Address for correspondence D. Md. Mostaque Hassan Chowdhury Manikganj Sadar Hospital,
Manikganj, Bangladesh Email: [email protected]
Original Article
Clinicopathological study of cutaneous
vasculitides
Md. Mostaque Hassan Chowdhury*, Md. Qamrul Hassan Jaigirdar**, ATM
Asaduzzaman**, Md. Mostaque Mahmud**, Agha Masood Choudhury**, Harashit Kumar Paul**
* Manikganj Sadar Hospital, Manikganj, Bangladesh
**Department of Dermatology and Venereology, Bangabandhu Sheikh Mujib Medical University, Dhaka
Abstract Objective To study the different patterns of cutaneous vasculitides along with their underlying etiologic factors and to assess the clinicopathological correlation.
Methods A cross sectional study was conducted on 30 consecutive patients, histologically diagnosed as cutaneous vasculitis in the department of dermatology and venereology, BSMMU, Dhaka. All patients were subjected to a baseline workup consisting of complete hemogram, serum-creatinine levels, liver function tests, chest X-ray, urine (routine and microscopic) examination besides antistreptolysin O titer, antinuclear antibody assay, rheumatoid factor assay, antineutrophilic cytoplasmic antibodies and hepatitis B and C. Histopathological examination was done in all patients while immunofluorescence was done in 9 patients.
Results Out of a total of 30 patients diagnosed histologically as cutaneous vasculitis, 22 were classified as cutaneous small vessel vasculitis (CSVV), 6 as Heinoch-Schonlein purpura, and one each as urticarial vasculitis, and Behcet’s syndrome. Approximately 30% of the patients had a significant drug history, 23.3% were attributed to infection. No cause was found in 46.7% cases. Only 9 patients could undergo direct immunofluorescence (DIF), out of which 4 were positive for vasculitis.
Conclusion Cutaneous small vessel vasculitis was the commonest type of vaculitis presenting to the dermatology outpatient department. The workup of patients with cutaneous vasculitis includes detailed history, clinical examination and investigations to rule out multisystem involvement followed by skin biopsy and DIF at appropriate stage of evolution of lesions. Follow up of these patients is very essential as cutaneous manifestations may be the formefruste of serious systemic involvement.
Key words
Leukocytoclastic vasculitis, urticarial vasculitis, Henoch-Schonlein purpura, Behcet’s syndrome.
Introduction
Vasculitis is a term used broadly to refer to multiple different clinicopathological entities in which inflammation and necrosis of the blood
vessels are central to the disease process.1
Cutaneous vasculitis is a histopathologic entity
characterized by neutrophilic transmural
inflammation of the blood vessel wall associated with fibrinoid necrosis, termed leukocytoclastic vasculitis. Other histologic findings that may be
seen include extravasated erythrocytes,
granulocytic debris (leukocytoclasis),
and deposition of immunoreactants in the vessel wall. Clinical manifestations of cutaneous vasculitis occur when small and/or medium vessels are involved. Small-vessel vasculitis can present as palpable purpura, urticaria, pustules, vesicles, petechiae, or erythema multiforme-like lesions. Signs of medium-vessel vasculitis include livedo reticularis, ulcers, subcutaneous nodules, and digital necrosis.
The overall annual incidence is estimated to be between 10 and 42 cases per million per year. Takayasu arteritis occurs predominantly in young females. While Kawasaki disease and
Henoch-Schonlein purpura are the most
common types of childhood vasculitis, temporal arteritis occurs in patients generally older than 55 years of age. Small-vessel vasculitis, predominantly cutaneous, occurs at all ages; but the underlying etiology differs between children and older adults.
The classification of vasculitis is controversial with no generally accepted classification system. The classification system of the American College of Rheumatology (ACR) and of the Chapel Hill Consensus Conference (CHCC) have gained wide acceptance. Yet, they need to
be updated, especially with regard to
leukocytoclastic vasculitis, the most common vasculitis of the skin.1 Classification system of
ACR of 1990 is based on clinical, histologic and disease history while that of CHCC is based solely on histopathology.2
No obvious triggering event has been detected to date in primary vasculitis; in contrast, the etiology of secondary vasculitis is known and includes inflammatory reaction to drugs, infection, neoplasia, or autoimmune disease.3
Based on current data, cutaneous vasculitis is associated with the following conditions: idiopathic (45%-55%), infection (15%-20%),
inflammatory disease (15%-20%), drug intake (10%-15%), and malignancy (5%).4 Most of the
vasculitic syndromes are generally thought to be mediated by immunopathologic mechanisms. Irrespective of the primary immunopathogenic events leading to vasculitis, activation of the vascular endothelium by several cytokines plays a pivotal role in the localization and propagation of vascular injury. The majority of vasculitides affecting the skin result from immunologic injury.5
Effective measurement of disease activity, disease damage and function are the current gold standards of the evaluation of patient status.6
Recognition of the clinical features of vasculitis and evaluation with selected laboratory and other clinical tests and histologic evaluation of biopsy specimens generally permits a specific diagnosis, which directs the evaluation of activity, extent, and damage, and guides treatment.7
In general, treatment of cutaneous vasculitis should include avoidance of triggers and the induction of therapy that follows a ladder from safe and cheap for non-ulcerative purpuric lesions to extensive and dangerous treatment for severe systematic disease with ulcers and infarcts.8 This study was planned to evaluate the
different patterns of cutaneous vasculitides and associated etiologic factors in our country and to determine the clinico-pathological correlation.
Methods
vasculitis of all age and sex group were included in the study.
Study procedure
Clinical diagnosis of cutaneous vasculitis was made on the basis of morphology of cutaneous lesions and associated signs and symptoms. A detailed clinical history and complete physical examination was carried out in all patients. Relevant history and clinical findings of other systemic involvement were enquired for and noted. All the information and findings were recorded in a properly designed data collection sheet. Primary selection was made from history and physical examination. These primarily selected patients were approached for being included in the study. The aims and objectives of the study were explained to the patients in easily
understandable local language and then
informed written consent was taken from interested patients. Patients unwilling to undergo investigations or those with bleeding disorder in whom skin biopsy was contraindicated were excluded from the study. All patients were subjected to a baseline workup consisting of complete hemogram, serum creatinine levels, liver function tests, chest X-ray, urine (routine and microscopic) examination, ASO titer, ANCA and hepatitis B and C antibody profile. Specific investigations such as ANA and RA tests were done in 26 and 18 patients, respectively. Histopathological examination of lesional skin biopsy specimen from all patients was done while direct immunofluorescence (DIF) test was done in 9 patients only. Histologically confirmed cutaneous vasculitis patients were finally selected for the study. The data regarding different variables were analyzed accordingly.
Results
The Table 1 shows the age distribution of respondents where minimum age was 10 years and maximum age was 65 years with mean age of 31.9±14.28 years. There were 15 (50%) females and 15 (50%) males. The marital status of the respondents was 70% (n=21) married and only 30% (n=9) unmarried. Service holders, 9 (30%); students, 8 (27%); and housewives, 7 (23%) constituted the majority of patients.
Minimum duration of disease was 5 days and maximum 120 days with more than 86% had history of sudden onset and progression of disease was rapid in about 80% cases.
Aggravating factors included, drugs in 30% cases, exercise in 26.7%, sun exposure in 6.7% and trauma, water and cold exposure in 3.3% each. History of drug intake was present in 9 (30%) patients. The drugs associated with vasculitis were NSAIDs in 2 (22%) cases, antibiotics in 2 (22%) and 1 (11%) each for frusemide, oral contraceptive pills (OCPs), sulfasalazine, antidiabetics and homeopathic drugs.
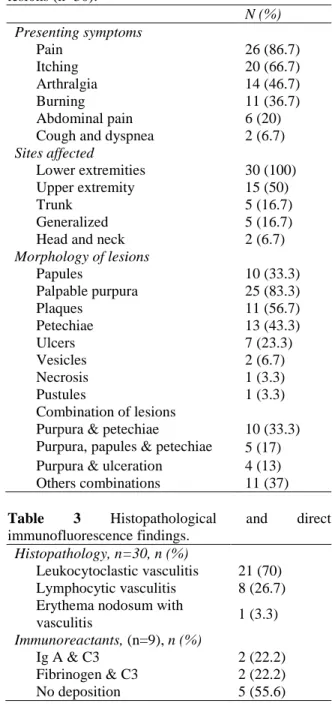
Table 2 shows the symptoms of the respondents where 26 (86.7%) developed pain, 20 (66.7%) itching, 14 (46.7%) arthralgia, 11 (36.7%) burning, 6 (20%) abdominal pain while only 2 (6.7%) respondents had had both cough and shortness of breath. The involvement of body parts of the respondents showed 30 (100%) of lower extremity, 15 (50%) of upper extremity, 5 (17%) of trunk, 2 (7%) of head and neck and generalized 5 (17%) involvement.
Table 1 Demographic and clinical characteristics of study population (n=30).
Age (years)
Minimum 10
Maximum 65
Mean 31.9±14.28
Sex, n (%)
Male 15 (50%0
Female 15 (50%0
Marital status, n (%)
Married 21 (71%)
Unmarried 9 (29%)
Occupations, n (%)
Service 9
Business 3
Housewife 7
Student 8
Others 3
Duration of disease (days)
Minimum 5
Maximum 120
Mean 28.20±27.03
Mode of onset, n (%)
Sudden 26 (86.7)
Insidious 4 (13.3)
Progression of disease, n (%)
Rapid 24 (80)
Slow 6 (20)
Aggravating factors, n (%)
Drugs 9 (30)
Exercise 8 (26.7)
Sun exposure 2 (6.7)
Trauma 1 (3.3)
Exposure to water 1 (3.3)
Exposure to cold 1 (3.3)
Past history of same disease, n (%)
Present 14 (46.7)
Absent 16 (53.3)
Drug history, n (%)
Present 9 (30)
Absent 21 (70)
Drugs used, n (%), n=9
NSAIDS 2 (22)
Antibiotics 2 (22)
Frusemide 1 (11)
Oral contraceptive pills 1 (11)
Sulfasalazine 1 (11)
Antidiabetics 1 (11)
Homeopathic 1 (11)
vesicles, pustules and necrosis. The most common combination of lesions was purpura and petechiae which was 10 (33%).
Table 2 Symptoms, morphology and distribution of lesions (n=30).
N (%) Presenting symptoms
Pain 26 (86.7)
Itching 20 (66.7)
Arthralgia 14 (46.7)
Burning 11 (36.7)
Abdominal pain 6 (20)
Cough and dyspnea 2 (6.7)
Sites affected
Lower extremities 30 (100)
Upper extremity 15 (50)
Trunk 5 (16.7)
Generalized 5 (16.7)
Head and neck 2 (6.7)
Morphology of lesions
Papules 10 (33.3)
Palpable purpura 25 (83.3)
Plaques 11 (56.7)
Petechiae 13 (43.3)
Ulcers 7 (23.3)
Vesicles 2 (6.7)
Necrosis 1 (3.3)
Pustules 1 (3.3)
Combination of lesions
Purpura & petechiae 10 (33.3) Purpura, papules & petechiae 5 (17) Purpura & ulceration 4 (13) Others combinations 11 (37)
Table 3 Histopathological and direct immunofluorescence findings.
Histopathology, n=30, n (%)
Leukocytoclastic vasculitis 21 (70) Lymphocytic vasculitis 8 (26.7) Erythema nodosum with
vasculitis 1 (3.3)
Immunoreactants, (n=9), n (%)
Ig A & C3 2 (22.2)
Fibrinogen & C3 2 (22.2)
No deposition 5 (55.6)
Histopathological and direct
immunofluorescence findings are shown in
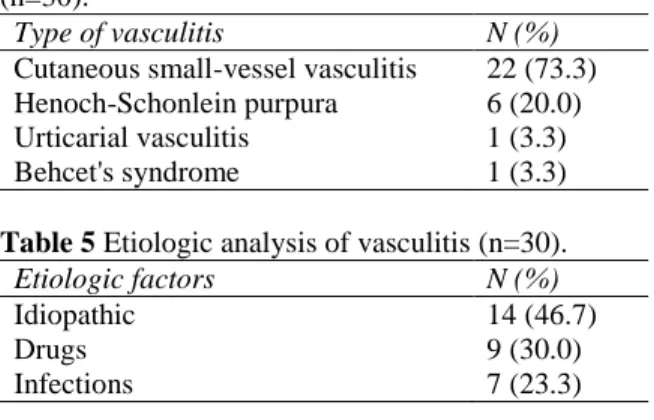
Table 4 Result of clinicopathological correlation (n=30).
Type of vasculitis N (%)
Cutaneous small-vessel vasculitis 22 (73.3) Henoch-Schonlein purpura 6 (20.0) Urticarial vasculitis 1 (3.3)
Behcet's syndrome 1 (3.3)
Table 5 Etiologic analysis of vasculitis (n=30).
Etiologic factors N (%)
Idiopathic 14 (46.7)
Drugs 9 (30.0)
Infections 7 (23.3)
and 2 (22.2%) had fibrin and C3 deposit. No deposition was found in 5 (55.6%) cases.
Table 4 shows the ultimate diagnosis of 30 respondents. Among them 22 (73%) had cutaneous small vessel vasculitis, 6 (20%) Henoch-Schonlein purpura, 1 (3%) had Behcet’s syndrome and urticarial vasculitis each. Regarding the etiology of vasculitis, it was idiopathic in majority i.e. 46.7%, drug-induced in 30%, and associated with infection in 23.3% (Table 5).
Discussion
Cutaneous vasculitis is a poorly understood entity due to its protean clinical manifestation and its overlap with various infections, connective tissue disorders and malignancies. In our study, we analyzed clinical features, relevant past history and various laboratory tests to reach a clinical diagnosis of cutaneous vasculitis among 30 respondents. An attempt was also made to find out etiology and to categorize the disease entities seen.
A total of 30 patients was analyzed, their age was from 10 to 65 years and mean age was 31.9 year and about 60% patients was within 20-40 year age group. Males and females were equally affected in our study. A similar study was performed by Leelavathi et al.9 (2009) on 85
patients. They found the age range 13-93 years and mean age was 36.5 years. Patients were more commonly within 20-40 years age groups with equal occurrence among males and females. Their study results were mostly similar with ours.
In our study we tried to search for aggravating factors of our respondents. Aggravating factors were identified in 22 (43%) patients; among them drugs, 9 (30%), exercise, 8 (26.7%) sun exposure, 2 (6.7%), trauma, water and cold exposure were the listed factors. In another study by Sais et al.10 (1998), exercise (30.5%)
was the main aggravating factor of cutaneous vasculitis. This result is near to our findings.
The mean duration of lesions at the time of presentation was found to be 28.2 days within a range of 5-120 days. We found that in most of the cases onset of disease was sudden 26 (86.7%) but insidious onset was in few cases. Progression of disease was rapid in 24 (80%) cases and was slow in rest of the cases.
Pain was the most common presenting symptoms of our respondents. 86.7% patients complained of pain, 46.7% had itching, 36.7% arthralgia and 6.7% abdominal pain. Sais et al.10
carried out a study on 160 patients and found 30% patients presented with pain in lesions, 41.4% with pruritus, 36.7% with arthralgia and 9.5% with abdominal pain. They found pruritus as most common symptoms whereas we found pain as the commonest one.
17% and head and neck 7%. Gupta et al.1 (2009)
in a similar study found 86% of skin lesions were palpable purpura and 44% of that was plaque, ulcer, bullae, vesicle, ecthyma, gangrene of toes and urticarial lesions. Alexander et al.11
(2003) found the most common affected site was lower limb (38%). The other affected sites were upper limb, trunk, face in that order of frequency either alone or in combination. Results of their study support our results in this regards.
Histopathology was done in all patients while direct immunofluorescence (DIF) study was carried out in 9 cases. Leukocytoclastic vasculitis was found in 21 (70%) cases where predominant cell was neutrophil with nuclear debris, 8 (27%) cases showed lymphocytic vasculitis and erythema nodosum with vasculitis was found in 1 (3%) case. Histopathological findings of our study were similar with that of Gupta et al.1 (2009) where they found 72% cases
with leukocytoclastic small-vessel vasculitis and 12% cases with lymphocytic vasculitis.
DIF was done in 9 cases where we found IgA and C3 deposition in 2 (22.2%) cases and fibrinogen and C3 deposition in 2 (22.2%) cases. No deposition was found in remaining 5 (55.6%) samples.
In our study diagnosis was made with correlating clinical features and pathological reports. Among 30 cases we diagnosed, 22 (73.3%) cases as cutaneous small-vessel vasculitis (CSVV), 6 (20%) cases as Henoch-Schonlein purpura (HSP), 1 (3.3%) case as urticarial vasculitis and 1 (3.3%) case as Behcet’s syndrome.
Our study was designed to search etiological factors of vasculitis. We found that 9 (30%) of our cases were drug-induced. List of the offending drugs was as: NSAIDs (2), oral
contraceptive pills (1), furosemide (1), oral hypoglycemic agent (1), homeopathic medicines (1), sulfasalazine (1) and azithromycin (2). 7 (23.3%) patients were associated with infection. Streptococcal infection was evidenced in all the cases. Causes of vasculitis were undefined in 14 (46.7%) cases. Therefore, we found that most common cause of vasculitis is idiopathic.
In a similar study of Alexander et al.11 (2003)
they found 78% cases were idiopathic, 4% due to infection, 4% were drug induced and 14% associated with collagen vascular diseases.
Their result was different from our findings. We found 46.7% as idiopathic whereas it was 78% in their results. Overall they identified causes in 22% cases but we detected etiologic factors in 53.3% cases.
Our study was designed to make diagnosis of vasculitis clinically and histopathologically and to find etiologic factors. We believed that early diagnosis of disease, identification of etiologic factors and their control would help us to manage cutaneous vasculitis patients properly. In this respect result of our study will enrich current knowledge of cutaneous vasculitic disorder in both nationally and globally in dealing with this type of patients.
Conclusion
This study shows that the commonest symptom of cutaneous vasculitis was pain and palpable purpura was the commonest skin lesion which mainly affected the lower limbs. The most common causes of cutaneous vasculitis were drugs and infections but in the majority of cases it remained unveiled. This highlights the importance of detailed drug history in patients presenting with cutaneous vasculitis. This is a
nonprescribed over the counter drugs are
randomly used. Literature on cutaneous
vasculitis is scarce nationally and globally. A large scale study is required to support our study outcome.
References
1. Gupta S, Handa S, Kanwar AJ et al. Cutaneous vasculitides: Clinico-pathological correlation. Indian J Dermatol Venereol Leprol. 2009;75:356-62.
2. Summa C, Hoffman C. Cutaneous vasculitis. J Am Osteopath Coll Dermatol. 2006;6:28-30.
3. Maunz G, Conzett T, Zimmerli W. Cutaneous vasculitis associated with fluoroquinolones. Infection. 2009;37:466-68.
4. Fiorentino DF. Cutaneous vasculitis. J Am Acad Dermatol. 2003;48:311-40.
5. Csernok E, Gross WL. Primary vasculitides and vasculitis confined to skin: clinical
features and new pathogenic aspects. Arch Dermatol Res. 2000;292:427-36.
6. Luqmani RA. Disease assessment in systemic vasculitis. J Indian Rheumatol Assoc. 2003;11:35-44.
7. Gamarra AI, Metteson EL, Restrepo JF. Small vessel vasculitis: History, classification, etiology, histopathology, clinic, diagnosis and treatment. Colomb Rheumatol. 2001;24:187-205.
8. Chen KR, Carlson JA. Clinical approach to cutaneous vasculitis: Treatment. Am J Clin Dermatol. 2008;9:71-92.
9. Leelavathi M, Aziz SA, Gangaram H B et
al. Cutaneous vasculitis: A review of
aetiology and clinical manifestations in 85
patients in Malaysia. Med J Malaysia.
2009;64:210-2.
10. Sais G, Vidaller A, Jucgla A et al. Prognostic factors in leukocytoclastic vasculitis: a clinicopathologic study of 160 patients. Arch Dermatol. 1998;134:309-15. 11. Alexander B, Rameshkumar K, Layaseelan