Xu Fei
1, 2, A, C, D, Zhuge Hongxiang
1, E, F, Chen Qi
2, B, C, Chen Daozhen
2, D, EMaternal Plasma Levels of Endothelial Dysfunction
Mediators Including AM, CGRP, sICAM-1 and tHcy
in Pre-eclampsia
Stężenie w osoczu matki mediatorów dysfunkcji śródbłonka
w stanie przedrzucawkowym – AM, CGRP, sICAM-1 i tHcy
1 Department of Pathogenic Microbiology, Suzhou University, Suzhou, Jiangsu Province, China
2 Department of Laboratory Medicine, Wuxi Municipal Women and Children Health Hospital, Jiangsu Province,
China
A – research concept and design; B – collection and/or assembly of data; C – data analysis and interpretation;
D – writing the article; E – critical revision of the article; F – final approval of article; G – other
Abstract
Background. Pre-eclampsia is a pregnancy-specific disorder of widespread vascular endothelial dysfunction that occurs after twenty weeks of gestation.
Objectives. The aim of the present study was to compare maternal circulating levels of endothelial dysfunction mediators, including the vascular actions of adrenomedullin (AM) and calcitonin gene-related peptide (CGRP), the angiogenic factor of soluble intracellular adhesion molecule-1 (sICAM-1) and the pro-oxidant activity factor of total homocysteine (tHcy), in the plasma of normal and pre-eclampsia pregnancies. Furthermore, the authors investigated whether magnesium sulfate therapy is involved in modulating the circulating levels of these four mol-ecules, thus helping to prevent pre-eclampsia.
Material and Methods. A total of 85 pregnant women were involved in this study, including 30 healthy pregnant women, 15 with pregnancy-induced hypertension (PIH) and 40 with pre-eclampsia (PE). The maternal levels of AM, CGRP, sICAM-1 and tHcy in plasma were determined by enzyme-linked immunoassay (ELISA). Furthermore, the effects of magnesium sulfate therapy on the plasma levels of these four molecules were compared.
Results. Compared to healthy pregnancies, maternal circulating concentration of AM, sICAM-1 and tHcy were significantly higher, while the plasma level of CGRP is significantly lower in pregnant women with hypertension or pre-eclampsia (P < 0.05). Magnesium sulfate therapy can effectively suppress the level of AM, sICAM-1 and tHcy, while increasing the level of CGRP in maternal circulation (P < 0.05).
Conclusions.Present results indicated that AM, CGRP, sICAM-1 and tHcy may be involved in the development and maintenance of hypertension during pregnancy. By modulating these four mediators, magnesium sulfate may inhibit the progress of pre-eclampsia (Adv Clin Exp Med 2012, 21, 5, 573–579).
Key words: adrenomedullin, calcitonin gene-related peptide, soluble intracellular adhesion molecule-1, total homocysteine, pre-eclampsia, magnesium sulfate therapy.
Streszczenie
Wprowadzenie. Stan przedrzucawkowy jest zaburzeniem ciąży związanym z dysfunkcją śródbłonka naczyniowe-go, które występuje po 20. tygodniu ciąży.
Cel pracy. Porównanie stężenia krążących w organizmie matki mediatorów zaburzeń śródbłonka, w tym działania naczyniowego adrenomeduliny (AM) i peptydu związanego z genem kalcytoniny (CGRP), czynnika angiogennego rozpuszczalnego międzykomórkowego czynnika adhezyjnego-1 (ICAM-1) i czynnika aktywności prooksydacyjnej homocysteiny całkowitej (tHcy) w osoczu w ciążach prawidłowych i powikłanych stanem przedrzucawkowym. Ponadto zbadano, czy leczenie siarczanem magnezu wpływa na stężenie tych czterech krążących cząsteczek, zapo-biegając w ten sposób stanowi przedrzucawkowemu.
Adv Clin Exp Med 2012, 21, 5, 573–579 ISSN 1899–5276
oRIGINAL PAPERS
Materiał i metody. Łącznie 85 ciężarnych kobiet wzięło udział w badaniu, w tym 30 zdrowych ciężarnych, 15 z nad-ciśnieniem indukowanym ciążą (PIH) i 40 ze stanem przedrzucawkowym (PE). Stężenie matczynych AM, CGRP, sICAM-1 i tHcy w osoczu u matek oznaczano za pomocą enzymatycznego testu immunologicznego (ELISA). Ponadto oceniono wpływ leczenia siarczanem magnezu na stężenie tych czterech krążących cząsteczek.
Wyniki. W porównaniu ze zdrowymi ciężarnymi, stężenie krążących PM, sICAM-1 i tHcy było znacznie większe, a stężenie CGRP w osoczu było znacznie mniejsze u kobiet ciężarnych z nadciśnieniem tętniczym lub stanem przedrzucawkowym (P < 0,05). Leczenie siarczanem magnezu może skutecznie zmniejszyć stężenie AM, sICAM-1 i tHcy, jednocześnie zwiększając stężenie CGRP w krwiobiegu matek (P < 0,05).
Wnioski. Przedstawione wyniki wskazują, że AM, CGRP, sICAM-1 i tHcy mogą mieć wpływ na rozwój i utrzy-manie nadciśnienia w ciąży. Siarczan magnezu może hamować rozwój stanu przedrzucawkowego przez modulację tych czterech mediatorów (Adv Clin Exp Med 2012, 21, 5, 573–579).
Słowa kluczowe: adrenomedulina, peptyd związanego z genem kalcytoniny, rozpuszczalny międzykomórkowy czynnik adhezyjny-1, homocysteina całkowita, stan przedrzucawkowy, leczenie siarczanem magnezu.
Hypertensive disorders of pregnancy, known as pre-eclampsia (PE), are high blood pressure disorders of pregnancy that frequently develop af-ter 20 weeks of gestation [1]. This disorder could affects 5–8% of all pregnancies and has long been one of the major problems in pregnancy [1, 2]. Despite intensive research efforts, the etiology and pathogenesis of pre-eclampsia is still not complete-ly understood. Increasing evidence suggests that vascular endothelial dysfunction might be the un-derlying cause of the disease. Some studies suggest that regulation of multiple signaling pathways may contribute to the endothelial dysfunction, which in turn leads to the progression and etiopathogenesis of pre-eclampsia [1, 2].
The vascular actions of calcitonin gene-relat-ed peptide (CGRP) and the structurally relatgene-relat-ed peptide adrenomedullin (AM) both belong to the CGRPsuperfamily. Experimental and clinical studies indicate that plasma levels of adiponectin and CGRP are associated with vascular-related diseases [3]. Soluble forms of intracellular ad-hesion molecule-1 (sICAM-1) may be released into the circulation during inflammation, thus increased plasma level may indicate endothelial dysfunction [4, 5]. Hyperhomocysteinemia is an independent risk factor for cardiovascular dis-eases and plasma total homocysteine (tHcy) has been proven to play an important role in promot-ing endothelial dysfunction [6–8]. Several studies have suggested that these four molecules are me-diators of endothelial dysfunction, thus the ma-ternal plasma levels of these factors may change in pregnant women with pre-eclampsia. [3, 4, 6]. However, a causative relationship between the plasma levels of these four molecules has not been demonstrated yet.
Magnesium sulfate is the anticonvulsant of choice for treating pre-eclampsia. In some cases, women with pre-eclampsia can be stabilized tem-porarily with magnesium sulfate intravenously to forestall seizures. The use of magnesium sulfate as a possible treatment was first reported in 1955. It
wasn’t until the late 70s that magnesium sulfate re-placed diazepam or phenytoin in clinics in the UK. These days, more and more studies indicate that magnesium sulfate therapy does help prevent the progress of pre-eclampsia [9–11].
In this study, the authors compared the circu-lating levels of AM, CGRP, sICAM-1 and tHcy in healthy pregnancies and those with hypertension or pre-eclampsia. The authors tried to investigate whether these four molecules were involved in the clinical characteristics of pre-eclampsia. Further-more, they also studied the effects of magnesium sulfate therapy on the plasma levels of these me-diators.
Material and Methods
Study Subjects
Administration of
Magnesium Sulfate
The loading dose was 4 g i.v. over 20 min and then the maintenance dose continued at 1 g/h for at least 24 h after delivery. Magnesium sulfate therapy was aggressively monitored with urinary output (> 120 ml in 4 h), deep tendon reflexes and serum magnesium levels. Magnesium sul-fate toxicity was indicated by loss of reflexes and drowsiness, poor urine output and high serum magnesium levels and treatment used included an antidote in the form of an infusion of 10 ml of 10% calcium gluconate; in addition, magnesium sulfate infusion would be stopped for 1–2 h.
Blood Sampling
Peripheral venous blood samples were collected in sterile tubes containing ethylenediamine-tetraa-cetic acid (EDTA). No drugs were taken by these patients for 24 h before the blood sampling. The blood collected in EDTA was immediately stored at 4℃ and further processed within 48 h. Samples were centrifuged at 800 g for 15 min and the supernatant was stored in 200 μL aliquots at –80°C.
Measurement of AM, CGRP,
sICAM-1 and tHcy
Plasma concentration of endothelial dysfunc-tion mediators including AM, CGRP sICAM-1 and
tHcy were measured using commercially available ELISA kits (R&D Systems, Heidelberg, Germany) according to the manufacturer’s instructions. All experiments were performed by an investigator blinded to the study group assignment. Samples were checked by serial dilution and measurements were performed at least in duplicate.
Statistical Analysis
Analysis of the data was performed using the Statistical Package for the Social Sciences for Windows version 15.0 (SPSS, Chicago, IL). The data is presented as mean ± SD. Differences between variables were compared using the Stu-dent’s t-test, and differences in proportions were compared using Fisher’s exact test as appropri-ate. A P-value less than 0.05 was considered to be significant.
Results
Patient Characteristics
The clinical characteristics of participants in the study are described in Table 1. There were no significant differences observed in demographic features (including maternal age, BMI and gesta-tional age at sampling) among the study groups (P > 0.05). Gestational age at delivery were sig-nificantly earlier and birth weights were signifi-cantly lower in the PIH and PE group than those
Table 1. Clinical characteristics of subjects
Tabela 1. Kliniczna charakterystyka pacjentek
Characteristics HC (n = 30) PIH (n = 15) PE
mild (n = 18) severe (n = 22) Age (year) 27.4 ± 4.3 28.5 ± 2.6 29.8 ± 3.5 27.8 ± 2.2 BMI (kg/m2) 28.6 ± 3.3 27.7 ± 1.6 28.4 ± 2.3 28.0 ± 2.5
Gestational age at sampling (week) 28.3 ± 2.4 27.6 ± 2.0 28.8 ± 2.1 28.1 ± 1.2 Gestational age at delivery (week) 39.2 ± 1.7 36.6 ± 1.3* 35.1 ± 1.4* 36.3 ± 2.1** Birth weight (g) 3163.5 ± 268.2 3011.1 ± 320.1* 2357.2 ± 210.3** 2218.0 ± 306.1**
Proteinuria (mg/dL) trace trace ≥ 30 ≥ 30
Systolic blood pressure (mm Hg) 105.1 ± 10.1 132.5 ± 6.8** 154.7 ± 6.1** 165.2 ± 10.1** Diastolic blood pressure (mm Hg) 62.7 ± 8.3 85.0 ± 4.5** 97.2 ± 5.8** 105.3 ± 7.2** All parameters are given as mean ± SD. The statistical analysis (P-values) between patients and healthy controls are shown. *P < 0.05; ** P < 0.01.
in the healthy control group (P < 0.05). There is no significant difference of gestational age at de-livery between newborns of patients with preg-nancy-induced hypertension and pre-eclampsia (P > 0.05), but the birth weight in the PE patients group was significant lower than the PIH group (p < 0.05). Systolic and diastolic levels were signifi-cantly increased as: severe PE>mild PE>PIH>HC (P < 0.01).
Plasma Levels of Endothelial
Dysfunction Mediators
The plasma levels of endothelial dysfunction mediators, including AM, CGRP, sICAM-1 and tHcy, in different groups are shown in Table 2. Plasma levels of the vascular actions of AM and CGRP were significantly different in PIH and PE pregnancies when compared with the healthy group. In general, the concentration of AM was much higher (P < 0.01), while CGRP was much lower in pre-eclampsia (P < 0.05). The plasma concentration of the angiogenic factor of sICAM-1 and the pro-oxidant activity factor of tHcy is found in such order as PE>PIH>Control (P < 0.05). Fur-thermore, plasma AM, CGRP, sICAM-1 and tHcy levels of severe PE pregnancies are significantly different than those in the mild PE group.
Effects of MgSO
4Treatment
on Endothelial Dysfunction
Mediators
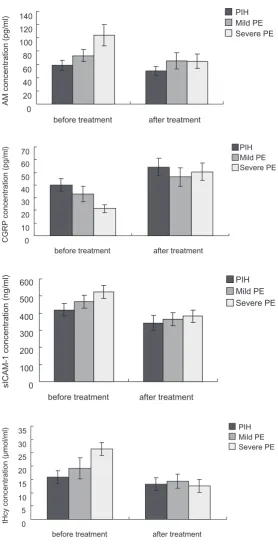
The effects of magnesium sulfate treatment on women with hypertension or pre-eclampsia were evaluated. The Student’s t-test was used to
com-pare the difference between data before and after treatment. The authors found that this therapy could help to control the development of PE, es-pecially elevated blood pressure and proteinuria. The plasma AM, CGRP, sICAM-1 and tHcy levels of pregnant patients before and after MgSo4 treat-ment were compared in Figure 1 (A-D). overall, the effects of MgSo4 treatment in the PIH and mild PE pregnancies groups are not significant. Among the four mediators, only sICAM-1 was significantly decreased after treatment in the mild PE group (P < 0.05). However, MgSo4 treatment showed significant effects in the severe PE group. The levels of vasodilator AM, sICAM-1 and tHcy were significantly lower after the treatment, while CGRP level was elevated (P < 0.01). Although Mg-So4 treatment did not regulate these mediators to their normal levels in the healthy pregnancy group, it still helped to inhibit the progress of pre-eclamp-sia by modulating these important mediators.
Discussion
Pre-eclampsia is a severe maternal condition that could lead to high risk of fetal growth retarda-tion, premature delivery and even maternal death [1, 2, 12]. Despite the unexplained pathogenesis, pre-eclampsia is thought to result from general-ized endothelial dysfunction. The plasma con-centration of vascular actions including AM and CGRP, the angiogenic factor of sICAM-1 and the pro-oxidant activity factor of tHcy are mediators of endothelial dysfunction and they have all been proven to play important roles in pre-eclampsia. In this study, the authors measured the levels of these four markers in the plasma of normal and pre-eclampsia pregnancies and the alteration of them before and after magnesium sulfate therapy
Table 2. Plasma levels of endothelial dysfunction mediators in healthy pregnant women, PIH and PE pregnancies
Tabela 2. Stężenie mediatorów zaburzeń śródbłonka w osoczu zdrowych ciężarnych, ciężarnych z nadciśnieniem tętniczym
i ze stanem przedrzucawkowym
Factors HC (n = 30) PIH (n = 15) PE
mild (n = 18) severe (n = 22) AM (pg/ml) 43.8 ± 6.12 58.3 ± 7.62* 73.23 ± 9.06** 104.3 ± 16.25** CGRP (pg/ml) 57.1 ± 9.42 39.9 ± 5.25* 32.84 ± 6.25* 21.5 ± 3.01* sICAM-1(ng/ml) 333.1 ± 42.53 419.6 ± 35.37** 466.8 ± 39.36** 524.6 ± 37.36** tHcy (μmol/l) 10.3 ± 2.60 15.9 ± 2.46* 19.1 ± 3.98* 26.4 ± 2.33*
Data is given as mean ± SD. The statistical analysis (P-values) between patients and healthy controls are shown. *P < 0.05; **
P < 0.01.
in patients with pre-eclampsia to explore their role in the pathogenesis of pre-eclampsia.
Endothelial dysfunction mediators, includ-ing AM, CGRP, sICAM-1 and tHcy, were previ-ously reported to participate in the pathogenesis of preeclampsia, but their mechanism is not yet completely understood. Some studies had found that the expression level of AM is lower in pre-eclampsia pregnancies compared to healthy preg-nancies [13–16]. However, more studies have indicated that there is no difference of AM level between preeclamptic and normotensive pregnant
women [17]. CGRP is a potent vasodilatory pep-tide which increases in both maternal and fetal circulation during late pregnancy. A low level of circulating CGRP was found to increase periph-eral resistance and blood pressure, thus it may be important in the pathogenesis of pre-eclampsia [18, 19]. ICAM-1 is involved in both adhesions of leukocytes to the endothelium and leukocyte mi-gration. The soluble form of ICAM-1 (sICAM-1) is present in plasma and functions as a regulatory molecule in ICAM-1/2-integrin interactions [20, 21]. tHcy measured in plasma is a marker of
EHIRUHWUHDWPHQW DIWHUWUHDWPHQW
$0FRQFHQWUDWLRQSJPO
3,+
0LOG3( 6HYHUH3(
EHIRUHWUHDWPHQW DIWHUWUHDWPHQW
&*53FRQFHQWUDWLRQSJPO
3,+
0LOG3( 6HYHUH3(
EHIRUHWUHDWPHQW DIWHUWUHDWPHQW
V,&$0FRQFHQWUDWLRQQJPO
3,+
0LOG3( 6HYHUH3(
EHIRUHWUHDWPHQW DIWHUWUHDWPHQW
W+F\FRQFHQWUDWLRQ˩PROPO
3,+
0LOG3( 6HYHUH3(
Fig. 1. Plasma levels of endothelial dys-function mediators before and after treat-ment
late status and cardiovascular disease. Increased tHcy has also been reported to be associatedwith placental-mediated adverse pregnancy outcomes. High tHcy in early pregnancy has been found to induce pregnancy loss and pre-eclampsia [7, 8], and it has been proposed that an increased circu-lating tHcy concentration could result in dysfunc-tionof the placental vasculature. Present results showed that plasma levels of the vascular actions of AM and CGRP were significantly different in PIH and PE pregnancies when compared to the healthy group. In general, the concentration of AM was much higher, while CGRP was much lower in pre-eclampsia (P < 0.05). The plasma concentration of the angiogenic factor of sICAM-1 and pro-oxidant activity factor of tHcy are found in such order as PE > PIH > Control (P < 0.05). Furthermore, the plasma AM, CGRP, sICAM-1 and tHcy levels of severe PE pregnancies are significantly different than those in the mild PE group (P < 0.05).
For a long time, magnesium sulfate has been used as a prophylactic anticonvulsive treatment in PE. Although several studies have demonstrated that MgSo4 might be involved in blood pressure regulation, the underlying mechanism is still not well understood [22, 23]. Since it has been shown that MgSo4 treatment is associated with changes in the circulating levels of blood pressure regula-tors, the authors were interested to investigate the effects of MgSo4 on plasma AM, CGRP, sICAM-1 and tHcy levels. Present studies showed that the effects of MgSo4 treatment in the PIH and mild
PE pregnancies groups are not significant. Among the four mediators, only sICAM-1 was significant-ly decreased after treatment in the mild PE group. However, MgSo4 treatment showed significant ef-fects in the severe PE group. The levels of vaso-dilator AM, sICAM-1 and tHcy were significantly lower after the treatment, while CGRP level was elevated (P < 0.01). Although MgSo4 treatment did not regulate these mediators to their normal levels in the healthy pregnancy group, it still helps to inhibit the progress of pre-eclampsia by regulat-ing these important mediators.
In summary, the authors determined the plasma concentrations of AM, CGRP, sICAM-1 and tHcy in normal pregnancies and pre-eclampsia. AM, sI-CAM-1 and tHcy levels are elevated in severe pre-eclampsia compared to normal pregnancies, while CGRP level was negatively associated with pre-ec-lampsia. Pre-eclampsia is an endothelial dysfunc-tion that begins under the endocrine and rheologic stress of pregnancy and may continue thereafter. Present study showed that the plasma concentra-tion of these four molecules will be useful in pre-dicting the severity of pre-eclampsia. Combined measurements of these four molecules will greatly improve the sensitivity and reduce false positives in early detection of pre-eclampsia. The authors hope that these new markers will improve diagnosis of pre-eclampsia, thereby enabling them to identify women at high risk of developing pre-eclampsia at an early stage of pregnancy, thereby preventing dangerous, life-threatening complications.
Acknowledgments
The authors wish to thank all of the volunteers and consultant obstetricians.
Reference
[1] Williams D: Long-term complications of pre-eclampsia. Semin Nephrol 2011, 31(1), 111–22.
[2] Young BC, Levine RJ, Karumanchi SA: Pathogenesis of pre-eclampsia. Ann Rev Pathol 2010, 5,173–192.
[3] Knerr I, Dachert C, Beinder E et al.: Adrenomedullin, calcitonin gene-related peptide and their receptors: evi-dence for a decreased placental mRNA content in pre-eclampsia and HELLP syndrome. Eur J obstet Gynecol Reprod Biol 2002, 101(1), 47–53.
[4] Freeman DJ, McManus F, Brown EA et al.: Short- and long-term changes in plasma inflammatory markers asso-ciated with pre-eclampsia. Hypertension 2004, 44(5), 708–714.
[5] Daniel Y, Kupferminc MJ, Baram A, Geva E, Fait G, Lessing JB: A selective increase in plasma soluble vascular cell adhesion molecule-1 levels in pre-eclampsia. Am J Reprod Immunol 1999, 41(6), 407–412.
[6] Hasanzadeh M, Ayatollahi H, Farzadnia M, Ayati S, Khoob MK: Elevated plasma total homocysteine in pre-eclampsia. Saudi Med J 2008, 29(6), 875–878.
[7] Ingec M, Borekci B, Kadanali S: Elevated plasma homocysteine concentrations in severe pre-eclampsia and eclampsia. Tohoku J Exp Med 2005, 206(3), 225–231.
[8] Herrmann W, Isber S, Obeid R, Herrmann M, Jouma M: Concentrations of homocysteine, related metabolites and asymmetric dimethylarginine in preeclamptic women with poor nutritional status. Clin Chem Lab Med 2005, 43(10), 1139–1146.
[9] Pritchard JA: The use of the magnesium ion in the management of eclamptogenic toxemias. Surg Gynecol obstet 1955, 100 (2), 131–140.
[10] Hibbard BM, Rosen M: The management of severe pre-eclampsia and eclampsia. Br J Anaesth 1977, 49 (1), 3–9.
[12] Baviera G, D’Anna R, Corrado F, Ruello A, Buemi M, Jasonni VM: ICAM-1 in maternal plasma and amniotic fluid as an early marker of pre-eclampsia and IUGR. J Reprod Med 2002, 47(3), 191–193.
[13] Minegishi T, Nakamura M, Abe K et al.: Adrenomedullin and atrial natriuretic peptide concentrations in normal pregnancy and pre-eclampsia. Mol Hum Reprod 1999, 5(8), 767–770.
[14] Li H, Dakour J, Kaufman S, Guilbert LJ, Winkler-Lowen B, Morrish DW: Adrenomedullin is decreased in pre-eclampsia because of failed response to epidermal growth factor and impaired syncytialization. Hypertension 2003, 42(5), 895–900.
[15] Boc-Zalewska A, Seremak-Mrozikiewicz A, Barlik M, Kurzawinska G, Drews K: The possible role of adrenom-edullin in the etiology of gestational hypertension and pre-eclampsia. Ginekol Pol 2011, 82(3), 178–184.
[16] Dikensoy E, Balat O, Pence S, Balat A, Cekmen M, Yurekli M: The changes of plasma malondialdehyde, nitric oxide, and adrenomedullin levels in patients with pre-eclampsia. Hypertens Pregnancy 2009, 28(4), 383–389.
[17] Di Iorio R, Marinoni E, Letizia C, Alo P, Villaccio B, Cosmi EV: Adrenomedullin, a new vasoactive peptide, is increased in pre-eclampsia. Hypertension 1998, 32(4), 758–763.
[18] Ariza AC, Bobadilla N, Diaz L, Avila E, Larrea F, Halhali A: Placental gene expression of calcitonin gene-re-lated peptide and nitric oxide synthases in pre-eclampsia: effects of magnesium sulfate. Magnes Res 2009, 22(1), 44–49.
[19] Halhali A, Wimalawansa SJ, Berentsen V, Avila E, Thota CS, Larrea F: Calcitonin gene- and parathyroid hor-mone-related peptides in pre-eclampsia: effects of magnesium sulfate. obstet Gynecol 2001, 97(6), 893–897.
[20] Portelinha A, Belo L, Tejera E, Rebelo I: Adhesion molecules (VCAM-1 and ICAM-1) and C-reactive protein in women with history of pre-eclampsia. Acta obstet Gynecol Scand 2008, 87(9), 969–971.
[21] Kim SY, Ryu HM, Yang JH et al.: Maternal plasma levels of VCAM-1, ICAM-1 and E-selectin in pre-eclampsia. J Korean Med Sci 2004, 19(5), 688–692.
[22] Halhali A, Wimalawansa SJ, Berentsen V, Avila E, Thota CS, Larrea F: Calcitonin gene- and parathyroid hor-mone-related peptides in preeclampsia: effects of magnesium sulfate. obstet Gynecol 2001, 97(6), 893–897.
[23] Ariza AC, Bobadilla N, Fernández C, Muñoz-Fuentes RM, Larrea F, Halhali A: Effects of magnesium sulfate on lipid peroxidation and blood pressure regulators in preeclampsia. Clin Biochem 2005, 38(2), 128–133.
Address for correspondence:
Zhuge Hongxiang
Department of Pathogenic Microbiology Suzhou University
Dushu Lake Campus 199 Renai Road Suzhou
Jiangsu Province China
E-mail: [email protected]
Conflict of interest: None declared