aDepartment of Global Health and Population, Harvard T.H. Chan School of Public Health, Harvard University, Boston, Massachusetts; and bDepartment of Epidemiology, Berkeley School of Public Health, University of California Berkeley, Berkeley, California
Mr Jeong conceptualized the study, screened studies for eligibility, extracted the data, conducted analyses, and drafted the manuscript; Ms Pitchik contributed to conceptualization of the study, screened studies for eligibility, extracted the data, and reviewed and edited the manuscript; Dr Yousafzai oversaw conceptualization of the study and reviewed and edited the manuscript; and all authors read and approved the final manuscript as submitted.
This trial has been registered with the PROSPERO register (identifier CRD42017064902). DOI: https:// doi. org/ 10. 1542/ peds. 2017- 3510
Accepted for publication Jan 3, 2018
To cite: Jeong J, Pitchik HO, Yousafzai AK. Stimulation Interventions and Parenting in Low- and Middle-Income Countries: A Meta-analysis. Pediatrics. 2018;141(4):e20173510 CONTEXT: Early childhood stimulation interventions positively impact early child development
(ECD) outcomes in low- and middle-income countries. However, trials have less
comprehensively evaluated the effects of such parenting programs on caregivers’ skills and capacities.
OBJECTIVE: We conducted a systematic review and meta-analysis to assess the effectiveness of
stimulation interventions on improving parenting outcomes.
DATA SOURCES: Six electronic bibliographic databases.
STUDY SELECTION: Inclusion criteria included randomized controlled trials of stimulation
interventions designed to improve ECD outcomes during the first 2 years of life that measured any maternal or parenting-related outcome after the start of the intervention.
DATA EXTRACTION: Two independent reviewers extracted data by using a structured form.
RESULTS: Fifteen studies representing 13 unique randomized controlled trials met the
inclusion criteria. Pooled standardized mean differences (SMDs) based on random-effects models revealed medium-to-large benefits of stimulation interventions for improving the home caregiving environment (n = 10; SMD = 0.57; 95% confidence interval [CI], 0.37 to 0.77), mother-child interactions (n = 3; SMD = 0.44; 95% CI, 0.14 to 0.74), and maternal knowledge of ECD (n = 6; SMD = 0.91; 95% CI, 0.51 to 1.31). No significant difference was seen for maternal depressive symptoms (n = 9; SMD = −0.10; 95% CI, −0.23 to −0.03).
LIMITATIONS: Limitations include heterogeneity across interventions, lack of standardized
measures, and different time points of assessments across studies.
CONCLUSIONS: Early childhood stimulation interventions improve several distinct aspects of
maternal parenting. Improvements in parenting capacities may serve as key mechanisms by which these programs benefit ECD outcomes.
Stimulation Interventions and
Parenting in Low- and
Middle-Income Countries: A Meta-analysis
Joshua Jeong, MSc, a Helen O. Pitchik, MSc, b Aisha K. Yousafzai, PhDaIt is estimated that 250 million children <5 years of age in low- and middle-income countries (LMICs) are failing to reach their developmental potential because of a host of co-occurring nutritional, psychosocial, and poverty-related risk factors.1 Inadequate stimulation,
in particular, has been highlighted as a key modifiable risk factor of poor child development in LMICs.2
Consequently, over the past decades, parenting interventions have become increasingly prioritized as a strategy for promoting early child development (ECD).3–5
Psychosocial stimulation interventions are designed to promote ECD by enhancing opportunities for young children to explore their environment, manipulate new objects, solve problems, and socially interact with others. These interventions are often targeted at parents, guiding them to promote developmentally appropriate stimulation by providing learning opportunities for the young child and to engage with the young child in stimulating play activities. These programs have been found to be effective in improving children’s cognitive, socioemotional, and motor development across diverse populations, settings, and implementation strategies in LMICs.3, 6–9 For example, a prior
systematic review and meta-analysis of psychosocial stimulation interventions that were conducted with children <2 years of age found medium-sized benefits for children’s early cognitive (d = 0.42;
n = 22) and language (d = 0.47; n = 9) development.6
A central aspect of early childhood stimulation programs that target the parent and child involves coaching, encouraging, and counseling caregivers to enhance parenting knowledge, beliefs, attitudes, and practices and foster positive parent-child interactions, to bring about improvements in
ECD outcomes.3 These hypothesized
parenting mechanisms are rooted in studies that have revealed how parenting knowledge translates into an improved home caregiving environment10, 11 and how such
parenting behaviors, in turn, strongly influence children’s development.12, 13
Several trials have supported positive intervention effects on a variety of maternal parenting outcomes. These include greater maternal knowledge of ECD, 14–16 improvements in the
home stimulation environment, 14, 16
and more sensitive mother-infant interactions.17 Less conclusive
evidence has been found regarding the effects on reducing maternal depression.14, 16, 18, 19
To date, 2 reviews in gray literature reports have mentioned some benefits of early stimulation interventions for caregivers in LMICs.7, 20 However, to the best of the
authors’ knowledge, no systematic review or quantitative synthesis has been produced in this body of literature. Considering the rapidly growing interest in stimulation interventions in LMICs, 21
a systematic review and meta-analysis evaluating the effectiveness of these programs on improving parenting behaviors can help to uncover parenting behavior change mechanisms that underlie these programs’ impacts on ECD outcomes. The primary objectives of the current study were (1) to systematically review the effects of early childhood stimulation interventions in LMICs that targeted children <2 years of age on distinct maternal parenting-related skills and capacities that promote ECD and (2) to summarize these effects across intervention studies by using meta-analytical techniques. Given the heterogeneity in stimulation intervention
programs, 8 a secondary goal of
this meta-analysis was to explore several potential moderators of intervention effects on parenting outcomes. More specifically, we
explored whether effects differed by sample characteristics, intervention characteristics, and outcome measures used across studies.
MeThODs search strategy
A systematic literature review of stimulation intervention studies in LMICs was conducted and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines.22 The methods were
prespecified and documented in a protocol (PROSPERO registration number: CRD42017064902). Six electronic bibliographic databases were searched for peer-reviewed, published studies from inception to May 1, 2017: Medline, Embase, PsycINFO, Cumulative Index to Nursing and Allied Health Literature, Web of Science, and Global Health Library. A string of search terms was used to combine keywords for 3 main concepts: caregivers’
stimulation, randomized controlled trials, and LMICs (Supplemental Information).
selection Criteria
was not a randomized controlled trial; (3) the study authors recruited children >24 months of age, on average; (4) the study was conducted in a high-income country; or (5) the study measured a nonpsychosocial parenting outcome (ie, mothers’
preventive health or dietary practices).
Data extraction
Two reviewers (Jeong and Pitchik) independently screened the titles and abstracts of each study identified in our systematic search. Full texts of selected studies were reviewed to assess eligibility. Reference lists of included studies and previous reviews were examined to identify any potentially relevant publications not found through the electronic search. Any discrepancy between the reviewers was resolved through discussion and consensus.
Two reviewers (Jeong and Pitchik) independently extracted data from each eligible study by using a structured form. Three main categories of data were extracted for each study: characteristics of the sample, intervention details, and measurement of parenting outcomes. Any discrepancy was resolved through discussion and consensus.
Outcomes
The primary outcomes for the current study were the home caregiving environment, observed mother-child interactions, maternal knowledge of ECD, and maternal depressive symptoms. In particular, the home caregiving environment included any observed or reported information on parenting practices, child care routines, child care environment, and children’s early stimulation and learning opportunities.
Risk of Bias Assessment
Two reviewers (Jeong and Pitchik) independently assessed risk of bias in included studies by using
the Cochrane Collaboration Risk of Bias Tool.23 Categorical ratings of
high, low, or unclear were assigned with regards to random sequence generation, blinding of participants and personnel, incomplete outcome data, and selective reporting in each study. Any discrepancy was resolved through discussion and consensus.
statistical Analysis
Treatment effect sizes (ESs) on parenting outcomes were calculated as the standardized mean differences (SMDs) between the control and intervention arms with respect to change in unadjusted mean value from baseline to follow-up. For each study, we measured the change in parenting outcome by subtracting the mean score at posttreatment from the mean score at baseline, separately for the intervention and control arms, to account for any potential baseline between-group differences in the parenting outcomes. The SMD was calculated as the bias-adjusted difference between the 2 study arms after standardization by their pooled SD, with studies weighted by the inverse variance method (Hedge’s g). Studies that reported effects for more than 1 parenting outcome were allowed to contribute to each appropriate meta-analyses; however, each study (or trial, in the case of 2 articles from 1 data set) was permitted to contribute only 1 ES to each analysis for a given outcome. In studies that had more than 1 follow-up assessment, the assessment closest to the completion of the intervention was used. Pooled ES estimates were based on a random effects model. The ESs of each study, as well as the overall pooled estimate, were illustrated by using a forest plot.
Heterogeneity of the mean ES was assessed by using the Q statistic and its P value and the I2 statistic.
Prespecified moderator analyses were conducted to explore whether effects might be moderated by
sample characteristics, intervention characteristics, or outcome measures used. Moderator analyses were conducted if at least 2 studies were available for each stratum. Study-level sample characteristics included mean child age at enrollment (< or ≥12 months), mean maternal education (incomplete primary school or complete primary school or higher), and country context (lower middle–income or upper middle–
income country). Intervention characteristics included delivery strategy (individualized only or group/individualized and group) and duration (< or ≥12 months). Outcome measure characteristics related to whether reliability of measure was reported; whether the Home Observation for Measurement of the Environment (HOME) inventory score was used as the measure of the home caregiving environment; the type of parenting knowledge assessed (child development
milestones or childrearing practices); and the scale used for maternal depressive symptoms varied (the Center for Epidemiologic Studies Depression [CES-D] scale or other). Stratified analyses were conducted for each subgroup, and the χ2
test was used to assess statistical significance (at P < .05) of difference in pooled estimates between groups. All data were prepared and analyzed by using Stata version 13 (StataCorp, College Station, TX).24
ResulTs
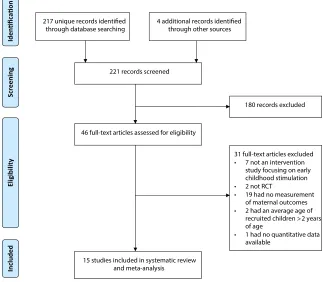
systematic literature search Results
full text, we additionally excluded 31 articles for not meeting our eligibility criteria (Fig 1). In total, 15 studies, representing 13 unique interventions, were included in our systematic review and meta-analysis. All 13 unique interventions were cluster-randomized controlled trails.
Risk of Bias
Overall, the risk of bias within individual studies was low (Supplemental Information, Supplemental Table 3). In all studies, the authors used blinded outcome assessors and described the completeness of outcome data. However, given the nature of parenting interventions, all studies were potentially at risk for performance bias due to knowledge of the intervention by participants. The risk of bias for selective reporting and other biases was unclear across all studies. No studies were excluded on the basis of overall risk of bias assessments.
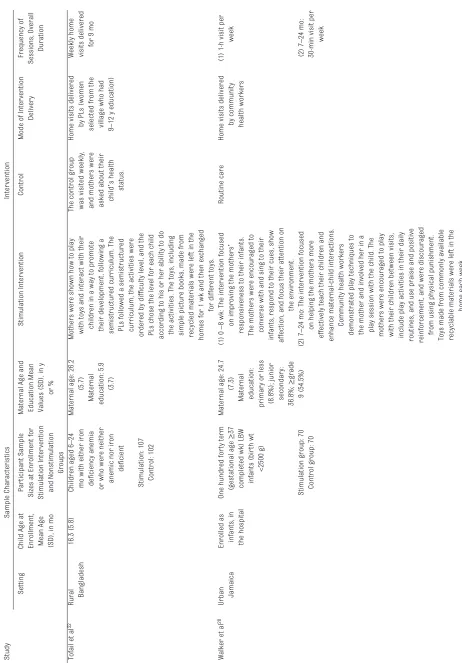
sample Characteristics
The authors of the 13 unique trials enrolled a total of 6267 participants, with sample sizes ranging from 125 in the trial by Powell et al25 to 1489
in the trial by Yousafzai et al.16 The
authors of 2 trials enrolled pregnant mothers in their third trimester of pregnancy17, 26; the authors of 3
trials enrolled newborn children in the first 3 months of life16, 27, 28; and
the authors of the remaining 8 trials enrolled infants across a broader age range over the first 2 years of life. Of the 11 trials in which children were enrolled, the average age at enrollment was 11.53 months (SD = 8.20), ranging from birth in the study by Walker et al28 to 22.4 months in
the study by Singla et al.29 Of the
10 trials in which maternal age at enrollment was reported, the average maternal age was 26.20 years (SD = 1.71). Of the 8 trials in which years of maternal education was reported, the average was 4.96 years (SD = 1.69),
which ranged from 2.3 years in the study by Yousafzai et al16 to 7.2 years
in the study by Attanasio et al.18
Five trials targeted undernourished children, 15, 19, 25, 28, 30–32 and 2 targeted
the poorest families in the study area.18, 33 Sample characteristics are
presented in Table 1.
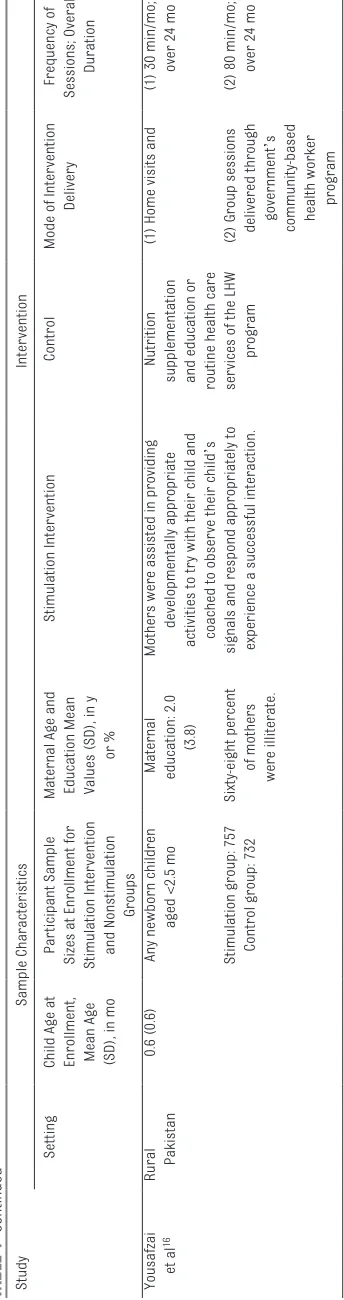
Intervention Characteristics
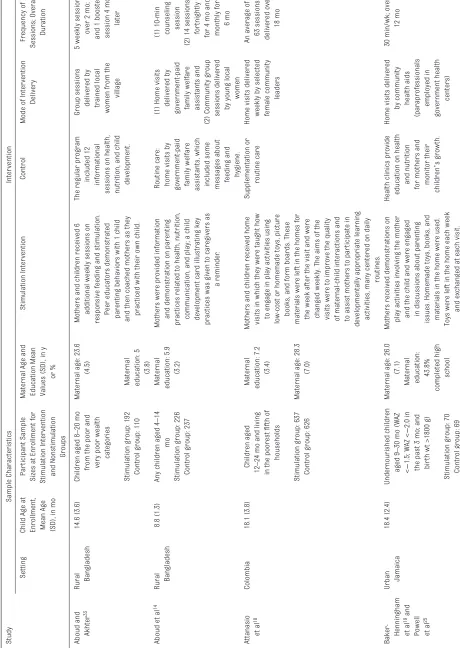
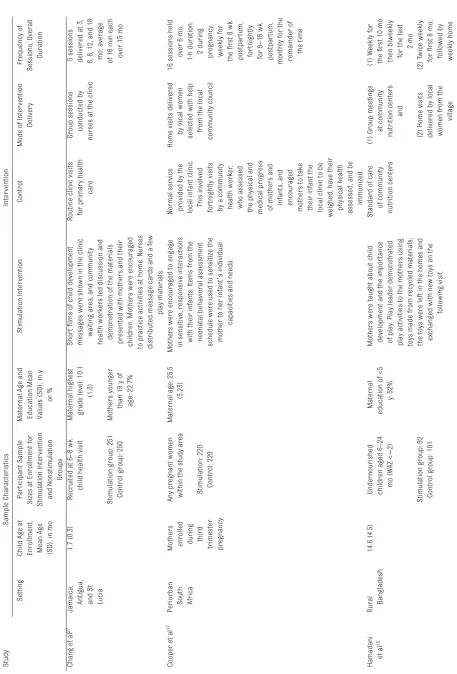
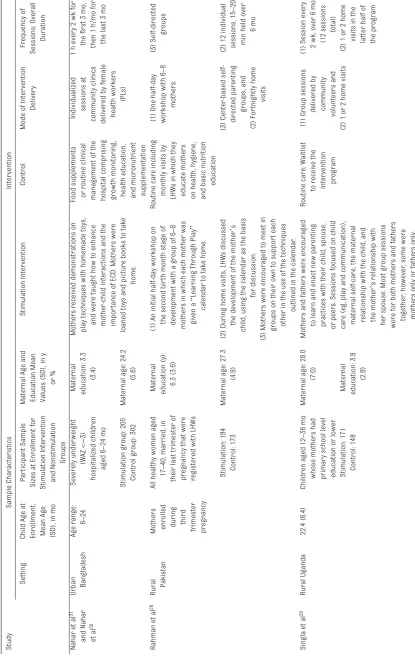
The 15 included studies represented 13 unique interventions that focused on promoting parenting behaviors and enhancing stimulation to improve ECD outcomes. A summary of the individual interventions is presented in Table 1. The interventions were conducted in 8 different countries: Bangladesh, 14, 15, 30–33 Colombia, 18
Pakistan, 16, 26 Uganda, 29 South Africa, 17
Jamaica, 19, 25, 27, 28 Antigua, 27 and
St Lucia.27 Six programs were
delivered only in individualized sessions, 17–19, 25, 28, 30–32 2 were
delivered only in group sessions, 27, 33
and 5 involved both group and individualized sessions.14–16, 26, 29
Six programs were delivered by government health
workers, 14, 16, 19, 25, 27, 28, 30, 31 6 were
delivered by trained community members, 15, 17, 18, 29, 32, 33 and 1 involved
both health workers and community members.26 The intended total
duration of the interventions was on average 11.5 months (SD = 5.95), which ranged from 6 months17, 26, 29–31, 33 to 24 months.16
All interventions focused on promoting positive parenting and enhancing developmentally appropriate learning opportunities for children through stimulation, such as playing, singing, and teaching. Intervention sessions revolved around coaching mothers on how to interact with their children to increase sensitivity to their children’s developmental needs. The majority of the interventions incorporated low-cost local or homemade toys to promote stimulation between the caregiver and child. Despite these common overall intervention
FIGuRe 1
TAB
le
1
Summary of Individual Studies Included in Meta-analysis
Study
Sample Characteristics
Inter
vention
Setting
Child Age at Enrollment, Mean Age (SD), in mo
Par
ticipant Sample
Sizes at Enrollment for Stimulation Inter
vention
and
nonstimulation groups Maternal Age and Education Mean Values (SD), in y
or %
Stimulation Inter
vention
Control
Mode of Inter
vention
Delivery
Frequency of
Sessions; Overall
Duration
Aboud and Akhte
r
33
Rural Bangladesh
14.6 (3.6)
Children aged 8
–
20 mo
from the poor and very poor wealth
categories
Maternal age: 23.6
(4.5)
Mothers and children received 6 additional weekly sessions on responsive feeding and stimulation. Peer educators demonstrated parenting behaviors with 1 child and then coached mothers as they practiced with their own child.
The regular program
included 12 informational sessions on health, nutrition, and child development. group sessions delivered by trained local women from the
village
5 weekly sessions
over 2 mo;
and 1 booster session 4 mo
later
Stimulation group: 192
Maternal education: 5
(3.8)
Control group: 110
Aboud et a
l
14
Rural Bangladesh
8.8 (1.3)
Any children aged 4
–
14
mo
Stimulation group: 226 Control group: 237 Maternal education: 5.9
(3.2)
Mothers were provided information and demonstration on parenting practices related to health, nutrition, communication, and play; a child development card illustrating key practices was given to caregivers as
a reminder
.
Routine care: home visits by government-paid family welfare assistants, which included some messages about feeding and
hygiene.
(1) Home visits delivered by government-paid family welfare assistants and (1) 10-min counseling session
(2) 14 sessions,
for
tnightly
for 4 mo and monthly for
6 mo
(2) Community group sessions delivered
by young local
women
Attanasio et a
l
18
Colombia
18.1 (3.8)
Children aged 12–24 mo and living
in the poorest fifth of
households
Maternal education: 7.2
(3.4)
Mothers and children received home visits in which they were taught how
to engage in play activities using
low-cost or homemade toys, picture books, and form boards. These materials were left in the homes for the week after the visit and were changed weekly. The aims of the visits were to improve the quality of maternal-child interactions and to assist mothers to par
ticipate in
developmentally appropriate learning activities, many centered on daily
routines.
Supplementation or
routine care
Home visits delivered weekly by selected female community
leaders
An average of 63 sessions delivered over
18 mo
Stimulation group: 637
Maternal age: 28.3
(7.0)
Control group: 626
Baker
-Henningham et a
l
19 and Powell et a
l
25
Urban Jamaica
18.4 (2.4)
Undernourished children
aged 9
–
30 mo (WAZ
<
−
1.5; WAZ <
−
2.0 in
the past 3 mo; and bir
th wt >1800 g)
Maternal age: 26.0
(7.1)
Maternal education: 43.8%
completed high
school
Mothers received demonstrations on play activities involving the mother
and the child and were engaged in discussions about parenting issues. Homemade toys, books, and materials in the home were used.
Toys were left in the home each week
and exchanged at each visit.
Health clinics provide education on health and nutrition for mothers and monitor their
children
’
s growth.
Home visits delivered
by community health aids
(paraprofessionals
employed in
government health
centers)
30 min/wk; over
12 mo
Study
Sample Characteristics
Inter
vention
Setting
Child Age at Enrollment, Mean Age (SD), in mo
Par
ticipant Sample
Sizes at Enrollment for Stimulation Inter
vention
and
nonstimulation groups Maternal Age and Education Mean Values (SD), in y
or %
Stimulation Inter
vention
Control
Mode of Inter
vention
Delivery
Frequency of
Sessions; Overall
Duration
Chang et a
l
27
Jamaica, Antigua, and St Lucia
1.7 (0.3)
Recruited at 6
–
8 wk
child health visit
Maternal highest grade level: 10.1
(1.3)
Shor
t films of child development
messages were shown in the clinic waiting area, and community health workers led discussion and demonstration of the materials presented with mothers and their children. Mothers were encouraged to practice activities at home.
nurses
distributed message cards and a few
play materials.
Routine clinic visits for primary health
care
group sessions conducted by nurses at the clinic 5 sessions delivered at 3, 6, 8, 12, and 18 mo; average of 16 min each over 15 mo
Stimulation group: 251
Mothers younger
than 19 y of age: 22.7%
Control group: 250
Cooper et a
l
17
Periurban South Africa Mothers enrolled during
third
trimester pregnancy Any pregnant women within the study area
Maternal age: 25.5
(5.23)
Mothers were encouraged to engage in sensitive, responsive interactions with their infants. Items from the neonatal behavioral assessment
schedule were used to sensitize the mother to her infant
’
s individual
capacities and needs.
normal ser
vice
provided by the local infant clinic This involved fortnightly visits by a community health worker
,
who assessed the physical and
medical progress of mothers and infants, and encouraged mothers to take their infant the local clinic to be weighed, have their physical health assessed, and be immunized.
Home visits delivered
by local women selected with help from the local
community council
16 sessions held
over 6 mo, 1-h duration: 2 during pregnancy, weekly for the first 8 wk postpar
tum,
for
tnightly
for 9
–
16 wk
postpar
tum,
monthly for the remainder of
the time
Stimulation: 220 Control: 229
Hamadani et a
l
15
Rural Bangladesh
14.6 (4.5)
Undernourished children aged 6
–
24
mo (WAZ <
−
2)
Maternal
education of <5
y: 52%
Mothers were taught about child development and the impor
tance
of play. Play leader demonstrated play activities to the mothers using toys made from recycled materials; the toys were left in the homes and exchanged with new toys on the
following visit.
Standard of care
of community
nutrition centers
(1)
group meetings at community nutrition centers
and
(1) Weekly for the first 10 mo then biweekly for the last
2 mo
Stimulation group: 92
(2) Home visits delivered by local women from the
village
(2) T
wice weekly
for first 8 mo, followed by weekly home visits for 4 mo
Control group: 101
TAB
le
1
Study
Sample Characteristics
Inter
vention
Setting
Child Age at Enrollment, Mean Age (SD), in mo
Par
ticipant Sample
Sizes at Enrollment for Stimulation Inter
vention
and
nonstimulation groups Maternal Age and Education Mean Values (SD), in y
or %
Stimulation Inter
vention
Control
Mode of Inter
vention
Delivery
Frequency of
Sessions; Overall
Duration
nahar et a
l
31
and
nahar
et a
l
30
Urban Bangladesh
Age range:
6
–
24
Severely under
weight
(WAZ <
−
3)
hospitalized children
aged 6
–
24 mo
Maternal education: 3.3
(3.4)
Mothers received demonstrations on play techniques with homemade toys, and were taught how to enhance mother
-child interactions and the
impor
tance of ECD. Mothers were
loaned toys and picture books to take
home.
Food supplements or routine clinical management of the hospital comprising growth monitoring, health education, and micronutrient supplementation Individualized sessions at community clinics delivered by female health workers
(PLs)
1 h every 2 wk for
the first 3 mo, then 1 h/mo for the last 3 mo
Stimulation group: 205
Maternal age: 24.2
(5.6)
Control group: 302
Rahman et a
l
26
Rural Pakistan Mothers enrolled during
third
trimester pregnancy
All healthy women aged
17
–
40, married, in
their last trimester of pregnancy that were registered with LHWs Maternal education (y): 6.3 (3.6) (1) An initial half-day workshop on the second bir
th month stage of
development with a group of 6
–
8
mothers in which each mother was given a
“
Learning Through Play
”
calendar to take home.
Routine care including
monthly visits by LHWs in which they educate mothers on health, hygiene, and basic nutrition
education
(1) One half-day workshop with 6
–
8
mothers.
(3) Self-directed
groups
Stimulation: 194 Control: 173
Maternal age: 27.3
(4.9)
(2) During home visits, LHWs discussed
the development of the mother
’
s
child, using the calendar as the basis
for discussion.
(3) Center
-based
self-directed parenting
groups, and
(2) For
tnightly home visits (2) 12 individual sessions, 15
–
20
min held over
6 mo
(3) Mothers were encouraged to meet in
groups on their own to suppor
t each
other in the use of the techniques
outlined in the calendar
.
Singla et a
l
29
Rural Uganda
22.4 (6.4)
Children aged 12
–
36 mo
whose mothers had primary school level education or lower
Maternal age: 28.0
(7.0)
Mothers and fathers were encouraged
to learn and enact new parenting practices with their child, spouse, or peers. Sessions focused on child care (eg, play and communication), maternal self-care, the maternal relationship with the child, and the mother
’
s relationship with
her spouse. Most group sessions were for both mothers and fathers together; however
, some were
mothers only or fathers only.
Routine care; Waitlist
to receive the inter
vention
program
(1)
group sessions delivered by community volunteers and (1) Session every 2 wk, over 6 mo
(12 sessions
total)
Stimulation: 171 Control: 148 Maternal education: 3.9
(2.9)
(2) 1 or 2 home visits
(2) 1 or 2 home
visits in the latter half of the program
TAB
le
1
Study
Sample Characteristics
Inter
vention
Setting
Child Age at Enrollment, Mean Age (SD), in mo
Par
ticipant Sample
Sizes at Enrollment for Stimulation Inter
vention
and
nonstimulation groups Maternal Age and Education Mean Values (SD), in y
or %
Stimulation Inter
vention
Control
Mode of Inter
vention
Delivery
Frequency of
Sessions; Overall
Duration
Tofail et a
l
32
Rural Bangladesh
16.3 (5.8)
Children aged 6
–
24
mo with either iron deficiency anemia or who were neither anemic nor iron
deficient
Maternal age: 26.2
(5.7)
Maternal education: 5.9
(3.7)
Mothers were shown how to play with toys and interact with their
children in a way to promote their development, following a semistructured curriculum. The PLs followed a semistructured curriculum, the activities were
ordered by difficulty level, and the PLs chose the level for each child according to his or her ability to do the activities. The toys, including simple picture books, made from recycled materials were left in the homes for 1 wk and then exchanged
for different toys.
The control group was visited weekly, and mothers were asked about their
child
’
s health
status.
Home visits delivered
by PLs (women selected from the village who had 9–12 y education) Weekly home visits delivered
for 9 mo
Stimulation: 107 Control: 102
Walker et a
l
28
Urban Jamaica Enrolled as infants, in the hospital
One hundred for
ty term
(gestational age
≥
37
completed wk) LBW infants (bir
th wt
<2500 g)
Maternal age: 24.7
(7.3)
Maternal education:
primary or less (8.8%); junior secondary: 36.8%;
≥
grade
9 (54.5%)
(1) 0
–
8 wk: The inter
vention focused
on improving the mothers
’
responsiveness to their infants. The mothers were encouraged to converse with and sing to their infants, respond to their cues, show affection, and focus their attention on
the environment.
Routine care
Home visits delivered
by community health workers
(1) 1-h visit per
week
Stimulation group: 70
(2) 7
–
24 mo: The inter
vention focused
on helping the mothers more
effectively teach their children and enhance maternal-child interactions.
Community health workers
demonstrated play techniques to the mother and involved her in a play session with the child. The mothers were encouraged to play with their children between visits, include play activities in their daily
routines, and use praise and positive reinforcement, and were discouraged from using physical punishment. Toys made from commonly available recyclable materials were left in the
home each week.
(2) 7
–
24 mo:
30-min visit per
week
Control group: 70
TAB
le
1
goals and features, there were some strategies that varied across interventions. For example, Chang et al27 presented educational videos in
clinic waiting rooms and distributed reminder cards with key messages for the mothers to take home; Rahman et al26 and Aboud et al14 also
provided visual aids for mothers to be reminded of key messages at home. Only the intervention by Singla et al29
involved both mothers and fathers in group sessions and simultaneously targeted maternal well-being as a key component of the program, alongside responsive stimulation.
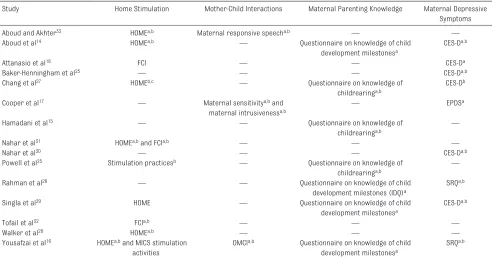
Outcome Measures
Out of the 13 unique interventions, 10 measured the quality of
stimulation in the home, 3 assessed maternal-child interaction, 7 measured maternal parenting knowledge about ECD, and 9 measured maternal depressive symptoms. Of note, there was variation in the parenting outcomes assessed within each study, as well as in the measures used for each parenting construct across studies. Table 2 presents the specific measurement tools used for each study and indicates whether there was any mention of its adaptation or reliability in the study setting. Three trials were structured to measure longer-term follow-up assessments of parenting outcomes after the completion of the intervention.17, 33, 34
For these studies, only the assessment immediately after the completion of the intervention contributed to the meta-analysis. The quality of the home caregiving environment was measured by using the HOME35 inventory in 7
studies, 14, 16, 27–29, 31, 33 the Family
Care Indicators (FCI)36 or select
subscales of the HOME inventory in 3 studies, 18, 31, 32 and a questionnaire
of caregivers’ stimulation practices in 2 studies.16, 25 For studies that
used multiple measures to evaluate the home caregiving environment,
Study
Sample Characteristics
Inter
vention
Setting
Child Age at Enrollment, Mean Age (SD), in mo
Par
ticipant Sample
Sizes at Enrollment for Stimulation Inter
vention
and
nonstimulation groups Maternal Age and Education Mean Values (SD), in y
or %
Stimulation Inter
vention
Control
Mode of Inter
vention
Delivery
Frequency of
Sessions; Overall
Duration
Yousafzai et a
l
16
Rural Pakistan
0.6 (0.6)
Any newborn children
aged <2.5 mo
Maternal education: 2.0
(3.8)
Mothers were assisted in providing
developmentally appropriate
activities to try with their child and coached to obser
ve their child
’
s
signals and respond appropriately to experience a successful interaction.
nutrition
supplementation and education or routine health care services of the LHW
program
(1) Home visits and
(1) 30 min/mo;
over 24 mo
Stimulation group: 757
Sixty-eight percent
of mothers
were illiterate.
(2)
group sessions delivered through government
’
s
community-based health worker
program
(2) 80 min/mo;
over 24 mo
Control group: 732
LBW
, low bir
th weight; LHW
, lady health worker; PL, play leader; WAZ, weight-for
-age
z
score.
TAB
le
1
we prioritized the HOME inventory measure over other measures (eg, the FCI) for estimation in the meta-analysis. Reliability of the home caregiving environment measures was mentioned in 8 out of 10 studies. Mother-child interactions were assessed in 3 studies for: maternal responsive speech during a mother-child picture-talk task, 33
maternal sensitivity and maternal intrusiveness during a free play session with the child, 17 and
mother-child interactions around a shared picture book reading activity.16, 37 We
focused on maternal sensitivity over maternal intrusiveness for better comparability in the construct with other studies. The reliability of the mother-child interaction measures was mentioned in all 3 studies. Maternal knowledge of ECD was measured in 7 studies. The authors of 4 studies captured knowledge of child development milestones, 14, 16, 26, 29 and the authors
of 3 studies captured knowledge of child rearing practices.15, 25, 27
The majority of the measures used were developed specifically for each study. The authors of only 3 out of 7 studies reported details about the reliability of the maternal knowledge questionnaire.
Finally, maternal depressive
symptoms were measured by using 3 different scales in 9 studies: the CES-D scale in 6 studies, 14, 18, 19, 27, 29, 30 the
Self Reporting Questionnaire 20-item in 2 studies, 16, 26 and the Edinburgh
Postnatal Depression Scale in 1 study.17 The reliability of the maternal
depressive symptoms measures was mentioned in 7 out of 9 studies.
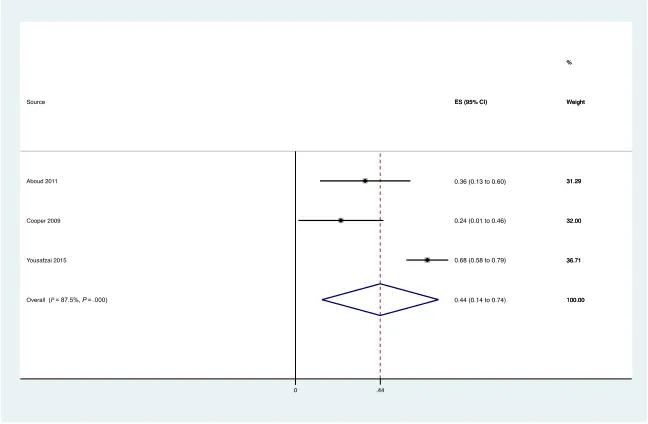
Pooled ess on Maternal Outcomes
Figures 2–5 present forest plots of posttreatment ESs, with SMDs and 95% confidence intervals (CIs) for each study. The pooled effect of stimulation interventions was significant and medium-to-large
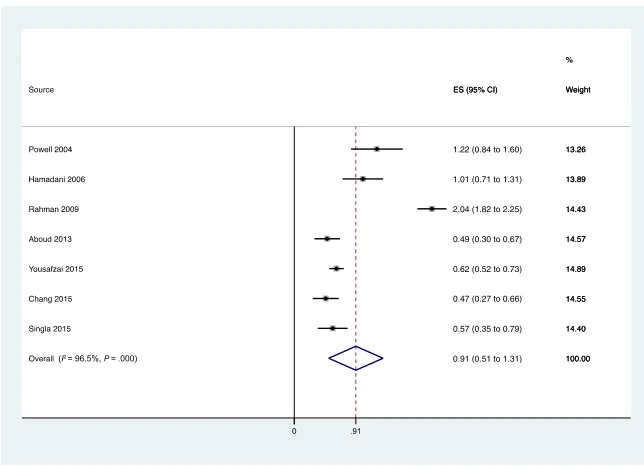
for improving the home caregiving environment (n = 10; SMD = 0.57; 95% CI, 0.37 to 0.77), mother-child interactions (n = 3; SMD = 0.44; 95% CI, 0.14 to 0.74), and maternal knowledge of ECD (n = 6; SMD = 0.91; 95% CI, 0.51 to 1.31). The pooled effect of interventions on reducing maternal depressive symptoms was not significant (n = 9; SMD = −0.10; 95% CI, −0.23 to 0.03).
heterogeneity and es Moderators
Results revealed considerable heterogeneity in pooled effects for the home caregiving environment (Q = 98.21, P < .001, I2 = 90.8%),
mother-child interactions (Q = 16.01,
P < .001, I2 = 87.5%), maternal
knowledge (Q = 169.27, P < .001,
I2 = 96.5%), and maternal depressive
symptoms (Q = 37.06, P < .001, I2 =
78.4%). Thus, several study-level variables were explored as potential moderators of the effect on the home caregiving environment, maternal knowledge of ECD, and maternal TABle 2 Measures Used for 4 Main Parenting Outcomes Categories Across Studies
Study Home Stimulation Mother-Child Interactions Maternal Parenting Knowledge Maternal Depressive Symptoms
Aboud and Akhter33 HOMEa, b Maternal responsive speecha, b — —
Aboud et al14 HOMEa, b — Questionnaire on knowledge of child
development milestonesa
CES-Da, b
Attanasio et al18 FCI — — CES-Da
Baker-Henningham et al25 — — — CES-Da, b
Chang et al27 HOMEb, c — Questionnaire on knowledge of
childrearinga, b
CES-Db
Cooper et al17 — Maternal sensitivitya, b and
maternal intrusivenessa, b —
EPDSa
Hamadani et al15 — — Questionnaire on knowledge of
childrearinga, b —
nahar et al31 HOMEa, b and FCIa, b — — —
nahar et al30 — — — CES-Da, b
Powell et al25 Stimulation practicesb — Questionnaire on knowledge of
childrearinga, b —
Rahman et al26 — — Questionnaire on knowledge of child
development milestones (IDQ)a
SRQa, b
Singla et al29 HOME — Questionnaire on knowledge of child
development milestonesa
CES-Da, b
Tofail et al32 FCIa, b — — —
Walker et al28 HOMEa, b — — —
Yousafzai et al16 HOMEa, b and MICS stimulation
activities
OMCIa, b Questionnaire on knowledge of child
development milestonesa
SRQa, b
EPDS, Edinburgh Postnatal Depression Screen; IDQ, Infant Development Questionnaire; MICS, Multiple Indicator Cluster Survey; OMCI, Observations of Mother-Child Interactions; SRQ, Self-Reporting Questionnaire. —, not applicable.
a Adapted for the study context. b Reliable for use in the study context.
depressive symptoms. Moderator analyses were not conducted for the effect on mother-child interactions, because the authors of only 3 studies assessed this outcome. None of the ESs for the home caregiving environment, maternal knowledge, or maternal depressive symptoms differed significantly by any of the examined moderators (Supplemental Information, Supplemental Table 4).
DIsCussIOn
This systematic review and meta-analysis identified and evaluated randomized controlled studies of interventions that were conducted to encourage stimulation between caregivers and children younger than 2 years of age in LMICs. We specifically investigated the effects of these interventions on improving parenting outcomes. Results revealed positive, medium-to-large effects on the home caregiving environment, maternal knowledge, and mother-child interactions, whereas null effects were found for maternal mental health. There was notable heterogeneity in estimated treatment effects on all 4 parenting outcomes. The authors of a previous review study of stimulation interventions in LMICs, 8 and of a meta-analysis
of intervention effects on ECD outcomes, 6 highlighted heterogeneity
in effects and emphasized several aspects of implementation and behavior change techniques that vary across these interventions. Exploratory moderator analyses revealed no significant differences in the effectiveness of these programs on the home caregiving environment, maternal knowledge, or maternal depressive symptoms by any of the examined characteristics. However, because few studies were included in moderator categories, our power to assess conditional differences in effectiveness was limited. Additional intervention studies are required to more conclusively determine if
the benefits of these programs for parenting skills are comparable across these various factors.
Although we found that parenting interventions principally focused on stimulation are effective in improving the home caregiving environment,
mother-child interactions, and maternal knowledge, we did not find evidence to support that these programs also universally brought about changes in maternal mental health.38 This could be explained
by the fact that the primary focus of stimulation interventions is
FIGuRe 2
Forest plot for effect of stimulation interventions on the home caregiving environment. Weights are from random effects analysis.
FIGuRe 3
to enhance positive caregiving behaviors with the goal of improving child development, with less of a direct focus on intervening on maternal mental health. In fact, although 9 interventions measured changes in maternal depressive
symptoms, only the intervention evaluated by Singla et al29 explicitly
targeted maternal depression as a primary outcome. Their particular intervention integrated principles of cognitive behavioral theory (eg, group discussions around building
positive relationships with family members and developing strategies for conflict resolution and emotion regulation; with opportunities to practice) with responsive stimulation and nutrition. This study’s authors found the largest reductions in maternal depressive symptoms (in addition to improvements in the home caregiving environment and maternal knowledge of ECD).29 Of note, the
nonsignificant pooled ES on maternal depression could also be attributable to a lack of power within each study to detect differences in this caregiver outcome. Considering the inextricable links between mothers’ emotional well-being, parenting capacities, and early childhood development, 39, 40
integrated and theoretically-informed programs that simultaneously target both maternal mental health and caregiving behaviors may be an effective strategy for amplifying impacts on both maternal and ECD outcomes.41
In light of our findings, a number of limitations should be noted. First, the early childhood stimulation body of literature is small, and only 13 interventions met our inclusion criteria, thereby reducing the power to estimate pooled intervention effects. Second, the small number of studies limited the power of our exploratory moderator analyses. Additionally, for some moderator analyses, there were no clearly established cutoff points for certain study-level characteristics (eg, intervention duration), and several cut points (eg, < or ≥12 months in duration) were determined to be conditional on the specific studies included in the review. As a result, the robustness of these moderators should be explored with future studies and alternative cut points. Third, although all interventions were focused on enhancing stimulation between the caregiver and child, there were notable differences among studies in terms of study population, intervention
FIGuRe 4
Forest plot for effect of stimulation interventions on maternal knowledge of ECD. Weights are from random effects analysis.
FIGuRe 5
curriculum, and delivery strategies that we could not quantitatively account for in this study. Finally, outcome measures were evaluated by using different assessment tools across different durations of time, which may have affected comparability across studies. For example, the HOME inventory, FCI, and questionnaires about caregivers’ stimulation practices have been used to evaluate changes in the home caregiving environment. Of note, only the HOME inventory incorporates direct observation with caregiver-report, whereas the FCI and other questionnaires are entirely caregiver-reported. Questionnaires on maternal knowledge of ECD were specifically designed for each study, and most did not indicate details about the development or reliability of the tool used. Moreover, these questionnaires were focused either on knowledge of child development milestones or caregiving practices, representing 2 distinct domains of parenting knowledge. In our review, we highlight the critical need for advancements in measurement of caregiving outcomes, so that tools are not only relevant across programs and cultural contexts but also
standardized to some degree to enable valid comparisons across studies. Despite the limitations, with our review and meta-analysis, we are the first to date to synthesize the impact of stimulation intervention on parenting outcomes in LMICs. In a body of literature that is rapidly growing, our review reveals several methodological areas that are worthy of future research attention. The dimensions of caregiving evaluated have been limited and inconsistent across studies. Of the 20 unique trials included in a previous meta-analysis6
regarding the effects of stimulation interventions on children’s early cognitive development, only 7 were conducted to evaluate changes in at least 1 parenting outcome. In the majority of trials included in our
study, the authors measured only 1 or 2 caregiving constructs. The authors of more recent studies have begun to examine 3 or more distinct parenting outcomes.14, 16, 27, 29
The Lancet ECD series has
conceptualized nurturing care as the anchor of successful ECD interventions.3 In the proposed
nurturing care framework, 3 pathways through which early child interventions can promote optimal caregiving practices are suggested: (1) strengthening parents’
knowledge, attitudes, practices, skills, and behaviors to provide children with care for development, feeding, health, security, and opportunities for early learning; (2) fostering an enabling environment to support parenting (eg, reducing parenting stress, building social support, managing conflict in the home); and (3) increasing access to quality services that support families with young children to provide optimal care (eg, linkages with social protection and poverty alleviation programs). Promoting interactions that are responsive, emotionally supportive, and developmentally stimulating directly targets the first of these theorized nurturing care pathways. However, little is known about the extent to which stimulation interventions as well as other early childhood programs impact the second and third theorized nurturing care pathways. The authors of future studies should expand the scope of stimulation interventions by adopting a holistic nurturing care framework to maximize intervention impacts on parents’ behaviors and their young children’s development and well-being outcomes. In addition, fathers, older siblings, and grandparents also provide nurturing care for young children. Future intervention studies should target and engage fathers and other primary caregivers and evaluate changes in multiple caregivers’ parenting practices in order to understand and
promote family-inclusive approaches to nurturing care and ECD.
COnClusIOns
This study is the first systematic review and meta-analysis to investigate the effectiveness of early childhood stimulation interventions on caregiving outcomes. We found medium-to-large effects of stimulation interventions on improving the home caregiving environment, observed mother-child interactions, and maternal knowledge of ECD. We found a nonsignificant effect of stimulation interventions on maternal depressive symptoms. The authors of many trials to date have not consistently or comprehensively evaluated changes in parenting outcomes. A holistic and standardized assessment of parenting outcomes can inform the caregiving mechanisms by which early childhood parenting programs benefit children's development and the design of the most impactful interventions.
ACknOwleDGMenTs
We acknowledge the study authors who responded to our inquiries and sent us data.
ABBRevIATIOns
CES-D: Center for Epidemiologic Studies Depression CI: confidence interval ECD: early child development ES: effect size
FCI: Family Care Indicators HOME: Home Observation for
Measurement of the Environment
LMIC: low- and middle-income countries
ReFeRenCes
1. Lu C, Black MM, Richter LM. Risk of poor development in young children in low-income and middle-income countries: an estimation and analysis at the global, regional, and country level. Lancet Glob Health. 2016;4(12):e916–e922
2. Walker SP, Wachs TD, gardner JM, et al; International Child Development Steering group. Child development: risk factors for adverse outcomes in developing countries. Lancet. 2007;369(9556):145–157
3. Britto PR, Lye SJ, Proulx K, et al; Early Childhood Development Interventions Review group, for the Lancet Early Childhood Development Series Steering Committee. nurturing care: promoting early childhood development. Lancet. 2017;389(10064):91–102
4. Engle PL, Fernald LC, Alderman H, et al; global Child Development Steering group. Strategies for reducing inequalities and improving developmental outcomes for young children in low-income and middle-income countries. Lancet. 2011;378(9799):1339–1353 5. Eshel n, Daelmans B, de Mello MC,
Martines J. Responsive parenting: interventions and outcomes. Bull World Health Organ. 2006;84(12):991–998 6. Aboud FE, Yousafzai AK. global health
and development in early childhood.
Annu Rev Psychol. 2015;66:433–457 7. Britto PR, Ponguta LA, Reyes C, Karnati
R. A Systematic Review of Parenting Programmes for Young Children in Low- and Middle-Income Countries. new York, nY: United nations Children’s Fund; 2015
8. Yousafzai AK, Aboud F. Review of implementation processes for integrated nutrition and psychosocial
stimulation interventions. Ann N Y Acad Sci. 2014;1308:33–45
9. Rao n, Sun J, Chen EE, Ip P. Effectiveness of early childhood interventions in promoting cognitive development in developing countries: a systematic review and meta-analysis.
Hong Kong J Paediatr. 2017;22: 14–25
10. Parks PL, Smeriglio VL. Relationships among parenting knowledge, quality of stimulation in the home and infant development. Fam Relat. 1986;35(3):411–416
11. Benasich AA, Brooks-gunn J. Maternal attitudes and knowledge of child-rearing: associations with family and child outcomes. Child Dev. 1996;67(3):1186–1205
12. Bornstein MH. Determinants of parenting. In: Cicchetti D, ed.
Developmental Psychopathology. Vol. 4. 3rd ed. Hoboken, nJ: John Wiley & Sons, Inc; 2016:180–270
13. Bornstein MH, Putnick DL. Cognitive and socioemotional caregiving in developing countries. Child Dev. 2012;83(1):46–61
14. Aboud FE, Singla DR, nahil MI, Borisova I. Effectiveness of a parenting program in Bangladesh to address early childhood health, growth and development. Soc Sci Med. 2013;97:250–258
15. Hamadani JD, Huda Sn, Khatun F, grantham-Mcgregor SM. Psychosocial stimulation improves the development of undernourished children in rural Bangladesh. J Nutr. 2006;136(10):2645–2652
16. Yousafzai AK, Rasheed MA, Rizvi A, Armstrong R, Bhutta ZA. Parenting skills and emotional availability: an
RCT. Pediatrics. 2015;135(5). Available at: www. pediatrics. org/ cgi/ content/ full/ 135/ 5/ e1247
17. Cooper PJ, Tomlinson M, Swartz L, et al. Improving quality of mother-infant relationship and infant attachment in socioeconomically deprived community in South Africa: randomised controlled trial. BMJ. 2009;338:b974
18. Attanasio OP, Fernández C, Fitzsimons EO, grantham-Mcgregor SM, Meghir C, Rubio-Codina M. Using the infrastructure of a conditional cash transfer program to deliver a scalable integrated early child development program in Colombia: cluster randomized controlled trial [published correction appears in BMJ. 2014;349:g6126]. BMJ. 2014;349: g5785
19. Baker-Henningham H, Powell C, Walker S, grantham-Mcgregor S. The effect of early stimulation on maternal depression: a cluster randomised controlled trial. Arch Dis Child. 2005;90(12):1230–1234
20. Baker-Henningham H, López Bóo F. Early Childhood Stimulation Interventions in Developing Countries: A Comprehensive Literature Review. Bonn, germany: IZA; 2010
21. Black MM, Walker SP, Fernald LCH, et al; Lancet Early Childhood Development Series Steering Committee. Early childhood development coming of age: science through the life course. Lancet. 2017;389(10064):77–90
22. Moher D, Liberati A, Tetzlaff J, Altman Dg; PRISMA group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement.
PLoS Med. 2009;6(7):e1000097 23. Higgins JP, Altman Dg, gøtzsche PC,
et al; Cochrane Bias Methods group; Address correspondence to Joshua Jeong, MSc, Department of global Health and Population, Harvard T.H. Chan School of Public Health, 665 Huntington Ave, 11th floor, Boston, MA 02115. E-mail: [email protected]
PEDIATRICS (ISSn numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2018 by the American Academy of Pediatrics
FInAnCIAl DIsClOsuRe: The authors have indicated they have no financial relationships relevant to this article to disclose. FunDInG: no external funding.
Cochrane Statistical Methods group. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928
24. Stata [computer program]. Version 13. College Station, TX; StataCorp: 2013 25. Powell C, Baker-Henningham H, Walker
S, gernay J, grantham-Mcgregor S. Feasibility of integrating early stimulation into primary care for undernourished Jamaican children: cluster randomised controlled trial.
BMJ. 2004;329(7457):89
26. Rahman A, Iqbal Z, Roberts C, Husain n. Cluster randomized trial of a parent-based intervention to support early development of children in a low-income country. Child Care Health Dev. 2009;35(1):56–62
27. Chang SM, grantham-Mcgregor SM, Powell CA, et al. Integrating a parenting intervention with routine primary health care: a cluster randomized trial.
Pediatrics. 2015;136(2):272–280 28. Walker SP, Chang SM, Powell CA,
grantham-Mcgregor SM. Psychosocial intervention improves the development of term low-birth-weight infants.
J Nutr. 2004;134(6):1417–1423 29. Singla DR, Kumbakumba E, Aboud FE.
Effects of a parenting intervention to address maternal psychological wellbeing and child development and growth in rural Uganda: a community-based, cluster randomised trial. Lancet Glob Health. 2015;3(8):
e458–e469
30. nahar B, Hossain I, Hamadani JD, Ahmed T, grantham-Mcgregor
S, Persson LA. Effect of a food supplementation and psychosocial stimulation trial for severely malnourished children on the level of maternal depressive symptoms in Bangladesh. Child Care Health Dev. 2015;41(3):483–493
31. nahar B, Hossain MI, Hamadani JD, Ahmed T, grantham-Mcgregor S, Persson LA. Effects of psychosocial stimulation on improving home environment and child-rearing practices: results from a community-based trial among severely
malnourished children in Bangladesh.
BMC Public Health. 2012;12:622 32. Tofail F, Hamadani JD, Mehrin F, Ridout
DA, Huda Sn, grantham-Mcgregor SM. Psychosocial stimulation benefits development in nonanemic children but not in anemic, iron-deficient children. J Nutr. 2013;143(6): 885–893
33. Aboud FE, Akhter S. A
cluster-randomized evaluation of a responsive stimulation and feeding intervention in Bangladesh. Pediatrics. 2011;127(5). Available at: www. pediatrics. org/ cgi/ content/ full/ 127/ 5/ e1191
34. Yousafzai AK, Obradović J, Rasheed MA, et al. Effects of responsive stimulation and nutrition interventions on children’s development and growth at age 4 years in a disadvantaged population in Pakistan: a longitudinal follow-up of a cluster-randomised factorial effectiveness trial. Lancet Glob Health. 2016;4(8):e548–e558 35. Caldwell BM, Bradley RH. Home
Observation for Measurement of the
Environment. Little Rock, AR: University of Arkansas at Little Rock; 1984 36. Hamadani JD, Tofail F, Hilaly A, Huda
Sn, Engle P, grantham-Mcgregor SM. Use of Family Care Indicators and their relationship with child development in Bangladesh. J Health Popul Nutr. 2010;28(1):23–33
37. Rasheed MA, Yousafzai AK. The development and reliability of an observational tool for assessing mother-child interactions in field studies- experience from Pakistan. Child Care Health Dev. 2015;41(6):1161–1171
38. nylen KJ, Moran TE, Franklin CL, O’hara MW. Maternal depression: a review of relevant treatment approaches for mothers and infants. Infant Ment Health J. 2006;27(4):327–343 39. Herba CM, glover V, Ramchandani Pg,
Rondon MB. Maternal depression and mental health in early childhood: an examination of underlying mechanisms in low-income and middle-income countries. Lancet Psychiatry. 2016;3(10):983–992
40. goodman SH, garber J. Evidence-based interventions for depressed mothers and their young children. Child Dev. 2017;88(2):368–377
DOI: 10.1542/peds.2017-3510 originally published online March 2, 2018;
2018;141;
Pediatrics
Joshua Jeong, Helen O. Pitchik and Aisha K. Yousafzai
A Meta-analysis
Stimulation Interventions and Parenting in Low- and Middle-Income Countries:
Services
Updated Information &
http://pediatrics.aappublications.org/content/141/4/e20173510
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/141/4/e20173510#BIBL
This article cites 37 articles, 11 of which you can access for free at:
Subspecialty Collections
alth_sub
http://www.aappublications.org/cgi/collection/international_child_he International Child Health
milestones_sub
http://www.aappublications.org/cgi/collection/growth:development_ Growth/Development Milestones
al_issues_sub
http://www.aappublications.org/cgi/collection/development:behavior Developmental/Behavioral Pediatrics
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2017-3510 originally published online March 2, 2018;
2018;141;
Pediatrics
Joshua Jeong, Helen O. Pitchik and Aisha K. Yousafzai
A Meta-analysis
Stimulation Interventions and Parenting in Low- and Middle-Income Countries:
http://pediatrics.aappublications.org/content/141/4/e20173510
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2018/02/28/peds.2017-3510.DCSupplemental
Data Supplement at:
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.