Original Research Article
Prevalence and pattern of alcohol consumption among males attending
primary health care setting using AUDIT in rural
Indore, Madhya Pradesh, India
Jayashri Bute, Sangeeta Kori*, V. K. Arora, Aarti Sahasrabuddhe
INTRODUCTION
Alcohol consumption is a major public health problem in developed as well as developing countries including India. In 2012, globally harmful use of alcohol caused approximately 3.3 million deaths which is 5.9% of all deaths. Five percent of the global burden of disease and injury was attributable to alcohol consumption. As per the most recent WHO data, globally individuals above 15
years of age drink on an average 6.2 liters of pure alcohol per year which is equal to 13.5 grams of pure alcohol per day. World’s 38.3% population is reported to consume alcohol regularly.1
There are more than 200 health conditions like alcohol dependence, cardiovascular diseases, liver cirrhosis, cancer of mouth, pharynx, colon etc. and injuries are related to alcohol. Also the new data has been concluded
ABSTRACT
Background: Alcohol consumption is one of the public health problems in India which acts as major attributable risk factor for majority of morbidity and mortality among adults. The objectives of the study were to find out the prevalence of alcohol consumption and its associated factors in rural area by using a WHO tool, AUDIT (Alcohol Use Disorder Identification Test) and to identify extent and pattern of alcohol consumption.
Methods: This study was cross-sectional study. Three hundred sixty four male patients ≥15 years of age, attending OPD in a primary health care setting were interviewed by using a structured questionnaire and AUDIT.
Results: The overall prevalence of ever consumed alcohol was found to be 49.7%; of which 38.2% were current drinkers and 11.5% were former drinkers while rest 50.3% were life time abstainers. Educational status, occupation, tobacco use and positive family history were significantly associated with alcohol consumption; while type and size of family, socioeconomic status were found insignificant association. About 53.9% preferred country-made liquor while 23.8% Indian Made Foreign Liquor (IMFL). Enjoyment (45.3%), relaxation or stress buster or social cause (29.5%), peer pressure (25.2%) being the reasons for alcohol consumption. In 33% of consumers, daily drinking and in 36% consumers, 1-5 times per week frequency for alcohol drinking was seen respectively. Three fourth of them purchased alcohol from local shops. Out of 364 subjects 75% belongs to AUDIT score of low risk, 11.2% with alcohol use in excess of low risk, 3.6% with harmful and hazardous drinking and 10.2% with dependent drinking.
Conclusions: In our study, alcoholism is found to be more common among illiterates, non-formers, among tobacco users and those having positive family history. Socio economic status and age is not the bar for alcohol consumption.
Keywords: Alcohol consumption, AUDIT, Prevalence, Pattern, Rural
Department of Community Medicine, Index Medical College Hospital and Research Center, Indore, Madhya Pradesh, India
Received: 18 July 2018
Revised: 28 August 2018
Accepted: 30 August 2018
*Correspondence:
Dr. Sangeeta Kori,
E-mail: [email protected]
Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
on causal relationships between the harmful use of alcohol and clinical outcomes of infectious disease such as Tuberculosis, HIV /AIDS and pneumonia.1-3
As per global status report of WHO the average Indian consumes 4.3 liters of alcohol per year while the average rural Indian consumes 11.4 liters of alcohol per year. About 30% Indian population consumes alcohol on regular basis.1 There are marked variations in pattern of alcohol consumption in different parts of India. Recently in India, due to impact of western culture and urbanization seem to have changed the trend from low level to higher levels of alcohol consumption.4
According to NFHS-III survey alcohol consumption ranges from 12.5% in Jammu & Kashmir to 61.1% in Arunachal Pradesh. As per NFHS-III, overall prevalence of alcohol consumption was found to be 31.9% among men and 2.2% in women in India and it was found to be 30.8% in men and 2.8% in women respectively in Madhya Pradesh.5
This study is aimed to find out the exact prevalence and pattern of alcohol consumption in a rural area of Indore district.
METHODS
Setting
This was a cross-sectional study carried out among outdoor male patients ≥15 yrs of age during October-December 2015 in primary health care setting i.e. Rural Health Training Centre which is field practice area for a Tertiary Care Level Teaching Institute, Indore. On an average 30-35 patients are visiting this centre daily for medical care. From these OPD patients, total 364 males who gave verbal consent were included in the study. In pilot study, prevalence of alcohol consumption among females was found negligible, so that they were excluded from study.
Study tool
After obtaining verbal consent, respondents were
interviewed by using a structured pre-tested
questionnaire. Informations on socio-demographic
details, pattern of alcohol consumption were collected.
AUDIT (Alcohol Use Disorder Identification Test), a self rated 10 item questionnaire, prepared by WHO was used to assess harmful and hazardous use of alcohol among study participants. AUDIT was developed to screen for excessive drinking and in particular to help practitioners identify people who would benefit from reducing or ceasing drinking. It has been validated in six countries including India.6-9
It was translated in local language i.e. Hindi and pre-tested for the study. It is again translated back to English to ensure its reliability and validity. Patients are further classified as per AUDIT score. Zone I refers to low risk of drinking or abstinence (AUDIT score=0-7), Zone II, consists of alcohol use in excess of low risk guidelines (AUDIT score =8-15), Zone III, refers to high risk of drinking (AUDIT score 16-19) indicative of harmful and hazardous drinking and Zone IV refers to alcohol dependence (AUDIT score >20).10-12
Definitions used1
Lifetime abstainers-people who have never consumed alcohol.
Current drinker-who had an alcoholic drink in last 12 months.
Former drinker-people who have previously consumed alcohol but who have not done so in the previous 12 months.
Measures of alcohol consumption
A standard drink is used to measure the alcohol intake. It always contains the same amount of pure alcohol regardless of the container size or the type of alcoholic beverage, but may not correspond to the typical serving size. It varies from country to country. In India, a standard drink corresponds to 10 ml of absolute alcohol. Depending on different concentration of alcohol in different liquor available in India one standard drink corresponds to different quantity for each type of beverage e.g. 300 ml of beer,100 ml of wine,30 ml of distilled spirit, 40 ml of arrack and 30 ml of IMFL.13 WHO guideline criteria for risk of consumption of alcohol for men on a single drinking day is low risk as 1 gm-40 gm of absolute alcohol, medium risk as 41-60 gm & high risk as >60 gm.14 So in our study, other than AUDIT scoring, depending on quantity & quality of beverage consumed, alcoholics were also categorized in three category i.e. low, medium and high risk as per WHO guideline.
Data collection and analysis
centre which is under department of community medicine of tertiary care level hospital and research centre, Indore. Dependent drinkers were further followed up at tertiary care hospital for detail management.
RESULTS
Table 1shows sociodemographic characteristics of study participants.
Table 1: Socio-demographic characters of study participants.
Characteristic variables
Proportion of total (N=364)
Percentage (%)
Age (years)
15-24 27 7.4
25-64 305 83.8
≥65 32 8.8
Education
Illiterate 92 25.3
Literate 272 74.7
Marital status
Unmarried 15 4.1
Married 345 94.8
Divorced/Separated/
Widower 04 1.1
Type of family
Single 15 4.1
Nuclear 81 22.3
Joint 242 66.5
Extended 26 7.1
Family size
<5 75 20.6
>5 289 79.4
Occupation
Farmer 245 67.3
Laborer 52 14.3
Service 16 4.4
Others 51 14
Socio-economic status#
Class I (Rs. ≥5638) 15 4.1
Class II (Rs. 2819-5638) 37 10.2
Class III (Rs. 1691-2818) 51 14
Class IV (Rs. 846-1690) 112 30.8
Class V (Rs. <846) 149 40.9
Tobacco use
Yes 98 27
No 266 73
Family history of alcohol
Yes 38 10.4
No 326 89.6
#15, 16, 17.
Males >15 year who gave consent for the study, i.e. 364 participants were included in the study. Most of the
participants 83.8% were from age group 25-64 years, three fourth (75%) of them were literate, while 25% were never attended school. Almost 95% respondents were married. As study was conducted in rural area, most of them 67.3% were farmers by occupation and 66.5% were from joint family. Pertaining to their socioeconomic class 72% were from lower socioeconomic and lower middle class as per Modified B.G. Prasad Classification (Table 1).15-17
Table 2 shows univariate analysis of socio-demographic factors with alcohol consumption.
Overall 139 (38.2%) of adults had consumed alcohol in past 12 months. Among the users, 39.7% of current drinkers were from the age between 25-64 years; we even observed that majority youths 37% were also involved in alcohol consumption. In this study, more percentage of alcohol consumers was found among illiterate males (48%) as compare to literates (35%). The proportion of alcohol users were higher (100%) among divorced/ separated or widower followed by married and then unmarried once. The difference was found to be statistically insignificant.
The proportion of alcohol consumers was higher among laborers 59.3% than farmers as well as service class. Alcohol consumption did not show any significant association with family size and type of family. Although in our study, socioeconomic status has not shown any significant association with alcohol use; but it was seen that proportion of alcohol consumers was increasing as income is decreasing. Associated tobacco use was found in 97 (69.8%) current alcohol user. All those who were having positive family history of alcohol consumption i.e. 38 (27.3%) have shown significant association with alcohol use.
On univariate analysis of socio-demographic characters determining alcohol consumption, it was found that education (p<0.028), occupation (p<0.0009), associated tobacco use (p<0.0001) and positive family history for alcohol intake (p<0.0003) were significantly associated with alcohol consumption. Proportion of alcohol consumption was higher among males who were illiterate
(OR=1.707, CI=1.05-2.76), laborers (OR=0.353,
CI=0.191-0.652), tobacco users (OR=517, CI=70.19-3812.88) and having positive family history for alcohol intake (OR=171.06, CI=10.40-2812.09) (Table 2).
Pattern of alcohol consumption
Table 2: Univariate analysis showing association between socio-demographic factors and alcohol consumption.
Variable
Alcohol users (current drinker) (N=139) (%)
Alcohol non users (lifetime abstainers +former drinkers) (N=225)(%)
Unadjusted
OR 95% CI P value
Age (year)
15-24 10 (37) 17 (63) 1
>0.78
25-64 121(39.7) 184 (60.3) 0.894 0.396-2.019
≥65 08 (25) 24 (75) 1.764 0.576-5.398
Literacy
Illiterate 44 (48) 48 (52) 1
<0.028
Literate 95 (35) 177 (65) 1.707 1.057-2.757
Marital status
Unmarried 05 (33.3) 10 (66.7) 1
>0.734
Married 130 (37.7) 215 (62.3) 0.826 0.276-2.473
Divorced/separated 04 (100) 00(0%) 0.058 0.002-1.29
Type of family
Single 06 (40) 09 (60) 1
>0.207
Nuclear 37 (45.7) 44 (54.3) 0.792 0.258-2.434
Joint 90 (37.2) 152 (62.8) 1.125 0.388-3.267
Extended 06 (23.1) 20 (76.9) 2.222 0.560-8.817
Family size
<5 32 (42.7) 43 (57.3) 1
>0.37
>5 107 (37) 182 (63) 1.265 0.755-2.120
Occupation
Farmer 84 (34.3) 161 (65.7) 1
<0.0009
Laborer 31 (59.3) 21 (40.4) 0.353 0.191-0.652
Service 07 (43.8) 09 (56.2) 0.670 0.241-1.864
Other 17 (33.3) 34 (66.7) 1.043 0.550-1.977
Socioeconomic class
Class I 04 (26.7) 11 (73.3) 1
>0.55
Class II 13 (35) 24 (65) 0.671 0.177-2.53
Class III 14 (27.5) 37 (72.5) 0.961 0.262-3.523
Class IV 43 (38.4) 69 (61.6) 0.583 0.174-1.949
Class V 65 (43.6) 84 (56.4) 0.46 0.14-1.54
Tobacco use
Yes 97 (99) 01 (1) 1
<0.0001
No 42 (15.8) 224 (84.2) 517.33 70.19-3812.88
Family history of alcohol
Yes 38 (100) 00 (0) 1
<0.0003
No 101 (31) 225 (69) 171.06 10.40-2812.09
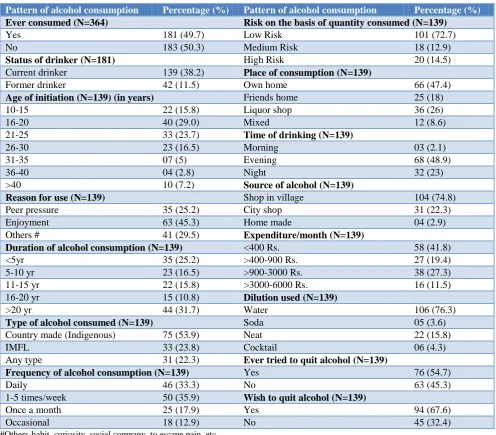
Among users, most of them 29% have started consuming alcohol between 16-20 year of age, while 15.8% started consuming alcohol below 15 yr of age. The reasons for alcohol consumption were, enjoyment in 45% of users, 29.5% to escape from pain or social company, while 25.2% were consuming due to peer pressure. About three-forth of the alcohol consumers were consuming alcohol for long term i.e. >5 years and alcohol was available to them in nearby shops of liquor within village itself. Majority of the users i.e.54% were using country-made liquor (indigenous) followed by 23.8% were consuming IMFL (Indian Made Foreign Liquor) and remaining 22.3% were consuming any kind of liquor
water while 16% were drinking without dilution. Regarding willingness of leaving the habit, 67.6% wish to
quit while 55% tried to quit in their lifetime (Table 3).
Table 3: Distribution of respondents as per pattern of alcohol consumption.
Pattern of alcohol consumption Percentage (%) Pattern of alcohol consumption Percentage (%)
Ever consumed (N=364) Risk on the basis of quantity consumed (N=139)
Yes 181 (49.7) Low Risk 101 (72.7)
No 183 (50.3) Medium Risk 18 (12.9)
Status of drinker (N=181) High Risk 20 (14.5)
Current drinker 139 (38.2) Place of consumption (N=139)
Former drinker 42 (11.5) Own home 66 (47.4)
Age of initiation (N=139) (in years) Friends home 25 (18)
10-15 22 (15.8) Liquor shop 36 (26)
16-20 40 (29.0) Mixed 12 (8.6)
21-25 33 (23.7) Time of drinking (N=139)
26-30 23 (16.5) Morning 03 (2.1)
31-35 07 (5) Evening 68 (48.9)
36-40 04 (2.8) Night 32 (23)
>40 10 (7.2) Source of alcohol (N=139)
Reason for use (N=139) Shop in village 104 (74.8)
Peer pressure 35 (25.2) City shop 31 (22.3)
Enjoyment 63 (45.3) Home made 04 (2.9)
Others # 41 (29.5) Expenditure/month (N=139)
Duration of alcohol consumption (N=139) <400 Rs. 58 (41.8)
<5yr 35 (25.2) >400-900 Rs. 27 (19.4)
5-10 yr 23 (16.5) >900-3000 Rs. 38 (27.3)
11-15 yr 22 (15.8) >3000-6000 Rs. 16 (11.5)
16-20 yr 15 (10.8) Dilution used (N=139)
>20 yr 44 (31.7) Water 106 (76.3)
Type of alcohol consumed (N=139) Soda 05 (3.6)
Country made (Indigenous) 75 (53.9) Neat 22 (15.8)
IMFL 33 (23.8) Cocktail 06 (4.3)
Any type 31 (22.3) Ever tried to quit alcohol (N=139)
Frequency of alcohol consumption (N=139) Yes 76 (54.7)
Daily 46 (33.3) No 63 (45.3)
1-5 times/week 50 (35.9) Wish to quit alcohol (N=139)
Once a month 25 (17.9) Yes 94 (67.6)
Occasional 18 (12.9) No 45 (32.4)
#Others-habit, curiosity, social company, to escape pain, etc.
AUDIT scoring
Figure 1 shows distribution of respondents as per AUDIT score. Overall prevalence of current drinkers was found to be i.e. 139 (38.2%). Out of 364, 273 respondents (75%) were with AUDIT score 0-7 (zone I) which includes complete abstainers and low risk drinkers. Forty one (11.2%) respondents were in excess alcohol use with AUDIT score 8-15 (zone II), while 13 (3.6%) respondents were harmful and hazardous alcohol users with AUDIT score 16-19 (zone III) and rest 37 (10.2%) respondents were having dependence of alcohol with AUDIT score ≥20 (zone IV) respectively. The mean
AUDIT score was 5.5 with SD ±8.66 (Figure 1). Figure 1: Distribution of the respondents as per
AUDIT score risk zone.
75% 11.20%
3.60% 10.20%
ZONE I
ZONE II
ZONE III
DISCUSSION
In this study details of prevalence, pattern of drinking was studied by using WHO developed tool-AUDIT among male patients visiting Rural health care centre of tertiary care level institute, Indore. Total 364 male patients of the age >15 yr, attended OPD over the period of three months were involved in the study. As we had recorded under-representation of female respondents consuming alcohol in pilot study so we excluded them from our study. Majority of the participants were from 25-54 years of age group. Twenty five percent populations were illiterate, 67% participants were farmers by occupation and majority i.e. 95% were married.
Prevalence of alcohol consumption
The overall prevalence of ever consumption of alcohol was found to be 49.7% while prevalence of current drinkers was 38.2%. Lifetime abstainers were 50.2% (183). The findings are at par with the study done by Pati et al in primary health care setting in district of Odisha.18 Sujiv et al in primary care setting in rural Puducherry reported lifetime use of alcohol and current users was 58.6% and 39.8% respectively while Bhardwaj et al reported it 37.7%.19,20 Chawala et al reported prevalence of ever alcohol consumption and current alcohol consumption 25.7% and 36.9% respectively in rural block of Haryana.21 Contradictory findings were found in study done in Tamil Nadu by Ganesh et al which stated prevalence of current alcohol use was 9.4%, 29.8% by Saxena et al and 30.8% in study by Bodhare et al respectively.22-24
Correlates of alcohol consumption
As for as the association of socio-demographic determinants were concerned, 39.7% current drinkers were belonged to the age between 25-64 yr with least being above 55 year of age. These results are in conformity with Gururaj et al and Sathya et al.4,25 But in our study, change in trend has been observed that 37% youth were involved in alcohol consumption. In our study educational status was found to be statistically associated with alcohol use. Nearly half of the users, 48% were illiterate. These results is in line with Deswal et al, Gupta et al.26,27
In our study, all the divorced or widower (100%) were consuming alcohol followed by married and then unmarried once. This might be due to stress in relationships or worries which let person indulge in such habit. The results were found insignificant which is consistent with Deswal et al, Singh et al, Negi et al.26,28,29 In present study association of type of family, family size and Socio-economic status with current alcohol intake was not found significant. Although it was seen alcohol intake was higher in nuclear family, class-V, lower
middle income group as per Modified BG Prasad but found to be statistically insignificantly associated.
It was observed that alcohol consumption was highest among laborers 59.3%, followed by service class (43.8%). These findings were found in line with the study done by Sumit et al.21 This is due to stress at workplace, peer pressure etc. Meena et al also found maximum alcohol use in laborer while Ramanan et al reported maximum use was among farmers.30,31
Based on our findings, association of tobacco use, family history of alcohol use was found highly significant (p<0.0003) with the current alcohol intake. It was found that 69.8% of alcohol users were also using tobacco, while Ramanan et al found it 45%.31 These findings are in congruent with study by Abdoul et al,and contradictory with the study by Mohan et al.32,33 Associated tobacco use along with the alcohol is said to have synergistic action. Tobacco use was found to be significantly associated.
Positive family history was seen in 27.3% alcohol users while these findings are similar to study done by Meena et al which stated positive family history in 23.2% cases.30 Highly significant association for positive family history was found. This is common practice in family, if parents are consuming alcohol children are obviously would have been affected by their behavior.
Pattern of alcohol consumption
In our study following pattern of drinking were observed. In present study, among 139 current drinkers, 29.5% were initiated alcohol drinking between the age of 16 to 20 years while 16% started consuming alcohol even before the 15 year which is legally prohibited age. Which signals the failure of law system, this finding is in congruent with Meena et al while Sumit et al reported corresponding it as 24 year.30,21 Basu et al reported as 18 years, while contradictory with deswal et al.34,35
When inquired about reason for alcohol use, 45% explained it for enjoyment and 29.5% were consuming for escaping from pain, work stress as well for social company and 25.2% were due to peer pressure. These findings were similar to study by Ramanan et al in which 44.4% used alcohol for fun while inconsistent findings were reported by Sreeraj et al and Meena et al i.e. 26.6% users cited to be sociable as reason for drinking, 23% to forget worries.31,35,30
About duration of alcohol consumption, three –fourth (74.8%) of drinkers were long term users i.e. consuming alcohol >5 years and 25% were recent users i.e. consuming alcohol < 5 yrs.
More than half of alcohol users (53.9%) were using country-made liquor due to cost factor as well as their easy availability in the vicinity of village, followed by 24% of them were consuming IMFL (Indian Made Foreign Liquor) and 22.3% were consuming any kind of liquor available showing their dependency. Sathya shown 62% consumers prefer locally brewed beverages and 38% men prefer IMFL in Andaman And Nicobar Islands.25 When inquired about frequency of alcohol consumption, 36% were consuming alcohol 1 to 5 times/ week, 33% were consuming alcohol daily due to dependency. This was found to be inconsistent with study done by Girish et al in rural area of Bangluru district which stated 29.7% users were consuming alcohol daily.36 Sumit et al reported 26.6% of the current users drank alcohol almost daily while Sugathan et al reported it to be 13%.21,37 Half of the users (49%) were consuming alcohol at evening time to get relieved by work stress while 26% were consuming any time of the day indicating their disturbed social and personal life due to dependency. Nearly half of the users (47.4%) were consuming alcohol at home and 26% were consuming at liquor shop indicating their urge of drinking while in a study by Girish et al it was 63% at home & 64% at wine shop in rural population, the difference may be due to multiple responses in this study.36 Three fourth of consumers (74.8%) purchased alcohol from local shops available in their villages itself or nearby villages. Other contributing factors were cheap rate and availability of small quantity packets commonly called as pouch or thaili. Locally country made alcohol was available as Safed (with lower concentration) and Lal or Narangi (with higher concentration)
When asked about expenditure nearly half of the users (41.5%) were spending <400 Rs/month as socioeconomic status may be constraint. Still 11.5% managed to spend >3000-6000 Rs/month. Nearly three forth of consumers (76%) were consuming alcohol after diluting with water, 19.4% with soda while 16% were consuming without dilution as directly related to health. More than half of users, (68%) want to quit the habit of alcohol, while 55% tried to quit in their life time.
AUDIT scoring
In this study, prevalence of low risk drinking or abstinence (Zone I: AUDIT score-0-7) was 62%, alcohol use in excess of low risk (Zone II: AUDIT score 8-15) was 11.2%, harmful & hazardous drinking (Zone III: AUDIT score-16-19) was 3.6% and alcohol dependence (Zone IV: AUDIT score ≥20) was 10.2%. So overall harmful drinking (AUDIT score ≥8) was found to be 25%. Study done among adults by Rathod et al in Sehore district of Madhya Pradesh estimated 33.2% hazardous drinking while 5.5% alcohol dependency.39 In a study of Paschim Medinipur district in the state of West Bengal, Arkaprapbha Sau reported 34.5% harmful and hazardous
drinking, while Anamitra et al reported high prevalence of 73% men with AUDIT score of >8.39,40 In study by Sathya et al at Andman Nicobar Islands, overall prevalence of alcohol consumption was 35% among males. One-fourth of the total users (23%) were alcohol dependents while almost 18.0% of male drinkers reported heavy drinking on typical drinking occasions. 25
CONCLUSION
Present study concludes that prevalence of alcohol is still high in the rural population. Alcoholism is more common among illiterates, non-farmers, among tobacco users & among those having positive family history. Socio economic status and age is not the bar for consumption. Changing trend of alcohol consumption is seen among the youths. Easy and low cost liquor availability within the vicinity also contributes. So there is need to implement more strict laws and policy makers must revise the strategies to reduce the prevalence. AUDIT was found to be very useful tool for screening of alcoholic patients at primary health care setting. So timely referral can be done for high risk alcoholic patients.
De-addiction programme, stress relievers in the form of meditation, yoga etc should also be made available to rural area.
Limitation of the study
Sample was restricted to rural population only & sample size was very small. Recall bias was also there which was unavoidable. So more studies are needed in this field to cover rural and urban population.
Funding: No funding sources Conflict of interest: None declared
Ethical approval: The study was approved by the Institutional Ethics Committee
REFERENCES
1. World Health Organization. A Summary of Global Status Report on Alcohol and Health, Management of Substance Dependence, Non-communicable Diseases, WHO, 2014. Available at: www.who. int/ substance_abuse/publication/global_alcohol_report/ en/. Accessed on 5 August 2015.
2. Babor T, Campbell R, Room R, Saunders J. Geneva:
Lexicon of Alcohol and Drug Terms. World Health Organization, 1994.
3. Reid MC, Fiellin DA, O’Connor PG. Hazardous and
harmful alcohol consumption in primary care. Arch Intern Med. 1999;159:1681-9.
4. Gururaj G, Girish N, Benegal V. Burden and
5. International Institute for Population Sciences (IIPS) and Macro International. 2008. National Family Health Survey (NFHS-III), India, 2005-2006: Madhya Pradesh, Mumbai: IIPS. Available at:
atiipsindia.org/research.htm Accessed on 8
December 2017.
6. Saunders JB, Aasland OG, Babor TF, de la Fuente,
Grant M. Development of the Alcohol Use Disorder Identification Test (AUDIT): WHO collaborative project on Early detection of persons with harmful alcohol consumption-II. Addiction. 1993;88:791-804.
7. Saunders JB, Aasland OG, Amundsen A, Grant M. Alcohol consumption and related problems among primary health care patients: WHO collaborative project on early detection of persons with harmful alcohol consumption. I. Addiction. 1993;88:349- 62. 8. Pal HR, Jena R, Yadav D. Validation of the Alcohol
Use Disorder Identification Test in urban
community outreach and de-addiction centre
samples in North India. J Stud Alcohol
2004;65:794-800.
9. Nayak MB, Bond JC, Cherpitel C, et al. Detecting alcohol-related problems in developing countries: a comparison of 2 screening measures in India. Alcohol Clin Exp Res. 2009;33:2057–66.
10. Clements R. A critical evaluation of several alcohol screening instruments using the CIDI-SAM as a criterion measure. Alcoholism: Clin Experimental Res. 1998;22(5):985-93.
11. Hays RD, Merz JF and Nicholas R. Response
burden, reliability and validity of the CAGE, Short MAST and AUDIT alcohol screening measures. Behavioural Res Methods Instruments Computers. 1995;27:277-80.
12. Babor TF, John C, Higgins-Biddle, John B,
Monteiro MG. AUDIT (Alcohol Use Disorder Identification Test) Guidelines for use in primary care, Second edition-2001 WHO document: Department of Mental Helath and Substance Dependence, 2001.
13. Types of alcohol beverages. Alcohol web India.
Available at https://www.alcoholwebindia.in/
content/types-alcoholic-beverages Accessed on 18 august 2015.
14. World Health Organization (2000) International guide for monitoring alcohol consumption and
related harm. World Health Organization,
Department of Mental Health and Substance Dependence, Non communicable Diseases and Mental Health Cluster, Copenhagen.
15. Sharma R. Revision of Prasad’s social classification and provision of an online tool for Real time updating, South Asia Journal Cancer 2013;2(3):157. 16. Sharma R. Online interactive calculator for Real
time update of Prasad’s social classification Available at: www.prasadscaleupdate.weekly.com. Accessed on 12th October 2015.
17. Modified B. G. Prasad Socio economic
classification. Available at www. labourbureau. nic. in/indnum.Htm. Accessed on 14 June 2016.
18. Pati S, Swain S, Mahapatra S, Hussain MA, Pati S. Prevalence, Pattern and correlats of alcohol misuse among male patients attending rural primary care in India. J Pharm Bioallied Sci. 2017;9(1):66–72.
19. Sujiv A, Chinnakali P, Balajee K,
Lakshminarayanan S, Kumar SG, Roy G. Alcohol use and alcohol use disorder among male outpatients in a primary care setting in rural Puducherry. Ind Psychiatry J. 2015;24(2):135-9. 20. Bhardwaj SD, Shwete MK, Bhatkule PR, Khadse
JR. Prevalence of risk factors for
Non-communicable disease in rural area of Nagpur district, Maharashtra-WHO STEP wise approach. Int J Bio Med Res. 2010;3:1413-8.
21. Chawala S, Baharti, Jain RB, Khanna P, Singh I. Prevalence and correlates of alcohol intake in a rural block of Haryana, India. Int J Interdisciplinary Multidisciplinary Studies. 2014;2(1):144-50.
22. Ganesh Kumar S, Premrajen KC, Subitha L, Suguna
E, Vinayagamoorthy, Kumar V. Prevalence and pattern of alcohol consumption using alcohol use disorders Identification test (AUDIT)in rural Tamil Nadu, India. J Clin Diagn Res. 2013;7(8):1637-9.
23. Saxena V, Kandpal SD, Goel D, Bansal S.
Prevalence of risk factors on non-communicable diseases in a rural population of block Doiwala, Dehradun. Indian J Community Health. 2011;23:65-8.
24. Bodhare TN, Venkatesh K, Bele S, Kashiram G, Devi S, Vivekanand A. A Behavioural risk factors for Non-communicable disease among rural adults in Andra Pradesh. Natl J Community Med. 2013;4:19-24.
25. Sathya PM, Attayuru PS, Kandavelu T,
Dhanasekara P, Kasturi SP, Vivek B. Alcohol consumption, hazardous drinking, and alcohol dependency among the population of Andaman and Nicobar Islands, India. Ind J Pub Health. 2017;61(2):105-11.
26. Deswal BS, Jindal AK, Gupta KK. Epidemiology of
alcohol use among residents of remote hills of Arunachal Pradesh. Indian J Community Med. 2006;31:26-30.
27. Gupta PC, Saxena S, Pednekar MS, Maulik PK. Alcohol consumption among middle aged & elderly men : A Community Study from Western India. Alcohol Alcoholism. 2003;38:327-31.
28. Singh J, Singh G, Mohan V. A comparative study of prevalence of regular alcohol users among male individuals in an urban & rural area of district Amritsar, Punjab. Indian J Community Med. 2000;25:238-44.
30. Meena, Khanna P, Vohra AK, Rajput R. Prevalence and Pattern of Alcohol and substance abuse in urban
area of Rohtak city. Indian J Psychiatr.
2002;44:348-52.
31. Ramanan VV, Sing SK. A study on Alcohol use and
its related Health & Social Problems in Rural Puducherry, India. J family Med Prim Care. 2016;5(4):804-8.
32. Abdoul HM, Dikshit M, Bhaduri D, Aghamolaei T,
S Mooavy SH, Azarpaykan A. Interaction of alcohol Use and Specific Types of Smoking on the Development of Oral Cancer. Int J High Risk Behav Addict. 2014;3(1):e12120.
33. Mohan D, Chopra A, Sethi H. The co-Occurrence of
tobacco and alcohol in general population of metropolis Delhi. Indian J Med Res. 2002;116:150-4.
34. Basu G, Biswas S, Chattergee C. The Behavioral risk factors of non communicable diseases: Experience from a village of Hugli district, West Bengal. IOSR J Dent Med Sci. 2013;4:19-24. 35. Sreeraj VS, Surjeet P, Christody RJK, Uvais NA.
Reasons for substance use: A Comparative Study of alcohol use in Tribals & Non Tribals. Indian J Psycho Med. 2012;34(3):242-6.
36. Girish N, Kavita R, Gururaj G, Benegal V. Alcohol use & implications for public health: patterns of use in Four Communities. IJCM. 2010;35(2):238-44.
37. Sugathan TN, Soman CR, Sankar Narayanan K.
Behavioral risk factors of non communicable diseases among adults in Kerala, India, Indian J Med Res. 2008;127:555-63.
38. Rathod SD, Nadkarni A, Bhana A, Shidhaye R. Epidemiological features of alcohol use in rural India: a population based cross-sectional study. BMJ Open. 2015;5:e009802.
39. Arkaprapbha S. AUDIT (Alcohol Use Disorders
Identification Test) to Estimate the Pattern and Correlates of Alcohol Consumption among the Adult Population of West Bengal, India: A Community Based Cross-sectional Study J Clin Diagn Res. 2017;11(4):1–4.
40. Anamitra B, Rajeshkumar R, Abhijeet C. Alcohol Use-Related Problems Among a Rural Indian Population of West Bengal: An Application of the Alcohol Use Disorders Identification Test (AUDIT) Alcohol Alcoholism. 2016;51(2):215–23.