Gestational Age and Developmental
Risk in Moderately and Late Preterm
and Early Term Infants
Luisa Schonhaut, MD, MPH, MSca,b, Iván Armijo, BScc, Marcela Pérez, MDa,b
abstract
OBJECTIVES:The objective of this study was to evaluate the association between gestational age (GA) at birth and risk of developmental delay at 8 and 18 months of corrected postnatal age.
METHODS:During 2008 to 2011, infants at a corrected postnatal age of 8 or 18 months attending health centers in Santiago, Chile, were recruited. Participants completed a form on
biographical and demographic characteristics and the Chilean validated version of the Ages and Stages Questionnaires, Third Edition (ASQ). Logistic regression was used to detect the capacity of GA to predict scores, 22 SDs on the basis of the Chilean ASQ reference group, in at least 1 ASQ domain, adjusted by different control variables.
RESULTS:A total of 1667 infants were included in the analysis. An inverse“dose response” relationship between developmental delay risk and GA at birth was found, both in the crude and adjusted models. Compared with those born full term, the odds ratio for developmental delay risk was 1.56 for those born early term (95% confidence interval [CI]: 1.19–2.06), 2.58 for infants born late preterm (95%CI: 1.66–4.01), and 3.01 for those born moderately preterm (95%CI: 1.59–5.71).
CONCLUSIONS:An inverse dose-response relationship between GA and risk of developmental delay was found in the tested population. Future prospective studies and predictive models are needed to understand whether this higher developmental risk in moderately and late preterm infants is transient and modifiable or persists throughout life, allowing for better targeting of early-intervention strategies.
WHAT’S KNOWN ON THIS SUBJECT:There is growing evidence reporting that moderately preterm, late preterm, and early term infants are at increased risk of developmental delay. The characteristics of this association are not well established in the literature.
WHAT THIS STUDY ADDS:In a sample of infants born between 32 and 41 weeks, there was an inverse and“dose response” relationship between gestational age and developmental delay risk using the ASQ at 8 and 18 months of corrected postnatal age.
a
Departmento de Pediatria, Clínica Alemana, Santiago, Chile;bFacultad de Medicina, Clinica Alemana-Universidad del Desarrollo, Santiago, Chile; andcFacultad de Psicología, Universidad Gabriela Mistral, Santiago, Chile
Dr Schonhaut conceptualized and designed this study, coordinated and supervised data collection, and drafted the initial manuscript; Mr Armijo carried out the statistical analyses and reviewed and revised the manuscript; Dr Pérez recruited the patients and reviewed and revised the manuscript; and all authors approved thefinal manuscript as submitted.
www.pediatrics.org/cgi/doi/10.1542/peds.2014-1957
DOI:10.1542/peds.2014-1957 Accepted for publication Jan 27, 2015
Address correspondence to Luisa Schonhaut, MD, MPH, MSc, Departamento de Pediatria, Clínica Alemana, Vitacura 5951, Santiago, Chile. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2015 by the American Academy of Pediatrics
Over the past decades, developed countries have seen a decrease in their natality rates, with a relative increase in births before 40 weeks of gestational age (GA).1,2This same trend has occurred in Chile, where total preterm births increased from 5.0% to 6.6% over the past 17 years.3 This situation can be explained by an increased obstetric risk as a result of late primiparity, an increase in multiple pregnancies, and better pregnancy and labor monitoring techniques.4
There has been growing research regarding the risk of moderately preterm (MPT; born by 320/7to 336/7 weeks of gestation), late preterm (LPT; 340/7to 366/7weeks), and early term (ET; 370/7to 386/7weeks) children compared with full-term (FT) infants (390/7to 416/7weeks of gestation) since 2005. These children have a higher risk of short-term perinatal morbidity2,5–7and long-term developmental, behavioral, and learning difficulties.8,9–18However, despite the evidence, there is still controversy regarding the actual impact of delivery before the end of gestation. For example, there is debate about the use of corrected postnatal age at the time of
assessment of MPT and LPT infants. Woythaler et al19showed that LPT infants had a 50% increased risk of developmental delay at
a chronological age of 2 years. Romeo et al20compared the performance of LPT children at 12 and 18 months, with and without correcting for postnatal age, and found that differences compared with children born FT disappeared after correction. On the other hand, Walsh et al21 recently showed that a group of MPT and LPT infants had smaller brain size, less myelination, and more immature gyral folding measured by MRI compared with term infants at 38 to 44 weeks’corrected GA.
Another controversy focuses on the determinants of developmental impact. Some authors have
speculated that it could be the result of prematurity, whereas others believe that it is due to associated factors, such as morbidity and NICU admission.22Gurka et al23reported that healthy LPT infants born after 340/7weeks, without neonatal complications, had long-term cognition, achievement, socioemotional, and behavioral development equivalent to FT infants. Baron et al24found lower
performance in infants with
complicated LPT birth compared with those with uncomplicated birth. This hypothesis has been discredited by MacGowan et al,25who found no significant differences in early childhood development between LPT infants admitted to the NICU and those who were not.
A real difficulty in drawing
conclusions regarding the impact of delivery before term is the
heterogeneity of instruments used and diverse ages of infants at the time of assessments, as well as the fact that most published studies were conducted in retrospective or population-based cohorts.11,26
The objective of this study was to evaluate the association between GA at birth and risk of developmental delay at 8 and 18 months of corrected postnatal age by using the Ages and Stages Questionnaires, Third Edition (ASQ).27These ages were selected on the basis of Chilean public health guidelines for screening of development in children.28
METHODS
A cross-sectional study was carried out with the use of a convenience sample of infants aged 8 to 18 months. The ET and FT sample of infants was extracted from the normative sample who participated in the validation study of the ASQ for the Chilean population, which took place between May 2008 and November 2011. In the same time period, MPT and LPT infants were selected by direct contact in health services. Children were
recruited from public health centers located in the southeastern and northern districts and from a private eastern center of the metropolitan region of Santiago, Chile.
Participants
A convenience sample was
constructed on the basis of patients who attended the health center for their routine follow-up visit. Term infants were recruited at scheduled health visits, and preterm infants were identified on the basis of local birth databases in each center and were contacted purposely for the study. Parents or primary caregivers who agreed to participate signed an informed consent and completed a form with medical and biographical and demographic information. GA information was disclosed by the parents and verified with medical records. The chronological age of infants born at#366/7weeks was corrected by subtracting the weeks remaining to complete 400/7weeks. Infants were classified on the basis of GA as MPT (320/7to 336/7weeks of gestation), LPT (340/7to 366/7weeks of gestation), ET (370/7to 386/7 weeks of gestation), or FT (390/7to 416/7weeks of gestation).26
Infants aged 7 to 8 months and 30 days and 17 to 18 months and 30 days were included in the study. Each child was tested only once during the study either at 8 or 18 months. The tests were completed on the basis of the appropriated chronological (for FT and ET) or corrected postnatal (for MPT and LPT) ages.
Infants with known genetic, metabolic, or neurologic disease (n= 14); those born at,32 weeks (n= 10); or those born equal at $420/7weeks (n= 33) were excluded. Those infants without known GA (n= 54) were also excluded. After exclusions, afinal sample of 1667 patients was included in the analysis.
Outcome Measures
skills and development from 1 to 66 months of age. Twenty-one
questionnaires are available within this age range. Parents answer 30 questions covering 5 domains of development, including
communication, gross motor,fine motor, problem-solving, and adaptive skills. Parents are instructed to try activities with their child to facilitate accurate assessment. A pass/fail score was assigned for each area of development. The presence of any domain that screened, 22 SDs below the mean area score for the Chilean reference group was considered to be a positive screen, indicating risk of developmental delay. The ASQ has been validated in several countries.29,30,31In Chile, the sensitivity and specificity ranges of 75% (95% CI 62%–85%) and 81% (95% CI 76%–86%), respectively, have been reported.32Parents also completed a form with personal, socioeconomic, demographic, perinatal, and medical information.
Ethics
The ethics committees of the National Fund approved this study for Health Research (FONIS), Southwest Santiago Health Service, Southeast Santiago Health Service, and Facultad de Medicina Clinica Alemana-Universidad del Desarrollo.
Statistical Analysis
Sample characteristics were
described by using the risk frequency for risk of developmental delay in the different GA groups. With the use of data on this criterion, a multivariate-adjusted logistic regression model was constructed. In addition, a series of dummy variables were generated to identify the risk associated with each week of gestation; 40 weeks of GA was used as a reference.
The analysis included the following control variables: socioeconomic status (based on the socioeconomic classification used as a reference for our country),33teenage mother (,19 years old at the time of birth), NICU
admission, small for GA (birth weight ,10th percentile according to validated tables for Chilean
population),34gender, multiple birth, and ASQ administration age (8 or 18 month). Analyses were performed by using R (Vienna, Austria) and Stata 12 (StataCorp, College Station, TX) platform statistics with a linear trend module.
RESULTS
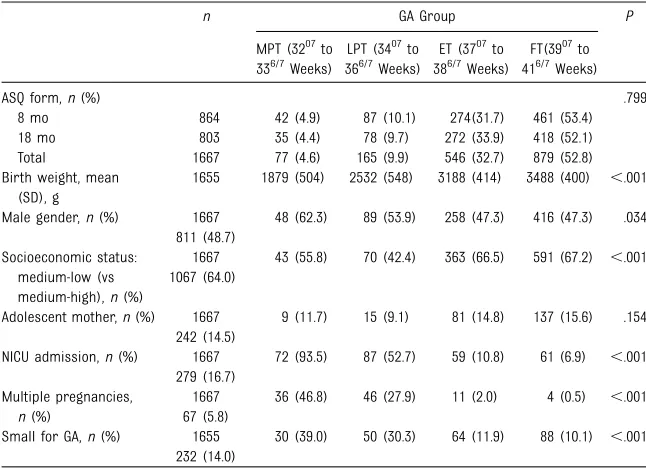
Perinatal and biographical and demographic characteristics of the 1667 participants are shown in Table 1. We observed that the GA distribution of infants evaluated at 8 and 18 months was homogeneous. There was a comparable frequency of teenage pregnancy in all GA groups. In contrast, there was a higher incidence of small for GA, NICU admitted, and multiple births in the preterm infants groups compared with FT group.
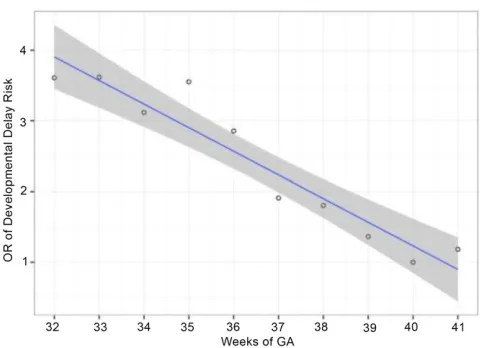
A trend toward decreased risk of developmental delay as GA increased was observed (42.86%, 37.58%, and 23.81% for MPT, LPT, and ET, respectively, compared with 17.63% for FT children). An inverse“dose response”relationship between GA
and risk of developmental delay was also observed (Fig 1).
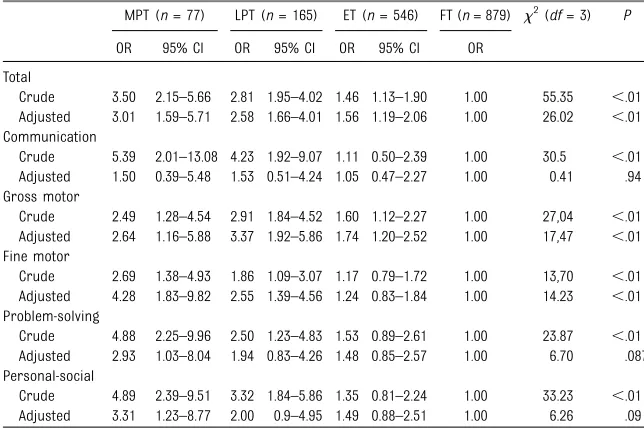
When adjusting for predefined variables, the odds of developmental delay risk based on ASQ scores also increased significantly and were inversely related to GA. Compared with those born FT, odds ratios (ORs) were 1.56 (95% confidence interval [CI]: 1.19–2.06) for those born ET, 2.58 (95% CI: 1.66–4.01) for infants born LPT, and 3.01 (95% CI: 1.59–5.71) for those born MPT. The number of affected domains increased as GA decreased. In MPT infants the OR was significant for all domains except for communication. In LPT infants the OR was significant for gross andfine motor domains, whereas for ET infants the OR was significant only in gross motor skills (Table 2). There was a trend for linearity between adjusted risk of developmental delay and GA in the 33- to 40-week interval (Fig 2). The x2for trend of ORs was 27.33 (P,.001). An evaluation for adjustment of linear trend of the relation between GA and development delay risk was significant (F= 81.87,P,.001,
R2= 0.90) and no significant improvements in adjustment were found for quadratic (F= 3.19,P= .11)
TABLE 1 Background Characteristics of Participating Children
n GA Group P
MPT (3207to 336/7Weeks)
LPT (3407to 366/7Weeks)
ET (3707to 386/7Weeks)
FT(3907to 416/7Weeks)
ASQ form,n(%) .799
8 mo 864 42 (4.9) 87 (10.1) 274(31.7) 461 (53.4) 18 mo 803 35 (4.4) 78 (9.7) 272 (33.9) 418 (52.1) Total 1667 77 (4.6) 165 (9.9) 546 (32.7) 879 (52.8) Birth weight, mean
(SD), g
1655 1879 (504) 2532 (548) 3188 (414) 3488 (400) ,.001
Male gender,n(%) 1667 48 (62.3) 89 (53.9) 258 (47.3) 416 (47.3) .034 811 (48.7)
Socioeconomic status: medium-low (vs medium-high),n(%)
1667 43 (55.8) 70 (42.4) 363 (66.5) 591 (67.2) ,.001 1067 (64.0)
Adolescent mother,n(%) 1667 9 (11.7) 15 (9.1) 81 (14.8) 137 (15.6) .154 242 (14.5)
NICU admission,n(%) 1667 72 (93.5) 87 (52.7) 59 (10.8) 61 (6.9) ,.001 279 (16.7)
Multiple pregnancies,
n(%)
1667 36 (46.8) 46 (27.9) 11 (2.0) 4 (0.5) ,.001 67 (5.8)
or cubic (F = 0.16,P= .70)fit, when compared with linearfit.
When evaluating the effect of each factor isolated from others using univariate analysis, we found associations between risk of developmental delay and GA, NICU admission, multiple pregnancy, and male gender. When controlling for the effects of other predictors using multivariate analysis, GA, male gender, adolescent mother, and ASQ administration age remained significant (Table 3).
DISCUSSION
We found an inverse, dose-response relationship between corrected GA and risk of developmental delay considering birth at 40 weeks as a reference and after adjusting for predefined control variables. In accordance with our results,
previous studies that used the ASQ to identify children at risk of
developmental delay found greater developmental delay risk in LPT and MPT infants compared with term infants.8,35
In our study, there was a significant linear inverse relationship between weeks of GA and risk of
developmental delay. In addition, no significant improvements were found comparing that adjustment with quadratic or cubicfit. Studies that included extremely preterm children found a linear association between decreasing GA and cognitive development,36,37whereas others reported an exponential association below 36 weeks by using the ASQ.37 Nevertheless, all studies reported a consistent inverse
relationship.13,39–42
The inverse relationship between weeks of GA and frequency of psychomotor problems has
a physiologic explanation. It has been described that the last weeks of pregnancy are a critical period for fetal brain development at molecular, neurochemical, and structural levels.43,44Kugelman and Colin45 presented a descriptive model that combined the pathology that is responsible for preterm delivery and the exposure of the immature brain to the hazards present in the
extrauterine environment. Kerstjens et al22described that LPT infants exposed to neonatal morbidities presented the highest risk of developmental delay. Moreover, the recent data published by Walsh et al21demonstrated that there is a significant measurable difference in brain size, myelination, and gyral folding between MPT, LPT, and term newborns after correcting for GA at birth, which could potentially explain the differences in development.
In our study, we found high
frequencies of risk of developmental delay over all GA groups, comparable to other researchers who used the ASQ.30,46Those frequencies were higher for 8-month-old children than for 18-month-old children. In the multivariate analysis, the most significant factor for developmental delay risk was ASQ administration age. Other studies conducted by our TABLE 2 Crude and Adjusted ORs and 95% CIs for Developmental Delay Based on the ASQ
MPT (n= 77) LPT (n= 165) ET (n= 546) FT (n= 879) x2(df= 3) P
OR 95% CI OR 95% CI OR 95% CI OR
Total
Crude 3.50 2.15–5.66 2.81 1.95–4.02 1.46 1.13–1.90 1.00 55.35 ,.01 Adjusted 3.01 1.59–5.71 2.58 1.66–4.01 1.56 1.19–2.06 1.00 26.02 ,.01 Communication
Crude 5.39 2.01–13.08 4.23 1.92–9.07 1.11 0.50–2.39 1.00 30.5 ,.01 Adjusted 1.50 0.39–5.48 1.53 0.51–4.24 1.05 0.47–2.27 1.00 0.41 .94 Gross motor
Crude 2.49 1.28–4.54 2.91 1.84–4.52 1.60 1.12–2.27 1.00 27,04 ,.01 Adjusted 2.64 1.16–5.88 3.37 1.92–5.86 1.74 1.20–2.52 1.00 17,47 ,.01 Fine motor
Crude 2.69 1.38–4.93 1.86 1.09–3.07 1.17 0.79–1.72 1.00 13,70 ,.01 Adjusted 4.28 1.83–9.82 2.55 1.39–4.56 1.24 0.83–1.84 1.00 14.23 ,.01 Problem-solving
Crude 4.88 2.25–9.96 2.50 1.23–4.83 1.53 0.89–2.61 1.00 23.87 ,.01 Adjusted 2.93 1.03–8.04 1.94 0.83–4.26 1.48 0.85–2.57 1.00 6.70 .087 Personal-social
Crude 4.89 2.39–9.51 3.32 1.84–5.86 1.35 0.81–2.24 1.00 33.23 ,.01 Adjusted 3.31 1.23–8.77 2.00 0.9–4.95 1.49 0.88–2.51 1.00 6.26 .09
The analysis included the following control variables: socioeconomic status, teenage mother (,19 years old at the time of birth), NICU admission, small for gestational age (birth weight,10th percentile according to validated tables for the Chilean population), gender, multiple birth, and ASQ form.df, degrees of freedom.
FIGURE 1
group also found a higher frequency of lower ASQ scores in smaller infants, probably associated with parenting practices, with a late catch-up in development. Another
significant factor was male gender, which is in accordance with the results of other authors, although there is no a clear explanation of the reason for this difference39,47Some authors even proposed the use of differentiated norms for boys and girls, but this issue still needs more research.29
Unexpectedly, giving birth in adolescence appears to be a protective factor for the risk of developmental delay. Although there
is evidence suggesting that teen mothers could be less accurate in identifying developmental delay risk in their children,48we believe that these results require further research, including the impact of cultural factors that could affect parenting styles, such as family constitution and family network support for the adolescent mother.
We found it appropriate to correct the GA of MPT and LPT infants both at 8 and 18 months of age on the basis of previous reports.20Although currently there are no published data to support correcting GA in ET infants, we believe this is a topic that needs further research. Nevertheless,
considering the application guidelines for the ASQ, with a 2-month window for child evaluation, correcting 2 or 3 weeks of age for ET has never changed the recommended application form.
A limitation of this study could be its cross-sectional design. Although the response rate was high, there is no information on the number of eligible children who declined to participate. Because of the nature of the sampling procedure
(convenience sampling), the sample is not necessarily representative of the overall population and some GA groups could be over- or
underrepresented. It is possible that there was a greater representation of parents/caregivers who were concerned about the health and development of their children, a variable that could be potentially relevant as has been proposed by other researchers.49
To increase the knowledge on these associations and to clarify the controversies raised, it is critical to have better prospective studies and predictive models to understand the long-term effect of each
developmental risk factor in these populations. Prospective research is necessary for a better understanding of whether the impact of moderate and late prematurity is transient and potentially modifiable or if the differences persist throughout life.50,51Clearly, much research remains to be done in these preterm populations to understand how these differences in development evolve throughout childhood and for better targeting of early-intervention strategies.
ACKNOWLEDGMENTS
We thank Dr Xavier Demestre and Dr Kevin Marks for reviewing and editorial assistance. We also thank Dr Sergio Muñoz for statistical assistance and Dr Andres Maturana for
final review and amendment of the
final version of the manuscript. FIGURE 2
Trend of ORs for risk of developmental delay based on the ASQ using 40 weeks of GA as the baseline. Note: ORs were adjusted to control the effects of ASQ administration age (8 or 18 month) socio-economic status, teenage mother, NICU admission, small for gestational age, gender, and multiple birth. Higher log ORs indicate higher probability of the presence of developmental delay risk in the child (equal OR:x2= 54.69,P,.001; trend of odds:x2= 27.33,P,.001). Solid line shows trend of ORs for risk of developmental delay and shaded area shows 95 CI trend.
TABLE 3 Univariate and Multivariate Analyses for Risk of Developmental Delay Based on the ASQ Variable Univariate Analysis Multivariate Analysis
OR (95% CI) P OR (95% CI) P
Fetal and neonatal risk factors
Weeks remaining to 40 weeks of GAa 1.21 (1.15–1.28) ,.001 1.21 (1.12–1.31) ,.001
NICU admission 1.87 (1.41–2.48) ,.001 0.96 (0.65–1.40) .832 Small for GA 1.10 (0.79–1.51) .573 0.85 (0.58–1.22) .383 Multiple pregnancy 2.65 (1.73–4.03) ,.001 1.35 (0.78–2.28) .268 Male gender 1.39 (1.11–1.75) .004 1.42 (1.11–1.81) .005 Other factors
Low socioeconomic status 0.64 (0.51–0.81) ,.001 0.88 (0.68–1.15) .342 Adolescent mother 0.53 (0.36–0.76) ,.001 0.56 (0.37–0.84) .006 ASQ administration age 3.15 (2.46–4.06) ,.001 3.36 (2.60–4.38) ,.001
FUNDING:Supported by the Clinica Alemana research grants program and grant SA7I20043 from the National Fund for Health Research (FONIS).
POTENTIAL CONFLICT OF INTEREST:The authors have indicated they have no potential conflicts of interest to disclose.
REFERENCES
1. Blencowe H, Cousens S, Oestergaard MZ, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications.Lancet. 2012; 379(9832):2162–2172
2. Guasch XD, Torrent FR, Martínez-Nadal S, Cerén CV, Saco MJ, Castellví PS. Prematuros tardíos: una población de riesgo infravalorada [Late preterm infants: a population at underestimated risk].An Pediatr (Barc). 2009;71(4):291–298
3. López PO, Bréart G. Trends in gestational age and birth weight in Chile, 1991-2008: a descriptive epidemiological study.BMC Pregnancy Childbirth. 2012;12:121
4. Spong CY, Mercer BM, D’alton M, Kilpatrick S, Blackwell S, Saade G. Timing of indicated late-preterm and early-term birth.Obstet Gynecol. 2011;118(2 pt 1): 323–333
5. Raju T, Higgins R, Stark A, Leveno K. Optimizing care and outcome for late-preterm (near-term) infants: a summary of the workshop sponsored by the National Institute of Child Health and Human Development.Pediatrics. 2006; 118(3):1207–1214
6. Teune MJ, Bakhuizen S, Gyamfi Bannerman C, et al. A systematic review of severe morbidity in infants born late preterm.Am J Obstet Gynecol. 2011;205 (4):374.e1–e9
7. Brown HK, Speechley KN, Macnab J, Natale R, Campbell MK. Neonatal morbidity associated with late preterm and early term birth: the roles of gestational age and biological determinants of preterm birth.Int J Epidemiol. 2014;43(3):802–814
8. Kerstjens JM, de Winter AF, Bocca-Tjeertes IF, ten Vergert EMJ, Reijneveld SA, Bos AF. Developmental delay in moderately preterm-born children at school entry.J Pediatr. 2011;159(1):92–98
9. Morse SB, Zheng H, Tang Y, Roth J. Early school-age outcomes of late preterm infants.Pediatrics. 2009;123(4). Available at: www.pediatrics.org/cgi/content/full/ 123/4/e622
10. Petrini JR, Dias T, McCormick MC, Massolo ML, Green NS, Escobar GJ. Increased risk of adverse neurological development for late preterm infants.
J Pediatr. 2009;154(2):169–176
11. McGowan JE, Alderdice FA, Holmes VA, Johnston L. Early childhood development of late-preterm infants: a systematic review.Pediatrics. 2011;127(6): 1111–1124
12. Schonhaut L, Perez M, Schonstedt M, et al. Moderately and late preterm newborns, a risk group for low cognitive development in thefirst years of life.Rev Chil Pediatr. 2012;83(4):358–365
13. Poulsen G, Wolke D, Kurinczuk JJ, et al. Gestational age and cognitive ability in early childhood: a population-based cohort study.Paediatr Perinat Epidemiol. 2013;27(4):371–379
14. Kirkegaard I, Obel C, Hedegaard M, Henriksen TB. Gestational age and birth weight in relation to school performance of 10-year-old children: a follow-up study of children born after 32 completed weeks.Pediatrics. 2006;118(4):1600–1606
15. Talge NM, Holzman C, Wang J, Lucia V, Gardiner J, Breslau N. Late-preterm birth and its association with cognitive and socioemotional outcomes at 6 years of age.Pediatrics. 2010;126(6):1124–1131
16. Noble KG, Fifer WP, Rauh VA, Nomura Y, Andrews HF. Academic achievement varies with gestational age among children born at term.Pediatrics. 2012; 130(2). Available at: www.pediatrics.org/ cgi/content/full/130/2/e257
17. Dong Y, Chen SJ, Yu JL. A systematic review and meta-analysis of long-term development of early term infants.
Neonatology. 2012;102(3):212–221
18. Rose O, Blanco E, Martinez SM, et al. Developmental scores at 1 year with increasing gestational age, 37-41 weeks.
Pediatrics. 2013;131(5). Available at: www.pediatrics.org/cgi/content/full/131/ 5/e1475
19. Woythaler MA, McCormick MC, Smith VC. Late preterm infants have worse 24-month neurodevelopmental outcomes than term infants.Pediatrics. 2011;
127(3). Available at: www.pediatrics.org/ cgi/content/full/127/3/e622
20. Romeo DM, Di Stefano A, Conversano M, et al. Neurodevelopmental outcome at 12 and 18 months in late preterm infants.
Eur J Paediatr Neurol. 2010;14(6): 503–507
21. Walsh JM, Doyle LW, Anderson PJ, Lee KJ, Cheong JLY. Moderate and late preterm birth: effect on brain size and maturation at term-equivalent age.
Radiology. 2014;273(1):232–240
22. Kerstjens JM, Bocca-Tjeertes IF, de Winter AF, Reijneveld SA, Bos AF. Neonatal morbidities and developmental delay in moderately preterm-born children.
Pediatrics. 2012;130(2). Available at: www.pediatrics.org/cgi/content/full/130/ 2/e265
23. Gurka MJ, LoCasale-Crouch J, Blackman JA. Long-term cognition, achievement, socioemotional, and behavioral development of healthy late-preterm infants.Arch Pediatr Adolesc Med. 2010; 164(6):525–532
24. Baron IS, Erickson K, Ahronovich MD, Baker R, Litman FR. Cognitive deficit in preschoolers born late-preterm.Early Hum Dev. 2011;87(2):115–119
25. McGowan JE, Alderdice FA, Doran J, et al. Impact of neonatal intensive care on late preterm infants: developmental outcomes at 3 years.Pediatrics. 2012; 130(5). Available at: www.pediatrics.org/ cgi/content/full/130/5/e1105
26. Vohr B. Long-term outcomes of moderately preterm, late preterm, and early term infants.Clin Perinatol. 2013; 40(4):739–751
27. Squires J, Bricker D.Ages and Stages Questionnaires, Third Edition (ASQ-3): A Parent-Completed Child-Monitoring System. Baltimore, MD: Brookes Publishing Company; 2009
Chile 2004. Available at: http://web. minsal.cl/sites/default/files/files/2004_ Normas_tecnicas_estimulacion_y_ evaluacion_desarrollo.pdf. Accessed February 9, 2015
29. Richter J, Janson H. A validation study of the Norwegian version of the Ages and Stages Questionnaires.Acta Paediatr. 2007;96(5):748–752
30. Juneja M, Mohanty M, Jain R, Ramji S. Ages and Stages Questionnaire as a screening tool for developmental delay in Indian children.Indian Pediatr. 2012; 49(6):457–461
31. Filgueiras A, Pires P, Maissonette S, Landeira-Fernandez J. Psychometric properties of the Brazilian-adapted version of the Ages and Stages Questionnaire in public child daycare centers.Early Hum Dev. 2013;89(8): 561–576
32. Schonhaut L, Armijo I, Schönstedt M, Alvarez J, Cordero M. Validity of the Ages and Stages Questionnaires in term and preterm infants.Pediatrics. 2013;131(5). Available at: www.pediatrics.org/cgi/ content/full/131/5/e1468
33. Adimark. Mapa Socioecónico de Chile. 2004. Available at: www.adimark.cl/ medios/estudios/mapa_
socioeconomico_de_chile.pdf. Accessed December 4, 2014
34. Milad M, Novoa JM, Fabres J, Samamé M, Aspillaga C. Recomendación sobre Curvas de Crecimiento Intrauterino.Rev Chil Pediatr. 2010;81(3):264–274
35. Marks K, Hix-Small H, Clark K, Newman J. Lowering developmental screening thresholds and raising quality improvement for preterm children.
Pediatrics. 2009;123(6):1516–1523
36. Kato T, Yorifuji T, Inoue S, Yamakawa M, Doi H, Kawachi I. Associations of preterm
births with child health and development: Japanese population-based study.J Pediatr. 2013;163(6): 1578–1584.e4
37. Soria-Pastor S, Padilla N, Zubiaurre-Elorza L, et al. Decreased regional brain volume and cognitive impairment in preterm children at low risk.Pediatrics. 2009;124(6). Available at: www.pediatrics. org/cgi/content/full/124/6/e1161
38. Kerstjens JM, de Winter AF, Bocca-Tjeertes IF, Bos AF, Reijneveld SA. Risk of developmental delay increases exponentially as gestational age of preterm infants decreases: a cohort study at age 4 years.Dev Med Child Neurol. 2012;54(12):1096–1101
39. Mathiasen R, Hansen B, Nybo Andersen AM, Forman J, Greisen G. Gestational age and basic school achievements: a national follow-up study in Denmark.
Pediatrics. 2010;126(6). Available at: www.pediatrics.org/cgi/content/full/126/ 6/e1553
40. MacKay DF, Smith GCS, Dobbie R, Pell JP. Gestational age at delivery and special educational need: retrospective cohort study of 407,503 schoolchildren.PLoS Med. 2010;7(6):e1000289
41. Shapiro-Mendoza C, Kotelchuck M, Barfield W, et al. Enrollment in early intervention programs among infants born late preterm, early term, and term.
Pediatrics. 2013;132(1). Available at: www.pediatrics.org/cgi/content/full/132/ 1/e61
42. Bhutta AT, Cleves MA, Casey PH, Cradock MM, Anand KJS. Cognitive and behavioral outcomes of school-aged children who were born preterm: a meta-analysis.
JAMA. 2002;288(6):728–737
43. Kinney HC. The near-term (late preterm) human brain and risk for periventricular
leukomalacia: a review.Semin Perinatol. 2006;30(2):81–88
44. Kapellou O, Counsell SJ, Kennea N, et al. Abnormal cortical development after premature birth shown by altered allometric scaling of brain growth.PLoS Med. 2006;3(8):e265
45. Kugelman A, Colin AA. Late preterm infants: near term but still in a critical developmental time period.Pediatrics. 2013;132(4):741–751
46. Guevara JP, Gerdes M, Localio R, et al. Effectiveness of developmental screening in an urban setting.Pediatrics. 2013; 131(1):30–37
47. Hintz SR, Kendrick DE, Vohr BR, Kenneth Poole W, Higgins RD; NICHD Neonatal Research Network. Gender differences in neurodevelopmental outcomes among extremely preterm, extremely-low-birthweight infants.Acta Paediatr. 2006; 95(10):1239–1248
48. Ryan-Krause P, Meadows-Oliver M, Sadler L, Swartz MK. Developmental status of children of teen mothers: contrasting objective assessments with maternal reports.J Pediatr Health Care. 2009; 23(5):303–309
49. Janus M, Goldberg S. Factors influencing family participation in a longitudinal study: comparison of pediatric and healthy samples.J Pediatr Psychol. 1997; 22(2):245–262
50. Lindström K, Lindblad F, Hjern A. Psychiatric morbidity in adolescents and young adults born preterm: a Swedish national cohort study.Pediatrics. 2009; 123(1). Available at: www.pediatrics.org/ cgi/content/full/123/1/e47
DOI: 10.1542/peds.2014-1957 originally published online March 2, 2015;
2015;135;e835
Pediatrics
Luisa Schonhaut, Iván Armijo and Marcela Pérez
Early Term Infants
Gestational Age and Developmental Risk in Moderately and Late Preterm and
Services
Updated Information &
http://pediatrics.aappublications.org/content/135/4/e835 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/135/4/e835#BIBL This article cites 44 articles, 16 of which you can access for free at:
Subspecialty Collections
al_issues_sub
http://www.aappublications.org/cgi/collection/development:behavior Developmental/Behavioral Pediatrics
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2014-1957 originally published online March 2, 2015;
2015;135;e835
Pediatrics
Luisa Schonhaut, Iván Armijo and Marcela Pérez
Early Term Infants
Gestational Age and Developmental Risk in Moderately and Late Preterm and
http://pediatrics.aappublications.org/content/135/4/e835
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.