ABSTRACT
Purpose
Evaluation of the results of radiotherapy in elderly patients with early laryngeal cancer, the relation between comorbidities and the overall treatment time, and the influence of treatment interruptions on the outcome of treatment.
MATeRiAlS And MeThodS
A clinical retrospective analysis of a group of 153 patients (≥70 years old) with laryngeal cancer stage I and II was carried out. Patients were irradiated between the years 1980 and 2005 in the Centre of Oncology in Cracow.
The analysed group consisted of 134 men (88%) and 19 women (12%). Patients’ age ranged from 70 to 87 years, median – 74 years. Most of them had various comorbidities. Three different irradiation techniques and fractionation schemes were used according to the site, stage and grade of cancer: two oblique beams including the larynx with total dose of 60 Gy in 24 fractions (67 patients), two opposed parallel Cobalt 60 beams including the larynx and cervical lymph nodes with total dose of 60 Gy in 30 fractions (50 patients), and mixed photon-electron unilateral beam including the larynx with total dose of 60 Gy in 30 fractions (36 patients).
ReSulTS
The median up was 52 months. During the follow-up period 105 patients (68.6%) died. Among them 31 patients (29,6%) died of laryngeal cancer, 13 (12,4%) patients of other malignancy, and 61 (58%) patients died of concomitant diseases without evidence of cancer.
The actuarial 5/10-year overall survival (OS), disease specific survival (DSS) and local control (LC) were 48%/21% and 79%/72% and 75%/71% respectively.
Is Radiotherapy for Early Laryngeal Cancer in
Elderly a Safe and Effective Treatment Method
Keywords: elderly, laryngeal cancer, radiotherapy
The overall tolerance of radiation therapy was good; only 6 patients had G3 early mucosal reaction, and 2 patient had G3 early skin reaction were observed. Comorbidities were not demonstrated to have statistically significant influence on DSS rate.
In 10 (6,5%) from 153 patients complete tumor regression was not achieved after radiotherapy. During the follow-up period loco-regional relapse were observed in 31 patients (19,6%), and distant metastases in 4 patients (2,6%).
ConCluSionS
Radiotherapy of the elderly patients with laryngeal cancer is effective and well tolerated method. Comorbidities do not significantly influence the treatment results. T stage, age over 73 years, fractionation dose under 2 Gy and overall treatment time over 43 days are statistically significant negative prognostic factor for DSS rate.
inTRoduCTion
nowadays increasing frequency of laryngeal cancer in elderly patients is noticed, mostly because of extending mean life span. The number of newly recorded laryngeal cancer in patients above 65 years in 2006 in Poland was 883 (806 males and 77 females). Between 1985 and 2005 in Poland the mortality rate for men with laryngeal cancer aged 65 years and more, increased from 38,2/100000 to 40/100000.1
The growing number of elderly patients creates problems concerning the optimal treatment, especially in the presence of coexisting diseases, i.e. medical and psychic disturbances with tendency towards depression. The oncological treatment may exacerbate these diseases which could make difficult administration of planned oncological therapy. Another question is: whether the oncological treatment evoking additional complaints (radiation-induced pain, necessity of submission to hospital regime, often necessity of taking increased amount of liquids and medicines) will have an impact on general-feeling, patient`s compliance and motivation. Cardiovascular diseases, such as ischaemic heart disease, arterial hypertension, circulatory insufficiency and chronic renal failure usually connected with acid-base balance and electrolyte disorders are often seen in the elderly. Chronic obstructive pulmonary disease is very often associated with laryngeal cancer, especially with regard to an etiology, i.e. long-lasting smoking.
in connection with side effects (radiation-induced skin reaction, mucositis, temporary or permanent xerostomy, electrolyte depletion secondary to increased salivation, taste impairment, hypodipsia) aggressive therapeutic management may lead to dehydration, weight loss, difficulties with taking so far administered medicines, and finally to destabilization of general condition.
Radiotherapy is a therapeutic method frequently used in treatment of early laryngeal cancer. The 5-year disease-free survival rates achieved with radiotherapy and possible salvage laryngectomy in early suppraglottic and glottic cancers were 70-90% and 75-99%, respectively.2,3,4,5,6,7,8,9,10
The aim of this paper is to evaluate irradiation results, the relation between comorbidities and the overall treatment time and the influence of treatment interruptions on the outcome of treatment in patients
≥70 years old with early laryngeal cancer.
MeThodS
A clinical retrospective analysis of a group of 153 patients (≥70 years old) with early laryngeal cancer was carried out. The 5-year and 10-year disease-specific survival (dSS) and local control (lC) rates were assumed as a criterion of treatment outcomes evaluation. in accordance with nCi definition, dSS was calculated from the date of treatment beginning until death due to laryngeal cancer, lC until the first symptoms of local relapse. The other causes of death were censored.11
Kaplan-Meier method was used for the 5-year and 10-year survival rates estimation. To analyse the statistic differences, log-rank test was applied. As a level of statistic significance, p < 0,05 was assumed. Statistic analyses were performed using computer program STATiSTiCA 7th version by StatSoft.
MATeRiAlS And MeThodS
Between 1st January, 1980 and 31st december, 2005 in the Centre of oncology in Krakow 153 patients with early laryngeal cancer ( stage i-ii according to TnM classification 200912) 70 and more years old were
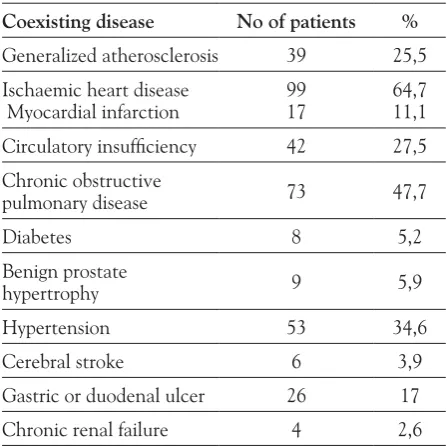
Table I. Comorbidities
Coexisting disease No of patients %
Generalized atherosclerosis 39 25,5 ischaemic heart disease
Myocardial infarction 9917 64,711,1 Circulatory insufficiency 42 27,5 Chronic obstructive
pulmonary disease 73 47,7
diabetes 8 5,2
Benign prostate
hypertrophy 9 5,9
hypertension 53 34,6
Cerebral stroke 6 3,9 Gastric or duodenal ulcer 26 17 Chronic renal failure 4 2,6
TReATMenT MeThodS
Three irradiation techniques were applied:7,10
1. Two oblique wedged Cobalt 60 beams, crossed at a right angle. irradiated volume included the larynx with a total dose of 60 Gy in 24 fractions. This technique was used in 67 patients (43,8%) with glottic cancer.
2. Two opposed lateral parallel wedged Cobalt 60 beams were applied in patients with supraglottic cancer, and in more advanced glottic cancer and in case of lower differentiated cancer. irradiated volume included the larynx along with the upper and middle cervical nodes. Total dose 60 Gy in 30 fractions was given. in these patients a boosted dose of 4-8 Gy to the reduced region, i.e. primary tumour with 1-2 cm tissue margin was administered with photon or electron. This irradiation technique was used in 50 patients (32,7%).
3. one mixed photon-electron lateral portal. The larynx alone was included into irradiated volume with a total surface dose 60 Gy in 30 fractions administered with photons and electrons half-and-half. Standard field size was 6 cm by 6 cm. This technique was used in 36 (23,5%) patients in poor medical condition, who were not able to bend the head backward.
Two patients received lower dose than planned because of radiation-induced reaction, in 2 patients irradiation was discontinued due to aggravation of ischaemic heart disease and circulatory insufficiency, in 1 patient the treatment was finished after 57,5 Gy, as he refused further treatment. Simultaneously to radiotherapy all patients were treated for their comorbidities. Sixty-four (42%) patients were irradiated without any interruption, remaining 89 patients had the interruptions ranging from 1 to 37 days (mean 3 days). The most frequent reason of irradiation interruption were holidays, machine failure and severe radiation-induced reaction. Comorbidities as a cause of interruption were observed in 5 patients: 1. exacerbation of ischaemic heart disease – 13 day gap, 2. exacerbation of depression – 5 day gap, 3. myocardial infarction – 37 day gap, 4. bleeding from duodenal ulcer – 14 day gap, 5. bronchitis and pneumonia – 5 day gap.
ReSulTS
1. Survival rates.
The mean patient observation, namely the time from the start of treatment until either death or the last clinic visit in our institute, was 58 months and the median observation time was 52 months. during the follow-up period 105 patients died (68,6%). laryngeal cancer was the reason of death in 31 patients (29,6%), second primary tumour in 13 patients (12,4%), while other diseases in 61 patients (58%) – among these patients 2 died in car crash, 1 of rupture of abdominal aortic
Figure 2 . local control probability
aneurysm, 1 of pulmonary embolism, 1 of cerebral stroke, 4 of circulatory insufficiency, 3 of myocardial infarction, 4 of coronary atherosclerosis and the rest of patients died of generalized atherosclerosis. Predicted the 5- and 10-years overall survival rates (generated on the basis of Kaplan-Meier method) in the analysed group of 153 patients irradiated were 48% and 21% respectively. Predicted the 5- and 10-years disease specific survival rates for laryngeal cancer (generated on the basis of Kaplan-Meier method) in the analysed group were 79% and 72% respectively. disease specific survival curve is presented at the Figure 1. Predicted the 5- and 10-years local control rates after radiotherapy alone were 75% and 71%, and after salvage surgery were 79,5% and 74% respectively. local control curve is presented at the Figure 2.
2. local treatment tolerance.
Acute radiation-induced skin reaction (valued according to RToG scale11) was noticed in 135 patients:
107 patients (79,2%) had G1, 26 patients (19,3%) had G2, 2 patient (1,5%) had G3 reaction. it was not observed in 18 patients. Acute radiation-induced mucosal reaction within the pharynx and the larynx was described in 134 patients: 84 patients (54,9%) had G1, 44 patients (28,8%) had G2, 6 patients (3,9%) had G3 reaction. The remaining 19 patients (12,4%) did not have any complaints about mucositis. The late effects of radiation were observed in 43 patients: G1- 32 patients (20,9%), G2 - 10 patients (6,5%), G3 - 1 patient (0,6%). in the last three cases there was a necessity of temporary tracheostomy.
Table III. Clinical, population and therapeutic factors and local control.
Factor Category no of patients
lC 5-years
% 10-years
% p
T 1
2 7578 8970 8566 0,00409 Primary
tumour supraglotticglottic 11934 6484 6477 0,10317 Age ≤ 73 years
> 73 years 75
78 8475 7772 0.22099 Fraction
dose > 200 cGy≤ 200 cGy 6687 8873 8864 0,03920 overall
treatment time
< 43
≥ 43 8073 8574 8563 0,16730
lC - local control
Factor Category no of patients
dSS
5-years %
10-years
% p
T 1
2 7578 9176 8262 0,01073
Primary
tumour supraglotticglottic 11934 7283 6276 0,10346 Age ≤ 73 years
> 73 years 7578 8977 7571 0,03613 Fraction
dose > 200 cGy≤ 200 cGy 6687 8773 8265 0,01574 overall
treatment time
< 43
≥ 43 8073 8474 8064 0,01972
dSS - disease specific survival
3. The results of prognostic factors analysis are shown in the Table ii and iii.
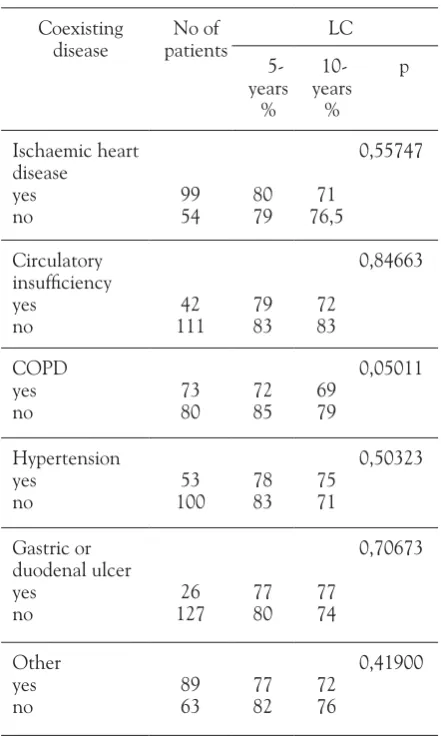
Statistically significant negative prognostic factors for disease-specific survival rates were: stage T2, age over 73 years, fraction dose 2 Gy or less, and overall treatment time 43 days or longer. Statistically significant negative prognostic factors for local control rates were: stage T2, and fraction dose 2 Gy or less. The results of comorbidities` influence on dSS and lC are shown in the Table iV and V. The comorbidities did not show any significant influence on dSS and lC.
4. Treatment failures.
in the group of 153 patients irradiated with curative intention, complete response was not achieved in 10 patients (6,5%). These patients were treated with salvage total laryngectomy. during the follow-up the locoregional failure was seen in 31 patients (19,6%), distant metastases (the bones, the lungs) in 4 patients (2,6%), second primary tumour in 21 patients (13,7%). From among 31 patients with locoregional failure, in 28 patients (18,3%) failure within larynx was confirmed and in 3 patients (2%) in regional lymph nodes. only one patient was operated on, as other patients were not fit enough for surgery. in the group of patients with the second primary tumour diagnosis, 12 were localised in the lungs, 4 in the digestive tract, 3 in the genitourinary system, and 2 on the skin.
Table IV. Comorbidities and disease-specific survival.
Coexisting disease no of
patients dSS 5-
years %
10-years
%
p
ischaemic heart disease
yes
no 9954 8476 7666
0,41925
Circulatory insufficiency yes
no 11142 8279 7372
0,96370
CoPd yes
no 7380 7885 6083
0,13423
hypertension yes
no 10053 7981 7471
0,37286
Gastric or duodenal ulcer yes
no 12726 7380 7372
0,94911
other yes
no 8963 7880 7367
0,84576
dSS - disease specific survival
CoPd - chronic obstructive pulmonary disease
Table V. Comorbidities and local control.
Coexisting
disease patientsno of lC 5- years %
10-years
%
p
ischaemic heart disease
yes
no 9954 8079 76,571
0,55747
Circulatory insufficiency yes
no 11142 7983 7283
0,84663
CoPd yes
no 7380 7285 6979
0,05011
hypertension yes
no 10053 7883 7571
0,50323
Gastric or duodenal ulcer yes
no 12726 7780 7774
0,70673
other yes
no 8963 7782 7276
diSCuSSion
There are a lot of publications concerning the laryngeal cancer management in elderly patients. Geinitz et al.13
believe that definitive treatment, even in patients over 85 years with expected survival of more than 4 years is justified, because cure and disease-specific survival rates are comparable to those observed in the younger patients. The authors point out the biological and molecular data which could indicate increase of ionizing radiation sensitivity in the elderly due to decreased ability to repair dnA damage. however there are insufficient experimental data, and lack of retrospective studies showing lower radiotherapy tolerance in older patients. According to Geinitz et al.13 more intense
irradiation-induced mucositis and weight loss are seen in older patients, whereas in the group of younger patients irradiation-induced dermatitis and nausea are more pronounced. Thus, they recommend careful monitoring for appropriate fluid intake and electrolyte serum level during the course of radiotherapy. The authors take into consideration performation status of patients and comorbidities as the factors influencing radiotherapy qualification. They do not see the neccessity of dose reduction because of advanced age and conclude that age itself does not constitute a contraindication for radiotherapy.
Schofield et al.14 treated by definitive radiotherapy 50
patients aged 80 with laryngeal cancer. The obtained 5-year rates for local control and cancer specific survival were 86% and 79%, respectively. in our own material (patients aged 70 and more) cancer specific survival rate at 5 and 10 years were 79% and 72%, while local control rates at 5 and 10 years were 79% and 74%, respectively. Bhattacharyya15 extracted data of patients with head
and neck cancers treated by definitive radiotherapy from the Surveillance, epidemiology and end Results (SeeR) database and segregated them into two age groups. he noticed significantly worse results with regard to mean overall survival in patients with glottic cancer aged ≥
70 years (73,9 months vs 96,7 months in the younger group). Similarly, significant differences in cancer-specific survival were observed (105,9 months vs 114,1 months in the younger group). however, after stage stratification older patients did not show any statistically significant poorer overall or cancer-specific survivals comparing to younger group. The author conclude that elderly patients with head and neck squamous cell carcinoma not always exhibit poorer survival results. From this it follows that age alone should not be used in choice of treatment options. Małecki16 determined the
age of 57 years and below as a unfavourable prognostic factor for patients with squamous cell carcinoma of the oral cavity, oropharynx, hypopharynx and larynx treated with induction chemotherapy followed by radiotherapy. de Andres et al.17 did not affirm any correlation
between general state, primary tumour location, age and gender in patients with head and neck cancer. levin et al.18 did not show any statistically significant difference
between the treatment results of patients with head and neck cancer below and over 57 years old with Karnofsky Performance Status >60%.
in our own material patients` age over 73 years was connected with statistically significant poorer prognosis. Sarini et al.19 assessed treatment results in patients
with head and neck cancers comparing two cohorts:
≥ 75 years old patients versus the younger ones. They did not notice any statistically significant differences in stage, comorbidities and treatment tolerance between both groups. in elderly patients late local failures and metachronous malignancies were rarely observed. According to these authors it was due to the shorter lifespan of these patients. Garman et al.20 underlined
the influence comorbidities on the general condition of 376 oncological patients aged over 64 years. They conclude that the older cancer survivors had impaired general condition more often due to comorbidities than to malignant disease per se. in the study by Vercelli et al.21 treatment results in elderly cancer patients from
17 european countries were analysed. They noticed a survival disadvantage in the elderly, particularly 1 year after diagnosis, and in the females. Also poorer survival rates in the elderly were observed in patients from eastern european countries. Many researchers report on better outcomes achieved for glottic cancer comparing to supraglottic cancer.2,5,6,9,10,22,23 The dependence
between treatment results and the stage of disease is obvious – this was confirmed in our material as well. in the analysed group of patients the fraction dose was an independent prognostic factor affecting specific survival (dose per fraction > 200 cGy : p= 0,02477). Kim et al. [24] show local control improvement from 79% to 96%, when the higher fractional dose administered for patients with early glottic cancer. other authors noticed better treatment outcomes in connection with higher fraction dose (225-250 cGy).24,25 The problem
often discussed in the literature is influence of overall treatment time and the role of treatment breaks on the final outcome.26 n our group statistically significant
Cancer,2006 ;5: 257-266.
8. Sas–Korczynska B. Analiza przyczyn niepowodzen leczenia u chorych na raka krtani po całkowitym wycieciu krtani i pooperacyjnej radioterapii. nowotwory 1998; 48: 643-662. 9. Silver Ce. laryngeal cancer. Thieme Medical Publishers, new York
1991.
10. Skolyszewski J, Reinfuss M, Kowalska T. Results of radiation therapy in carcinoma of the larynx. Acta Radiologica oncology 1988; 23: 415-420.
11. national Cancer institute – dictionary of Cancer Terms; http:// www.cancer.gov/dictionary , accesed 19.01.2011.
12. Sobin lh, Gospodarowicz M, Wittekind Ch. in: TnM Classification of Malignant tumours 7e. Wiley Publication, new York 2009. 13. Geinitz h, Zimmermann FB, Molls M. Radiotherapy of the elderly
patient. Radiotherapy tolerance and results in older patients. Strahlenther onkol. 1999; 175 (3): 119-27.
14. Schofield CP, Sykes AJ, Slevin n, Rashid nZZ. Radiotherapy for head and cancer in elderly patients. Radiotherapy oncol 69 (2003) 37-42.
15. Bhattacharyya n. A matched survival analysis for squamous cell carcinoma of the head and neck in the elderly. laryngoscope. 2003; 113 (2): 368-72.
16. Malecki K. ocena klinicznych, histologicznych i molekularnych czynnikow rokowniczych i predykcyjnych u chorych na plłaskonablonkowego raka jamy ustnej, ustnej i krtaniowej czesci gardła oraz krtani napromienianych po indukcyjnej chemioterapii. CooK, Kraków. doctoral thesis 2004.
17. de Andres l, Brunet J, lopez-Pousa A. et al. Randomized trial of neoadjuvant cisplatin and fluorouracil versus carboplatin and fluorouracil in patiets with stage iV – M0 head and neck cancer. J Clin onkol 1995; 13 (6): 1493-500.
18. lewin F, damber l, Jasson h et al. neoadjuvant chemotherapy with cisplatin and 5-fluorouracil in advanced squamous cell carcinoma of the head and neck: a randomized phase iii study. Radioth onkol 1997; 43(1): 23-8.
19. Sarini J, Fournier C, lefebvre Jl, Bonafos G et al. head and neck squamous cell carcinoma in elderly patients: a long-term retrospective review of 273 cases. Arch otolaryngol head neck Surg 2001; 127 (9): 1089-92.
20. Garman KS, Pieper CF, Seo P, Cohen hJ. Function in elderly cancer survivors depends on comorbidities. J Gerontol A Biol Sci Med Sci 2003; 58 (12): M1119-24.
21. Vercelli M, Quaglia A, Casella C, Parodi S et al. Relative survival in elderly patients in europe. eur J Cancer 1998; 34 (14) 2264-2270. 22. Fu KK. The endolarynx and hypopharynx. in: Cox Jd. Moss'
radiation oncology – rationale, technique, results. Mosby 1994. 23. hope – Stone hF. Radiotherapy in clinical practice. Butterworths
1986.
24. Kim RY, Marks Me, Salter MM. early – stage glottic cancer: importance of dose fractionation in radiation therapy. Radiology 1992; 182 (1): 273 – 275.
25. Perez CA, Brady lW. halperin eC. Principles and Practice of Radiation oncology. Fifth edition. in: JB lippincott Williams & WilkinsCompany. Philadelphia 2008.
26. Skladowski K, Tarnawski R, Maciejewski B, Wygoda A, Slosarek K. Clinical radiobiology of glottic T1 squamous cell carcinoma. int J Radiot oncol Biol Phys 1999; 43 (1): 101-106.
location, dose, overall treatment time patients aged ≥
70 years appeared to be similar to those observed in the younger patients.
The appropriate comorbidities management in elderly patients is essential for oncological treatment. Possession of this ability is necessary in order to prevent irradiation breaks caused by chronic diseases exacerbation. To obtain this aim, radiation oncologist should be acquainted with internal medicine. equally vital for optimal cancer patient management is proper cooperation with other specialists and general practitioner as well.
ConCluSionS
1. Radiotherapy of elderly patients (≥ 70 years old) with early laryngeal cancer is effective and well tolerated. An appropriate management of comorbidities enables satisfying results of cancer treatment. 2. identified unfavourable prognostic factors are: stage,
age ≥ 73 years, fraction dose equal or lower than 200 cGy, and overall treatment time longer than 43 days.
ReFeRenCeS
1. Wojciechowska u, didkowska J, Zatonski W.nowotwory złosliwe w Polsce w 2006 roku. Centrum onkologii,Warszawa 2008. 2. Betkowski A, Szuber K, Wiewiorska T et al. Wyniki leczenia raka
krtani napromienianiem metoda konwencjonalna. otolaryngol Pol 1990; 44:35-38.
3. Cellai e, Frata P, Magrini SM et al. Radical radiotherapy for early glottic cancer: results in a series of 1087 patients from two italian radiation oncology centers. i. The case of T1n0 disease. int J Radiation oncology Biol. Phys.2005; 63 (5): 1378-1386. 4. Frata P, Cellai e, Magrini SM et al. Radical radiotherapy for early
glottic cancer: results in a series of 1087 patients from two italian radiation oncology centers. ii. The case of T2n0 disease. int J Radiation oncology Biol. Phys.2005; 63 (5): 1387-1394. 5. Million RR, Cassini nJ, Mancuso AA. larynx. in: Million
RR, Cassini nJ. Management of head and neck cancer: a multidisciplinary approach. J.B. lippincot Company, Philadelphia 1994.
6. overgaard J, hansen hS, Jorgensen K, hansen Mh. Primary radiotherapy of larynx and pharynx carcinoma – an analysis of some factors influencing local control and survival. int J Radiat oncol Biol Phys 1986; 12: 515-521.