What to do if you’re worried
a child is being abused
C
ontents
Preface – Safeguarding Children
5
1
Introduction – Working with children about whom
there are child welfare concerns
7
2
What
is
a
child
in
need
?
7
3.1
What
does
safeguarding
and
p
ro
m
oting
the
welfare
of
children
m
ean
?
8
4.1
What
is
significant
har
m?
8
4.2
What
is
abuse
and
neglect
?
8
5
The processes for safeguarding children
9
7
Child welfare concerns…
10
8
I
n
general
10
10.1 A
ll
p
ractitioners
wor
k
ing
with
children
and
fa
m
ilies
should
…
11
If you have concerns about a child’s welfare…
13
11.
A
ll
p
ractitioners
should
...
13
12.
S
ocial
wor
k
ers
and
their
m
anagers
,
in
res
p
onding
to
a
referral
,
should
...
14
13.1 P
olice
officers
should
...
15
F
lowchart
1: R
eferral
16
F
lowchart
2:
What
ha
pp
ens
following
initial
assess
m
ent
?
17
F
lowchart
3: U
rgent
action
to
safeguard
children
18
F
lowchart
4:
What
ha
pp
ens
after
the
strategy
discussion
?
19
F
lowchart
5:
What
ha
pp
ens
after
the
child
p
rotection
14
If an initial assessment is required…
21
16.1
S
ocial
wor
k
ers
should
…
21
17.1
P
olice
officers
should
…
22
18.1
A
ll
p
ractitioners
should
…
22
What happens next where there is…
…no suspected actual or likely significant harm?
23
19.1
S
ocial
wor
k
ers
should
...
...
...
23
…suspected actual harm or likely significant harm?
23
20.1
S
ocial
wor
k
ers
should
…
23
21.1
P
olice
officers
should
24
22
If you need to take urgent action to protect a child…
24
23.1
S
ocial
wor
k
ers
, p
olice
officers
or
NSPCC
wor
k
ers
should
24
24
If you need to have a strategy discussion…
25
26
What
are
the
tas
k
s
of
the
strategy
discussion
?
26
27
Who
should
be
in
v
ol
v
ed
in
the
strategy
discussion
?
26
28.1
A
tea
m m
anager
or
senior
social
wor
k
er
should
…
27
29.1
P
olice
officers
should
…
27
30.1
H
ealth
p
rofessionals
should
…
27
31.1
A
ll
p
ractitioners
should
…
27
32
What happens when s47 enquiries are initiated?
27
33.1
S
ocial
wor
k
ers
should
…
28
34.1
P
olice
officers
should
…
28
35.1
H
ealth
p
ractitioners
should
…
29
36.1
A
ll
other
p
ractitioners
should
…
29
What happens if after the s47 enquiries…
…concerns are not substantiated?
30
37.1
S
ocial
wor
k
ers
should
…
30
39
…concerns are substantiated, but the child is not
judged to be at continuing risk of significant harm?
30
40.1 S
ocial
wor
k
ers
should
…
31
41.1 C
hildren’s
social
care
m
anagers
should
...
...
...
31
42.1 P
olice
officers
should
…
31
43.1 O
ther
p
ractitioners
should
…
31
…concerns are substantiated and the child is judged
to be at continuing risk of significant harm?
32
44.1 C
hildren’s
social
care
m
anagers
should
32
45.1 S
ocial
wor
k
ers
should
…
33
46.1 GP
s
and
/
or
m
edical
consultants
should
…
33
47.1 A
ll
p
ractitioners
should
…
33
48
What happens at a child protection conference?
34
50
Pre-birth child protection conference
35
51
What happens after the child protection conference if
the child becomes the subject of a child protection plan? 36
51.1 T
he
na
m
ed
k
eywor
k
er
should
…
36
52.1 T
he
core
grou
p
should
…
36
53.1 A
ll
other
p
rofessionals
should
…
37
54
Planning
37
56.1 T
he
na
m
ed
k
eywor
k
er
should
…
37
57.1 O
ther
p
rofessionals
should
…
38
58
Intervention
38
64.1 T
he
na
m
ed
k
eywor
k
er
should
…
39
65.1 O
ther
p
ractitioners
should
…
40
66
Child protection review conference
40
69.1 T
he
na
m
ed
k
eywor
k
er
should
…
41
70.1 A
ll
p
ractitioners
should
…
41
80
When may a child cease to be the subject of a child
protection plan?
42
81
What happens if a child dies or suffers serious injury
or sexual abuse?
42
82.1 A
ll
agencies
should
…
43
83.1 A
ll
p
rofessionals
should
…
43
84.1 D
esignated
health
p
rofessionals
should
…
43
Appendices
App
endi
x 1 U
se
of
q
uestionnaires
and
scales
to
e
v
idence
assess
m
ent
and
decision
m
a
k
ing
44
App
endi
x 2 L
egislati
v
e
F
ra
m
ewor
k
48
App
endi
x 3 I
nfor
m
ation
sharing
54
P
reface
–
S
afeguarding
C
hildren
This practiceguidancehasbeendevelopedtoassist practitionerstowork togetherto safeguardand promotechildren’swelfare. Itisforanyonewhosework bringsthem into contactwithchildrenandfamilies, but particularlythosewhowork inearlyyears, social care, health, education, schoolsandcriminal justiceservices. Itisrelevanttothoseworking inthestatutoryortheindependentsector, aswellasto membersofthewidercommunity, andappliestoallchildrenandyoung peopleirrespective of whether they are living at home with their families and carers or away from home. This includes young people over the age of 16 years who are members of the Armed Forces, in hospital, prison or Young Offenders’ Institutions. Wherechildrenarelivinginfostercareorinaninstitutional setting, includingcustody, assessmentsanddecisionsaboutfurtheractionshouldalso includeconsiderationoftheroleoftheresponsiblecarers, residentialorcustodialstaffas wellas parentsandotherfamily members. Thedocumentrecognisesthatconcernsabouta child’swelfarecan varygreatlyintermsofthenatureandseriousnessofthoseconcerns, howthoseconcernshavebeenidentifiedandoverwhatdurationtheyhavearisen. By ensuringthatsuchconcernsareappropriatelysharedwithstatutoryagenciesandother individualsresponsibleforsafeguardingchildrenwithinagencies, thewelfareofchildren andthesafeguards providedforthem willbeenhanced.
Thedocumentfocuseson:
• whatyoushoulddoifyouhaveconcernsaboutchildreninordertosafeguardand
promotethewelfareofchildren, includingthosewhoaresuffering, oratrisk ofsuffering, significantharm;
• whatwillhappenonceyouhaveinformedsomeoneaboutthoseconcerns;
• whatfurthercontributionyou maybeaskedorexpectedto maketothe processesof
assessment, planning, workingwithchildren, andreviewingthatwork, includinghow youshouldshareinformation;
• somebasicinformationandbackgroundaboutthelegislativeframework withinwhich
children’swelfareissafeguardedand promoted (Appendix 2).
• Appendix 3 reproducesthe Government’s practiceguidanceInformation sharing:
Practitioners’ guide (2006c). Itisdesignedtoassistyouwhen makingdecisionsabout
consent, confidentialityandinformationsharing. Referencestotherelevant Government Guidanceonsafeguardingand promotingthewelfareofchildrenaretobefoundon pages 71–72.
• Togive practitionersconfidencetoapplytheguidancein practice, itisimportantthat
theyhave:
– asystematicapproachwithintheiragencytoexplainingtochildren, young people andfamilieswhentheyfirstaccesstheservice, howandwhyinformation maybe shared, whichwillbuildtheconfidenceofallinvolved;
– clearsystems, standardsand protocolsforsharinginformation. These mayderive from theiragency’s policies, anylocal protocolsin place, orfrom their professional codeofconduct;
– accesstotrainingwheretheycandiscussissueswhichconcernthem andexplore caseexampleswithother practitioners;
– asourceofadviceandsupportoninformationsharingissues.
This publicationisissuedby HM Government. It summarises briefly the key processes but does not replace Working Together to Safeguard Children (2006a) or the Framework for
I
ntroduction
–
Wor
k
ing
with
children
about
who
m
there
are
child
welfare
concerns
1 Achievinggoodoutcomesforchildrenrequiresallthosewithresponsibilityfor assessmentandthe provisionofservicestowork togetheraccordingtoanagreed planof action. Effectivecollaborativeworkingrequires professionalsandagenciestobeclear about:
• theirrolesandresponsibilitiesforsafeguardingand promotingthewelfareofchildren; • the purposeoftheiractivity, whatdecisionsarerequiredateachstageofthe process
andwhataretheintendedoutcomesforthechildandtheirfamily members;
• thelegislativebasisforthework;
• the protocolsand procedurestobefollowed, includingthewayinwhichinformation
willbesharedacross professionalboundariesandwithinagencies, andberecorded;
• whichagency, team or professionalhasleadresponsibility, andthe preciserolesof
everyoneelsewhoisinvolved, includingthewayinwhichthechildrenandotherfamily memberswillbeinvolved;
• anytimescalessetdownin Regulationsor Guidancewhichgovernthecompletionof
assessments, makingof plansandtimingofreviews.
What is a child in need?
2 Childrenwhoaredefinedasbeing ‘inneed’, underthe Children Act 1989, arethose whose vulnerabilityissuchthattheyareunlikelytoreachor maintainasatisfactorylevelof healthordevelopment, ortheirhealthanddevelopmentwillbesignificantlyimpaired, withoutthe provisionofservices (s17(10) ofthe Children Act 1989) plusthosewhoare disabled. Thecriticalfactorstobetakenintoaccountindecidingwhetherachildisinneed underthe Children Act 1989 arewhatwillhappentoachild’shealthordevelopment
without services, andthelikelyeffecttheserviceswillhaveonthechild’sstandardof healthanddevelopment.
What does safeguarding and promoting the welfare of children mean?
3 Safeguardingand promotingthewelfareofchildrenisdefinedforthe purposeof statutoryguidanceunderthe Children Acts 1989 and 2004 respectivelyas:
• protectingchildrenfrom maltreatment;
• preventingimpairmentofchildren’shealthordevelopment;
• ensuringthatchildrenaregrowingup incircumstancesconsistentwiththe provision
ofsafeandeffectivecare; and
• undertakingthatrolesoastoenablethosechildrentohaveoptimum lifechances
andtoenteradulthoodsuccessfully.
What is significant harm?
4.1 Somechildrenareinneedbecausetheyaresufferingorlikelytosuffersignificantharm. The Children Act 1989 introducedtheconceptofsignificantharm asthethresholdthat justifies compulsoryinterventioninfamilylifeinthebestinterestsofchildren. Thelocalauthorityis underadutyto makeenquiries, orcauseenquiriestobe made, whereithasreasonablecause tosuspectthatachildissuffering, orlikelytosuffer, significantharm (s47 ofthe Children Act 1989). To makeenquiriesinvolvesassessingwhatishappeningtoachild. Wheres47 enquiries arebeing made, theassessment (the ‘coreassessment’) shouldconcentrateontheharm that hasoccurredorislikelytooccurtothechildasaresultofchild maltreatmentinordertoinform future plansandthenatureofservicesrequired. Decisionsaboutsignificantharm arecomplex andshouldbeinformedbyacarefulassessmentofthechild’scircumstances, anddiscussion betweenthestatutoryagenciesandwiththechildandfamily.
What is abuse and neglect?
4.2 Abuseandneglectareformsof maltreatment – a person mayabuseorneglectachild byinflictingharm, orbyfailingtoactto preventharm. Childrenandyoung people maybe abusedinafamilyorinaninstitutionalorcommunitysetting; bythose knowntothem or, morerarely, byastranger.
• Physical abuse mayinvolvehitting, shaking, throwing, poisoning, burningor scalding, drowning, suffocating, orotherwisecausing physicalharm toachild. Physical harm mayalsobecausedwhena parentorcarerfabricatesthesymptomsof, or
deliberatelyinduces, illnessinachild.
• Emotional abuse isthe persistentemotional maltreatmentofachildsuchastocause
severeand persistentadverseeffectsonthechild’semotionaldevelopment. It may involveconveyingtochildrenthattheyareworthlessorunloved, inadequate, or valued
onlyinsofarasthey meettheneedsofanother person. It mayfeatureage
ordevelopmentallyinappropriateexpectationsbeingimposedonchildren. These may includeinteractionsthatarebeyondthechild’sdevelopmentalcapability, aswellas overprotectionandlimitationofexplorationandlearning, or preventingthechild participatinginnormalsocialinteraction. It mayinvolveseeingorhearingthe
ill-treatmentofanother. Itmayinvolveseriousbullying, causingchildrenfrequentlytofeel frightenedorindanger, ortheexploitationorcorruptionofchildren. Somelevelof emotionalabuseisinvolvedinalltypesof maltreatmentofachild, thoughit mayoccur alone.
• Sexual abuse involvesforcingorenticingachildoryoung persontotake partinsexual
activities, including prostitution, whetherornotthechildisawareofwhatishappening. Theactivities mayinvolve physicalcontact, including penetrative (e.g. rape, buggeryor oralsex) ornon-penetrativeacts. They mayincludenon-contactactivities, suchas involvingchildreninlookingat, orinthe productionof, sexualon-lineimages, watching sexualactivities, orencouragingchildrentobehaveinsexuallyinappropriateways.
• Neglect isthe persistentfailureto meetachild’sbasic physicaland/or psychological
needs, likelytoresultintheseriousimpairmentofthechild’shealthordevelopment. Neglect mayoccurduring pregnancyasaresultof maternalsubstanceabuse. Oncea childisbornit mayinvolvea parentfailingto:
– provideadequatefood, clothingandshelter (includingexclusionfrom homeor abandonment)
– protectachildfrom physicalandemotionalharm ordanger
– ensureadequatesupervision (includingtheuseofinadequatecare-givers) – ensureaccesstoappropriate medicalcareortreatment.
It mayalsoincludeneglectof, orunresponsivenessto, achild’sbasicemotionalneeds.
The processes for safeguarding children
5 Four key processesunderpinwork withchildreninneedandtheirfamilies, eachof whichneedstobecarriedouteffectivelyinordertoachieveimprovementsinthelivesof childreninneed. Theyareassessment, planning, interventionandreviewing (Department of Health, 2002a). Atanystage, areferral maybenecessaryfrom oneagencytoanother, or receivedfrom a memberofthe public.
6 Theflowchartsinthisdocument (pp16-20) illustratethe processesforsafeguarding and promotingthewelfareofchildren:
• from the pointthatconcernsareraisedaboutachildandarereferredtoastatutory
agencythatcantakeactiontosafeguardand promotethewelfareofthechild (flowchart 1);
• throughaninitialassessmentofthechild’ssituationandwhathappensafterthat
(flowchart 2);
• takingurgentaction, ifnecessary (flowchart 3);
• tothestrategydiscussion, wherethereareconcernsaboutthechild’ssafety, and
beyondthattothechild protectionconference (flowchart 4); and
• whathappensafterthechild protectionconference, andthereview process
(flowchart 5).
Child welfare concerns…
7 Childwelfareconcerns mayarisein manydifferentcontexts, includingwhereachild orfamilyisalready knowntochildren’ssocialcare. There maybeanumberofexplanations forthe perceivedimpairmenttoachild’shealthordevelopmentandeachrequirescareful considerationandreview.
In general
8 Allthosewhocomeintocontactwithchildrenandfamiliesintheireverydaywork, including practitionerswhodonothaveaspecificroleinrelationtosafeguardingchildren, haveadutytosafeguardand promotethewelfareofchildren. Youarelikelytobeinvolved inthree mainways:
• you mayhaveconcernsaboutachild, andreferthoseconcernstochildren’ssocialcare
orthe police. Schoolstaff (bothteachingandnon-teaching) shouldbeawareofthelocal procedurestobefollowedforreportingconcernsabouta particularchild. Thiswill normallybe viatheschool’sdesignatedsenior memberofstaffortheirnominated deputyorifneitherareavailable, anothersenior memberoftheschool’sstaff. In emergencies, however, contactthe policedirect;
• you maybeapproachedbychildren’ssocialcareandaskedto provideinformation
aboutachildorfamilyortobeinvolvedinanassessment. This mayhappenregardless ofwho madethereferraltochildren’ssocialcare;
• you maybeaskedto providehelp oraspecificservicetothechildora memberoftheir
9 Somewho mayalsocomeintotheabovecategory, suchas paediatricians, speech therapistsand psychologists, maybeaskedtoundertakespecifictypesofassessments aspartofaninitialorcoreassessment, to providereportstoinform achild protection conference, toattendthatconference, ortocontributetoongoingtherapeuticwork with achildandareviewofthatwork.
All practitioners working with children and families should…
10.1 Befamiliarwithandfollowyourorganisation’s proceduresand protocolsfor
promotingandsafeguardingthewelfareofchildreninyourarea, and knowwhotocontact inyourorganisationtoexpressconcernsaboutachild’swelfare.
10.2 Rememberthatanallegationofchildabuseorneglect mayleadtoacriminal investigation, sodon’tdoanythingthat may jeopardisea policeinvestigation, suchas askingachildleading questionsorattemptingtoinvestigatetheallegationsofabuse.
10.3 Ifyouareresponsiblefor makingreferrals, knowwhotocontactin police, health, education, schoolandchildren’ssocialcaretoexpressconcernsaboutachild’swelfare.
10.4 Referanyconcernsaboutchildabuseorneglecttochildren’ssocialcareorthe police.
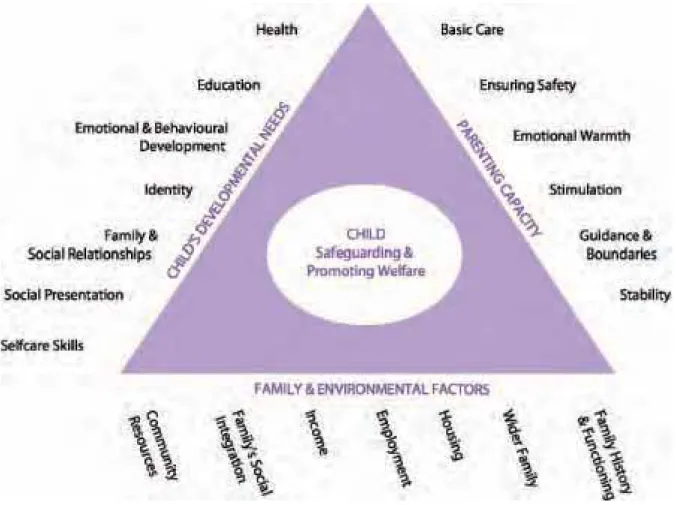
10.5 HaveanunderstandingoftheFramework for the Assessment of Children in Need and
their Families (see Figure 1), whichunderpinsthe processesofassessingneeds, planning
servicesandreviewingtheeffectivenessofservice provisionatallstagesofwork with childreninneedandfamilies. (Thedimensionsofthe Common Assessment Framework (2006b) arebasedonthoseinthe Assessment Framework.)
10.6 Whenreferringachildtochildren’ssocialcareyoushouldconsiderandincludeany informationyouhaveonthechild’sdevelopmentalneedsandtheir parents’/carers’ability torespondtotheseneedswithinthecontextoftheirwiderfamilyandenvironment. This information mayhavebeenobtainedduringthecompletionofa Common Assessment (2006b). Similarly, whencontributingtoanassessmentor providingservicesyoushould considerwhatcontributionyouareableto makeinrespectofeachofthesethreedomains. Specialistassessments, in particular, arelikelyto provideinformationrelevanttoaspecific dimension, suchashealth, educationorfamilyfunctioning.
10.7 Seethechildandascertainhisorherwishesandfeelingsas partofconsideringwhat actiontotakeinrelationtoconcernsaboutthechild’swelfare.
10.8 Communicatewiththechildinawaythatisappropriatetotheirage, understanding and preference. Thisisespeciallyimportantfordisabledchildrenandforchildrenwhose preferredlanguageisnot English. Thenatureofthiscommunicationwillalsodependon thesubstanceandseriousnessoftheconcernsandyou mayrequireadvicefrom children’s
socialcareorthe policetoensurethatneitherthesafetyofthechildnoranysubsequent investigationis jeopardised. Whereconcernsariseasaresultofinformationgivenbya childitisimportanttoreassurethechildbutnotto promiseconfidentiality.
10.9 Recordfullinformationaboutthechildatfirst pointofcontact, includingname(s), address(es), gender, dateofbirth, name(s) of person(s) with parentalresponsibility (for consent purposes) and primarycarer(s), ifdifferent, and keep thisinformationup todate. Inschools, thisinformationwillbe partofthe pupil’srecord.
10.10 Recordinwritingallconcerns, discussionsaboutthechild, decisions made, andthe reasonsforthosedecisions. Thechild’srecordsshouldincludeanup-to-datechronology, anddetailsoftheleadworkerintherelevantagency – forexample, asocialworker, GP, health visitororteacher.
10.11 Talk toyour managerandother professionals: alwaysshareyourconcerns, and discussanydifferencesofopinion. Followup yourconcerns. Alwaysfollowup oral communicationstoother professionalsinwritingandensureyour messageisclear.
I
f
you
ha
v
e
concerns
about
a
child’s
welfare
…
All practitioners should...
11.1 Discussyourconcernswithyour manager, namedordesignatedhealth professional ordesignated memberofstaff, dependingonyourorganisationalsetting. Ifyoustillhave concerns, youoryour managercouldalso, withoutnecessarilyidentifyingthechildin question, discussyourconcernswithseniorcolleaguesinanotheragencyinorderto develop anunderstandingofthechild’sneedsandcircumstances.
11.2 If, afterthisdiscussion, youstillhaveconcerns, andconsiderthechildandtheir parentswouldbenefitfrom furtherservices, considerwhichagency, includinganother part ofyourown, youshould makeareferralto. Ifyouconsiderthechildisor maybeachildin need, youshouldreferthechildandfamilytochildren’ssocialcare. This mayincludea childwhom youbelieveis, or maybeatrisk ofsufferingsignificantharm. Ifyourconcerns areaboutachildwhoisalready knowntochildren’ssocialcare, theallocatedsocialworker shouldbeinformedofyourconcerns. Inadditiontochildren’ssocialcare, the policeand the NSPCC have powerstointerveneinthesecircumstances.
11.3 Ingeneral, seek todiscussyourconcernswiththechild, asappropriatetotheirage andunderstanding, andwiththeir parentsandseek theiragreementto makingareferralto children’ssocialcareunlessyouconsidersuchadiscussionwould placethechildatan increasedrisk ofsignificantharm. Appendix 3 reproducesthetextofInformation sharing:
Practioners’ guide (HM Government, 2006c). In particular, Section 4 ofthis Guide provides
furtherguidanceonconsentandonthecircumstanceswhenit mightor mightnotbe appropriatetodiscussthese matterswithchildren.
11.4 Whenyou makeyourreferral, agreewiththerecipientofthereferralwhatthechild and parentswillbetold, bywhom andwhen.
11.5 Ifyou makeyourreferralbytelephone, confirm itinwritingwithin 48 hours.
receivingit, soifyouhavenotheardback within 3 workingdays, contactchildren’ssocial careagain.
Social workers and their managers, in responding to a referral, should...
12.1 Followingareferral, youandyour managershoulddecideonthenextcourseof actionwithinoneworkingdayandrecordthisdecisiononthe Referraland Information Record (Departmentof Health, 2002c). Furtheraction mayincludeundertakinganinitial assessment, referraltootheragencies, provisionofadviceorinformation, ornofurther action.
12.2 Ifyouandyour managerdecidethatyoushouldtakenofurtheractionatthisstage, tellthereferrerofthisdecisionandthereasonsfor makingit. Whereareferralhasbeen receivedfrom a memberofthe public, dothisinawaythatisconsistentwithrespecting theconfidentialityofeach party.
12.3 Newinformation maybereceivedaboutachildorfamilywherethechildorfamily memberisalready knowntochildren’ssocialcare. Ifthechild’scaseisopen, andthereare concernsthatthechildisor maybesufferingharm, thenadecisionshouldbe madeabout whetherastrategydiscussionshouldbeinitiated. It maynotbenecessarytoundertakean initialassessmentbeforedecidingwhattodonext. It may, however, beappropriateto undertakeacoreassessmentortoupdatea previousone, inordertounderstandthe child’scurrentneedsandcircumstancesandinform futuredecision-making. Ifthis informationcausesyoutobeconcernedaboutachild’ssafetythendiscussitwithyour manager. Ifyouconsiderthechildisor maybesufferingharm, decidewhether, asthechild andfamilywillbewell knowntochildren’ssocialcareitisappropriatetoholdastrategy discussionwithoutundertakinganinitialassessment.
12.4 Youandyour managershouldconsiderwhetheracrime mayhavebeencommitted. Ifso, discussthechildwiththe policeattheearliestopportunity, asitistheirresponsibility tocarryoutanycriminalinvestigationinaccordancewiththeagreed planforthechild.
12.5 Whenyouhavereceivedareferralfrom a memberofthe public, ratherthananother professional, rememberthat personalinformationaboutreferrers, includinganythingthat couldidentifythem, shouldonlybedisclosedtothird parties (includingsubjectfamilies andotheragencies) withtheconsentofthereferrer. Ifthe policeareinvolved, youwill needtodiscusswiththem whentoinform the parentsaboutreferralsfrom third parties, as thiswillhaveabearingontheconductof policeinvestigations.
Police officers should...
13.1 Whereyoubecomeinvolvedwithachildaboutwhom youhavechildwelfare concerns, refertochildren’ssocialcareandagreea planofaction.
13.2 Whereyouarecontactedbychildren’ssocialcareaboutachild, considerwhetherto beginacriminalinvestigationandleadonanyinvestigation.
13.3 Undertaketheevidencegathering processwhilstworkingin partnership andsharing relevantinformationwithchildren’ssocialcareandotheragencies.
13.4 Takeimmediateactionwherenecessarytosafeguardachild, consultingwith children’ssocialcareandagreeinga planofactionassoonas practicable.
Flow chart 1 – Referral
PRACTITIONER HAS CONCERNS ABOUT CHILD’S WELFARE
Practitionerdiscusseswith managerand/orothersenior colleaguesastheythink appropriate
Practitionerrefersto LA children’s socialcare, followingup inwriting
within 48 hours
Initialassessmentrequired
Nofurther LA children’ssocialcare involvementatthisstage, although otheraction maybenecessary,
e.g. onwardreferral
Concernsaboutchild’s immediatesafety
See flow chart 3 on emergency action
See flow chart 2 on initial assessment
Socialworkerand manager acknowledgereceiptofreferral
anddecideonnextcourseof actionwithinoneworkingday
Nofurtherchild protectionaction,
although mayneedtoacttoensure services provided
Feedback toreferreronnext courseofaction
Flow chart 2 – What happens following initial assessment?
INITIAL ASSESSMENT COMPLETED WITHIN 7 WORKING DAYS FROM REFERRAL TO
LA CHILDREN’S SOCIAL CARE
Feedback to referrer
Childinneed
No LA children’ssocialcare supportrequired, butother action maybenecessary,
e.g. onwardreferral
Socialworkerdiscusseswithchild,
familyandcolleaguestodecide onnextsteps
Strategydiscussion, involving LA
children’ssocialcare, policeand relevantagencies, todecide whethertoinitiateas47 enquiry
Noactualorlikely significantharm
Actualorlikely significantharm
Decidewhatservicesarerequired
In-depthassessmentrequired
Concernsariseaboutthe child’ssafety
Socialworkerleadscore assessment; other professionals
contribute
Furtherdecisions madeabout service provision
See flow chart 4
Socialworkerco-ordinates provision ofappropriateservices, and
recordsdecisions
Reviewoutcomesforchildand whenappropriateclosethecase
Flow chart 3 – Urgent action to safeguard children
DECISION MADE THAT EMERGENCY ACTION MAY BE NECESSARY TO SAFEGUARD A CHILD
Immediatestrategydiscussionbetween LA children’s socialcare, policeandotheragenciesasappropriate
Relevantagencyseekslegaladviceandoutcomerecorded
Immediatestrategydiscussion makesdecisionsabout: • immediatesafeguardingaction
• informationgiving, especiallyto parents
Relevantagencyseeschildandrecordsoutcome
Appropriateemergency
Noemergencyactiontaken
actiontaken
Strategydiscussionands47 Childinneed enquiriesinitiated
See flow chart 2 See flow chart 4
With family and other professionals, agree plan for ensuring child’s future safety and welfare and record decisions
Flow chart 4 – What happens after the strategy discussion?
STRATEGY DISCUSSION MAKES DECISIONS ABOUT WHETHER TO INITIATE S47 ENQUIRIES AND DECISIONS ARE RECORDED
Nofurther LA children’ssocial careinvolvementatthisstage,
butotherservices may berequired
Decisiontocommence
coreassessmentunder s17 of Children Act 1989
Decisiontoinitiate Policeinvestigate possiblecrime s47 enquiries
Socialworkerleadscoreassessmentunders47 of Children Act 1989
andother professionalscontribute
Concernsaboutharm not substantiatedbutchildisa
childinneed
With family and other professionals, agree plan for ensuring child’s future safety
and welfare and record decisions
Concernssubstantiated, child
atcontinuingrisk ofharm
Concernssubstantiated butchildnotatcontinuing
risk ofharm
Agreewhetherchild protection conferencenecessaryand
recorddecision
YES NO
Socialworkerleadscompletion ofcoreassessment
With family and other
Socialwork managerconveneschild professionals, agree plan for
protectionconferencewithin 15 working ensuring child’s future safety
daysoflaststrategydiscussion and welfare and record decisions
Decisions madeandrecordedatchild protectionconference
Childatcontinuingrisk of Childnotatcontinuing significantharm risk ofsignificantharm
Child is subject of child Furtherdecisions made
protection plan; outline child aboutcompletionofcore
protection plan prepared; assessmentandservice
core group established – provisionaccording
Flow chart 5 – What happens after the child protection conference, including the review process?
CHILD IS THE SUBJECT OF A CHILD PROTECTION PLAN
Coregroup meetswithin 10 Keyworkerleadsoncoreassessment workingdaysofchild protection tobecompletedwithin 35 working
conference daysofcommencement
Coregroup memberscommission furtherspecialistassessments
asnecessary
Child protection plandevelopedby keyworker,
togetherwithcoregroup members, andimplemented
Coregroup members provide/commissionthenecessary interventionsforchildand/orfamily members
Firstchild protectionreviewconferenceisheldwithin
3 monthsofinitialconference
Reviewconferenceheld
Someremainingconcerns
Nofurtherconcernsaboutharm aboutharm
Childnolongerthesubjectofchild
protection planandreasonsrecorded
Furtherdecisions madeabout continuedservice provision
Childremainssubjectofachild
protection planwhichisrevised andimplemented
Reviewconferenceheldwithin
6 monthsofinitialchild
I
f
an
initial
assess
m
ent
is
re
q
uired
…
14 Aninitialassessmentisabriefassessmentofeachchildreferredtochildren’ssocial caretodetermine ‘whetherthechildisinneed, thenatureofanyservicesrequired, and whetherafurther, moredetailedcoreassessmentshouldbeundertaken’ (paragraph 3.9 of the Assessment Framework). Theinitialassessmentshouldbeundertakeninaccordance withthe Assessment Framework andwherea Common Assessmenthasbeenundertakenit shouldbuildonthisinformation. Informationshouldbegatheredandanalysedwithinthe threedomainsofthe Assessment Framework (see Figure 1), namely:
• thechild’sdevelopmentalneeds;
• the parents’orcaregivers’capacitytorespondappropriatelytothoseneeds; and
• thewiderfamilyandenvironmentalfactors.
15 Theinitialassessmentshouldbecarefully planned, withclarityaboutwhoisdoing what, aswellaswhenandwhatinformationistobesharedwiththe parents. The planning processanddecisionsaboutthetimingofthedifferentassessmentactivitiesshouldbe undertakenincollaborationwithallthoseinvolvedwiththechildandfamily.
Social workers should…
16.1 Leadonaninitialassessmentandcompleteitwithin 7 workingdays, inaccordance
withThe Framework for the Assessment of Children in Need and their Families.
16.2 Seethechildwithinatimescalethatisappropriatetothenatureoftheconcerns expressedatreferral, accordingtoanagreed plan (which mayincludeseeingthechild withouthisorhercarers present). Thisincludesobservingandcommunicatingwiththechild ina mannerappropriatetohisorherageandunderstanding. Thechild’swishesandfeelings shouldbeascertainedandtakenaccountofwhen planningthe provisionofservices.
16.3 Conductinterviewswithchildandfamily members, separatelyandtogetheras appropriate. Theseshouldbeundertakeninthe preferredlanguageofthechildandeach family member. Forsomedisabledchildrenandfamily membersexpertiseinnon-verbal
communicationwillbenecessary. It will not necessarily be clear whether a criminal offence has been committed, soeveninitialdiscussionswiththechildshouldbe
conductedinawaythat minimisesdistresstothem and maximisesthelikelihoodthatthey will provideaccurateandcompleteinformation, avoidingleadingorsuggestive questions.
16.4 Involverelevantagencieswhoareworkingwith/or knowntothechildandfamilyin gatheringand providinginformation, asappropriate (forfurtherinformationon
informationsharing, see Appendix 3).
16.5 Oncetheinitialassessmentiscomplete, togetherwithyour managerandallother relevantagencies, decideonfurtheraction. Involvethechildand parentsinthese
discussions, unlessthis may placeachildatrisk ofsignificantharm again, forexample, the child maybe physicallyabusedfortalkingabouthis/herabuse. Ifyouhaveconcernsabout aparent’sabilityto protecttheirchild, considercarefullywhatthe parentsshouldbetold whenandbywhom, takingaccountofthechild’swelfare.
16.6 Recordtheassessmentfindingsandyourinitialanalysisanddecisionsfollowingthe initialassessment, includingthereasonsforanydecisions madeandfurtheractiontobe takeninthe Initial Assessment Record (Departmentof Health, 2002c). Inform, inwriting, all therelevantagenciesandthefamilyofyourdecisionsand, ifthechildisachildinneed, of the planfor providingsupporttothem andtheirchild.
Police officers should…
17.1 Considerhowyou mightbeabletoassistotheragenciescarryouttheir
responsibilitiesand, wheretherearechildprotectionconcerns, whetherornotacrimehas beencommitted.
All practitioners should…
18.1 Beinvolvedintheinitialassessment processaccordingtotheagreed plan, including providingfurtherinformationaboutthechildandfamily, andinthe processofagreeing furtheraction.
18.2 Seek informationfrom relevantservicesifthechildandfamilyhavespenttime abroad. Professionalsfrom suchagenciesashealth, children’ssocialcareorthe police shouldrequestthisinformationfrom theirequivalentagenciesinthecountry(ies) inwhich thechildhaslived. Informationaboutwhotocontactcanbeobtained viathe Foreignand Commonwealth Officeon 020 7008 1500 ortheappropriate Embassyor Consulatebasedin London (youcanobtaincontactinformationaboutallthe Embassiesin London – the London Diplomatic List, ISBN 0 11 591772 1 – from the Stationery Officeon 0870 600 5522 orfrom the FCO websitewww.fco.gov.uk)
What
ha
pp
ens
ne
x
t
where
there
is
…
…
no
sus
p
ected
actual
or
li
k
ely
significant
har
m?
Social workers should...
19.1 Decidewithyour managerwhetheryouthink thechild maybeachildinneedandif sowhetheritwouldbeappropriatetoundertakeacoreassessmentinordertodetermine whathelp maybenefitthechildandfamilyoralternativelywhethertoofferservicestothe childorfamilybasedonthefindingsoftheinitialassessment.
19.2 Discussanyoptionsforfurtheractionwiththechildand parentsinthelightofthe findingsoftheinitialassessmentandconsiderationofwhatwouldbe mosthelpfultothe childandfamily.
19.3 Discussthefindingsoftheinitialassessmentwithotherrelevant professionalsto inform decisionsaboutwhattypesofservices, includingacoreassessment, itwouldbe appropriatetooffer.
…
sus
p
ected
actual
har
m
or
li
k
ely
significant
har
m?
Social workers should…
20.1 Initiateastrategydiscussiontoenableyouandyour managerstogetherwithother agenciestodecidewhethertoinitiateenquiriesunders47 ofthe Children Act 1989 and thereforetocommenceacoreassessmentasthe meansbywhichtheseenquirieswillbe carriedout.
20.2 Considercarefullywhat parentsaretold, whenandbywhom. The police, GP, health visitor, schoolnurse, any paediatricianwho knowsthechild, theseniorwardnurse (ifthe childisanin-patient), teacherandotherrelevant professionalsshouldbeinvolvedin makingthesedecisions.
20.3 Ifthechildis physically presentinyourlocalauthority’sarea, regardlessofwherehe orsheactuallylives, youneedtoinitiateastrategydiscussiontodecidewhetherthereis evidencetosupportcommencings47 enquiries, ortoapplyforanemergency protection orderunlessappropriatealternativearrangementshavebeen madewiththelocalauthority wherethechildnormallylives.
20.4 Ifthechildisnormallyresidentinanotherlocalauthority, youoryour manager shouldnegotiateatransferofstatutoryresponsibilitytothechild’slocalauthorityof residenceandagreehowthechild’scasewillbe managedbeforerelinquishinglead responsibility. Inthesecircumstanceswhotakesleadresponsibilitywilldependona numberoffactors, suchaswherethechildisgoingtocontinuetobelivinginthenear futureandwhethertheallegationsrelatetoa personlivingorworkinginthesameareaas thechildislivingcurrentlyornot.
20.5 Ifyouthink thatacriminaloffence mayhavebeencommittedagainstachild, you shoulddiscussthechildwiththe policeassoonas possible. Youandthe policewillthen considertogetherwithotherrelevantagencieshowto proceedtosafeguardthechild.
Police officers should...
21.1 Respondtoinformationfrom children’ssocialcareanddecidewhatfurtheractionit mightbenecessarytotake, includingtakingfullresponsibilityforcarryingoutanycriminal investigationina promptandefficient manner.
I
f
you
need
to
ta
k
e
urgent
action
to
p
rotect
a
child
…
22 Wherethereisarisk tothelifeofachildoralikelihoodofseriousimmediateharm, an agencywithstatutorychild protection powers, i.e. children’ssocialcare, policeor NSPCC,
should act quickly to secure the immediate safety of the child (see paragraph 15 in Appendix 2 forasummaryofstatutory powerstosafeguardchildren).
Social workers, police officers or NSPCC workers should...
23.1 Initiateastrategydiscussionimmediatelytodiscuss plannedemergencyactionoras soonas possibleafteranagencyhashadtotakeimmediate protectiveaction.
23.2 Seethechild (thisshouldbedonebya practitionerfrom theagencytakingthe emergencyaction) as partofdecidinghowbestto protecthim orher, includingdeciding whethertoseek anemergencyorder.
23.3 Normallyobtainlegaladvicebeforeinitiatinglegalaction, in particularwhenan Emergency Protection Orderisbeingsought. Police protection powers should only be used in exceptional circumstances where there is insufficient time to seek an Emergency Protection Order or for reasons relating to the immediate safety of the child.
23.4 Whenconsideringwhetheremergencyactionisnecessary, alwaysconsiderwhether actionisrequiredtosafeguardotherchildreninthesamehousehold (e.g. siblings), inthe householdofanalleged perpetrator, orelsewhere. Thenatureoftheabusewillbea key determiningfactor, i.e. ifitis knownachild’slifeisindangerthenimmediate action ought to be taken.
23.5 Recordthedecisions madeattheStrategy Discussion (DepartmentofHealth, 2002c). Keep underconstantreviewdecisionsabout possibleimmediateaction.
I
f
you
need
to
ha
v
e
a
strategy
discussion
…
24 Ifthereisreasonablecausetosuspectthe childissuffering, orislikelytosuffersignificant harm, children’ssocialcareshouldconvenea
strategydiscussion. Dependingonthenatureofthechild’sneedsandtheurgencyofthe situation, this mighttaketheform ofanactual meeting, orbeaseriesoftelephone conversations. Incomplex typesof maltreatmentorneglecta meetingis likely to be the mosteffectivewayofdiscussingthechild’swelfareand planningfutureaction. Morethan onestrategydiscussion maybenecessary. Thisislikelytobewherethechild’s
circumstancesare verycomplex andanumberofdiscussionsarerequiredtoconsider whetherand, ifso, whentoinitiates47 enquiries. Sucha meetingshouldbeheldata convenientlocationforthe keyattendees, suchasahospital, school, policestationor children’ssocialcareoffice.
25 The purposeofthestrategydiscussionistoagreewhethertoinitiates47 enquiries andasaconsequencetocommenceor, whereoneisalreadyin progress, tocompletea coreassessmentunderthissectionofthe Children Act 1989. Itisalsotoidentifythe relevanttasksandtimescalesforeachinvolved professionalandagency, andagreewhat furtherhelp orsupport maybenecessary.
What are the tasks of the strategy discussion?
26 Thediscussionshouldbeusedtoundertakethefollowingtasks:
• agreetheconductandtimingofanycriminalinvestigation;
• decidewhetheracoreassessmentunders47 ofthe Children Act (s47 enquiries) should
beinitiatedorcontinuedifithasalreadybegun;
• planhowthes47 enquiryshouldbeundertaken (ifoneistobeinitiated), includingthe
needfor medicaltreatment, andwhowillcarryoutwhatactions, bywhenandforwhat purpose;
• agreewhatactionisrequiredimmediatelytosafeguardand promotethewelfareofthe
child, and/or provideinterim servicesandsupport. Thiswillinclude, whereachildisin hospital, makingdecisionsabouthowtosecurethesafedischargeofthechild;
• determinewhatinformationaboutthestrategydiscussionwillbesharedwiththe
family, unlesssuchinformationsharing may placeachildatrisk ofsignificantharm or jeopardise policeinvestigationsintoanyallegedoffence(s); and
• determineiflegalactionisrequired.
Who should be involved in the strategy discussion?
27 Thefollowing professionals maybeinvolvedinastrategydiscussion:
• Thestaffinvolvedshouldbesufficientlyseniortobeabletocontributetothediscussion
ofinformation, andto makedecisionsonbehalfoftheiragencies. Theagencies
representedshouldincludeata minimum children’ssocialcare, the policeandrelevant others, includingthereferringagency, thechild’snursery/schoolandhealth;
• Ifthechildisahospital patient (in-orout-patient) orreceivingservicesfrom achild
developmentteam, thestrategydiscussionshouldinvolvethe medicalconsultant responsibleforthechild’shealthcareand, ifthechildisanin-patient, aseniorward nurse;
• Wherea medicalexamination maybenecessaryorhasalreadytaken placeasenior
doctorfrom the providingserviceshouldbeincluded;
• It mayalsobeappropriatetoinvolvethelocalauthority’ssolicitor;
• Itisimportantalsotoconsiderwhetheritisnecessarytoseek advicefrom, orhave
present, additional professionalswhohaveexpertiseinthe particulartypeofsuspected maltreatmentorneglect. Thiswouldenablecomplex informationtobe presentedand evaluatedfrom asoundevidencebase.
A team manager or senior social worker should…
28.1 Ensurethatthestrategydiscussiontakes placeandthatitconsidersthechild’s welfareand plansfutureactions.
28.2 Ensurethatthediscussionidentifieswhatinformationwillbesharedwiththechild andfamilyonthebasisthattheinformationisnotsharediftodoso may placeachildat risk ofsignificantharm or jeopardise policeinvestigations.
28.3 Recordtheagreeddecisionsandactionsonthe Strategy Discussion Record (Departmentof Health, 2002c) andsendthisrecordtoallrelevant professionalsand agencieswithinoneworkingday.
28.4 Considerwhatfurtheractionisrequiredwherean Emergency Protection Orderisin placeorthechildisthesubjectof police powersof protection.
Police officers should…
29.1 Discussthebasisforanycriminalinvestigation, andanyrelevant processesthatother agencies mightneedto knowabout, includingthetimingand methodsofevidence
gathering.
Health professionals should…
30.1 Ifthechildisinhospital, decisionsshouldalsobe madeabouthowtosecurethesafe dischargeofthechild.
All practitioners should…
31.1 Provideavailableinformation verifiedatsource, inaclearandcomprehensible format.
What
ha
pp
ens
when
s
47
en
q
uiries
are
initiated
?
32 A coreassessmentisthe meansbywhichas47 enquiryiscarriedout. Itisanin-depth assessmentthataddressesthecentralor mostimportantaspectsoftheneedsofachild andthecapacityofhisorher parentsorcaregiverstorespondappropriatelytotheseneeds withinthewiderfamilyandcommunitycontext. Thecoreassessmentshouldbeginby focusing primarilyontheinformationidentifiedduringtheinitialassessmentasbeingof mostimportancewhenconsideringwhetherthechildissufferingorislikelytosuffer significantharm. Itshould, however, coverallrelevantdimensionsinthe Assessment Framework beforeitscompletion.
Social workers should…
33.1 LeadonthecoreassessmentassetoutintheFramework for the Assessment of
Children in Need and their Families andrecordthefindingsinthe Core Assessment Record
(Departmentof Health, 2002c).
33.2 In particular, seethechild, ascertainhisorherwishesandfeelingsandestablishtheir understanding, ifoldenough, oftheirsituationandthenatureoftheirrelationship with eachsignificantfamily member (includingallcaregivers).
33.3 Determineeachofthecaregivers’relationshipswiththechild, the parents’ relationship witheachotherandthechildreninthefamily, aswellasthewiderfamily, socialandenvironmentalfactorsimpactingonthem. Userelevant Questionnairesand Scales (see Appendix 1 fordetails) toobtaininformationonspecificareasoffamilylife.
33.4 Systematicallygatherinformationaboutthehistoryofthechildandeachfamily member, buildingonthatalreadygatheredduringthecourseofeachagency’s involvementwiththechildandrecorditinthechronology. Usethefindingsfrom any specificassessmentsofthechildand/orfamily memberstoinform thecoreassessment.
33.5 Keep carefulanddetailednotes, asthisis veryimportantforanysubsequent police investigationorcourtaction. Recordanyunusualeventsand makeadistinctionbetween eventsreportedbythecarerandthoseactuallywitnessedbyothersincluding
professionals. Notesshouldbetimed, datedandsignedlegiblyand keptinasecure place sothattheyarenotabletobeaccessedbyunauthorised persons.
33.6 Attheconclusionofthis phaseoftheassessment, togetherwithyour managerand other professionals, analysethefindingstoreachanunderstandingofthechild’s
circumstanceswhichshouldinform future plans, theobjectivesofthe plananddecisions aboutwhattypesofservicesshouldbe provided.
Police officers should…
34.1 Assiststafffrom otheragenciestounderstandthereasonsfortheconcernsaboutthe child’swelfareincludingtheirsafety. Whileyourinvestigations may produceconclusive evidenceof maltreatment, they mayalsoconfirm thatthecarerisnotresponsiblefor causingthechildharm.
34.2 Whetherornot policeinvestigationsrevealgroundsforinstigatingcriminal
proceedings, makeavailabletoother professionalsanyevidencethatyouhavegathered, toinform discussionsaboutthechild’swelfare.
34.3 Whereyouobtainevidencethatacriminaloffencehasbeencommittedbythe parent orcarer, anda prosecutioniscontemplated, itisimportantthatthesuspect’srightsare protectedbyadherencetothe Policeand Criminal Evidence Act 1984. Thiswouldnormally ruleout, forexample, thesuspectbeingconfrontedwiththeevidenceby personnelfrom thestatutoryagencies, otherthanthe policeastheleadinvestigativeagency.
34.4 Whereadecisionhadbeen madetoundertakeaninterviewofthechildas partofthe criminalinvestigations, youandyourcolleaguesfrom otheragenciesshouldfollowthe guidancesetoutinAchieving Best Evidence in Criminal Proceedings: Guidance for Vulnerable or intimidated witnesses, including children.
Health practitioners should…
35.1 Undertakefurther medicaltests, examinationsorobservationsdependingonthe evidenceavailableabouthowthechild’shealthordevelopment maybebeingimpaired.
35.2 Theleadhealth practitioner (probablyaconsultant paediatrician, orpossibly thechild’s GP) mayalsoneedtocommissionanyofarangeofspecialistassessments. Forexample, physiotherapists, occupationaltherapists, speechtherapistsandchild psychologists maybeinvolvedinspecificassessmentsrelatingtothechild’s
developmentalprogress.
35.3 Ensureappropriatefollow-up ofhealthconcerns.
All other practitioners should…
36.1 Contributetothecoreassessmentandtheanalysisofthefindingsasrequiredand requestedbychildren’ssocialcare, including providinginformationyouholdaboutthe childor parents, contributespecialist knowledgeoradvicetochildren’ssocialcareor undertakespecialistassessments.
36.2 Keep carefulanddetailedcontemporarynotes, asthisis veryimportantforany subsequent policeinvestigationorcourtaction – Youshouldrecordanyunusualevents and makeadistinctionbetweeneventsreportedbythecarerandthoseactuallywitnessed byothersincluding professionals. Notesshouldbetimed, datedandsignedlegiblyand keptinasecure placesothattheyarenotabletobeaccessedbyunauthorised persons.
What
ha
pp
ens
if
after
the
s
47
en
q
uiries
…
…
concerns
are
not
substantiated
?
Social workers should…
37.1 Discusswiththe parentsandother professionals, drawingonanunderstandingfrom theassessmentand/or policeinvestigations, whatfurtherhelp orsupportthefamily may require, forexample, with parentingdifficulties. This mayberelatedtothechild’shealthor developmentorto moregeneral matterswithinthefamily.
37.2 Considerwhetherthechild’shealthanddevelopmentrequirecontinued monitoring againstthespecificobjectivesandwhohasresponsibilityforthis monitoring.
37.3 Considerwhetherfurtherwork isrequiredtocompletethecoreassessmentinorder todecidewhatfurtherhelp orsupportthefamily mayrequire, andifso, completeit.
37.4 Recordalldecisionsandthereasonsforthem onthe Outcomeofthes47 Enquiries Record (Departmentof Health, 2002c).
Other practitioners should…
38.1 Participateinthesediscussionsandconsiderationswhenrequested.
38.2 Contributetothecompletionofthecoreassessmentasappropriate.
38.3 Provideservicesasspecifiedinthe planforthechild.
…
concerns
are
substantiated
,
but
the
child
is
not
j
udged
to
be
at
continuing
ris
k
of
significant
har
m?
39 There maybesubstantiatedconcernsthatachildhassufferedsignificantharm, butit isagreedbetweentheagenciesinvolvedwiththechildandfamilythata planforensuring thechild’sfuturesafetyandwelfarecanbedevelopedandimplementedwithouttheneed forachild protectionconferenceorachild protection plan. Suchanapproachwillbeof particularrelevancewhereitiscleartotheagenciesinvolvedthatthereisnocontinuing risk ofsignificantharm. Thisis particularlyrelevantwhere, forexample, thecarerhastaken
responsibilityfortheharm theycausedthechild, thefamily’scircumstanceshavechanged orthe personresponsiblefortheharm isnolongerincontactwiththechild.
Social workers should…
40.1 Discussthefindingsofthes47 enquiryandagreewiththeotheragenciesinvolved withthechildandfamilythata planforensuringthechild’sfuturesafetyandwelfarecan bedevelopedandimplementedwithouttheneedforachild protectionconferenceora child protection plan.
40.2 Recordalldecisionsandreasonsforthem onthe Outcomeofthes47 Enquiries Record (Departmentof Health, 2002c).
40.3 Ifnecessary, completethecoreassessment, toinform thedevelopmentofthechild’s plan. In particular, thechild’shealthanddevelopment mayrequirecareful monitoringover timewith milestonesfor progressclearlysetoutinthe plan.
40.4 Explaintothechild, asappropriate, andthe parents, thenatureand purposeofthis monitoringbyagenciesotherthanchildren’ssocialcare, andclarifywhohasresponsibility forwhich partsofthe monitoring.
Children’s social care managers should...
41.1 Considercarefully, togetherwithsocialworkersandotheragencies, whetherto proceedtoachild protectionconferencewhereitis knownthatachildhassuffered significantharm.
41.2 Conveneachild protectionconferencewhereallagenciesagreethisisappropriate, or whereoneor moreother professionals, supportedbyasenior manageroranamedor designated professional, requestsone.
Police officers should…
42.1 Considerwhetherornottocontinuewithacriminalinvestigation.
Other practitioners should…
43.1 Befullyinvolvedindecisionsandanyfuture planforthechildandfamily.
43.2 Befullyinvolvedindiscussionsaboutwhethertoconveneachild protection conference.
43.3 Requestthatchildren’ssocialcareconveneachild protectionconferenceifyouhave seriousconcernsthatachild maynototherwisebeadequatelysafeguarded.
…
concerns
are
substantiated
and
the
child
is
j
udged
to
be
at
continuing
ris
k
of
significant
har
m?
Children’s social care managers should...
44.1 Ensurethatachild protectionconferenceisconvened, within 15 workingdaysofthe strategydiscussion (orthelast, if morethanonehasbeenheld) toenablethose
professionals mostinvolvedwiththechildandfamily, andthechildandfamilythemselves, toassessallrelevantinformationand planhowtosafeguardthechildand promotehisor herwelfare.
44.2 Ensurethatallrelevant professionals (thosewhohavebeeninvolvedinthechild’s life) areinvitedandabletoattend, aswellasthosewhoarelikelytobeinvolvedinfuture work withthechildandfamily. Incomplex cases, youshouldconsiderwhethertoinvitea professionalwhohasexpertiseinthe particulartypeofharm sufferedbythechildorina child’s particularcondition, forexample, adisabilityorlongterm illness. Inallcases, the mostrelevant peoplefrom eachagencyshouldbeinvited.
44.3 Considerwhethertoseek advicefrom, orhave present, a medical professionalwho can presentthe medicalinformationina mannerwhichcanbeunderstoodbyconference attendeesandenablesuchinformationtobeevaluatedfrom asoundevidencebase.
44.4 Ensurethe parentsareinvitedandhelpedto participate. Family membersshouldbe giventhechild protectionconferencereportsinadvanceoftheconferenceandthey shouldbewrittenintheir preferredlanguage. Wherenecessary, youshoulddiscusswith theconferencechair (who maywishtodiscusswith policeofficers) whetherit maybe necessarytoexcludeoneor morefamily membersfrom allor partoftheconference. It maynotbe possibleforallfamily memberstobe presentatthesametime, andthe extentand mannerofinvolvementoffamily membersshouldbeinformedbywhat isknownaboutthem.
44.5 Discusswiththeconferencechairwhetheranystepsarerequiredto protect professionalstafffrom intimidationeitherintheconferenceorafterit, perhapsthrough policeorlegalaction, andinitiatethisactionifnecessary.
44.6 Ensurethatthedecisionsarerecordedinthe Outcomeofthes47 Enquiries Record (Departmentof Health, 2002c), thereasonsforthem andwhatactionstobetakenby whom andbywhen.
Social workers should…
45.1 Involvethechildinawayappropriatetotheirageandunderstanding. Thisincludes talkingtothem aboutthe purposeoftheconference, the meansbywhichtheywantto expresstheirwishesandfeelings (includingbyattending), aswellaswhattheywantsaidto whom andsharingtheconferencereportswiththem inadvance. Somechildren maynot understandwhathasbeenhappeningtothem and maythereforefinditdifficultto understandwhatyouaretellingthem. Others maybe veryclearbut maynothavebeen abletotalk toatrustedadultor maynothavebeenlistenedto. Allarelikelytohave sufferedemotionalabuse. This meansthatyoushould makesurebeforeanydiscussions thatthechild knowsheorsheisnowsafe.
45.2 Involvethe parentsasappropriateandshareyourreportwiththem inadvanceofthe conference.
45.3 Bringinformationfrom allsourcestogetherintoasystematicchronology. Bringtothe chair’sattention, forresolutionattheconference, anycontradictoryinformation.
45.4 Prepareareportforthe Child Protection Conference (Departmentof Health, 2002c).
GPs and/or medical consultants should…
46.1 Provideareportforthechild protectionconference.
46.2 Wherethechildisanin-patient, considerwithwardstaffand, withcolleaguesinthe coreagencies, howbesttoensuresafedischargeofthechildand, attheappropriate point, sharingofinformationwith primarycarestaff.
46.3 Makeeveryefforttoattendthechild protectionconference.
All practitioners should…
47.1 Contributetoyouragency’swrittenreportinadvanceoftheconference, whichsets outthenatureofinvolvementofstaffattheagencywiththefamily.
47.2 Consider, withtheconferencechair, who maywishtoinvolvethe policeinthese discussions, whetheryourreportcanandshouldbesharedwiththe parents, andifso, when.
What
ha
pp
ens
at
a
child
p
rotection
conference
?
48 Theconferenceshoulddecidewhetherthechildisatcontinuingrisk ofsignificant harm andwhether, therefore, heorsherequiresachild protection plantobe putin place. It maybedecided, wherethechildisnotconsideredtobeatrisk ofcontinuingharm, that sheorhewillnotbethesubjectofachild protection plan. Inthissituation, consideration shouldbegiventothechild’sneedsandwhatfuturehelp wouldassistthefamilyin respondingtothem. Whereappropriate, achildinneed planshouldbedrawnup and reviewedatregularintervalsofno morethaneverysix months (Paragraphs 4.33 and 4.36, Assessment Framework).
49 Whereachildbecomesthesubjectofachild protection plan, itistheresponsibilityof theconferencetoconsiderand makerecommendationsonhowagencies, professionals andthefamilyshouldwork togethertoensurethatthechildwillbesafeguardedfrom harm inthefuture. Thisshouldenableboth professionalsandthefamilytounderstand exactlywhatisexpectedofthem andwhattheycanexpectofothers. Specifictasksinclude thefollowing:
• appointtheleadagency (eitheralocalauthorityorthe NSPCC) anda keyworker (the
lead professional), whoshouldbea qualifiedandexperiencedsocialworkerwhoisa memberofstaffoftheleadstatutoryagency;
• identifythe membership ofacoregroup of professionalsandfamily memberswhowill
develop andimplementthechild protection planasadetailedworkingtool;
• establishhowthechildren, parents (includingallthosewith parentalresponsibility) and
widerfamily membersshouldbeinvolvedintheongoingassessment, planningand implementation process, andthesupport, adviceandadvocacyavailabletothem;
• establishtimescalesfor meetingsofthecoregroup, productionofachild protection
plan, andforchild protectionreview meetings;
• identifyinoutlinewhatfurtheractionisrequiredtocompletethecoreassessmentand
whatotherspecialistassessmentsofthechildandfamilyarerequiredto makesound judgementsonhowbesttosafeguardand promotethechild’swelfare;
• outlinethechild protection plan (Departmentof Health, 2002c), especiallyidentifying
whatneedstochangeinordertosafeguardand promotethewelfareofthechild. Theplanshould: