Secular Changes in Sleep Position During Infancy: 1995–1998
Michael J. Corwin, MD*; Samuel M. Lesko, MD, MPH*‡; Timothy Heeren, PhD*;
Richard M. Vezina, MPH‡; Carl E. Hunt, MD§; Frederick Mandell, MD储; Mary McClain, RN*储; and Allen A. Mitchell, MD*‡
ABSTRACT. Objective. Prone sleeping among infants
has been associated with an increased risk of sudden infant death syndrome. The objective of this study was to compare factors associated with sleep position in 1995– 1996 and 1997–1998 and to assess secular trends in use of prone infant sleep position from 1995 through 1998 among families stratified by race and education.
Methods. A prospective cohort study was conducted in eastern Massachusetts and northwest Ohio of 12 029
mothers of infants who weighed >2500 g at birth.
De-scriptive statistics and multivariate odds ratios were used to relate maternal and infant characteristics to prone and supine sleeping.
Results. A total of 14 206 mothers (25% of those eli-gible) were enrolled. A total of 12 029 mothers (85% of enrolled) responded to the 1-month and 11 552 mothers (81% of enrolled) responded to the 3-month follow-up questionnaire. A decline in use of the prone sleep posi-tion and increase in use of the supine posiposi-tion was ob-served during the 4 years of the study. Factors associated with prone and supine sleep position were similar in 1995–1996 and 1997–1998. In 1997–1998, use of prone
sleeping at 1 month of age reached the goal of<10% only
among infants of white and Asian women, married women, women who were older than 25 years, women who were college graduates, and women with incomes >$55 000 per year. At 3 months of age, however, prone sleeping increased to 12% to 17% in these groups. These same groups were most likely to use the supine position; 38% to 45% were supine at 1 month, increasing to 56% to 64% by 3 months of age. However, as of the end of 1998, approximately 27% of infants of non– college-educated black and Hispanic mothers were placed to sleep in the prone position and only 20% to 30% were being placed to sleep in the supine position at 3 months of age.
Conclusions. Recommendations to avoid prone sleep position and especially the recommendation that supine
sleep position is preferred have not been effectively de-livered to black and Hispanic families and to families of
low-income and less than a college education.Pediatrics
2003;111:52– 60;infant sleep position, sudden infant death
syndrome, Back to Sleep, racial disparities.
ABBREVIATION. SIDS, sudden infant death syndrome.
S
udden infant death syndrome (SIDS) is defined as the sudden death of an infant not expected by history and unexplained by a thorough post-mortem examination, which includes a complete au-topsy, death scene investigation, and medical history review. In the United States, SIDS continues to be the most common cause of death for infants between 1 and 12 months of age, despite falling from a rate of 1.2 per 1000 live births in 1992 to 0.72 cases per 1000 live births in 1998.1The cause of SIDS is unknown, but a number of factors have been associated with an increased risk. Incidence is higher among blacks than whites, is inversely proportional to birth weight, is increased by maternal illicit drug use and smoking during pregnancy, and may be decreased by breast-feeding.2 A number of studies have shown that in-fants who sleep prone (lying on their stomach) are at increased risk3–5and that infants who sleep supine are at lower risk than those who sleep on their side.6,7 After successful campaigns to reduce the prevalence of prone sleeping, SIDS rates have decreased sub-stantially.8 –13In April 1992, the American Academy of Pediatrics recommended that healthy newborns be placed on their side or back to sleep, and in 1994, the Back to Sleep campaign was initiated in the United States by a joint statement of the American Academy of Pedi-atrics, several government agencies, and SIDS orga-nizations. In 1996, the recommendations were amended to emphasize supine sleep position as the preferred position. The goal of the Back to Sleep effort is to reduce the prevalence of prone sleeping among infants to 10% or less.14 Annual telephone surveys of households with infants younger than 8 months indicate that the average prevalence of prone sleeping in this age group decreased from 70% in 1992 to 17% in 1998 and that the prevalence of prone sleeping was higher among blacks and older in-fants.15 We have previously reported that in 1995 and 1996 nearly 30% of US infants slept prone at 3 months of age and that a substantial proportion of infants slept nonprone early but changed to prone by
From the *Departments of Pediatrics and Epidemiology and Biostatistics, Boston University Schools of Medicine and Public Health, Boston, Massa-chusetts; ‡Slone Epidemiology Unit, School of Public Health, Boston Uni-versity School of Medicine, Boston, Massachusetts; §Department of Pediat-rics, Medical College of Ohio, Toledo, Ohio; and储Massachusetts Center for Sudden Infant Death Syndrome, Boston, Massachusetts.
Dr Hunt is currently at the Center on Sleep Disorders Research, National Heart, Lung, and Blood Institute, National Institutes of Health, Bethesda, Maryland.
The content of this publication does not necessarily reflect the views or policies of the Department of Health and Human Services, and mention of trade names, commercial products, or organizations does not imply en-dorsement by the US government.
Received for publication Jan 9, 2002; accepted Jun 4, 2002.
Reprint requests to (M.J.C.) Department of Pediatrics, Boston Medical Cen-ter, One Boston Medical Center Pl, Boston, MA 02118. E-mail: mjcorwin@ bu.edu
3 months.16These reports and others have identified a number of characteristics associated with increased risk of prone sleep position, including maternal race and education. What is not clear from these reports, however, is whether characteristics associated with choice of sleep position have changed over time and how these factors are related to secular changes in infant sleep position. The purpose of the current report is to compare factors associated with sleep position in 1995–1996 and 1997–1998 and to assess secular trends in the use of prone infant sleep posi-tion from 1995 through 1998 among families accord-ing to race and education.
METHODS
The Infant Care Practices Study was a prospective longitudinal study conducted in Boston, Lowell, and Lawrence, Massachusetts, and Toledo, Ohio. The principal aims of the study were to describe current newborn sleep practices, to document changes in sleep position with age and calendar time, and to identify determinants and health consequences of various sleep practices among infants during the first 6 months of life. Between February 1995 and December 1998, mothers of newborn infants were contacted at selected birth hospitals in these cities and invited to participate. Each working day, study personnel reviewed the obstetrical records to identify women who delivered live infants during the previous 24 hours. Women were ineligible when they resided out of state (or planned to move out of state within 6 months), would not be caring for the child, were not fluent in English or Spanish, or when their child had a major congenital malformation or other medical condition that might have influenced sleep position. Eli-gible women whose infants weighed at least 2500 g at birth were contacted and invited to participate according to a list ordered by the terminal 2 digits of the mother’s medical record number. The order on the list was random with respect to maternal and infant characteristics and time of delivery. Our goal was to enroll at least 50% of eligible mothers and infants. (A similar approach, using a separate list, was used for women who delivered infants who weighed⬍2500 g; these subjects are not considered in this report.) After informed consent was obtained, mother–infant pairs were enrolled and followed until the child’s first birthday. Descriptive data (eg, maternal age, race, ethnicity, parity, the infant’s birth weight) and information on SIDS risk factors (eg, history of ma-ternal smoking during pregnancy) were collected by interview at the time of enrollment. Follow-up data were collected by mailed questionnaire when the infants were 1, 3, and 6 months of age. Mothers who did not respond to the mailed questionnaire were interviewed by telephone. At each follow-up, data were obtained on infant health status and infant care practices (including the position in which the infant was placed for sleep on the previous night and factors that influenced the mother’s choice of position).
Statistical Methods
The2test was used to compare proportions across groups
defined by time or demographic variables. The paired sample2
test was used to compare changes in proportions within a group over time. Percentages in the prone sleep position were compared with the targeted 10% through the2goodness-of-fit test. Multiple
logistic regression was used to evaluate potential risk factors (predictors) for sleep position while controlling for the potential confounding effects of other factors.17Indicator terms were
in-cluded in the logistic regression models for the following: race/ ethnicity, maternal age, marital status, parity, education, smoking while pregnant, annual household income, infant’s gender and postnatal age, breastfeeding, and calendar time. Associations are described with adjusted odds ratios and their 95% confidence intervals. Plots were made to show secular trends in 1- and 3-month sleep position within the following 4 strata based on maternal race/ethnicity and education: 1) white, college graduate; 2) white, non– college graduate; 3) black/Hispanic, college grad-uate; and 4) black/Hispanic, non– college graduate. Black and Hispanic families were pooled in the stratified analysis because the trends were similar in these families and to ensure that each stratum was large enough to assess secular trends. There were not
a sufficient number of Asian families to include in this stratified analysis. Smoothing was performed using a 9-month moving av-erage centered on each calendar quarter. A Mantel-Haenszel2
test for trend was used to assess changes in sleep position over calendar time.18Assessment of factors associated with sleep
posi-tion was limited to the 1- and 3-month data, because 6 months of age is beyond the period of highest risk for SIDS.
RESULTS
Of 24 358 women who delivered a live infant on a covered day at participating hospitals between Feb-ruary 22, 1995, and December 31, 1998, 20 082 (82%) were determined to be eligible for the study. Sixteen percent (3116) of those eligible were not invited to participate either because the mother was discharged before she could be contacted or the recruiter’s time did not permit. Of the 16 966 mothers approached, 1853 (11%) refused to participate or provided an unsatisfactory interview, resulting in 15 113 mother– infant pairs (75.3% of those eligible) being enrolled in the study. This analysis was limited to the 14 206 enrolled mothers who had an infant who weighed at least 2500 g at birth. Of these mothers, 12 029 (85%) responded to the 1-month, 11 552 (81%) responded to the 3-month, and 11 347 (80%) responded to the 6-month follow-up questionnaire. Approximately 25% of responses were obtained by telephone. The pattern of responses obtained by telephone was con-sistent with those obtained by mail. Descriptive char-acteristics of mothers who provided follow-up data at 1 and 3 months and their infants are shown in Tables 1 and 2 (characteristics were similar at 6 months; data not shown). The majority were non-Hispanic whites, 11% were non-non-Hispanic blacks, and 11% to 12% were Hispanic. The mean maternal age was 28 years, the mean birth weight was 3520 g, and 98% of the infants were singletons.
Sleep position for these infants at 1-month, 3-month, and 6-month follow-ups, stratified by years of birth 1995–1996 (published previously16) and 1997–1998 is shown in Fig 1. In 1997–1998, compared with 1995–1996, use of supine sleep position at any given age increased and use of prone sleep position decreased across all ages. However, the pattern ob-served in 1995–1996 of an increasing use of prone sleeping with increasing infant age was still present in 1997–1998 (P⬍.001 for prone sleep at 3 months vs 1 month and at 6 months vs 3 months, paired sample 2). At 1 month of age, the proportion of infants who slept prone declined from 18% in 1995–1996 to 12% in 1997–1998 (P ⬍ .001), with supine sleep position increasing from 18% to 36% (P ⬍ .001). Side sleep position was most common at 1 month of age, used by 49% of infants in 1997–1998. In 1997–1998, 52% of 3-month-old infants were placed to sleep in the su-pine position; however, 20% were still being placed in the prone position.
Fig 1. Percentage of study infants who were placed to sleep in the prone (A), supine (B), or side (C) position at 1, 3, and 6 months of age, respectively, for infants who were recruited during 1995 to 1996 (previously reported14) and 1997 to 1998. Infants who were placed to sleep
ciated with prone and supine sleep position were similar in 1995–1996 and 1997–1998.
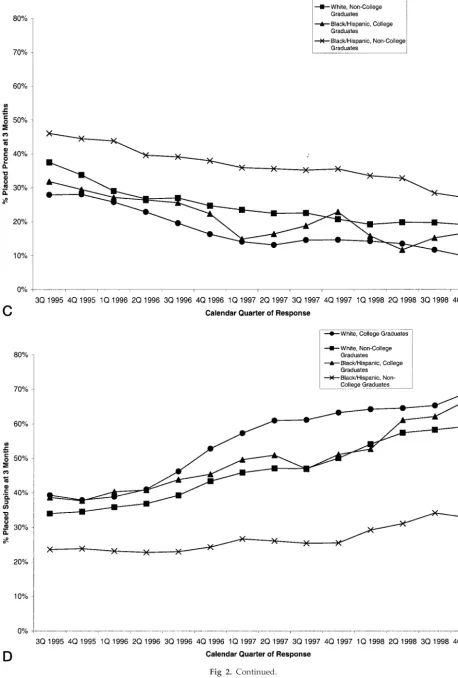
At 1 month of age, the use of prone sleeping failed to reach the goal of ⱕ10% among infants in any groups in 1995–1996, but by 1997–1998, the goal was reached among infants of white and Asian women, women who were older than 25 years, married women, women who were college graduates, and women with household incomes⬎$55 000 per year. At 3 months of age, however, prone sleeping rose to 12% to 17% in these groups (P ⬍ .05 for each by paired sample 2 test). Similarly, in 1997–1998, women with these characteristics were more likely to place their infants to sleep in the supine position; 39% to 45% supine at 1 month, rising to 58% to 64% supine at 3 months of age (P⬍.001 for all groups). The secular trend in prone and supine sleep posi-tion at 1 and 3 months of age, stratified by race and education, is shown in Fig 2. During the 4 years from early 1995 to the end of 1998, prone sleeping at 1 month of age declined in all strata (P ⬍ .01 in all strata). However, black/Hispanic non– college grad-uates did not sustain this decline through 1998 (test for trend over 1997–1998 was not significant,P⫽.9) and was the only stratum that did not approach the target of ⬍10% prone sleeping; during the last 6 months of 1998, prone sleeping was used by 21% of black/Hispanic non– college graduates, a figure that is significantly more than 10% (P⬍.001). During this same period, prone sleeping was used by 3% of white college graduates (a figure that is significantly less than 10%, P ⬍ .001), 11% of black/Hispanic college graduates, and 9% of white non– college graduates (figures that are not significantly different from 10%). Similarly, use of supine sleep position at 1 month of age increased in all strata (P ⬍ .001 for test of trend in all strata); however, at the end of 1998, black/Hispanic non– college graduates had the low-est level of supine sleep at 1 month of age (P⬍ .001 for each pair-wise comparison). Prone sleeping at 3 months of age declined in all strata (P⬍ .01 for test of trend in all strata), but only infants of college-educated white mothers came close to the goal of ⱕ10% (11% in the last 6 months of 1998, not signifi-cantly different from 10%), whereas in each of the other strata, even among infants enrolled at the end of 1998, 18% to 27% of 3-month-old infants were reported as sleeping prone (significantly⬎10%,P⬍
.05 for all strata). Similarly, supine sleep position at 3 months of age increased in all strata (P⬍.001 for test of trend in all strata). However, during the last 6 months of 1998, supine sleeping was markedly less for black/Hispanic non– college graduates (34%) than for the other 3 strata (59%; P ⬍ .001 for each pair-wise comparison).
DISCUSSION
The current study documents that between 1995 and late 1998, lower proportions of parents placed their infant to sleep in the prone sleep position, and greater proportions used the supine infant sleep po-sition. However, the factors associated with in-creased risk of prone sleeping and dein-creased likeli-hood of supine position did not change substantially
between 1995 and 1998, suggesting that in 1997–1998, sleep position recommendations continued to be less effective among black and Hispanic families and families of low income and mothers with less than a college education. For these families, at the end of 1998, the prevalence of prone sleeping at 3 months of age (the peak age for SIDS) was⬎20%.
These data are consistent with the US national telephone survey that indicates the prevalence of prone sleeping has declined from 44% to 17% and supine sleeping increased from 17% to 51% between 1994 and 1998.15These data are also consistent with reports indicating that black and low-income fami-lies are more likely to place their infants to sleep in the prone position.13,15,19 –21 However, the present study includes a larger sample of minority infants than earlier reports, resulting in more stable esti-mates and permitting the detection of significant as-sociations between race/ethnicity and prone sleep-ing. Because the present study enrolled a representative sample of all women who delivered a child at a participating hospital, our data are also less subject to selection bias than telephone surveys, which by definition are limited to households with telephones. Furthermore, the unique longitudinal design of this study provides an opportunity to ob-serve changes in sleep position as children grow and to identify those infants who change to the prone position between 1 and 3 months.
There are several limitations to these data. Sleep position was based on maternal description, not di-rect observation. Mothers were enrolled only in east-ern Massachusetts and northwest Ohio and com-pared with the US population; a higher proportion of study mothers had some postsecondary education. As such, these women may not be representative of all US women who gave birth during this time. In particular, the Hispanic women in our study were predominantly of Puerto Rican origin and may not reflect attitudes and behaviors of other Hispanic groups (eg, Mexican Americans), and the total num-ber of Asian women (predominantly of Southeast Asian origin) was small. In addition, it is possible that the rate of supine sleeping overall may be lower in other areas of the United States because the sub-jects of this report had an overrepresentation of col-lege-educated women, a predictor for supine sleep-ing.
CONCLUSION
If one considers initial choice of sleeping position (ie, at 1 month of age), then the goal of ⱕ10% of infants sleeping prone was achieved in 1998 only among infants of white, college-educated, and older mothers; however, the rate of prone sleeping remains
addition, the factors associated with increased risk of prone sleeping and decreased likelihood of supine position have not changed substantially between 1995 and 1998. Therefore, it seems reasonable that efforts intended to reduce further the prevalence of prone sleeping should be designed to target the pop-ulation groups that are at particular risk for this practice. It also seems clear that increased emphasis on supine sleeping may be warranted, especially for the groups that have been least likely to use this position. In virtually all other countries where a pub-lic health intervention has been undertaken to change infants’ sleep position, the prevalence of prone sleeping has decreased substantially and is now generally below 10%.6,22–27The challenge that remains is to design or identify strategies that will have a comparable benefit among high-risk groups in the United States.
ACKNOWLEDGMENTS
This project has been supported by funds from the National Institute of Child Health and Human Development and National Institute on Deafness and Other Communicative Disorders, Na-tional Institutes of Health, under contract N01-HD-4-3221, and was conducted with the cooperation of the Massachusetts Depart-ment of Public Health.
We thank Sandra Hatfield, Dottie Powers, and Debra Zagaeski for research assistance; Maria Francescon, Patricia Brousseau, Chris DeArmond, Cynthia Nagle, Heather Wightmann, and Grace Adeya for recruiting patients and conducting the interviews; Paul Paslaski and Leonard Gaetano for programming assistance; and Theodore Colton, ScD, for advice on study design and data anal-ysis. We are indebted to the physicians and nurses at the following hospitals: Boston Medical Center and the Beth Israel Hospital (Boston, MA), Lowell General Hospital (Lowell, MA), Lawrence General Hospital (Lawrence, MA), and St Vincent Mercy Medical Center and Toledo Hospital (Toledo, OH).
REFERENCES
1. Mathews TJ, Curtin SC, MacDorman MF. Infant mortality statistics from the 1998 period linked birth/infant death data set.Natl Vital Stat Rep. 2000;48:1–25
2. Hunt CE. Sudden infant death syndrome. In: Behrman RE, Kliegman RM, Jenson HB, eds.Nelson Textbook of Pediatrics. 16th ed. Philadelphia, PA: WB Saunders Company; 1999:2139 –2143
3. Fleming PJ, Gilbert RE, Azaz Y, et al. The interaction between bedding and sleeping position in sudden infant death syndrome: a population-based case-control study.Br Med J.1990;301:85– 89
4. Mitchell EA, Scragg R, Stewart AW, et al. Results from the first year of the New Zealand cot death study.N Z Med J.1991;104:71–76 5. Dwyer T, Ponsonby A-L, Newman NM, Gibbons LE. Prospective cohort
study of prone sleeping position and sudden infant death syndrome.
Lancet.1991;337:1244 –1247
6. Fleming PJ, Blair PS, Bacon C, et al. Environment of infants during sleep
and risk of the sudden infant death syndrome: results of 1993–5 case-control study for confidential inquiry into stillbirths and deaths in infancy.BMJ.1996;313:191–195
7. Scragg RKR, Mitchell EA. Side sleeping position and bed sharing in the sudden infant death syndrome.Ann Med.1998;30:345–349
8. Irgens LM, Markestad T, Baste V, Schreuder P, Skjaerven R, Oyen N. Sleeping position and sudden infant death syndrome in Norway 1967–91.Arch Dis Child.1995;72:478 – 482
9. de Jonge GA, Burgmeijer RJF, Engleberts AC, Hoogenboezem J, Ko-stense PJ, Sprij AJ. Sleeping position for infants and cot death in the Netherlands 1985–91.Arch Dis Child.1993;69:660 – 666
10. Mitchell EA, Brunt JM, Evard C. Reduction in mortality from sudden infant death syndrome in New Zealand.Arch Dis Child.1994;70:291–294 11. Dwyer T, Ponsonby A-L, Blizzard L, Newman NM, Cochrane JA. The contribution of changes in prevalence of prone sleeping position to the decline in sudden infant death syndrome in Tasmania.JAMA.1995;273: 783–789
12. Gilbert R. The changing epidemiology of SIDS.Arch Dis Child.1994;70: 445– 449
13. Willinger M, Hoffman HJ, Wu K-T, et al. Factors associated with the transition to nonprone sleep positions in the United States: the National Infant Sleep Position Study.JAMA.1998;280:329 –335
14. Task Force on Infant Positioning and SIDS. Positioning and sudden infant death syndrome (SIDS): update.Pediatrics.1996;98:1216 –1218 15. Willinger M, Ko C-W, Hoffman HJ, Kessler RC, Corwin MJ. Factors
associated with caregivers’ choice of infant sleep position, 1994 –1998: the National Infant Sleep Position Study.JAMA.2000;283:2135–2142 16. Lesko SM, Corwin MJ, Vezina RM, et al. Changes in sleep position
during infancy: a prospective longitudinal Assessment.JAMA.1998;280: 336 –340
17. Armitage P.Statistical Methods in Medical Research. New York, NY: John Wiley and Sons; 1971:319 –320
18. Mantel N, Haenszel W. Statistical aspects of the analysis of data from retrospective studies of disease.J Natl Cancer Inst.1959;22:719 –748 19. Brenner RA, Simons-Morton BG, Bhasker B, et al. Prevalence and
pre-dictors of the prone sleep position among inner city infants.JAMA. 1998;280:341–346
20. Johnson CM, Borkowski MM, Hunter KE, et al. A telephone survey of inner-city parents of color.Pediatrics.1999;104:1208 –1211
21. Gibson E. Infant sleep position 2 years into the “back to sleep” cam-paign.Clin Pediatr.2000;39:285–289
22. Mitchell EA, Tonkin S. Publicity and infants’ sleeping position [letter]. BMJ.1993;306:858
23. Scragg LK, Mitchell EA, Tonkin SL, Hassall IB. Evaluation of the cot death prevention programme in South Auckland.N Z Med J.1993;106: 8 –10
24. Ponsonby A-L, Dwyer T, Kasl SV, Cochrane JA, Newman NM. An assessment of the impact of public health activities to reduce the prev-alence of the prone sleeping position during infancy: the Tasmanian Cohort Study.Prev Med.1994;23:402– 408
25. Markestad T, Skadberg B, Hordvik E, Morild I, Irgens LM. Sleeping position and sudden infant death syndrome (SIDS): effect of an inter-vention programme to avoid prone sleeping.Acta Paediatr.1995;84: 375–378
26. Hiley CMH, Morley CJ. Evaluation of government’s campaign to re-duce risk of cot death.BMJ.1994;309:703–704
DOI: 10.1542/peds.111.1.52
2003;111;52
Pediatrics
Hunt, Frederick Mandell, Mary McClain and Allen A. Mitchell
Michael J. Corwin, Samuel M. Lesko, Timothy Heeren, Richard M. Vezina, Carl E.
1998
−
Secular Changes in Sleep Position During Infancy: 1995
Services
Updated Information &
http://pediatrics.aappublications.org/content/111/1/52
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/111/1/52#BIBL
This article cites 25 articles, 9 of which you can access for free at:
Subspecialty Collections
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_
Fetus/Newborn Infant
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.111.1.52
2003;111;52
Pediatrics
Hunt, Frederick Mandell, Mary McClain and Allen A. Mitchell
Michael J. Corwin, Samuel M. Lesko, Timothy Heeren, Richard M. Vezina, Carl E.
1998
−
Secular Changes in Sleep Position During Infancy: 1995
http://pediatrics.aappublications.org/content/111/1/52
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.