434-8.
28. Ryan ME, Carnu O, Kamer A. The influence of diabetes on the periodontal tissues. J Am
Dent Assoc 2003;134:34S-40S.
29. Mealey BL, Oates TW. Diabetes mellitus and periodontal diseases. J Periodontol 2006;77(8):1289-303.
30. Weiss RE, Gorn A, Nimni ME. Abnormalities in the biosynthesis of cartilage and bone proteoglycans in experimental diabetes. Diabetes 1981;30:670-77.
31. Monnier VM, Glomb M, Elgawish A, Sell DR. The mechanism of collagen cross-linking in diabetes. A puzzle nearing resolution. Diabetes 1996;45(Suppl. 3):S67-S72.
32. Monnier VM, Khon RB, Cerami A. Accelerated age related browning of human collagen in diabetes mellitus. Proc Natl Acad Sci U S A 1984;81:583-87.
33. Spanhaimer RG. Direct inhibition of collagen production in vitro by diabetic rat serum.
Metabolism 1988;37:479-85.
34. Wang X, Shen X, Li X, Agrawal CM. Age-related changes in the collagen network and toughness of bone. Bone 2002;31:1-7.
35. Vashisht D, Gibson GJ, Khoury JI, Schaffler MB, Kimura J, Fyhrie DP. Influence of nonenzymatic glycation on biomechanical properties of cortical bone. Bone 2001;28:195-201. 36. Verzijl N, DeGroot J, Ben ZC, et al. Crosslinking by advanced glycation end products increases the stiffness of the collagen network in human articular cartilage: A possible
mechanism through which age is a risk factor for osteoarthritis. Arthritis Rheum 2002;46:114-123.
37. Gunczler P, Lanes R, Paoli M, Martinis R, Villaroel O, Weisinger JR. Decreased bone mineral density and bone formation markers shortly after diagnosis of clinical type 1 diabetes mellitus. J Pediatr Endocrinol Metab 2001;14:525-528.
38. McCarthy AD, Etcheverry SB, Bruzzone L, Lettierri G, Barrio DA, Cortizo AM. Non-enzymatic glycosylation of a type I collagen matrix: Effects on osteoblastic development and oxidative stress. BMC Cell Biol 2001;2:16-21.
39. Santana RB, Xu L, Chase HB, Amar S, Graves DT, Trackman PC. A role for advanced glycation end products in diminished bone healing in type 1 diabetes. Diabetes 2003;52:1502-1510.
17
41. Valerio G, Franzese A, Esposito-Del Puente A, et al. Increased urinary excretion of collagen crosslinks in type 1 diabetic children in the first 5 years of disease. Horm Res 1999;51:173-177. 42. Okazaki R, Totsuka Y, Hamano K, et al. Metabolic improvement of poorly controlled noninsulin-dependent diabetes mellitus decreases bone turnover. J Clin Endocrinol Metab 1997;82:2915-2920.
43. Okazaki R, Miura M, Toriumi M, et al. Short-term treatment with troglitazone decreases bone turnover in patients with type 2 diabetes mellitus. Endocr J 1999;46:795-801.
44. Erbagci AB, Araz M, Ergabci A, Tarakcioglu M, Namiduru ES. Serum prolidase activity as a marker of osteoporosis in type 2 diabetes mellitus. Clin Biochem 2002;35:263-268.
45. Cloos C, Wahl P, Hasslacher C, et al. Urinary glycosylated, free and total pyridinolines and free and total deoxypyridinoline in diabetes mellitus. Clin Endocrinol (Oxf) 1998;48:317-323. 46. Schmidt AM, Hori O, Cao R, et al. RAGE: A novel cellular receptor for advanced glycation end products. Diabetes 1996;45(Suppl. 3):S77-S80.
47. Schmidt AM, Yan SD, Wautier J-L, Stern D. Activation of receptor for advanced glycation end products. A mechanism for chronic vascular dysfunction in diabetic vasculopathy and atherosclerosis. Circ Res 1999;84:489-497
48. Frantzis T, Reeve C, Brown A Jr. The ultrastructure of capillary basement membranes in the attached gingiva of diabetic and nondiabetic patients with periodontal disease. J Periodontol 1971;42:406-11.
49. Schmidt A, Hasu M, Popov D, et al. Receptor for advanced glycation end products (AGEs) has a central role in vessel wall interactions and gene activation in response to circulating AGE-proteins. Proc Natl Acad Sci U S A 1994;91:8807-11.
50. Schmidt A, Hori O, Chen J, Brett J, Stern D. AGE interaction with their endothelial receptors induce expression of VCAM-1: a potential mechanism for the accelerated vasculopathy of diabetes. J Clin Invest 1995;96:1375-403.
51. Schmidt A, Weidman E, Lalla E, et al. Advanced glycation end-products (AGEs) induce oxidant stress in the gingiva: a potential mechanism underlying accelerated periodontal disease associated with diabetes. J Periodontal Res 1996;31:508-15.
52. Soory M. Hormone mediation of immune response in the progession of diabetes, rheumatoid arthritis and periodontal diseases. Curr Drug Targets Immune Endocr Metabol Disord
2002;2:13-25.
18
54. Balint E, Szabo P, Marshall C, Sprague SM. Glucose-induced inhibition of in vitro bone mineralization. Bone 2001;28(1):21-8
55. Zayzafroon M, Botolin S, McCabe LR. P38 and activating transcription factor-2 involvement in osteoblast osmotic response to elevated extracellular glucose. J Biol
Chem 2002;277(40):37212-8.
56. McCabe LR. Understanding the pathology and mechanisms of type I diabetic bone loss. J
Cell Biochem 2007;102:1343-57.
57. Weiss RE, Reddi AH. Influence of experimental diabetes and insulin on matrix-induced cartilage and bone differentiation. Am J Physiol 1980;238(3):E200-7.
58. Lu H, Kraut D, Gerstenfeld LC, Graves DT. Diabetes interferes with the bone formation by affecting the expression of transcription factors that regulate osteoblast differentiation.
Endocrinology 2003;144(1):346-52.
59. Retzepi M, Donos N. The effect of diabetes mellitus on osseous healing. Clin Oral Implants Res 2010;21(7):673-81.
60. Tyndall WA, Beam HA, Zarro C, O'Connot JP, Lin SS. Decreased platelet derived growth factor expression during fracture healing in diabetic animals. Clin Orthop Relat Res
2003;(408):319-30.
61. Gandhi A, Beam HA, O'Connor JP, Parsons JR, Lin SS. The effects of local insulin delivery on diabetic fracture healing. Bone 2005;37(4):482-90.
62. Kawaguchi H, Kurokawa T, Hanada K, Hiyama Y, Tamura M, Ogata E, Mastumoto T. Stimulation of fracture repair by recombinant human basic fibroblast growth factor in normal and streptozotocin-diabetic rats. Endocrinology 1994 Aug;135(2):774-81.
63. Macey LR, Kana SM, Jungishi S, Terek RM, Borretos J, Bolander ME. Defects of early fracture-healing in experimental diabetes. J Bone Joint Surg Am 1989;71(5):722-33.
64. Topping RE, Bolander ME, Balian G. Type X collagen in fracture callus and the effects of experimental diabetes. Clin Orthop Relat Res 1994;(308):220-8.
65. Goodman WG, Hori MT. Diminished bone formation in experimental diabetes. Relationship to osteoid maturation and mineralization. Diabetes 1984;33(9):825-31.
19
67. Shires R, Teitelbaum SL, Bergfeld MA, Fallon MD, Slatopolsky E, Avioli LV. The effect of streptozotocin-induced chronic diabetes mellitus on bone and mineral homeostasis in the rat. J
Lab Clin Med 1981;97(2):231-40.
68. Verhaeghe J, Suiker AM, Nyomba BL, Visser WJ, Einhorn TA, Dequeker J, Bouillon R. Bone mineral homeostasis in spontaneously diabetic BB rats. II. Impaired bone turnover and decreased osteocalcin synthesis. Endocrinology 1989;124(2):573-82.
69. Verhaeghe J, van Herck E, Visser WJ, Suiker AM, Thomasset M, Einhorn TA, Faierman E, Bouillon R. Bone and mineral metabolism in BB rats with long-term diabetes. Decreased bone turnover and osteoporosis. Diabetes 1990;39(4):477-82.
70. Hou JC, Zernicke RF, Barnard RJ. Effects of severe diabetes and insulin on the femoral neck of the immature rat. J Orthop Res 1993;11(2):263-71.
71. Suzuki K, Miyakoshi N, Tsuchida T, Kasukawa Y, Sato K, Itoi E. Effects of combined treatment of insulin and human parathyroid hormone (1-34) on cancellous bone mass and structure in streptozotocin-induced diabetic rats. Bone 2003;33(1):108-14.
72. Kotsovilis S, Karoussis IK, Fourmousis I. A comprehensive and critical review of dental implant placement in diabetic animals and patients. Clin Oral Implants Res 2006;17(5):587-99. 73. Iyama S, Takeshita F, Ayukawa Y, Kido MA, Suetsugu T, Tanaka T. A study of the regional distribution of bone formed around hydroxyapatite implants in the tibiae of
streptozotocin-induced diabetic rats using multiple fluorescent labeling and confocal laser scanning microscopy.
J Periodontol 1997;68(12):1169-75.
74. Giglio MJ, Giannunzio G, Olmedo D, Guglielmotti MB. Histomorphometric study of bone healing around laminar implants in experimental diabetes. Implant Dent 2000;9(2):143-9. 75. Siqueira JT, Cavalher-Machado SC, Arana-Chavez VE, Sannomiya P. Bone formation around titanium implants in the rat tibia: role of insulin. Implant Dent 2003;12(3):242-51. 76. Ottoni CE, Chopard RP. Histomorphometric evaluation of new bone formation in diabetic rats submitted to insertion of temporary implants. Braz Dent J 2004;15(2):87-92.
77. Takeshita F, Iyama S, Ayukawa Y, Kido MA, Murai K, Suetsugu T. The effects of diabetes on the interface between hydroxyapatite implants and bone in rat tibia. J Periodontol
1997;68(2):180-5.
78. Takeshita F, Murai K, Iyama S, Ayukawa Y, Suetsugu T. Uncontrolled diabetes hinders bone formation around titanium implants in rat tibiae. A light and fluorescence microscopy, and image processing study. J Periodontol 1998;69(3):314-20.
79. McCracken M1, Lemons JE, Rahemtulla F, Prince CW, Feldman D. Bone response to
20
80. Gerritsen M, Lutterman JA, Jansen JA. Wound healing around bone-anchored percutaneous devices in experimental diabetes mellitus. J Biomed Mater Res 2000;53(6):702-9.
81. Retzepi M1, Lewis MP, Donos N. Effect of diabetes and metabolic control on de novo bone formation following guided bone regeneration. Clin Oral Implants Res 2010;21(1):71-9
82. Canalis E. Effect of insulinlike growth factor I on DNA and protein synthesis in cultured rat calvaria. J Clin Invest 1980;66(4):709-19.
83. Glajchen N, Epstein S, Ismail F, Thomas S, Fallon M, Chakrabarti S. Bone mineral metabolism in experimental diabetes mellitus: osteocalcin as a measure of bone remodeling.
Endocrinology 1988;123(1):290-5.
84. Ishida H, Seino Y, Taminato T, Usami M, Takeshita N, Seino Y, Tsutsumi C, Moriuchi S, Akiyama Y, Hara K, et al. Circulating levels and bone contents of bone gamma-carboxyglutamic acid-containing protein are decreased in streptozocin-induced diabetes. Possible marker for diabetic osteopenia. Diabetes 1988;37(6):702-6.
85. Locatto ME, Abranzon H, Caferra D, Fernandez MC, Alloatti R, Puche RC. Growth and development of bone mass in untreated alloxan diabetic rats. Effects of collagen glycosylation and parathyroid activity on bone turnover. Bone Miner 1993;23(2):129-44.
86. Fiorellini JP, Nevins ML, Norkin A, Weber HP, Karimbux NY.
The effect of insulin therapy on osseointegration in a diabetic rat model. Clin Oral Implants Res 1999;10(5):362-8.
87. Iwase M, Uchizono Y, Tashiro K, Goto D, Iida M. Islet hyperperfusion during prediabetic phase in OLETF rats, a model of type 2 diabetes. Diabetes 2002;51(8):2530-5.
88. Komaki K, Ohno Y, Aoki N. Gonadal hormones and gonadal function in type 2 diabetes model OLETF (Otsuka Long Evans Tokushima Fatty) rats. Endocr J 2005;52(3):345-51. 89. Jia D, Taguchi M, Otsuki M. Synthetic protease inhibitor camostat prevents and reverses dyslipidemia, insulin secretory defects, and histological abnormalities of the pancreas in genetically obese and diabetic rats. Metabolism 2005;54(5):619-27.
90. Yamamoto M, Jia DM, Fukumitsu KI. Imoto I, Kihara Y, Hirohata Y, Otsuki M.
Metabolic abnormalities in the genetically obese and diabetic Otsuka Long-Evans Tokushima Fatty rat can be prevented and reversed by alpha-glucosidase inhibitor. Metabolism
1999;48(3):347-54.
21
92. Wang F, Song YL, Li DH, Li CX, Wang Y, Zhang N, Wang BG. Type 2 diabetes mellitus impairs bone healing of dental implants in GK rats. Diabetes Res Clin Pract 2010;88(1):e7-9.
93. Wang F, Song YL, Li DH, Li CX, Wang Y, Zhang N, Wang BG. Type 2 diabetes mellitus impairs bone healing of dental implants in GK rats. Diabetes Res Clin
Pract 2010;88(1):e7-9.
94. Fiorellini JP, Chen PK, Nevins M, Nevins ML. A retrospective study of dental implants in diabetic patients. Int J Periodontics Restorative Dent 2000;20(4):366-73.
95. Chrcanovic BR, Albrektsson T, Wennerberg A. Diabetes and oral implant failure: a systematic review. J Dent Res 2014;93(9):859-67.
22
CHAPTER 2: OSTEOGENIC ACTIVITY ASSOCIATED WITH DENTAL IMPLANT PLACEMENT IN PATIENTS WITH TYPE 2 DIABETES
MELLITUS AS COMPARED TO HEALTHY INDIVIDUALS Introduction
Diabetes mellitus (DM) is a chronic metabolic disorder characterized by hyperglycemia due to impaired insulin secretion, insufficient action or both.1 Type 2 diabetes mellitus (T2DM) is characterized by impaired insulin function and accounts for 90 to 95% of patients with diabetes.2 In the aging population, in which both tooth loss and DM coexist, the need for oral rehabilitation with dental implants is high.3 The use of dental implants in patients with DM is a debatable issue due to the adverse effects of hyperglycemia on osseointegration.4 The predictability of implant therapy relies on the osseointegration formed during the healing period,5 and the critical dependence on bone metabolism for implant survival may be heightened in patients with DM.3
23
elimination of metabolic waste.9,10 The interaction of AGEs with RAGEs present in monocytes causes an increase in cellular oxidant stress and activation of NF-kB, which alters the monocyte/macrophage phenotype resulting in an increase of pro-inflammatory cytokines (IL-1β, TNF-α,7,8 IL-611), MMPs and adhesion molecules.12 An overproduction of these products can amplify the inflammatory response, delaying wound healing and inducing bone resorption and connective tissue damage.13 Furthermore, increased levels of AGEs in bone collagen may affect cellular, structural, and functional characteristics leading to alterations in bone metabolism.14-16
The effect of DM on osseous healing has been extensively studied; models of experimentally induced diabetes have shown decreased cellularity and impaired osteoid matrix formation during the early phases of osseous healing possible due to a defficit in the recruitment of mesenchymal stem cells (MSCs) in the osteoblastic lineage, impaired differentiation and proliferation, and suppresed osteoblastic activity.17,18 Decreased expression of transcription factors necessary for the acquisition of the osteoblastic phenotype has been observed in the early phase of intramembranous ossification suggesting a possible mechanism for the impaired commitment of MSCs in the osteoblastic lineage.19 Plausible mechanism responsible for the reduction in cell proliferation is that DM may downregulate pathways involved in cell division, energy production and osteogenesis during the proliferative phase of intramembranous bone healing.20 Also, DM may decrease the levels of growth factors involved in early osteogenesis by altering the normal progression of the inflammatory phase and osseous formation. 21, 22
24
bone formation,27 reduced bone-to-implant contact25-30, and decreased alkaline phosphatase levels.30 However, no infectious complications or implant loss were associated to diabetes in animal models, suggesting that osseointegration can be accomplished even though they presented with impaired bone healing.25,31 Most of the experimental studies on diabetes have been conducted in proven models for T1DM; even though they represent a hyperglycemic state, they do not represent the most prevalent diabetes type for which implant therapy in humans is considered. Later investigations have studied the effect of diabetes on implant osseointegration in experimental T2DM models,32-34 and reported smaller volume of peri-implant cortical bone,32 decreased bone-to-implant contact,32,33 decreased maturation,33 delayed bone mineralization and expression of TGF-B1,34 and elevated levels of pro-inflammatory cytokines.34
In regard to clinical studies; it has been concluded from retrospective35-37 and prospective studies38-41 that high survival rates may be obtained in patients with DM. Some clinical studies reported some early implant failures before osseointegration could be established.35-40 However, other studies have reported later failures40,42 that could be attributed to a mechanical overload, caused by a diabetes-induced lower percetage bone-to implant contact, immature, or incorrectly formed bone.42
25
To the best of out knowledge, there are no human studies examining the effects of DM on the implant implant-bone interphase at the early stages of osseointegration in terms of gene expression and pathway analysis. Furthermore it is important to examine the molecular pathways that modulate implant osseointegration5 in both health and disease to understand and explain the delayed osseous healing observed in patients with diabetes as well as the early or late failures that have been reported in the literature.
In this study we are aiming to identify differentially expressed genes and those molecular pathways that modulate osseous healing around dental implants in bone biopsies obtained from healthy individuals and patients with T2DM at two and four weeks after implant placement. We are also seeking to compare the differences between patients with T2DM and healthy individuals to test our hypothesis that during the initial phase of wound healing and osseointegration of endosseous dental implants, patients with T2DM will present with delayed osseous healing as compared to healthy subjects.
Materials and Methods
Participants and bone biopsy collection
26
bisphosphonates, active infectious disease, pregnancy, current smokers or history of smoking within the last two years, subjects with blood disorders and/or anticoagulant therapy, chemotherapy, and radiotherapy. An edentulous ridge area with sufficient space to place two titanium test cylinders (each approximately 2.9-3 x 5 mm) was confirmed radiographically, followed by a CBCT taken with a radiographic stent. For each patient, two titanium test cylinders were placed on the mandible at the level of the crestal bone and covered with a collagen membrane (BioMend, Zimmer Dental, Carlsbad, CA, USA) to prevent soft tissue downgrowth, primary closure was obtained. Test cylinders were removed at two and four weeks using a slightly larger trephine drill and sites received a screw vent implant (Zimmer Dental, Carlsbad, CA, USA). Each test cylinder was placed into microfuge tubes containing RNAlater solution and temporarily stored at 4ºC overnight. The next morning, the solution was decanted and the samples were flash frozen in liquid nitrogen and stored at -80ºC until analysis.
RNA isolation and quality control
Total RNA was isolated from the bone biopsies using a miRNAeasy Mini Kit (QIAgen, Valencia, CA, USA) according to the manufacturer's instructions. RNA quality and purity were analized by spectophotometer using the NanoDrop ND-1000 and Agilent 2100 Bioanalyzer. Gene expression analysis
27 Quantitative Real-time PCR
Gene expression data seen on the Affymatrix arrays was confirmed with quantitative real-time PCR. RNA was reverse transcribed to cDNA using RT2 first strands kit (QIAgen, Valencia, CA, USA). To examine genes of interest, we used human osteogenesis RT2 Profiler PCR Array (PAHS-026Z) in a 7500 Sequence Detection system (ABI prism, Applied Biosystems). The human osteogenesis panel included the following functional gene groups: skeletal development, bone mineral metabolism, cell growth and differentiation, extracellular matrix molecules and transcription factors and regulators.
Statistics
28
PCR array data analysis version 3.5. We also used the Chi square test for proportions to determine whether T2DM influenced gene expression of genes involved in human osteogenesis. Results
Demographic information of the study participants
The demographic information, including age, gender and race are listed in Table 1. The mean age of the study participants was 63.7+5.8 years. There was an even sex distribution and the study group consisted of 7 Caucasians and 3 African Americans.
Expression of top molecules obtained from Affymetrix analysis
29
downregulated at 4 weeks in both healthy and diabetic groups; this downregulation was only statistically significant in the healthy group (p<0.05). None of these molecules had a FDR p-value of <0.05.
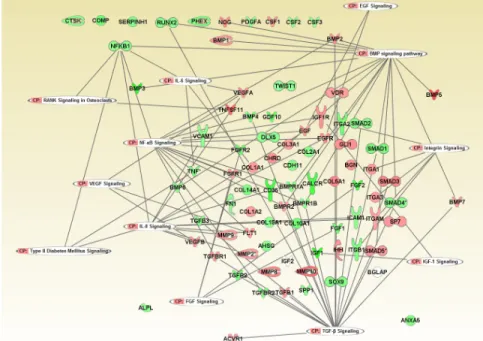
Expression of genes involved in human osteogenesis obtained from Affymetrix analysis To obtain an insight of the gene expression and associated pathways involved in osteogenesis around dental implants, we analyzed specific genes associated with human osteogenesis and created a pathway using these genes. Also, we included the associated canonical pathways pertinent to healing around endosseous implants. Figure 1 shows the expression of genes associated with human osteogenesis and their interactions in healthy patients at 4 weeks as compared to 2 weeks, showing that the majority of the human osteogenesis genes appeared downregulated at this time point. VEGFB, SMAD3, COL3A1, FGFR1, CTSK, BGN,
COL2A1, TGFBR2, COL5A1, COL1A2 and TGFB3 appeared significantly downregulated and
only VEGFA appeared significantly upregulated (p<0.05, Table 3). Figure 2 shows the gene expression of human osteogenesis genes in patients with T2DM at 4 weeks as compared to healthy patients at 2 weeks; we observed that some genes that appeared downregulated in the healthy group at 4 weeks appeared upregulated in the diabetic group. However, SPP1 and ITGB1 appeared statistically significant downregulated (p<0.05, Table 4), and only SPP1 had a FDR p-value of <0.05. Figure 3 shows the expression of human osteogenesis genes weeks comparing the diabetic group versus the healthy group at the same time point of 2 weeks. BMPR1B,
TGFBR2, CALCR, ANXA5 and IGF1 appeared downregulated in the diabetic group as compared
30
group; CD36, MMP8, SP7, BMP4, DLX5, SOX9, RUNX2, COL1A2, BMPR1A, GLI1, COL1A1 and TGBR appeared upregulated and ICAM1 was downregulated (p<0.05, Table 6), none of these genes had a FDR of p<0.05. To confirm if the osteogenesis pathway was significantly upregulated or downregulated in all our group comparisons, we created Chi square contingency tables for all the possible combinations. However, only in the diabetic group versus the healthy group at 4 weeks, the osteogenesis pathway was statistically significant upregulated when we compared to the healthy group 4 weeks versus two weeks (p<0.001, Table 7), diabetic group at 4 weeks versus healthy group at 2 weeks (p=0.0016, Table 8), and diabetic versus healthy at 2
weeks (p=0.0044, Table 9). Real time quantitative PCR
Using real time PCR we confirmed downregulation of COL1A2, COL2A1, CTSK and upregulation of VEGFA from 2 weeks to 4 weeks after implant placement in healthy individuals. Comparing patients with T2DM versus healthy individuals at 2 weeks, we confirmed that IGF-1 was downregulated in patients with T2DM. We also confirmed that at 4 weeks, patients with T2DM showed upregulation of SP7, COL1A2, COL1A1, CD36, MMP8, BMP4, RUNX2, SOX9, DLX5, and downregulation of ICAM1 as compared to healthy individuals.
Discussion
31
To the best of our knowledge this is the first human study that has analyzed gene expression and molecular pathways after implant placement in healthy and diabetic patients using Affymetrix analysis, and also for a period of more than 2 weeks after implant placement.
In this study, we isolated RNA from bone biopsies obtained from healthy subjects and patients with T2DM at 2 and 4 weeks after titanium test cylinder placement to identify differentially expressed genes and those molecules that modulate osseous healing around dental implants in both health and T2DM. We also compared the differences in the expression of genes involved in human osteogenesis at two and four weeks after implant placement in patients with T2DM as compared to healthy individuals to find a plausible explanation of the delayed osseous healing and the early or late implant failure that has been reported in the literature.
32
33
Using IPA software (QIAgen, Valencia, CA, USA), we created a pathway that included genes involved in human osteogenesis to obtain an insight of the gene expression and changes at 2 and 4 weeks in both health and T2DM. We were not able to find a statistically significant difference in gene expression in the majority of the human osteogenesis genes. However, we observed that in healthy individuals there was a fold change decrease of the majority of the genes at 4 weeks as compared to 2 weeks (Figure 1). In contrast patients with T2DM presented upregulation of key genes involved in increased osteogenesis at 4 weeks as compared to healthy patients at 2 weeks, including PHEX, RUNX2, DLX5, and SP7 (Figure 2). We also observed that when we compared gene expression at 4 weeks in patients with T2DM versus healthy individuals the majority of the genes involved in human osteogenesis appeared upregulated in the diabetic group (Figure 4) These findings suggest that patients with T2DM present with increased osteogenic activity at 4 weeks as compared to healthy subjects, however we speculate that this could reflect that the increased osteogenic activity observed after implant placement in healthy patients occurred before 4 weeks and at this time point they are already showing downregulation. The observations made from this clinical study suggest that patients with T2DM present with delayed osseous healing around dental implants as compared to healthy patients.
34
osteoclasts and involved in bone remodeling and resportion52 presents an upregulation from 4 days to 2 weeks after implant placement,51 followed by a decreased expression at 4 weeks in healthy patients suggesting that the bone remodeling and resorption phase is decreased at 4 weeks after implant placement.
We also confirmed that patients with T2DM presented downregulation of IGF-1 at 2 weeks as compared to healthy individuals. Patients with diabetes present specific alterations in bone metabolism associated with insulin since it stimulates osteoblastic matrix synthesis and indirectly stimulates IGF-1 production by the liver.5 IGF-1 is involved in skeletal system development, blood coagulation, positive regulation of cell proliferation, bone mineralization involved in bone maturation and positive regulation of osteoblast differentiation.53, 54 IGF-1 increases matrix synthesis increasing the number of osteoblasts present and upregulates the function of differentiated osteoblasts.5 Several studies conducted on diabetic animal models that have assessed fracture healing have reported decreased expression of IGF-1 at fracture sites.21,22 The downregulation of IGF-1 seen in patients with T2DM suggest that these patients present an altered bone metabolism that could delay and impair osteogenesis around dental implants.
Furthermore, patients with T2DM presented upregulation of COL1A2, COL1A1, CD36,
MMP8, BMP4, SP7, RUNX2, SOX9, DLX5, and downregulation of ICAM1 at 4 weeks after
35
osteogenesis and increased bone formation.55,56 BMPs are multifunctional cytokines belonging to the TGF-β superfamily, it has been observed that BMP4 is a key factor involved in bone development and repair. 57 BMP4 appears during the stages of periosteal response and primary bone formation during the process of bone fracture healing. Also, BMP4 from the bone matrix stimulates the production of VEGF.57 During osseous formation and fracture healing, a cross-talk is established between osteoblasts and endothelial cells.58 Osteoblast derived VEGFs play an important role in osseous healing since they may act as paracrine factors, modulating endothelial and osteoclast functions and they also act as autocrine factors, modulating osteoblast differentiation.59 VEGFA, that appeared upregulated at 4 weeks as compared to 2 weeks in healthy, is produced by osteoblasts in response to BMPs, couples angiogenesis to bone formation.58
36
speculate that this incresed osteogenic activity occurred before 4 weeks in healthy patients and this accounts for the difference observed at 4 weeks.
In addition a decreased expression of BMPR1B observed at 2 weeks in patients with T2DM, indicates a possible alteration in bone healing since BMPs exert their biologic effects by binding to this receptor, and the BMP signaling pathway induces osteoblastic differentiation through BMPR1B.63 Also, The decreased expression of SPP1 observed in the diabetic group at 4 weeks suggests a possible decrease in bone remodeling and osseous repair. SPP1 has been defined as one of the major noncollagenous bone matrix proteins produced by osteoblasts.64 It appears to form an integral part of the mineralized matrix and is important to cell-matrix interaction. This protein is important in bone remodeling65 as well as fracture repair.66 Even though it is involved with bone resorption; it has a role in osteoblast differentiation and biomineral tissue development.64
37
period of 7 to 14 weeks. However, by studying gene expression in a patient population that presents with delayed wound healing such as T2DM for an extended period of 4 weeks, we found differences in gene expression as compared to healthy individuals.
Conclusion
38
Table 1. Demographic information of the study participants
Table 2. Expression of top molecules in healthy individuals at 4 weeks as compared to 2 weeks and patients with T2DM at 4 weeks as compared to healthy individuals at 2 weeks
39
Table 3. Gene expression of human osteogenesis genes at 4 weeks as compared to 2 weeks in healthy individuals
*ANOVA
Table 4. Gene expression of human osteogenesis genes comparing patients with T2DM at 4 weeks versus healthy individuals at 2 weeks
40
Table 5. Gene expression of human osteogenesis genes comparing patients with T2DM versus healthy individuals at 2 weeks
*ANOVA
Table 6. Gene expression of human osteogenesis genes comparing patients with T2DM versus healthy individuals at 4 weeks.
41
Table 7. Contingency table: patients with T2DM versus healthy individuals at 4 weeks as compared to healthy individuals at 4 weeks versus 2 weeks.
*Chi square test p<0.001, Yates correction p<0.001
Table 8. Contingency table: patients with T2DM versus healthy individuals at 4 weeks as compared to patients with T2DM at 4 weeks versus healthy individuals at 2 weeks
*Chi square test p=0.0016, Yates correction p=0.0017
Table 9. Contingency table: patients with T2DM versus healthy individuals at 4 weeks as compared to patients with T2DM versus healthy individuals at 2 weeks.
42
Table 10. List of genes and corresponding Gene Ontology classification
43
Figure 1. Human osteogenesis genes and associated canonical pathways (gene expression at 4 weeks as compared to 2 weeks in healthy individuals).
44
Figure 3. Human osteogenesis genes and associated canonical pathways (gene expression in patients with T2DM as compared to healthy individuals at 2 weeks).
45
REFERENCES
1. King GL. The role of inflammatory cytokines in diabetes and its complications. J Periodontol 2008;79 Suppl 8:1527-1534.
2. American Diates Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2005;28:S37-S-42
3. Oates T, Huynh-Ba G, Vargas A, Alexander P, Feine J. A critical review of diabetes, glycemic control, and dental implant therapy. Clin Oral Implants Res 2013;24(2):117-27.
4. Javed F, Romanos GE. Impact of diabetes mellitus and glycemic control on the osseointegration of dental implants: a systematic literature review. J Periodontol 2009;80(11):1719-30.
5. Fiorellini JP, Nevins ML. Dental implant considerations in the diabetic patient. Periodontol 2000 2000;23:73-7.
6. Weiss RE, Gorn A, Nimni ME. Abnormalities in the biosynthesis of cartilage and bone proteoglycans in experimental diabetes. Diabetes 1981:30:670-77.
7. Schmidt AM, Hori O, Cao R, et al. RAGE: A novel cellular receptor for advanced glycation end products. Diabetes 1996;45(Suppl. 3):S77-S80.
8. Schmidt AM, Yan SD, Wautier J-L, Stern D. Activation of receptor for advanced glycation end products. A mechanism for chronic vascular dysfunction in diabetic vasculopathy and atherosclerosis. Circ Res 1999;84:489-497
9. Ryan ME, Carnu O, Kamer A. The influence of diabetes on the periodontal tissues. J Am Dent
Assoc 2003;134:34S-40S.
10. Frantzis T, Reeve C, Brown A Jr. The ultrastructure of capillary basement membranes in the attached gingiva of diabetic and nondiabetic patients with periodontal disease. J Periodontol 1971;42:406-11.
11. Schmidt A, Hasu M, Popov D, et al. Receptor for advanced glycation end products (AGEs) has a central role in vessel wall interactions and gene activation in response to circulating AGE-proteins. Proc Natl Acad Sci U S A 1994;91:8807-11.
12. Schmidt A, Hori O, Chen J, Brett J, Stern D. AGE interaction with their endothelial receptors induce expression of VCAM-1: a potential mechanism for the accelerated vasculopathy of diabetes. J Clin Invest 1995;96:1375-403.
46
14. Wang X, Shen X, Li X, Agrawal CM. Age-related changes in the collagen network and toughness of bone. Bone 2002;31:1-7.
15. Vashisht D, Gibson GJ, Khoury JI, Schaffler MB, Kimura J, Fyhrie DP. Influence of nonenzymatic glycation on biomechanical properties of cortical bone. Bone 2001;28:195-201. 16. Verzijl N, DeGroot J, Ben ZC, et al. Crosslinking by advanced glycation end products increases the stiffness of the collagen network in human articular cartilage: A possible
mechanism through which age is a risk factor for osteoarthritis. Arthritis Rheum 2002;46:114-123.
17. McCabe LR. Understanding the pathology and mechanisms of type I diabetic bone loss. J
Cell Biochem 2007;102:1343-57.
18. Weiss RE, Reddi AH. Influence of experimental diabetes and insulin on matrix-induced cartilage and bone differentiation. Am J Physiol 1980;238(3):E200-7.
19. Lu H, Kraut D, Gerstenfeld LC, Graves DT. Diabetes interferes with the bone formation by affecting the expression of transcription factors that regulate osteoblast differentiation.
Endocrinology 2003;144(1):346-52.
20. Retzepi M, Donos N. The effect of diabetes mellitus on osseous healing. Clin Oral Implants Res 2010;21(7):673-81.
21. Tyndall WA, Beam HA, Zarro C, O'Connot JP, Lin SS. Decreased platelet derived growth factor expression during fracture healing in diabetic animals. Clin Orthop Relat Res
2003;(408):319-30.
22. Gandhi A, Beam HA, O'Connor JP, Parsons JR, Lin SS. The effects of local insulin delivery on diabetic fracture healing. Bone 2005;37(4):482-90.
23. Iyama S, Takeshita F, Ayukawa Y, Kido MA, Suetsugu T, Tanaka T. A study of the regional distribution of bone formed around hydroxyapatite implants in the tibiae of
streptozotocin-induced diabetic rats using multiple fluorescent labeling and confocal laser scanning microscopy.
J Periodontol 1997;68(12):1169-75.
24. Ottoni CE, Chopard RP. Histomorphometric evaluation of new bone formation in diabetic rats submitted to insertion of temporary implants. Braz Dent J 2004;15(2):87-92.
47
27. Siqueira JT, Cavalher-Machado SC, Arana-Chavez VE, Sannomiya P. Bone formation around titanium implants in the rat tibia: role of insulin. Implant Dent 2003;12(3):242-51. 28. Takeshita F, Iyama S, Ayukawa Y, Kido MA, Murai K, Suetsugu T. The effects of diabetes on the interface between hydroxyapatite implants and bone in rat tibia. J Periodontol
1997;68(2):180-5.
29. Takeshita F, Murai K, Iyama S, Ayukawa Y, Suetsugu T. Uncontrolled diabetes hinders bone formation around titanium implants in rat tibiae. A light and fluorescence microscopy, and image processing study. J Periodontol 1998;69(3):314-20.
30. McCracken M1, Lemons JE, Rahemtulla F, Prince CW, Feldman D. Bone response to
titanium alloy implants placed in diabetic rats. Int J Oral Maxillofac Implants 2000;15(3):345-54. 31. Gerritsen M, Lutterman JA, Jansen JA. Wound healing around bone-anchored percutaneous devices in experimental diabetes mellitus. J Biomed Mater Res 2000;53(6):702-9.
32. Hasegawa H, Ozawa S, Hashimoto K, Takeichi T, Ogawa T. Type 2 diabetes impairs implant osseointegration capacity in rats. Int J Oral Maxillofac Implants 2008;23:237-246.
33. Wang F, Song YL, Li DH, Li CX, Wang Y, Zhang N, Wang BG. Type 2 diabetes mellitus impairs bone healing of dental implants in GK rats. Diabetes Res Clin Pract 2010;88(1):e7-9.
34. Wang F, Song YL, Li DH, Li CX, Wang Y, Zhang N, Wang BG. Type 2 diabetes mellitus impairs bone healing of dental implants in GK rats. Diabetes Res Clin
Pract 2010;88(1):e7-9.
35. Farzad P, Andersson L, Nyberg J. Dental implant treatment in diabetic patients. Implant Dent 2002;11:262-267.
36. Abdulwassie H, Dhanrajani PJ. Diabetes mellitus and dental implants: A clinical study.
Implant Dent 2002;11:83-86.
37. Balshi TJ, Wolfinger GJ. Dental implants in the diabetic patient: A retrospective study.
Implant Dent 1999;8:355-359.
38. Peled M, Ardekian L, Tagger-Green N, Gutmacher Z, Machtei EE. Dental implants in patients with type 2 diabetes mellitus: A clinical study. Implant Dent 2003;12:116-122.
39. Olson JW, Shernoff AF, Tarlow JL, Colwell JA, Scheetz JP, Bingham SF. Dental endosseous implant assessments in a type 2 diabetic population: A prospective study. Int J Oral Maxillofac
Implants 2000;15:811-818.
48
41. Morris HF, Ochi S, Winkler S. Implant survival in patients with type 2 diabetes. Ann
Periodontol 2000;5(1):157-65.
42. Fiorellini JP, Chen PK, Nevins M, Nevins ML. A retrospective study of dental implants in diabetic patients. Int J Periodontics Restorative Dent 2000;20(4):366-73.
43. Nishimura I. Genetic networks in osseointegration. J Dent Res 2013;92(12 Suppl):109S-18S. 44. Sharifi M, Ereifej L, Lewiecki EM. Sclerostin and skeletal health. Rev Endocr Metab Disord 2015; Feb 12.
45. Kim J, Liu X, Wang J, Chen X, Zhang H, Kim S, et al. Wnt signaling in bone formation and its therapeutic potential for bone diseases. Ther Adv Musculoskelet Dis 2013;5:13–31
46. Ke H, Richards W, Li X, Ominsky M. Sclerostin and Dickkopf-1 as therapeutic targets in bone diseases. Endocr Rev 2012;33:747–83.
47. Li X, Zhang Y, Kang H, et al. Sclerostin binds to LRP5/6 and antagonizes canonical Wnt signaling. J Biol Chem 2005;280(20):19883–7.
48. Semenov M, Tamai K, He X. SOST is a ligand for LRP5/LRP6 and a Wnt signaling inhibitor. J Biol Chem 2005;280(29):26770–5.
49. Van Bezooijen RL, Svensson JP, Eefting D, et al. Wnt but not BMP signaling is involved in the inhibitory action of sclerostin on BMPstimulated bone formation. J Bone Miner Res
2007;22(1):19–28.
50. Van Buchem FS, Hadders HN, Ubbens R. An uncommon familial systemic disease of the skeleton: hyperostosis corticalis generalisata familiaris. Acta Radiol 1955;44(2):109–20. 51.Ivanovski S, Hamlet S, Salvi GE, Huynh-Ba G, Bosshardt DD, Lang NP, Donos N.
Transcriptional profiling of osseointegration in humans. Clin Oral Implants Res 2011;22(4):373-81.
52. Motyckova G, Fisher DE. "Pycnodysostosis: role and regulation of cathepsin K in osteoclast function and human disease." Curr. Mol. Med. 2003;2(5):407–21.
53. De Ranieri A, Virdi AS, Kuroda S, Shott S, Dai Y, Sumner DR. Local application of rhTGF-beta2 modulates dynamic gene expression in a rat implant model. Bone 2005;36(5):931-40. 54. Monjo M, Lamolle SF, Lyngstadaas SP, Rønold HJ, Ellingsen JE. In vivo expression of osteogenic markers and bone mineral density at the surface of fluoride-modified titanium implants. Biomaterials 2008;29(28):3771-80.
49
55. Niyibizi C, Eyre DR. Structural characteristics of cross-linking sites in type V collagen of bone. Chain specificities and heterotypic links to type I collagen. Eur J Biochem
1994;224(3):943-50.
56. Thalji G, Cooper LF. Molecular assessment of osseointegration in vivo: a review of the current literature. Int J Oral Maxillofac Implants 2013;28(6):e521-34.
57. Carreira AC, Lojudice FH, Halcsik E, Navarro RD, Sogayar MC, Granjeiro JM. Bone morphogenetic proteins: facts, challenges, and future perspectives. J Dent Res 2014;93(4):335-45.
58. Deckers MM, van Bezooijen RL, van der Horst G, Hoogendam J, van Der Bent
C, Papapoulos SE, Löwik CW. Bone morphogenetic proteins stimulate angiogenesis through osteoblast-derived vascular endothelial growth factor A. Endocrinology 2002;143(4):1545-53. 59. Deckers MM, Karperien M, van der Bent C, Yamashita T, Papapoulos SE, Löwik CW. Expression of vascular endothelial growth factors and their receptors during osteoblast differentiation. Endocrinology 2000;141(5):1667-74.
60. Deschaseaux F, Sensébé L, Heymann D. Mechanisms of bone repair and regeneration.
Trends Mol Med 2009;15(9):417-29.
61.Nishimura R, Hata K, Matsubara T, Wakabayashi M, Yoneda T. Regulation of bone and cartilage development by network between BMP signalling and transcription factors. J Biochem 2012;151(3):247-54.
62.Takayanagi H. Osteoimmunology and the effects of the immune system on bone. Nat Rev
Rheumatol 2009;5(12):667-76
63. Rigueur D, Brugger S, Anbarchian T, Kim JK, Lee Y, Lyons KM.The Type I BMP Receptor ACVR1/ALK2 is Required for Chondrogenesis During Development. J Bone Miner
Res 2015;30(4):733-41.
64. McKee MD, Glimcher MJ, Nanci A. High-resolution immunolocalization of osteopontin and osteocalcin in bone and cartilage during endochondral ossification in the chicken tibia. Anat Rec 1992;234(4):479-92.
65. Chellaiah MA, Kizer N, Biswas R, Alvarez U, Strauss-Schoenberger J, Rifas L, Rittling SR, Denhardt DT, Hruska KA. Osteopontin deficiency produces osteoclast dysfunction due to reduced CD44 surface expression. Mol Biol Cell 2003;14(1):173-89.
66. Nakase T, Sugimoto M, Sato M, Kaneko M, Tomita T, Sugamoto K, Nomura S, Kitamura Y, Yoshikawa H, Yasui N, Yonenobu K, Ochi T. Switch of osteonectin and osteopontin mRNA expression in the process of cartilage-to-bone transition during fracture repair. Acta