Improving Standardization of Paging
Communication Using Quality
Improvement Methodology
Rachel M. Weigert, MD,aAnna H. Schmitz, MD,bPaula J. Soung, MD,bKelsey Porada, MA,bMichael C. Weisgerber, MDb
abstract
BACKGROUND AND OBJECTIVES:Paging is a primary mode of communication in
hospitals, but message quality varies. With this project, we aimed to
standardize paging, thus improving end user (EU) satisfaction, patient safety, and efficiency. Objectives were to increase the percent of pages containing 6 critical elements (CEs) (ie, the sender’sfirst and last name, a 7-digit callback number, patient name, room number, and urgency indicator [information only, call, or come] to 90%); improve EU satisfaction to 80% rating paging communication as good or excellent; and decrease the frequency of safety events related to paging.
METHODS:This multidisciplinary, system-wide quality improvement study was
conducted at our stand-alone academic children’s hospital. CEs were determined by EU consensus. Outcome measures were inclusion of all 6 CEs, provider satisfaction, and frequency of safety events. Process measures were inclusion of individual CEs and appropriateness and timeliness of response to pages. Balancing measures included number of work-arounds (WAs). Interventions included education, engineering a platform with requiredfields, and optimization enhancements. Statistical process control charts (p-charts; XmR) were used to track the impact of interventions.
RESULTS:Special-cause improvement was noted in use of all 6 CEs
(4.4%–79.7%) and individual CEs. EU satisfaction improved from 50% to 85% rating paging communication as good or excellent. Safety events related to paging remain infrequent. Specific WA use decreased by 60%.
CONCLUSIONS:System-wide use of required fields produced significant
improvement in inclusion of all 6 CEs and EU satisfaction. WAs were curbed by improving the ease of CE incorporation. Requiredfields should be considered at institutions seeking improved paging communication.
Communication is the foundation of all patient care, with paging serving as a primary mode of communication in hospital systems nationwide. Paging systems may be numeric or
alphanumeric or bidirectional or asynchronous, meaning the recipient cannot respond directly and must either call or page to respond. Breakdowns in paging communication lead to inefficiencies, patient harm, and
provider dissatisfaction.1–4Variable message contents leave the potential for misinterpretation, incorrect response triage, medical errors, and patient harm.3–6On the basis of analyses of page contents, authors of recent studies have called for interventions to standardize and prioritize paging communication.5–7 Interventions to date include providing nurses with alphanumeric pagers8and
aDepartment of Pediatric Emergency Medicine, Children's
Hospital and Clinics of Minnesota, Minneapolis, Minnesota; andbDepartment of Pediatrics, Medical College of
Wisconsin and Children’s Hospital of Wisconsin, Milwaukee, Wisconsin
Dr Weigert conceptualized and designed the study, designed data collection instruments, conceptualized and performed interventions, collected data, conducted initial analyses, drafted the initial manuscript, and reviewed and revised thefinal manuscript; Dr Schmitz conceptualized and designed the study, designed data collection instruments, conceptualized and performed interventions, collected data, conducted initial analyses, and reviewed and revised thefinal manuscript; Dr Soung conceptualized and designed the study, designed data collection instruments, conceptualized interventions, conducted initial analyses, and reviewed and revised thefinal manuscript for important intellectual content; Ms Porada collected data, conducted ongoing analyses, and reviewed and revised thefinal manuscript for important intellectual content; Dr Weisgerber conceptualized and designed the study, designed data collection instruments, conceptualized interventions, and reviewed and revised thefinal manuscript for important intellectual content; and all authors approved thefinal manuscript as submitted and agree to be accountable for all aspects of the work.
DOI:https://doi.org/10.1542/peds.2018-1362 Accepted for publication Jan 3, 2019
Address correspondence to Rachel M. Weigert, MD, 345 N Smith Ave, Mail Stop 504, St Paul, MN 55102. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2019 by the American Academy of Pediatrics
education on optimal information to include.9Improvements in
communication and satisfaction have been noted with these strategies, but a gap still exists regarding how to ensure standardized paging is consistently used.
At our stand-alone academic children’s hospital, we identified the quality of information contained in asynchronous alphanumeric pages pertaining to patient care as an area for potential improvement. Baseline data revealed low provider
satisfaction stemming from a lack of standardized page contents, which made responding appropriately a challenge. Incomplete sender information, including last name and full callback phone number, made contacting the sender difficult. Often, pages were ambiguous as to whether the sender expected a callback, which resulted in the sender feeling dissatisfied with the interaction despite intentions of the recipient.
Given the breadth of work
demonstrating a lack of standardized paging communication, along with concerns of lack of efficiency,
workflow disruption, and potential for error and patient harm, we designed a quality improvement (QI) study to remedy these deficiencies. Our primary aims to be achieved by April 2018 were (1) increase the percent of pages including all 6 critical elements (CEs) (ie, urgency indicator
[information only (FYI), call, or come], sender’sfirst and last name, 7-digit callback number, patientfirst name, and room number), (2) improve provider satisfaction with the paging system to.80% rating paging as good or excellent, and (3) decrease the frequency of adverse patient safety events related to paging.
METHODS
Setting and Context
This QI initiative was conducted at Children’s Hospital of Wisconsin
(CHW), a large academic pediatric quaternary care center encompassing a network of outpatient clinics, ambulatory surgery center, urgent cares, and a satellite hospital. Our paging system is used by a variety of end users (EUs), including residents and fellows in multiple subspecialty programs, rotating emergency and family medicine residents, health sciences students, nurses, and ancillary staff in addition to pediatric and subspecialty attending providers. Communication methods within our hospital system include alphanumeric paging, hands-free voice communication, and hospital-sponsored and personal cell phones. Paging remains the universal mode of communication spanning the entire hospital system.
Planning Interventions
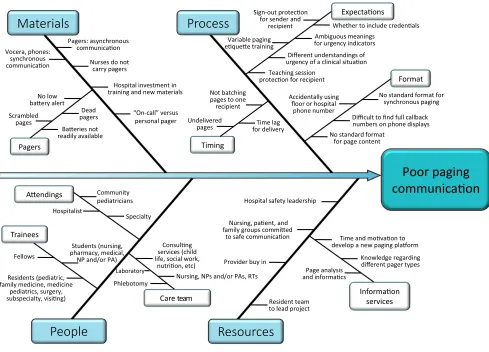
With baseline survey and paging data in mind, a multidisciplinary team led by pediatric residents and faculty with the support of hospital leadership created afishbone diagram demonstrating areas for improvement (Fig 1). The team then used process improvement tools to assess the source of lapses in communication and determined 6 CEs to include in every page to triage and respond appropriately. These included an urgency designation (information only [FYI], callback requested [call], or a provider is requested at bedside [come]), the sender’sfirst and last name, a 7-digit callback number, and the patient’s name and room number.
Interventions
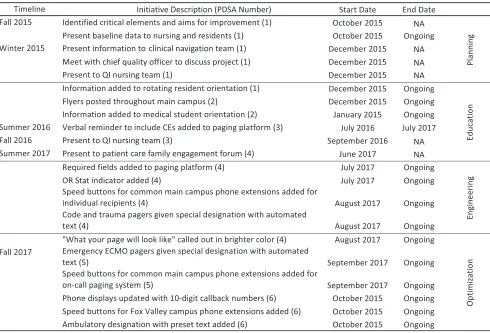
Plan-do-study-act (PDSA) cycles were implemented to increase the use of CEs in paging communication focused on (1) education, (2) engineering, and (3) optimization (Fig 2).
Education
Initial interventions that were aimed at behavior change through education included meetings with various provider groups,flyers posted in
work areas throughout our main campus, and a visual reminder of CEs on the paging platform. Educational interventions began in fall 2015 targeting nurses and pediatric residents. Orientation materials on the CEs were initiated for rotating residents and medical students in winter 2015. A visual reminder of the CEs was added to the paging platform in summer 2016, which was visible to all EUs when typing a page.
Engineering
For the subsequent year, a team composed of pediatric residents, physician support, and information services worked to design and gain stakeholder approval for a thorough update to the paging platform. In July 2017, the platform was revised to include requiredfields for all CEs except patient name and room number, knowing that not all pages sent are related to a specific patient. Information boxes depicting the correct use of each urgency designation were added through hover functionality.
Optimization
In response to data analysis and EU feedback through multiple PDSA cycles, many enhancements were made to the paging platform to improve functionality and increase compliance. In summer 2017, the platform was further optimized to include shortcut (speed) buttons for common callback number prefixes and exemption of requiredfields for
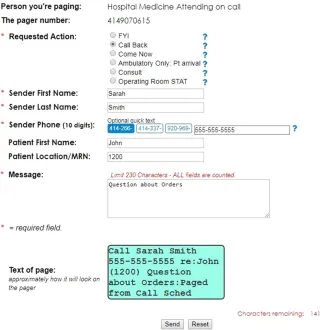
page contents in real time with standardized page formatting depending on urgency designation (Fig 3).
Study of the Intervention
Initial page analysis began in December 2015. The target population for this study included any employee of CHW or affiliate site using the paging platform. As such, a subset of pagers chosen for analysis were selected on the basis of the large number of pages sent and received monthly. Specific pagers analyzed include 6 acute care ward pass-off pagers held by residents, an infectious disease attending’s personal pager, and the
first-call surgery resident pass-off pager. All pagers analyzed were held by providers who work
exclusively at our main campus site. Most pages were sent by EUs at our main campus but did include senders from other sites.
Pages excluded were those not pertaining to patient care, pages from satellite campuses due to information barriers, and those with preset text such as code and/or trauma pages. No paging data were collected from March and April 2017 because of a transition in the data server.
To determine baseline usage of the 6 CEs,.300 pages were analyzed before interventions were undertaken. Because of the large number of pages received monthly, a randomization strategy of analyzing everyfifth page up to 100 pages per month was used.
Measures
Outcome measures included (1) the percent of pages including all 6 CEs, (2) the rating of provider satisfaction with paging system as good or excellent, and (3) the number of patient safety reportsfiled related to paging per month (Fig 4).
A survey, in which a 5-point Likert scale was used, was developed to assess satisfaction with the paging system. Analysis was completed by evaluating the percent of respondents rating satisfaction as good
or excellent. Paper surveys were distributed by project leaders via in-person convenience sampling on a variety of inpatient and intensive carefloors, the emergency
department, and at required house staff, hospitalist, and nursing
FIGURE 1
meetings. Surveys were distributed at
∼3-month intervals and after each major intervention. An open-ended question used to request
feedback drove subsequent PDSA cycles.
As the third outcome measure, patient safety reports from all sites were monitored through Midas, the internal incident reporting system. Incident reports pertaining to breakdowns in communication due to the paging system were included as obtained with the search queries
“paging,” “paged,” “page,”or“pager.” All incident reports were reviewed by project leaders.
Process measures included the percent of pages containing each individual CE. Each page was analyzed for the presence or absence of individual CEs. Pages were not
assessed for“correct”usage of urgency indicators; rather, an urgency indicator was considered present if the words“call,” “come,”or“FYI”were included in the page. Survey
responses rating timeliness and appropriateness of response to pages as good or excellent were also monitored as process measures via items on the paper survey. Objective criteria for appropriateness and timeliness of responses were not provided.
Balancing measures included the use of 000-000-0000 as a phone number as a work-around (WA) to the required phone number field and the use of OR Stat, which deselects all requiredfields. These 2 WAs were tracked as an absolute number of pages per month from July 2017 onward.
Analysis
Statistical process control charts (p-charts) were used to track our outcome measure (ie, the percent of pages containing all 6 CEs) and process measures of including individual CEs during the study period. The numerator was derived from the absolute number of pages that contained either all 6 CEs or each individual element, and the denominator was the total number of pages analyzed in a given month. We used p-charts to track survey data, including the
outcome measure (ie, the percent of provider satisfaction rating of good or excellent) and process
measures (ie, the percent rating of appropriateness and timeliness of response to pages as good or excellent). XmR charts were
FIGURE 2
used to monitor the number of 000-000-0000 and OR Stat WAs. Charts were generated by using the QI Charts add-on for Microsoft Excel. Analysis was completed by using established rules for identifying special-cause variation for run and control charts.10–12Eight or more consecutive points above or below the centerline were used to
prompt a midline shift on the control charts.
Ethical Considerations
This project was exempt by the CHW Institutional Review Board. Risk management assisted in determining CEs that maintain compliance to the Health Insurance Portability and Accountability Act in a nonencrypted
system. It was decided thatfirst name and room number would be
unlikely to identify a patient to a reader who was not a hospital staff person.
RESULTS
Table 1 reveals the demographics of both senders and recipients of pages analyzed throughout the study. Page standardization improved with an increase from 4.4% to 79.7% of pages containing all 6 CEs (Fig 5A). Special-cause improvement was noted in each of the 6 individual CEs after the institution of requiredfields in the paging system in July 2017 (Fig 5 B–D). Although special-cause improvement was noted for senders’
first name, patient name, and room number, the baseline level of inclusion was high before study initiation.
Survey data representing a variety of EUs (Table 2) revealed that the outcome measure (ie, percent of providers rating the paging system as good or excellent on a 5-point Likert
FIGURE 3
Paging platform after requiredfields were added.
FIGURE 4
Chart depicting outcome, process and balancing measures as decided on by a consensus group at the outset of the project.
TABLE 1Page Sender and Recipient Demographics
Roles n(%)
Senders
Nurse 3473
(69.7)
Resident 350 (7.0)
Attending 241 (4.8)
Unknown 230 (4.6)
Therapy (RT, OT, PT, or speech) 183 (3.7)
Pharmacy 113 (2.3)
Social work and case management
93 (1.9)
Advanced practice provider 81 (1.6)
Fellow 79 (1.6)
Health unit coordinator 50 (1.0) Laboratory and imaging 24 (0.5)
Other 65 (1.3)
Total pages analyzed,N 4984 Recipients
Resident 3879
(77.8)
Surgery 630 (12.6)
scale) improved from 55% to 85% throughout the course of the study. However, survey process measures (ie, rating of timeliness and
appropriateness of response) did not change significantly throughout the course of the study. Due to timely hand collection of surveys, there was a 100% response rate.
Overall, the outcome measure of safety events related to paging remained infrequent, ranging from 0 to 4 monthly.
Because the paging platform was enhanced after recurrent PDSA cycles,
new opportunities for WAs emerged, including the use of 000-000-0000 as a phone number and the OR Stat designation to deselect all required
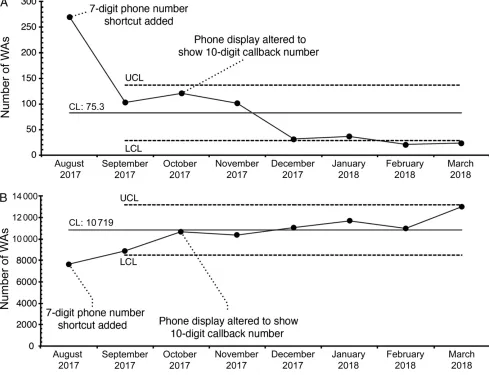
fields. After speed buttons were added for commonly used callback numbers, use of 000-000-0000 decreased by 60%. The use of OR Stat has continued to increase over time (Fig 6).
DISCUSSION
Our team significantly impacted paging standardization within our hospital system using QI methodology,
including multiple PDSA cycles involving education, engineering of requiredfields, and optimization of the paging platform in response to feedback. The inclusion of all 6 CEs in each page improved, with 2 specific shifts noted (one at the time of introduction of a visual reminder on the paging platform to include all CEs and again after the institution of requiredfields). EU satisfaction increased to 85% rating the paging system as good or excellent. Pager-related patient safety events were unchanged by the platform upgrade. EUs created several WAs to evade
FIGURE 5
proper usage, some of which were curbed by further paging platform optimization.
The most novel aspect of this study is the inclusion of requiredfields
to assist in standardizing page content. Despite being completed in a pediatric hospital, the
varied EU population serves as a good proxy for all hospital systems, regardless of size or patient base. Although other institutions have sought to standardize paging through education, our engineering solution is sustainable and produced increased CE usage and EU satisfaction. Studies of voluntary communication systems, either electing to use a bidirectional system or standardized
language, decrease in effectiveness over time.13
Furthermore, improvements were noted in use of individual CEs. The greatest gains were demonstrated in the inclusion of an urgency indicator, a 7-digit phone number, and the sender’s last name (Fig 5). The primary driver for the desired standardization at conception of this study were these 3 measures, with goals of improving triage of and appropriate response to pages. The culture at our institution was to typically include a 4- or 5-digit phone number extension and to only include afirst name when sending pages. This often led to confusion for those unfamiliar with our internal extensions and created difficulty in
TABLE 2EU Survey Demographics n(%) Participants
Resident 148 (54.4)
Nurse 88 (32.4)
Attending 20 (7.4)
Case manager 3 (1.1)
Fellow 3 (1.1)
Respiratory therapist 2 (0.7)
Pharmacist 1 (0.4)
Other 7 (2.6)
Total,N 272
FIGURE 6
identifying the page sender.
Ultimately, requiredfields led to the greatest improvement in inclusion of CEs in every page. Notably, patient name and room, as well as the sender’sfirst name were consistently included at high rates from the beginning of the study, which is interesting because neither patient name nor room number are
currently requiredfields. This trend is likely indicative of a cultural norm in page contents and may also be indicative that the introduction of some but not all requiredfields can still yield more complete page contents.
While creating change in such a vital and commonly used communication modality at a large hospital system, a concern arose that providers would have difficulty with the transition from“good intent”paging to a system engineered to provide a framework for standardization. Provider dissatisfaction with the content received in pages was also an impetus for the project.
Therefore, provider satisfaction was tracked closely as an outcome measure. Most providers surveyed feel that the paging system is good or excellent in its current state, and satisfaction improved during the project.
With an additional aim of improving patient safety, incident reports related to paging were monitored. Overall, events were infrequent at baseline and remained low throughout the study period. The majority of events were either determined to fall into the Healthcare Performance Improvement Safety Event Classifications of not a safety event, no detectable harm, or no harm. There was no change noted in the event type after the institution of requiredfields. A common theme was delayed response to pages, which guided future interventions, including education regarding the standard use of urgency indicators. The lack of or inconsistent use of urgency indicators
has been noted in other studies.5,14 We were unable to quantify delayed response to pages for multiple reasons, including lack of time stamping when a page is sent, and lack of forced delay quantification in incident reports.
The use of required fields was a dramatic change from our previous alphanumeric paging system whose only limit was a maximum character count. As such, the culture of our institution was heavily impacted, which is a phenomenon that has been noted in previous studies, and as providers continued to use the new system, they uncovered various WAs.1,8Monitoring the use of WAs drove further PDSA cycles with system optimization to improve ease of paging. For example, in monitoring the use of 000-000-0000 as
a phone number, we found that this WA was reduced significantly as speed buttons for common callback number prefixes were added and phone displays in the hospital were altered to show a full 7-digit number rather than extension only. In reviewing additional WAs, we noted that the use of OR Stat, which is used to deselect all requiredfields, has continued to increase monthly. Our team is planning further
interventions to curb inappropriate use of this indicator, including preset language pertaining to OR locations only. Additional WAs, such as increased use of bidirectional texting on personal phones, are difficult to measure, although they have been reported by some EUs.
Additional consideration should be provided to the variety of
technologies available to hospital systems, including bidirectional texting, phones, and hands-free voice communication, some of which are used in specific units in our own institution. However, bidirectional communication enables workflow disruptions, and asynchronous communication permits providers to
triage responses when adequate information is included, which may reduce wait times for responses to urgent concerns.4,15At our multisite institution, the process of
applying and studying various interventions ultimately led to inclusion of requiredfields on our paging platform, which has proven to be the most effective means of impacting standardized communication throughout our organization.
Among the limitations of this study, only pagers from our main campus hospital were analyzed despite the broader impact of the update throughout the organization. All interventions before the paging system upgrade were performed exclusively at our main campus. During the study period, our group posited that the number of pages sent may decrease as EUs respond in a timely and appropriate manner given more complete page contents. However, the number of pages sent could not be
obtained retrospectively because the data repository resets after 30 days. The mixed communication methods used within our
institution may impact the results and applicability to other institutions. Additionally, paging data involved primarily nurse and resident communication,
which may not fully represent system-wide impact. In the same vein, survey results
were focused primarily on nursing, residents, and attending
physicians and may not be representative of the entire organization. Cost and time commitment to complete such a project and potential upgrade should also be considered.
CONCLUSIONS
of all 6 CEs and improved provider satisfaction with paging communication. Safety events related to paging were minimal. The
sociotechnical culture of our hospital revealed the development of WAs, which were curbed by system enhancements. As demonstrated by our study, institutions seeking to improve paging communication and provider satisfaction should strongly consider redesigning alphanumeric
paging interfaces to implement requiredfields.
ACKNOWLEDGMENTS
This project would not have been possible without the support of Debbie Dolata-Drent, Larry
Reeder, Drs Steffes, Velazquez, Lhost, and Gulbranson, and the
mentorship of Drs Gutzeit, Spahr, and Gray.
ABBREVIATIONS
CE: critical element
CHW: Children’s Hospital of Wisconsin
EU: end user
FYI: for information only OR: operating room PDSA: plan-do-study-act QI: quality improvement WA: work-around
FINANCIAL DISCLOSURE:The authors have indicated they have nofinancial relationships relevant to this article to disclose.
FUNDING:No external funding.
POTENTIAL CONFLICT OF INTEREST:The authors have indicated they have no potential conflicts of interest to disclose.
REFERENCES
1. Wu R. Turning the page on hospital communications slowly.BMJ Qual Saf. 2017;26(1):4–6
2. Smith AD, de Vos MS, Smink DS, Nguyen LL, Ashley SW. Text paging of surgery residents: efficacy, work intensity, and quality improvement.Surgery. 2016; 159(3):930–937
3. Ferguson A, Aaronson B, Anuradhika A. Inbox messaging: an effective tool for minimizing non-urgent paging related interruptions in hospital medicine provider workflow.BMJ Qual Improv Rep. 2016;5(1):u215856.w7316 4. Nguyen C, McElroy LM, Abecassis MM,
Holl JL, Ladner DP. The use of technology for urgent clinician to clinician communications: a systematic review of the literature.Int J Med Inform. 2015;84(2):101–110
5. Luxenberg A, Chan B, Khanna R, Sarkar U. Efficiency and interpretability of text paging communication for medical inpatients: a mixed-methods analysis.
JAMA Intern Med. 2017;177(8): 1218–1220
6. Carlile N, Rhatigan JJ, Bates DW. Why do we still page each other? Examining the frequency, types and senders of pages in academic medical services.BMJ Qual Saf. 2017;26(1):24–29
7. Kummerow Broman K, Kensinger C, Phillips C, et al. Characterizing the clamor: an in-depth analysis of inpatient paging communication.Acad Med. 2016;91(7):1015–1021
8. Quan SD, Wu RC, Rossos PG, et al. It’s not about pager replacement: an in-depth look at the interprofessional nature of communication in healthcare.
J Hosp Med. 2013;8(3):137–143 9. Goyal P, Cohen-Mekelburg S, Egan C,
et al. New uses of old technology: can nurse-pagers improve communication between resident-physicians and nurses.Appl Nurs Res. 2018;44:1–5 10. Provost LP, Murray SK.The Health Care
Data Guide: Learning From Data for
Improvement. San Francisco, CA: Jossey-Bass; 2011
11. Benneyan JC, Lloyd RC, Plsek PE. Statistical process control as a tool for research and healthcare improvement.
Qual Saf Health Care. 2003;12(6): 458–464
12. Perla RJ, Provost LP, Murray SK. The run chart: a simple analytical tool for learning from variation in healthcare processes.BMJ Qual Saf. 2011;20(1): 46–51
13. Hill J, Janko M, Angell KF, et al. Hospital text paging communication as a surgical quality improvement initiative.J Surg Res. 2017;213:84–89 14. Espino S, Cox D, Kaplan B. Alphanumeric
paging: a potential source of problems in patient care and communication.
J Surg Educ. 2011;68(6):447–451 15. Mandl KD, Khoong E. Pagers and beyond
DOI: 10.1542/peds.2018-1362 originally published online March 19, 2019;
2019;143;
Pediatrics
Weisgerber
Rachel M. Weigert, Anna H. Schmitz, Paula J. Soung, Kelsey Porada and Michael C.
Improvement Methodology
Improving Standardization of Paging Communication Using Quality
Services
Updated Information &
http://pediatrics.aappublications.org/content/143/4/e20181362 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/143/4/e20181362#BIBL This article cites 14 articles, 4 of which you can access for free at:
Subspecialty Collections
sub
http://www.aappublications.org/cgi/collection/quality_improvement_
Quality Improvement
unication_skills_sub
http://www.aappublications.org/cgi/collection/interpersonal_-_comm
Interpersonal & Communication Skills
e_management_sub
http://www.aappublications.org/cgi/collection/administration:practic
Administration/Practice Management
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2018-1362 originally published online March 19, 2019;
2019;143;
Pediatrics
Weisgerber
Rachel M. Weigert, Anna H. Schmitz, Paula J. Soung, Kelsey Porada and Michael C.
Improvement Methodology
Improving Standardization of Paging Communication Using Quality
http://pediatrics.aappublications.org/content/143/4/e20181362
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.