Gezondheidsraad
H e a l t h C o u n c i l o f t h e N e t h e r l a n d s
To the State Secretary of Housing, Spatial Planning and the Environment
Subject : Asbestos
Your reference : DGM/SAS/2006229816 Our reference : I-187/SD/db/819-A
Enclosure(s) : 1
Date : May 9, 2006
State Secretary,
The results of a study into cases of pleural cancer (pleural mesothelioma) in the Goor region
of the Netherlands were published in 2005.1,2 From the 1930s to the 1970s, asbestos was
used to pave roads and yards in that region. In the course of their research, Erasmus MC, the Integraal Kankercentrum Stedendriehoek Twente (Integrated Cancer Centre of the City Triangle Region, Twente), and hospitals in the province of Twente found increased incidences of this condition. In women, the incidence was five times higher than in the rest of the population, while in men it was twice as high. According to this study, there is a strong indication that environmental exposure to asbestos has been a major factor in the occurrence of pleural mesothelioma in fifteen women who lived in the Goor region.
This prompted you to contact the Health Council of the Netherlands on 2 February 2006. You asked the Council to determine whether the findings concerning this form of non-occupational exposure necessitate a revision of the Maximum Permissible Risk (MPR) and of the Negligible Risk (NR) for asbestos. I have formulated a second, supplementary question. Does the level of knowledge after 1987, when the risks were identified, indicate that the standards should be revised?
I submitted these questions to the Committee on the Evaluation of the Carcinogenicity of Chemical Substances and to the Standing Committee on Health and Environment. In responding to these questions, the Committee and the Standing Committee were supported by Prof. D.J.J. Heederik and Dr. J.H. van Wijnen. You will find details of their main conclusions in this advisory memorandum. A background note is attached. There you can read a more detailed account of the findings and considerations that underpin this Health Council advisory report.
Gezondheidsraad
H e a l t h C o u n c i l o f t h e N e t h e r l a n d s
Subject : Asbestos
Our reference : I-187/SD/db/819-A
Page : 2
Date : May 9, 2006
Does the study carried out in the Goor region necessitate a review of the MPR and NR?
The Health Council takes the view that the study into the occurrence of non work-related mesothelioma is of good quality. The Committee endorses the conclusion that the additional cases of pleural mesothelioma are most likely the result of environmental exposure. Dr A. Burdorf, the first author of the report on exposure in the Goor region, gave a presentation during a meeting of the Committee on the Evaluation of the Carcinogenicity of Chemical Substances. The task of estimating exposure to asbestos was not initially part of his assignment, which meant that it was very limited in nature. To verify the number of cases of pleural mesothelioma found, the study looked at the number of cases of mesothelioma that would be expected to result from the estimated exposure on the basis of a risk analysis
technique developed by Hodgson and Darnton.3 The authors of the Erasmus MC report had
not planned to evaluate the MPR and NR values.
Both the Committee and the Standing Committee feel that it is not possible to adequately estimate past levels of asbestos exposure on the basis of the available data. In the study, exposure was estimated on the basis of the measured asbestos emissions from a single road. This one series of measurements cannot be seen as representative of asbestos emissions throughout the entire region. A more serious objection is that emission
measurements do not reliably reflect the level of exposure experienced by women who have lived in the Goor region. For instance, such exposure is not only dependent on the quantity of asbestos fibres released by roads and yards (emissions), it is also influenced by the frequency of exposure (how often, and for how long, people have been in contact with the fibres) and by the type of contact involved (walking, cycling, or when driving a vehicle). Exposure can also occur at home, due to fibres blown in by the wind or brought in on clothing and footwear. A reliable estimate of exposure to asbestos fibres is only possible where personal measurements of the indoor and outdoor environments have been made in the past, over a protracted period of time.
How does this restriction affect the issue of a possible revision of the MPR and NR limit values? It is no longer possible to retroactively determine the level of asbestos exposure in the Goor region, so it is impossible to establish what level of exposure resulted in disease in that area. Accordingly, it cannot be concluded from the study conducted by the Erasmus MC, the Integrated Cancer Centre of the City Triangle Region, Twente, and hospitals in the
Gezondheidsraad
H e a l t h C o u n c i l o f t h e N e t h e r l a n d s
Subject : Asbestos
Our reference : I-187/SD/db/819-A
Page : 2
Date : May 9, 2006
Is a review of the MPR and NR required on the basis of the current level of knowledge?
The study in the Goor region therefore provides no guidance in assessing the current limit values for exposure to asbestos. Since 1987, when the MPR and NR values were established
on the basis of proposals in the RIVM’s4 asbestos criteria document, have new insights and
knowledge become available which might indicate a need for revision?
The Council concludes that this is indeed the case. The most important new publications
are a meta-analysis by Hodgson and Darnton3 published in the year 2000, and an EPA5
report published in 2003. Hodgson and Darnton’s meta-analysis is based on a large number of studies, some of which were not published until after 1987. After a comprehensive consideration of all available studies, the EPA report concluded that the cancer risk is mainly determined by asbestos fibres that are more than 10 µm in length. The current standards are based on the view that a significant increase in risk is associated with fibres that are more than 5 µm in length.
How to proceed?
The recent study into cases of mesothelioma in the Goor region, following exposure to asbestos, has not produced sufficient information for an evaluation of the current limit values. Happily, the requisite information is available in the form of knowledge and insights obtained since 1987. The Committee and the Standing Committee have concluded that a review of the MPR and NR limit values is required.
How should this be tackled? I would suggest to you that a revision of the existing MPC be carried out by the Health Council’s Committee on the Evaluation of the Carcinogenicity of Chemical Substances. This Committee is prepared to start work at the earliest
opportunity, and to deliver a proposal for a new value by the middle of next year. Yours sincerely,
(signed)
Prof. J.A. Knottnerus,
Background information to the
advisory letter on asbestos
to:
the State Secretary of Housing, Spatial Planning and the Environment No. 2006/09E, The Hague, May 9, 2006
The Health Council of the Netherlands, established in 1902, is an independent scientific advisory body. Its remit is “to advise the government and Parliament on the current level of knowledge with respect to public health issues and health (services) research...” (Section 22, Health Act).
The Health Council receives most requests for advice from the Ministers of Health, Welfare & Sport, Infrastructure & the Environment, Social Affairs & Employment, Economic Affairs, Agriculture & Innovation, and Education, Culture & Science. The Council can publish advisory reports on its own initiative. It usually does this in order to ask attention for developments or trends that are thought to be relevant to government policy.
Most Health Council reports are prepared by multidisciplinary committees of Dutch or, sometimes, foreign experts, appointed in a personal capacity. The reports are available to the public.
This report can be downloaded from www.healthcouncil.nl. Preferred citation:
Health Council of the Netherlands. Asbest. The Hague: Health Council of the Netherlands, 2006; publication no. 2006/09E.
all rights reserved
The Health Council of the Netherlands is a member of the European Science Advisory Network for Health (EuSANH), a network of science advisory bodies in Europe.
I N A H TA
The Health Council of the Netherlands is a member of the International Network of Agencies for Health Technology Assessment (INAHTA), an international collaboration of organisations engaged with health technology assessment.
Contents
1 Introduction 5
1.1 Background 5
1.2 Requests for advice 6
1.3 Types of asbestos 7
1.4 Asbestos-paved roads: history, extent, composition 7
2 Does the study carried out in the Goor region necessitate a review of the standards? 9
2.1 The researchers’ findings 9
2.2 Description of the method used to estimate exposure 12
2.3 Comments on the method used to estimate exposure 13
2.4 Conclusion 14
3 Is reform of the standards required, based on the current level of knowledge? 17
3.1 Method used to derive standards 17
3.2 View of new findings 18
3.3 Conclusion 20
References 21
Annexes 23
A Request for advice 25
1
ChapterIntroduction
1.1 Background
The request for a Health Council advisory report on asbestos was prompted by a study carried out in the Goor region, by Erasmus MC and the Integrated Cancer Centre of the City Triangle Region, Twente, in collaboration with hospitals in the province of Twente. From the 1930s to the 1970s, asbestos was used to pave roads and yards in that region.
The first partial report reveals that the incidence of pleural mesothelioma (pleural cancer) in the area around Goor is higher than in the rest of the Netherlands (almost five times higher for women and two times higher for
men).1 This is a strong indication that environmental exposure to asbestos has
been a major factor in the greatly increased incidence of pleural cancer in the risk area. This is particularly true of women, as they are generally less exposed to asbestos in the course of professional activities.
The second partial report concluded that, in the cases of fifteen women, exposure to asbestos in the environment (from roads and yards that had been paved with asbestos) from 1989 to 2003 was the most likely cause of the
1.2 Requests for advice
In response to these reports, the State Secretary of the Ministry of Housing, Spatial Planning and the Environment asked the Health Council to determine whether the findings in question indicate that the current limit values for asbestos exposure should be reviewed (Annex A). Accordingly, the first question to be addressed in the advisory memorandum is:
1 Does the epidemiological study into non work-related cases of mesothelioma
in the Goor region necessitate a review of the Dutch government’s standards concerning acceptable risks in the tolerance of asbestos in society, i.e. the NR
(Negligible Risk) and the MPR (Maximum Permissible Risk)?*
Furthermore, information that has become available since the publication of the National Institute for Public Health and the Environment's (RIVM) criteria document on asbestos in 1987 has been examined to determine whether this might necessitate a review of the standards derived from that document. Accordingly, the advisory memorandum addresses the following question:
2 Does the current level of knowledge indicate that the NR and the MPR are in
need of revision?
Should revision prove to be necessary, then the State Secretary asks how this might best be achieved:
3 How much time would the Health Council require to prepare a possible
advisory report on a new standard for dealing with asbestos in Dutch society? The main information on which the Health Council bases its response to the first question is contained in section 2 of this memorandum. Section 3 sets out the answer to the second question, and the grounds on which this is based. This section concludes by setting out recommendations on how a possible review might be tackled.
* Deze voetnoot is weggevallen. In het Nederlands stond er: De MTR en VR zijn – conform het risicobeleid – concentraties die overeenkomen met een risico dat één op de miljoen respectievelijk honderd miljoen mensen per jaar een kwaadaardige tumor krijgt als gevolg van de blootstelling aan die stof.
1.3 Types of asbestos
Asbestos is a collective name for six groups of mineral fibres. The groups of fibres are divided into serpentines (chrysotile: white asbestos) and amphiboles (the other five groups). The most important amphiboles are amosite (brown asbestos), and crocidolite (blue asbestos). In commercial terms, white asbestos (chrysotile) is by far the most widely used type. Crocidolite (blue asbestos) is
generally assumed to be significantly more carcinogenic than chrysotile.4-8
1.4 Asbestos-paved roads: history, extent, composition
From the 1930s to the early 1970s, asbestos cement waste was widely used to pave roads and yards within a radius of about fifteen kilometres of the Eternit asbestos cement plant at Goor. The waste, which people were able to collect free of charge at the asbestos cement plant, consisted of waste and rejected batches of asbestos cement sheets, as well as waste and turnings from piping. This material
had been broken down into small pieces in a crusher.9
The Centre for Environmental Sciences estimates that, in total, about 83 roads
and yards were involved, with an estimated area of 33,500 square metres.10 The
thicknesses of the layers varied from a few centimetres up to as much as one meter. Based on the percentage of waste from the production process, TNO (the Netherlands Organisation for Applied Scientific Research) has estimated that a total of 360 to 4,400 tons of solid asbestos waste was generated (assuming an
average asbestos content of 10 percent).11 The waste can contain both chrysotile
2
ChapterDoes the study carried out in the Goor
region necessitate a review of the
standards?
2.1 The researchers’ findings
The study focused mainly on cases of mesothelioma in women, as this group involved very little work-related exposure (the most common form of exposure). Any cases in which there was even the slightest reason to suspect that
occupational exposure might have been involved were excluded from the analysis. For example, women whose partner worked at Eternit could have been exposed to asbestos fibres shed from their partner’s clothing. Fifteen cases of mesothelioma in women from the Goor region are attributed to asbestos exposure in those surroundings.
In addition, an estimate was made of the average exposure experienced by the 75,000 women in the risk area. For the purposes of this estimate, the authors used the concentrations of asbestos fibres measured by TNO near an
asbestos-paved road in the Goor region in 1987.11 They then determined how many cases
of mesothelioma would be expected to result from this estimated exposure, using
a risk analysis technique developed by Hodgson and Darnton.3
With reference to the TNO report, the authors (from the Erasmus Medical Centre) make the following assumption on exposure:
With regard to the situation in the Goor risk area, the authors of this (!) report estimated that, in the course of an entire year, anyone who walked, cycled or drove over asbestos-paved yards and roads on a daily basis experienced an average asbestos exposure of about 3,000 fibres/m3. This estimate is based on the median value of the calculated distribution of asbestos measurements for an entire week (Seven 24-hour days). We therefore estimate that one year of exposure at this level has resulted in an average cumulative exposure of 0.003 fibre-years. (0.003 fibre/ml-year)
The study estimated the average duration of exposure for women in the mesothelioma risk area at 37.6 years. Multiplying the exposure time by the exposure concentration gives a cumulative exposure of 0.11 fibre-years.
This value is then used for a comparison with Hodgson’s risk analysis technique. In their own risk analysis, the researchers assumed that all 75,000 women in the risk area were exposed to 0.11 fibre-years.
The researchers conclude that the number of cases of mesothelioma in Goor corresponds to the number of cases projected by the risk analysis on the basis of that estimated concentration. They further note that the number of cases seen in the Goor region roughly corresponds to the number of cases that would be expected if exposure was approximately equal to the MPR. The MPR value is defined as the concentration corresponding to the risk that, per year, one in every million people exposed to the substance in question will develop a malignant tumour.
Units and measures of exposure to asbestos
Asbestos concentrations are expressed as fibres/m3 (per square meter) or fibres/ml. Concentration values are sometimes accompanied by details of the measurement method used to obtain them: phase contrast microscopy (PCM) or transmission electron microscopy (TEM) (see box: measurements of asbestos by PCM and TEM).
In the case of asbestos, it is assumed that the occurrence of effects correlates with cumulative exposure (the product of the concentration multiplied by the number of years of exposure). The resulting measure is expressed as fibre-years per ml. Accordingly, cumulative exposures are almost always expressed as fibre-years per ml, not per m3. The unit used in the main table in Hodgson’s meta-analysis (Table 11), for example, is fibre/ml.years. This value refers to a cumulative lifetime exposure, measured using PCM.
Measurements of asbestos using phase contrast microscopy and electron microscopy
An air pump is used to collect air samples, after which any airborne fibres are trapped by a filter. The fibres are then counted by light microscopy or electron microscopy.
A few decades ago, these counts were made using ordinary light microscopes, at a magnification of 400 times. Later on, improved measurements in the working environment involved the use of Phase Contrast Microscopes, usually at a magnification of 1,250 times. The advantage of Phase Contrast Microscopy is that it enables measurements to be made more quickly and more cheaply. However, Phase Contrast Microscopy (PCM) can only be used to measure fibres that are longer than 5 µm, and that have a length:thickness ratio that is equal to, or greater than, 3:1. Small fibres and long, thin fibres cannot be detected using this technique. Moreover, this method cannot distinguish the individual fibres in bundles of fibres, which are then counted as a single fibre. The different types of asbestos cannot be distinguished from one another using PCM. Moreover, this technique is unable to distinguish asbestos fibres from fibres of other substances.
Both scanning and transmission electron microscopy provide reliable counts of asbestos fibres. Transmission electron microscopy is the technique most commonly used for this purpose. Electron microscopy provides much higher magnifications (at very high resolution) than is possible using light microscopy. This technique therefore enables fibres that are less than 5 µ m in size to be easily resolved, as well as very thin fibres. It also enables the individual fibres in a bundle to be counted reliably. Asbestos measurements obtained using TEM are often combined with those obtained using other measurement techniques (energy dispersive X-ray analysis) which also enables different types of asbestos to be identified, on the basis of differences in chemical composition. Such techniques can also distinguish asbestos fibres from fibres of other substances. One disadvantage of using a TEM for asbestos measurements is that only a very small part of the preparation is examined. As a result, these counts are of only limited accuracy.
The use of electron microscopy is stipulated for environmental samples. This makes it possible to identify the various types of asbestos, and to distinguish asbestos fibres from fibres of other substances. In the past, measurements in the workplace were generally performed using phase contrast microscopy. In such cases, the type of asbestos involved was known and the preference was for a quick and inexpensive measurement. In general, the use of PCM can produce substantial underestimates of the number of asbestos fibres in a sample. One exception is the situation (as is so often the case with measurements of indoor air) in which there are many airborne fibres of substances other than asbestos (such as wool, cotton, and glass).
Based on these findings, therefore, there would be no reason to review the MPR value. However, there is some question concerning the firmness of the conclusions about exposure. The researchers too point out a number of limitations in this matter.
2.2 Description of the method used to estimate exposure
The estimated asbestos exposure for the 75,000 women who live in the risk area
around Goor is based entirely on measurements carried out by TNO.11
Long-term measurements
In 1985 and 1986, TNO made a series of long-term measurements near a road in the Goor region (Diepenheim). Following the publication of the initial results of this analysis, in 1985, no more measurements were made. This was due to heavy rainfall, which prevented fibres from becoming airborne, thereby producing measured values that were at or below the detection limit. In 1986, long-term measurements were made close to three roads between late April and late September. Each month, four weekly samples were pooled. The concentration was subsequently determined using both electron microscopy and light microscopy.
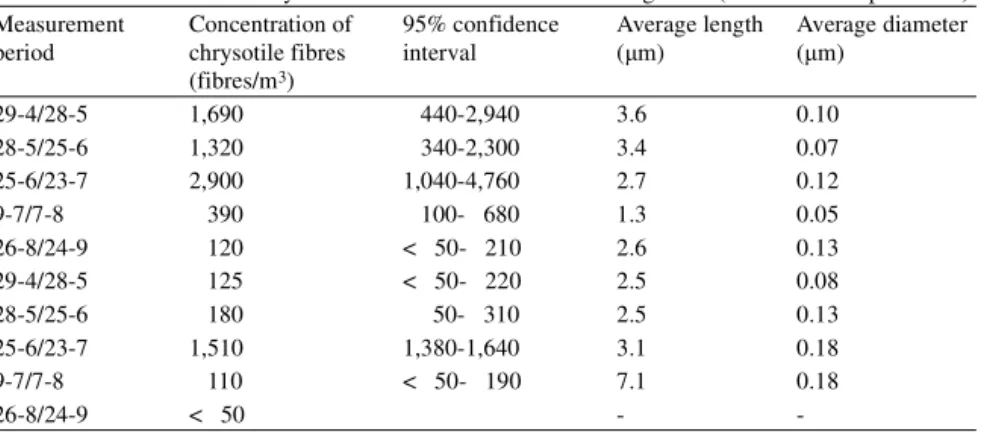
The results of the measurements of chrysotile and crocidolite a few meters from the road (on which the researchers based their exposure estimate) are shown in Table 1. Both at the measuring point (one hundred meters from the road) and at the reference point, all the measured values were just above or below the detection limit.
Table 1 Concentrations of chrysotile and crocidolite measured using TEM (source TNO report 1987). Measurement period Concentration of chrysotile fibres (fibres/m3) 95% confidence interval Average length (µm) Average diameter (µm) 29-4/28-5 1,690 440-2,940 3.6 0.10 28-5/25-6 1,320 340-2,300 3.4 0.07 25-6/23-7 2,900 1,040-4,760 2.7 0.12 9-7/7-8 390 100- 680 1.3 0.05 26-8/24-9 120 < 50- 210 2.6 0.13 29-4/28-5 125 < 50- 220 2.5 0.08 28-5/25-6 180 50- 310 2.5 0.13 25-6/23-7 1,510 1,380-1,640 3.1 0.18 9-7/7-8 110 < 50- 190 7.1 0.18 26-8/24-9 < 50 -
-Short-term measurements
Short-term measurements were also carried out near three roads during a very dry period. These measurements were made right beside and above the road, to gain insight into the concentrations of asbestos in the air when cars were using the road. The results of these measurements are shown in Table 2.
Near the Hazendammerweg (the same road that was used for the long-term measurements), chrysotile concentrations ranging from 20,000 to 50,000 fibres
per m3 were measured. These measurements were made by means of phase
contrast microscopy.
In the TNO study, the long-term measurements were made using both TEM and PCM. The researchers note that only 4 percent of the chrysotile fibres analysed using a transmission electron microscope were detectable with a light microscope. Translated to the short-term measurements, this means that the air actually contained an estimated 500,000 to 1,250,000 chrysotile fibres (as measured by TEM). This indicates that there can be an extremely large variation in concentrations, as the highest value obtained with the short-term
measurements is over 400 times higher than the highest average monthly value.
2.3 Comments on the method used to estimate exposure
In partial report 2, the researchers point out that it is not easy to assess whether the measurements accurately reflect the actual exposure experienced by individual women. The Health Council concludes that, on the basis of TNO’s data, it is actually impossible to arrive at a reliable retrospective estimate. There are two reasons for this.
The measurements used are not representative of the exposure
This is because, of the three roads for which long-term measurements were obtained, only a single monthly average for just one of these roads was used as
Table 2 Average hourly concentrations of asbestos fibres near three roads in the Goor region, measured using PCM (Source: TNO report 1987).
Name of the road Chrysotile fibre concentrations (fibres/m3)
Crocidolite fibre concentrations (fibres/m3)
Hazendammerweg 20,103-50,103 15,103-30,103
Nieuwe Sluisweg 0-5,103
the basis for estimating exposure. With regard to TNO’s measurements, it has
been shown that the monthly average of 3,000 fibres/m3 is not representative of
the measurements obtained at other times of the year, as the other monthly average values are considerably lower.
Moreover, TNO’s short-term measurements show that concentrations can vary substantially within the space of a few hours. Values in excess of one
million fibres/m3 have been measured, while the monthly average was just 3,000
fibres/m3. This large degree of variation is not limited to the amounts of asbestos
released from the roads, it is also apparent in the types and lengths of fibres involved. This is important, as the types of fibre involved (blue or white asbestos) and their length significantly influence the risk that exposure will result in mesothelioma. Given these uncertainties, it is no longer possible to make a representative retroactive estimate of the prevailing concentrations at or near roads on the basis of the limited measurements made near three roads in the past.
It is not possible to translate these data into exposure levels throughout the entire region
The second and most important reason why it is no longer possible to make exposure estimates is that emission measurements tell us nothing about the asbestos exposure experienced by women who have lived in the Goor region. For instance, such exposure is not only dependent on the quantity of asbestos fibres released by roads and yards (emission), it is also influenced by the frequency of exposure (how often, and for how long, people have been in contact with the fibres) and by the type of contact involved (walking, cycling, or when driving a vehicle). Exposure can also occur at home, due to fibres blown in by the wind or brought in on clothing and footwear. A reliable estimate of exposure to asbestos fibres is only possible where personal measurements of the indoor and outdoor environments have been made in the past, over a protracted period of time.
2.4 Conclusion
Last year, standards for asbestos levels in the soil were introduced. It is clear that these standards were greatly exceeded in the area around Goor. This is because the upper layer of asbestos paved roads and yards consists of asbestos cement waste, about 10% of which consists of asbestos. The researchers from Erasmus MC, the Integrated Cancer Centre of the City Triangle Region, Twente, and hospitals in the province of Twente were the first in the Netherlands to show that
the additional cases of pleural mesothelioma in this region were probably caused by environmental exposure to asbestos.
In the Health Council’s judgement, it is not possible (on the basis of TNO’s measurements) to make an adequate retrospective estimate of the level of asbestos exposure experienced by the 75,000 women who lived in the risk area. This inability to retrieve data on past exposure levels means that, on the basis of the study conducted in the Goor region, no assessment can be made of the accuracy of the MPR. Nor, indeed, was this ever the authors’ intention.
This means that using Hodgson’s risk analysis technique to determine the number of expected cases at the estimated cumulative exposure is a rather pointless exercise. For the same reason, there is little point in attempting to account for the extra incidence of fifteen cases of mesothelioma by comparing them to the number that would be expected on the basis of the MPR. All things considered, the study provides no points of reference that might serve as the basis for a different system of standardisation.
3
ChapterIs reform of the standards required,
based on the current level of
knowledge?
3.1 Method used to derive standards
The Dutch standards for asbestos have been derived from a large number of cohort studies. These include cohort studies carried out from the 1950s onwards, in various branches of industry and many different countries. To derive the standards, the high concentrations to which people in various branches of industry were exposed were translated to a low exposure, which is appropriate for the purposes of standards. This was based on the assumption that there is a linear relationship between high and low levels of exposure. This is because asbestos is a carcinogen to which no threshold value applies. The standards are based on its ability to cause mesothelioma, as this is the most socially sensitive effect of asbestos.
Two levels of risk are identified. The MPR and NR are values that correspond, respectively, to the risk of one in a million and one in a hundred million people per year developing a malignant tumour from exposure to the substance in question.
In addition, separate MPR and NR values have been derived for chrysotile and amphibole fibres (crocidolite and amosite). This is because it is generally accepted that amphiboles have a greater potency to cause mesothelioma than chrysotile. The MPR and NR for amphibole were originally derived from a risk
analysis carried out by the WHO.8 According to Doll and Peto (1985), chrysotile
asbestos criteria document, this notion underpins the proposed separate MPR and
NR values for chrysotile.4 Table 3 shows the estimated risks of one in ten
thousand (MPR) and one in a million (NR) associated with a lifetime’s exposure to chrysotile and amphiboles. The MPR and NR values were ultimately fixed as the upper limit of the range of values given in Table 3.
3.2 View of new findings
Of the literature published since 1987, the meta-analysis by Hodgson and Darnton (2000) and a report by the Environmental Protection Agency (EPA) give
cause for a revision of the MPR and NR.3,5
Hodgson and Darnton (2000)
Hodgson and Darnton’s analysis (2001) is based on a meta-analysis of seventeen individual cohort studies. A meta-analysis combines the results of a range of different studies, to enhance their validity. Some of the studies analysed in the course of this work were not yet available in 1987, when the asbestos criteria document was published.
The risks of mesothelioma are indicated in a lifetime table. This technique provides an important correction, as people can – of course – also die from other disorders. Hodgson and Darnton’s analysis also involved separate calculations of the risks associated with chrysotile, and with the amphiboles amosite and crocidolite. They conclude that amphiboles’ potency to cause mesothelioma is about one hundred to five hundred times greater than that of chrysotile. The EPA endorsed this order of magnitude in its 2003 report.
This means that, in addition to the publication of new cohort studies, a better method for deriving standards is now available. In the old method of calculating the MPR and the NR there was no correction for other causes of death. It was also assumed that chrysotile was just one tenth less dangerous than crocidolite.
Table 3 Risk assessment for the general population associated with a lifetime exposure to asbestos in outdoor air (in fibres/m3).
Mesothelioma effect Fibres longer than 5 µm, per m3, measured using electron microscopy 10-4 risk for chrysotile 10,000-100,000
10-4 risk for amphiboles 1,000- 10,000 10-6 risk for chrysotile 100- 1,000 10-6 risk for amphiboles 10- 100
Hodgson and Darnton’s meta-analysis appears to be a good, solid study. It can certainly be used for a review of the MPR and NR.
EPA 2003
The EPA report entitled Technical Support Document for a Protocol to Assess
Asbestos-Related Risk contains a comprehensive analysis of all available cohort
studies.5 This document places great emphasis on the importance of
characterising exposure as accurately as possible in those studies. Old studies have been extensively evaluated. Every effort was made to retrieve information on exposure (concentrations, types of fibre, and fibre length).
The report proposed that, when deriving future standards, a distinction should be drawn between fibres that are longer than 10 µm and those of smaller dimensions. Today’s standards (both at home and abroad) are based on a fibre length of 5 µm. According to the authors of the EPA report, the risk of
mesothelioma posed by fibres longer than 10 µm is three hundred times greater than that associated with exposure to fibres ranging from 5 µm to 10 µm in length.
That, too, has implications for standard setting. In principle, each standard is linked to a given measurement method. In theory, therefore, any change to a measurement method will result in an amendment of the standard. If allowance is made for the 10 µm limit and the type of fibre involved, then the variation in estimates of the risk in the twenty cohort studies examined falls from a factor of 1,000 to well over 30. It appears that this report could be of use in the review of the MPR and NR.
Discussion of the findings
According to Hodgson and Darnton’s meta-analysis and to the EPA report, the standards for exposure to airborne asbestos need to be reviewed. Aside from the availability of more recent cohort studies, Hodgson’s study reveals that a new factor is needed to account for the difference in potency between chrysotile and amphiboles. An investigation should also be carried out to determine whether a standard based on a different limit for fibre length (as indicated in the EPA report) is desirable and feasible.
This initial, limited exploration of the literature shows that the outcome of the standard-setting process is not immediately obvious. This will require additional work. However, both findings could have a major impact on the assessment of environmental samples. Asbestos in the environment (outdoor air)
usually takes the form of chrysotile fibres, which are quite short, whereas the cohort studies from which the current standards have been derived generally involve longer fibres.
An investigation could also be carried out to determine the most appropriate conversion factor for transforming the MPR and NR (measured using PCM) into TEM concentrations. The current factor of 2 is probably quite conservative. The ATSDR and the NRC use a factor of 50 or more for the purpose of this
conversion.
Interestingly, the asbestos criteria document on which the present standard is based indicates that the WHO's risk assessment methods were adopted. This makes no mention of the fact that, following the publication of a letter in the journal Science, a later version proposed that a correction of the WHO value
should be implemented.13 In terms of Dutch values, this correction would have
resulted in an MPR value for amphiboles of 1,000 fibres/m3, rather than 10,000
fibres/m3. Accordingly, that would be yet another reason to adopt a new standard
for airborne asbestos. It should be noted that the NR value for asbestos (which serves as the limit value in the Netherlands for policy purposes) is a factor of 100 lower than the MPR.
3.3 Conclusion
Recent knowledge and insights about asbestos necessitate a review of the current standards governing the concentrations of this substance in the air. The impact of a review of the MPR and NR values for asbestos is not immediately obvious.
How can the review of standards be tackled? This was previously carried out by RIVM as part of its criteria document proposals for limit values, which were subsequently assessed by the Health Council. These values were then fixed by the Ministry of Housing, Spatial Planning and the Environment. Given the limited nature of a review of the MPR and NR for asbestos, and particularly given the social urgency involved, this work could be carried out by the Health Council’s Committee on the Evaluation of the Carcinogenicity of Chemical Substances (with support from the RIVM where necessary). This Committee is prepared to start work at the earliest opportunity, and to deliver a proposal for a new value by the middle of next year.
References
1 Burdorf A, Siesling S, Sinninghe Damste H. Regionale spreiding van het maligne mesothelioom in nederland. Deelrapport 1. Rotterdam/ Enschede: Erasmus MC Rotterdam: 2005.
2 Burdorf A, Siesling S, Sinninghe Damste H. Invloed van milieublootstelling aan asbest in de regio rond GOor op het optreden van het maligne mesothelioom onder vrouwen. Deelrapport 2. Rotterdam/ Enschede: Erasmus MC Rotterdam: 2005.
3 Hodgson JT, Darnton A. The quantitative risks of mesothelioma and lung cancer in relation to asbestos exposure. Ann Occup Hyg 2000; 44(8): 565-601.
4 Slooff W, Blokzijl PJ. Basisdocument asbest. Bilthoven: RIVM; 1987: 758473006.
5 EPA. Report on the Peer Consultation Workshop to Discuss a Proposed Protocol to Assess Asbestos-Related Risk. Washington, DC: 2003: 68-C-98-148.
6 ATSDR. Toxicological profile for asbestos. ATSDR; 2001.
7 Gezondheidsraad. Asbest. Toetsing van een ontwerp-basisdocument. ‘s-Gravenhage: 2006: 1988/31. 8 WHO. Air Quality Guidelines. Copenhagen: WHO; 1987.
9 Biesheuvel PJ, Buurmeijer JF, Swuste PHJJ. Asbest: Van Goor naar Hof van Twente. Goor: Gemeenteraad Hof van Twente; 2003.
10 Hennekam M, Kaper W, Kole M, Reinders A. Asbestcementafval als wegverharding. Leiden: Centrum voor milieukunde Leiden; 1984.
11 Boeft J den. Asbestconcentraties nabij een met asbestafval verharde weg in Diepenheim. Delft: 1987: MT-TNO rapportR87/155.
12 Doll R, Peto J. Effects on health of exposure to asbestos. Report to the Health and Safety Committee. London UK: Her Majesty's Stationery Office: 1985.
A Request for advice
A
AnnexRequest for advice
Dear President,
The report of an epidemiological study into non work-related mesothelioma victims (("Regionale spreiding van het maligne mesothelioom in Nederland" [Regional distribution of malignant mesothelioma in the Netherlands] (partial report 1, June 2005) and “Invloed van de
milieublootstelling aan asbest in de regio rond Goor op het optreden van Maligne mesothelioom onder vrouwen” [Influence of environmental exposure to asbestos in the region around Goor on the occurrence of malignant mesothelioma among women] (partial report 2, August 2005)) by the Erasmus MC (et al) showed that there were significantly more victims than expected due to asbestos-paved roads. I submitted the results of this study to the Lower House of the Dutch parliament on 4 November 2005 ("Aanbieding rapportage evaluatie Saneringsregeling asbestwegen eerste fase en aanbieding rapportage epidemiologisch onderzoek naar niet beroepsgebonden
mesothelioomslachtoffers" [Submission of report on Remediation Regulations for asbestos-paved roads - first phase and submission of report on epidemiological studies into non work-related mesothelioma victims] DGM/SAS/2005190340). This led me to seek the advice of the Health Council concerning government standards for acceptable risk levels regarding the use of asbestos in our society.
In more specific terms, the question that I wish to submit to the Health Council is as follows: 1 In the Health Council's view, does the report on the epidemiological studies into non
concerning acceptable risks in the tolerance of asbestos in society, i.e. NR (Negligible Risk) and MPR (Maximum Permissible Risk)?
2 Should the Health Council feel obliged to answer the above question in the affirmative, how soon can it produce an advisory report on the formulation of a new set of standards for dealing with asbestos in Dutch society?
At the official level, contacts have already taken place to prepare for your work in this matter. To address the issue of possible unrest in society as a result of this report's findings, I would ask you to send me your response to these questions no later than 20 February 2006, so that I can inform the Lower House of the Dutch parliament in good time.
Yours sincerely,
the State Secretary for Housing, Spatial Planning and the Environment, (signed)
B
AnnexThe experts consulted
Drawn up by:
• J.W. Dogger, Scientific secretary
Health Council of the Netherlands, The Hague With the assistance of:
• Prof. D.J.J. Heederik
Epidemiologist; Institute for Risk Assessment Sciences (IRAS), Utrecht
• Dr. J.H. van Wijnen
Specialist in Environmental Medicine, Amsterdam
Members of the Committee on the Evaluation of the Carcinogenicity of Chemical Substances
• Prof. A.A. van Zeeland, chairperson
Professor of Molecular Radiation Dosimetry and Radiation Mutagenesis, Leiden University Medical Center
• Dr. G.M.H. Swaen
Epidemiologist, Maastricht University Medical Center
• Dr. P.J. Boogaard
Toxicologist, Shell International BV, The Hague
• H.C. Dreef-van der Meulen
• Prof. H. van Loveren
Professor of Immunotoxicology, Maastricht University; the National Institute for Public Health and the Environment (RIVM), Bilthoven
• Prof. G.J. Mulder
Professor of Toxicology, Leiden; Amsterdam Center for Drug Research, Leiden
• Dr. M.J.M. Nivard
Molecular biologist and genetic toxicologist, Leiden University Medical Center
• Dr. H. te Riele
Molecular biologist, The Netherlands Cancer Institute, Amsterdam
• Dr. H. Roelfzema, advisor
Ministry of Health, Welfare and Sport, The Hague
• Prof. W. Slob
Professor of Quantitative Risk Assessment, University of Utrecht
• Prof. A.L.M. Verbeek
Professor of Clinical Epidemiology, Radboud University Nijmegen
• Dr. R.A. Woutersen
Toxicologic pathologist, Netherlands Organisation for Applied Scientific Research (TNO), Zeist
• Prof. E.J.J. van Zoelen
Professor of Cell Biology, Radboud University Nijmegen
• Dr. A. van der Burght, Scientific secretary
Health Council of the Netherlands, The Hague
• Dr. J.M. Rijnkels, Scientific secretary
Health Council of the Netherlands, The Hague Guest speaker
• Dr. A. Burdorf
Epidemiologist, Erasmus Medical Center, Rotterdam
The Health Council and interests
Members of Health Council Committees are appointed in a personal capacity because of their special expertise in the matters to be addressed. Nonetheless, it is precisely because of this expertise that they may also have interests. This in itself does not necessarily present an obstacle for membership of a Health Council Committee. Transparency regarding possible conflicts of interest is nonetheless important, both for the chairperson and members of a Committee
and for the President of the Health Council. On being invited to join a Committee, members are asked to submit a form detailing the functions they hold and any other material and immaterial interests which could be relevant for the Committee’s work. It is the responsibility of the President of the Health Council to assess whether the interests indicated constitute grounds for non-appointment. An advisorship will then sometimes make it possible to exploit the expertise of the specialist involved. During the inaugural meeting the
declarations issued are discussed, so that all members of the Committee are aware of each other’s possible interests.