Improved Survival in Heart Failure Associated
with Aspirin Alone or in Combination with ACE
Inhibition: An Observational Study
by
Sandeep R. Das, MD
A Master's Paper submitted to the faculty of The University of North Carolina at Chapel Hill
In partial Fulfillment of the requirements for The degree ofMaster of Public Health in
The Public Health Leadership Program
ACKNOWLEDGMENTS
Kirkwood F. Adams, Jr., MD- Provided overall guidance and direction through all stages of the project. Provided feedback for all sections of the
manuscript.
Linda Kinsinger, MD, MPH- Primary reader and advisor. Provided feedback for all sections of the manuscript.
Deborah Porterfield, MD, MPH- Second reader. Provided feedback for all sections of the manuscript.
ABSTRACT
Background
The appropriate role of aspmn m heart failure is controversial. Retrospective analyses have suggested the use of aspirin may attenuate the benefit seen with angiotensin converting enzyme inhibitor (ACEI) therapy. This study investigates the relationship between aspirin use and survival in the UNC Heart Failure Database. This cohort has substantially greater representation of women (32%), African-Americans (44%), and patients with heart failure of a non-ischemic etiology ( 68%) than previously examined populations.
Methods
Results
Multivariate, adjusted survival analysis indicated aspirin use at baseline was associated with a significant reduction in all-cause mortality, with a hazard ratio (HR) for aspirin use of0.71 (95% CI 0.55-0.92). In patients taking ACEI at baseline, the HR for aspirin use was 0.76 (0.57-1.01) compared to a HR of 0.61 (0.31-1.19) for those not taking ACEI. In patients with ischemic heart disease
(lliD) as their primary HF etiology, the HR for aspirin use was 0.65 (0.46-0.94) compared to a HR of0.93 (0.64-1.34) for those with a primary HF etiology other than lliD.
Conclusion
INTRODUCTION
Context
As the U.S. population ages, and as Americans survlVe longer with hypertension and ischemic heart disease (lliD), heart failure (HF) continues to increase in prevalence.[!] Currently, this clinical syndrome affects almost five million Americans, and based on data from the American Heart Association, over 500,000 new cases of.HF are diagnosed each year.[2] Despite a steady stream of therapeutic advances, heart failure continues to be associated with significant morbidity and mortality.[2, 3]
Over the past two decades, ischemic heart disease has emerged as a major etiology of chronic heart failure due to left ventricular (LV) systolic dysfunction and studies have demonstrated an increased risk of death when lliD is the primary HF etiology. [ 4-6] This increased risk appears to stem from instability in atherosclerotic plaques, with platelet-mediated progression leading to chronic myocardial dysfunction, even in the absence of clinically overt ischemic events. [7, 8] The platelet is now well established to play a critical role in the transition from plaque instability to ischemic events in patients with lliD.[7, 8]
to be ideal for this purpose, being both inexpensive and widely studied. However, there has been no randomized trial of aspirin in heart failure.
Angiotensin converting enzyme inhibitors (ACEI) have a well-established beneficial effect on morbidity and mortality in patients with left ventricular dysfunction and are a fundamental part of standard heart failure therapy. The mechanism of this beneficial effect has not been fully elucidated, but is most likely derived via alterations in the levels of circulating mediators such as bradykinin and certain prostaglandin subtypes. Therefore, the combined use of aspirin and ACEI seems logical in patients with HF due to lliD.
However, retrospective studies have suggested a possible attenuation of benefit when using aspirin and angiotensin converting enzyme inhibitors together.[ll-14] Aspirin works by inhibiting the cyclooxygenase enzyme
(COX-I), which decreases the conversion of arachadonic acid precursors into vasoactive prostaglandins PGI2 and PGE3, as well as the thromboxane, TXAz. This suggests
a biologically plausible mechanism for an adverse interaction between aspirin and ACEI. Since ACEI are a well-established part of heart failure therapy,[15-20] it is important to further assess the effects of aspirin in this population.
(32%), African-Americans (44%), and patients with heart failure of a non-ischemic etiology ( 68%) than previously examined populations.
Aspirin in ischemic heart disease
The Antiplatelet Trialists' Collaboration has presented a meta-analysis that indicates aspirin therapy results in approximately a 25% reduction in vascular events, defined as myocardial infarction (MI), stroke (CV A), or cardiovascular (CV) death, in several categories of patients at high risk for such events. In patients post acute MI, aspirin reduced the subsequent vascular event rate to 10%, compared to 14% for placebo. Similarly, in patients with a history ofMI, vascular events were reduced to 13% with aspirin, compared to 17% with placebo. The relative risk reduction seen in patients with a history of stroke or with several other cardiac risk factors was similar. All cause mortality was significantly reduced in high-risk patients with a rate of 8.0% for patients taking aspirin compared to 9.5% for placebo. The average duration of therapy was 2 years. Aspirin doses ranged from 75 to 1500 mg per day, with no material difference in efficacy seen based on dose. [21]
CI 15% to 30%) reduction in the odds of death. [22] The Collaborative group of the Primary Prevention Project (PPP) reported the results of a randomized controlled open-label trial of low-dose aspirin, 100 mg per day, for primary prevention of cardiovascular events in patients with one or more risk factors. In this trial of 4,495 patients followed for a mean duration of 3.6 years, aspirin reduced cardiovascular death from 1.4% to 0.8%, a relative risk of 0.56 (95% CI 0.31-0.99) [23]
Angiotensin converting enzyme inhibitors in heart failure
Several large trials have been published which serve to illustrate the benefit of ACEI therapy in HF. The second Veteran's Administration Cooperative Vasodilator-Heart Failure Trial (V-HeFT II) showed that the ACEI enalapril reduced mortality in patients with symptomatic heart failure. In fact, the reduction in mortality seen with enalapril was significantly greater than that seen with the combination of hydralazine and isosorbide dinitrate, suggesting that the beneficial effect of ACEI is more than can be explained by its properties as a vasodilator. The cumulative mortality at one year was 9% for enalapril, compared to 13% for hydralazine-isosorbide dinitrate and an estimated 20% for placebo. This dramatic relative advantage decreased, but still persisted, over four years where the cumulative mortality for enalapril was 42% compared to 47% for hydralazine-isosorbide dinitrate and an estimated 54% for placebo.[l5]
(Treatment trial) and without (Prevention trial) clinical HF. The SOL VD Treatment trial randomized 2,569 patients to enalapril vs. placebo and used the primary endpoint of all-cause mortality. Patients randomized to enalapril had a lower rate of death (35.2% vs. 39.7% for placebo, p<0.0036) with a risk reduction of 16% (95% CI 5% to 26%).[16]
The SOL VD Prevention trial was also designed to examine the primary endpoint of all-cause mortality as well as secondary endpoints of unstable angina (USA), MI, CV death, and development of HF. The 4,228 patients were also randomized to enalapril vs. placebo and followed for an average of 40 months. There was a non-significant trend toward lower all-cause mortality with enalapril (14.8% vs. 15.8% for placebo, p=0.30) and there was a statistically significant difference in development of HF that favored enalapril (20. 7% vs. 30.2% for placebo) with a risk reduction of37% (95% CI 28% to 44%).[17]
For the composite endpoint of CV death or non-fatal MI, enalapril had lower mortality in patients with HF (33.4% vs. 39.3% for placebo) for a risk reduction of 19% (95% CI 8 to 29%). In patients without clinical HF, the risk reduction with enalapril was similar (15.6% vs. 19.5% for placebo), with a value of 23% (95% CI 11% to 33%). The relative risk reduction for enalapril vs. placebo was roughly the same for each of the three previously mentioned
mortality.[18]
In the Survival and Ventricular Enlargement (SAVE) study, 2,231 patients
without clinical HF were randomized to captopril vs. placebo and followed for an average of 42 months. All-cause mortality was significantly reduced by captopril (20% vs. 25%, p=0.019) This was a 19% risk reduction (95% CI 3% to 32%) which was present out to an average of 42 months, however no difference in mortality was apparent until after one year. Roughly similar reductions were seen in non-fatal major cardiovascular events, such as development of heart failure and recurrent MI. The subgroup taking aspirin had a significantly lower mortality rate with ramipril (16.6% vs. 21.4% for placebo) with a relative risk reduction of24% (95% CI 2% to 41%). In contrast, the subgroup not taking aspirin had no significant difference in mortality with ramipril (26.0% vs. 29.2% for placebo). [ 19]
The Acute Infarction Ramipril Efficacy (AIRE) study was a randomized, double blind trial that investigated the effect of ramipril, an oral ACEI, in 2, 006 hemodynamically stable post-MI patients with mild to moderate clinical heart failure. Patients assigned to ramipril had significantly lower all-cause mortality at an average of 15 months compared to placebo (17% vs. 23%, p=0.002) for a relative risk reduction of 27% (95% CI 11% to 40%). The point estimate for the relative risk of death (ramipril vs. placebo) for the subgroup taking aspirin was approximately 0.8 compared to approximately 0.6 for the subgroup not taking
. . b h. d"ffi . . 11 • "fi
asptnn, ut t 11s 1 erence was not stattstlca 1y stgm. 1cant, and there was no
Angiotensin converting enzyme inhibitors in ischemic heart disease
Aspirin and Angiotensin converting enzyme inhibitors interaction
Administration of ACEI results in the accumulation of bradykinin, which may have beneficial effects by promoting vasodilation and limiting cardiac remodeling. Experimental evidence suggests the influence of bradykinin accounts for at least part of the benefit of ACEI in HF or post-MI.[l2, 26] Beneficial effects of bradykinin appear to be related to activation of NO production and COX which stimulate synthesis of a variety of PG's which have vasoactive and cytoactive effects that may be beneficial in these diseases.[19] In contrast, aspirin blocks COX, which in tum decreases the conversion of the precursors of arachadonic acid to vasoactive prostaglandins like PGiz and PGE3 . [27]
The issue of possible attenuation of the effect of ACEI by aspirin has been an area of intense debate. Given potential deleterious effects of aspirin with respect to renal function[28, 29] or dyspepsia/gastrointestinal bleeding,[30] its use in HF patients is not without potential harm. Prostaglandins (PG) play an important endogenous vasodilatory role and counteract the enhanced peripheral vasoconstriction state of heart failure.[13] ACEI reduce plasma levels of the vasoconstrictor angiotensin II (ATII); they also inhibit breakdown of bradykinin (BK) that stimulates PG synthesis. Increase in BK is the predominant reason for the antihypertensive effect of ACEI.[ll] The beneficial effect of ACEI cannot be entirely explained by the inhibition of ATII. ACEI produce persistent benefits, although circulating levels of ATII gradually return to normal. [ 13] A study found that patients with severe HF had levels of PGE2 and PGiz that were three to ten
anti-inflammatory drug that inhibits PG synthesis, caused worsenmg hemodynamics. [II]
Using invasive hemodynamic monitoring, Hall and co-workers observed that aspirin inhibited the vasodilator effect of enalapril in patients with severe HF. [31] Guazzi and colleagues showed that enalapril improved pulmonary gas exchange and lung volumes. Beneficial changes in pulmonary gas exchange were counteracted by aspirin.[26] A dose of 325 mg aspirin was given for 8 weeks to patients with dilated cardiomyopathy and NYHA class II-III HF (18 on ACEI, 8 not on ACEI, not randomized). Aspirin had inhibitory effect on measures of oxygen exchange. [32] In a 1993 study, van Wijngaarden, et al. determined that the ACEI captopril, given alone, did not change circulating levels of the vasodilatory prostaglandins PGI2 and PGE2 or the vasoconstricting thromboxane A2 (TXA2). However, co-administration of a single dose of aspirin reduced circulating PGE2 and TXA2 levels, without a corresponding hemodynamic effect. [27] In this study, a low dose of aspirin was used. Low doses of aspirin inhibit TXA2; higher doses are needed to reduce PG's.[27] Evans, et al., found no hemodynamic, neurohumoral, or renal effect of low dose aspirin alone in a canine model. [33]
In addition to in vitro studies, retrospective data analysis has been done on data from several cliPical trials. A retrospective ana!ysis[34] of patients in the
collected, clopidogrel was not available, and the use of dipyridamole was limited, so the anti-platelet agents referred to in SOL VD can safely be assumed to be aspirin. In patients taking aspirin there was no benefit to enalapril, while in patients not taking aspirin, there was benefit if randomized to enalapril. Adjusted for confounders, anti platelet agent (AP A) use was associated with reduction in CV death, but not associated with death due to worsening HF or non-cardiac death. Point estimates for the effects of AP A in the combined group were: all cause mortality (0.82), CV death (0.80), sudden death (0.78), HF death (0.92/NS), fatal MI (0.58), and non-CV death (1.27/NS).
No significant interaction between aspirin use and enalapril was seen with respect to mortality; however a significant association between aspirin use and survival was seen only in patients with an ischemic etiology. There was a non-significant trend toward improved survival among non-ischemics receiving
aspirin. The HR for enalapril users vs. non-users for all cause mortality stratified by aspirin use were: aspirin (1.1 0/NS), no aspirin (0. 77). Possible explanations for these results are: 1) aspirin antagonizes enalapril, 2) aspirin and enalapril derive benefit via same mechanism, or 3) the interaction between aspirin and enalapril is multifactorial.
analysis of patients from the GUSTO-I and EPILOG trials[12] determined that the combined use of aspirin and ACEI was associated with increased mortality in GUSTO-I patients (HR 2.2, 95% CI 1.1 to 4.3) and in EPILOG patients (HR 2.1, 95% CI 1.1 to 3.8) compared with aspirin alone.
A post hoc analysis of the Captopril and Thrombolysis (CATS) study[35] showed that aspirin did not attenuate effects of ACEI after acute MI, but independently reduces LV dilation after MI. The Acute Myocardial Infarction Survival (AMIS) trial[28] showed an increase in mortality in most subgroups with aspirin, while the second Persantine Aspirin Reinfarction Study (PARIS 11)[29] showed an overall trend toward benefit, but a trend toward harm in heart failure. These are older studies and used higher aspirin doses, up to 1500 mg/day.[14]
The Acute Infarction Ramipril Efficacy (AIRE) study also suggested an interaction between ACEI use and the effect of aspirin on mortality in HF patients. The point estimates for the relative risk of death for the subgroup taking aspirin suggested less benefit from ACEI compared to the subgroup not taking aspirin, although investigators were unable to show a statistically significant interaction between the two drugs.[20] In the Survival and Ventricular Enlargement (SAVE) trial also, no interaction between aspirin use and the effect of ACEI on mortality was seen.[19] Finally, in the Benzafibrate Infarction 0·e·ve-tt·~- 'BTD\ • ..:"1 Af"'PT :- "~mb:nat:on ""•h aspt"n"n ha-l a b~n~r.l":at ~""~~• .1. 1 11 VU \ _Ll_ ) U lCU' ~'-'.J..j.J. Ul VVI.l H 1 .l VV .1'- 1 .L 1 l U- .... ""-'- ... .l "-'lll,.,v._
Limitations related to the available clinical data concerning the aspmn-ACEI interaction must be acknowledged. Analysis of the SOL VD and CONSENSUS II data was done on a retrospective basis. Patients were not randomly assigned to aspirin use in these studies. Unknown differences in baseline characteristics, not accounted for in the statistical analysis, might have existed. In contrast, studies using hemodynamic end points, like SVR, were done prospectively and clearly indicate that antagonism of the hemodynamic effects of ACEI by aspirin occurs. The effect may be dose-dependent. One alternative explanation for the lack of additive benefit from ACEI and aspirin is that the principal effects of ACEI were anti-ischemic. [ 11] Aspirin may negate the benefits of ACEI, or it may be that ACE offers no additional advantage.[14]
In summary, previous work on aspirin in heart failure has been somewhat contradictory, but has suggested that there may be an adverse interaction between aspirin and ACEI such that use of aspirin in HF patients taking ACEI may need to be reconsidered. The greatest weakness of the prior published data is the absence of any randomized controlled trial of aspirin in heart failure. Given that such an undertaking is at this time unlikely, the best current evidence comes from a synthesis of retrospective data sources. The principal data sources being
considered, as described above, have generally used a patient population that is
METHODS
Patients
The present study utilizes data from the University of North Carolina Heart Failure Database. All patients seen in the University of North Carolina heart failure clinic are entered into the database at the time of their initial clinic visit. History and physical examination findings at that time are recorded, including a detailed medication history. For the purposes of this study, medications initiated at a patient's first visit are considered part of their baseline medications. The majority of patients received their continuing care in the University of North Carolina heart failure clinic according to the general heart failure guidelines at the time of the patient's enrollment. However, treatment was not rigorously standardized, as it would have been in a clinical trial.
Variables
Information on New York Heart Association class, aspmn and ACE
inhibitor use at baseline, gender, age, and history of diabetes was obtained from a
detailed history and physical examination at time of study entry. Available
clinical, laboratory and autopsy data were used to assign a primary etiology for
heart failure and to determine the presence or absence of coronary artery disease
in each patient. Presence of atrial fibrillation was determined by baseline
electrocardiogram. Left ventricular ejection fraction and left ventricular volume
were determined by radionuclide ventriculography within 6 months of study
entry. Vital status was ascertained at last follow-up from contact with the patient,
a family member, or the referring physician, and was used to assign a cause of
death. Patients undergoing cardiac transplantation were considered alive and
censored at the time of surgery.
Analysis
Statistical analysis was performed usmg the SAS software package
(Version 8.2, SAS Institute, Cary NC). Bivariate analysis was performed for all
independent variables against the primary outcome of all cause mortality, and
against the principal exposure of aspirin use. P-values are reported from
individual comparisons using Student's t-test or the Chi-square test as appropriate,
with two-sided p-values of less than 0.05 considered statistically significant.
differences between the curves tested for significance by the log-rank statistic. [3 6]
RESULTS
Baseline characteristics
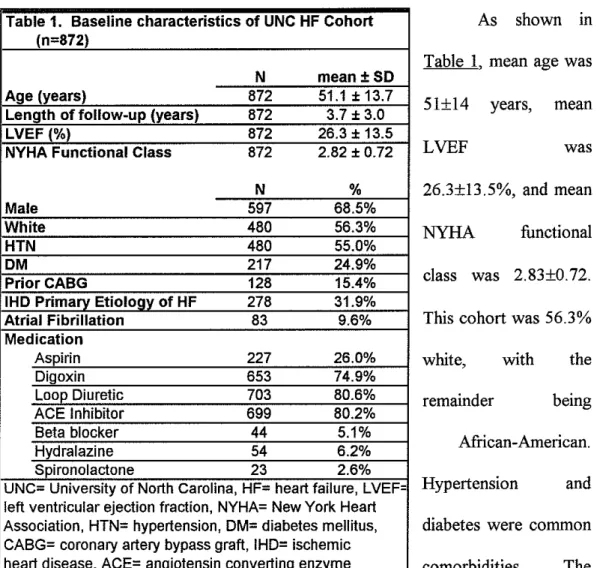
Table 1. Baseline characteristics of UNC HF Cohort As shown in (n=872)
Table 1, mean age was
N mean±SD
Age (years) 872 51.1 ± 13.7
Length offollow-up (years) 872 3.7 ± 3.0 51±14 years, mean
LVEF (%) 872 26.3 ± 13.5
NYHA Functional Class 872 2.82 ± 0.72
LVEF
wasN % 26.3±13.5%, and mean
Male 597 68.5%
White 480 56.3% NYHA functional
HTN 480 55.0%
DM 217 24.9%
PriorCABG 128 15.4% class was 2.83±0.72.
IHD Primary Etiology of HF 278 31.9%
Atrial Fibrillation 83 9.6% This cohort was 56.3%
Medication
Aspirin 227 26.0% white, with the
Digoxin 653 74.9%
Loop Diuretic 703 80.6%
ACE Inhibitor 699 80.2% remainder being
Beta blocker 44 5.1%
Hydralazine 54 6.2% African-American.
Spironolactone 23 2.6%
UNC- University of North Carolina, HF= heart failure, LVEF= Hypertension and
left ventricular ejection fraction, NYHA= New York Heart
Association, HTN= hypertension, DM= diabetes mellitus, diabetes were common
CABG= coronary artery bypass graft, IHD= ischemic
heart disease, ACE= angiotensin converting enzyme comorbidities. The
collected. Other commonly used drugs in our population included long-acting nitrates (20.2%), calcium channel blockers (13.8%), and warfarin (36.7%).
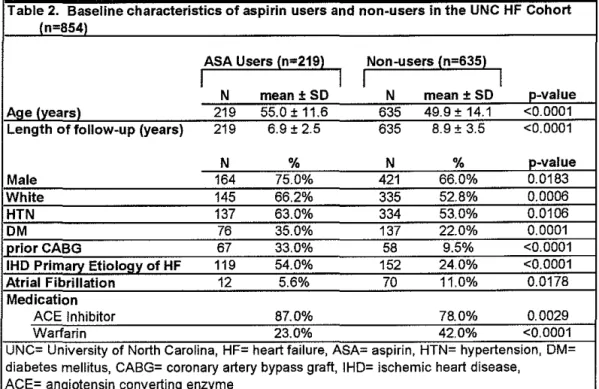
Table 2. Baseline characteristics of aspirin users and non-users in the UNC HF Cohort {n=854)
ASA Users {n=219)
I
I
Non-users {n=635)
I
I
N mean± SO N mean+ SO p-value
Age {years) 219 55.0±11.6 635 49.9 ± 14.1 <0.0001
Length of follow-up {years) 219 6.9 ± 2.5 635 8.9 ± 3.5 <0.0001
N % N % p-value
Male 164 75.0% 421 66.0% 0.0183
White 145 66.2% 335 52.8% 0.0006
HTN 137 63.0% 334 53.0% 0.0106
OM 76 35.0% 137 22.0% 0.0001
prior CABG 67 33.0% 58 9.5% <0.0001
IHO Primary Etiology of HF 119 54.0% 152 24.0% <0.0001
Atrial Fibrillation 12 5.6% 70 11.0% 0.0178
Medication
ACE Inhibitor 87.0% 78.0% 0.0029
Warfarin 23.0% 42.0% <0.0001
UNC University of North Carolina, HF heart failure, ASA aspirin, HTN hypertension, DM diabetes mellitus, CABG= coronary artery bypass graft, IHD= ischemic heart disease, ACE= angiotensin converting enzyme
Characteristics of aspirin users vs. non-users overall
patients not taking aspirin had a higher prevalence of atrial fibrillation (11% vs. 5.6%, p=0.0178) and were more likely to be on anticoagulants (42% vs. 23%, p<0.0001). In Table 3, a description of patient characteristics for the 699 patients on ACE inhibitor is shown. The differences in descriptive statistics for aspirin use or non-use in patients taking ACEI at baseline were essentially the same as those for aspirin use versus non-use in the overall population.
users vs non-users among users
ASA Users (n=197) Non-users (n=502)
I
54
enzyme
ASA= aspirin, LVEDVI= left ventricular end diastolic volume index, LVESVI= left ventricular end systolic volume index, HTN= hypertension, DM=diabetes mellitus, CABG= coronary artery bypass
IHD= ischemic heart disease
Characteristics of aspirin users vs. non-users by etiology
fibrillation (15.1% vs. 3.3%, p=0.0010) and trended toward a higher likelihood of taking warfarin than those taking aspirin (45.5% vs. 29.0%, p=0.0051), although absolute numbers were small. Table 5 summarizes patient characteristics for the subset of patients without ischemic heart disease. For the 594 patients with a primary heart failure etiology other than IHD, the differences in descriptive statistics based on aspirin use or non-use were similar to those for aspirin use or non-use in the overall population with a few exceptions. Patients without IHD as a primary HF etiology taking or not taking aspirin were equally likely to be male or to be white. Overall likelihood of atrial fibrillation was similar between the two groups, but patients not taking aspirin had a higher likelihood of taking warfarin than those taking aspirin (40.3% vs. 15.5%, p<0.0001).
Table 4. Baseline characteristics of aspirin users vs non-users among patients with
an IHD HF etioloQV in the UNC HF Cohort ln=278)
ASA Users (n=124)
I
I
I
Non-users (n=154)I
N mean +SO N mean ±SD p-value
Aqe lvearsl 124 57.1 ± 10.0 154 58.5± 11.0 0.2938
Body mass lk!1/m2l 118 25.8 + 4.4 146 26.0 ± 4.8 0.7218
LVEF (units) 124 25.0 ± 10.9 154 24.1 ± 10.3 0.5213
LVEDVI (ml/m2) 120 169.2 ± 58.5 147 176.9 + 61.3 0.2868
NYHA Functional Class 124 2.86 ± 0.70 154 2.93 ± 0.76 0.4593
N % N % p-value
Male 108 87.1% 133 86.4% 0.8580
White 101 84.9% 117 77.0% 0.1037
HTN 66 53.2% 82 53.3% 0.9972
DM 42 33.9% 53 34.4% 0.9242
prior CABG 67 55.4% 57 38.3% 0.0050
Atrial Fibrillation 4 3.3% 23 15.1% 0.0010
Medication
ACE Inhibitor 103 83.1% 117 76.0% 0.1481
Warfarin 36 29.0% 70 45.5% 0.0051
Table 5. Baseline characteristics of aspirin users vs non-users among patients with a non-IHO HF etiology in the UNC HF Cohort Jn=594)
ASA Users (n=103)
I
I
Non-users (n=491)
I
I
N mean+ SO N mean± SO p-value
Age (years) 103 52.8 ± 12.7 491 46.9 + 13.9 <0.0001
Body mass (kg/m2) 98 29.0 + 7.5 477 27.6 ± 6.8 0.0638
LVEF (%) 103 29.3 + 14.5 491 26.8 + 14.6 0.1054
LVEOVI (mllm2) 101 171.5 ± 75.7 471 187.9 ± 69.2 0.0344
NYHA Functional Class 103 2.80 ± 0.65 491 2.78 ± 0.72 0.8131
N % N % p-value
Male 63 61.1% 293 59.7% 0.7789
White 44 44.0% 218 45.2% 0.8222
HTN 77 74.8% 255 51.9% <0.0001
OM 37 35.9% 85 17.4% <0.0001
priorCABG 2 2.2% 2 0.4% 0.0633
Atrial Fibrillation 8 7.9% 48 9.8% 0.5580
Medication
ACE Inhibitor 94 91.3% 385 78.4% 0.0027
Warfarin 16 15.5% 198 40.3% <0.0001
ACE- angiotensin converting enzyme, UNC- University of North Carolina, HF= heart failure, ASA= aspirin, LVEDVI= left ventricular end diastolic volume index, IHD= ischemic heart disease HTN= hypertension, DM=diabetes mellitus, CABG= coronary artery bypass graft
Survival Analysis
i ""'
~ 6
l ...
~
L .
.
.,
.. ,'
Kaplan_.~~r ~I'VE!$ fQr }\.$A V$. r-!l)t
""""'
... '(
""'
'""'""'
31AA.'ll!i: ----ASAP_,-0 - · - AsAf> .. id
Figure 1. Survival (Kaplan-Meier) curves for aspirin users (dashed line) and non-users (solid line). Results are unadjusted, and outcome is all-cause mortality. Vertical axis is percent survival, and horizontal axis is length of follow-up in days.
Kaplan-Meier
curve~for
ASA vs.
N()tl'hl:4+ <>n AOB
...
'
-
"'"·L.---.---~----~,---~---•
STPATA: - A."SA~ 0 - --A!!A:P'»-'1
.,
•
''"'"""
S'"""'.f:f- -··:AOEJift -~:ACE.+<!ISA :.,-•. --:tW._..
Figure 3. Survival (Cox proportional-hazards analysis) curves for aspirin users (dashed line) and non-users (solid line), among patients taking ACEI at baseline. Results are adjusted for New York Heart Association Class, left ventricular ejection fraction, sex, age, left ventricular end diastolic volume, atrial fibrillation, and diabetes mellitus. Outcome is all-cause mortality. Vertical axis is percent survival, and horizontal axis is length offollow-up in days. Top-most dashed line is the curve for patients on ACEI and aspirin, solid line represents patients on ACEI but not aspirin, and the lowest dashed line (poorest survival) represents patients on neither ACEI nor aspirin.
wide. There was no statistically significant effect modification due to ACE use on the relationship between aspirin use and mortality.
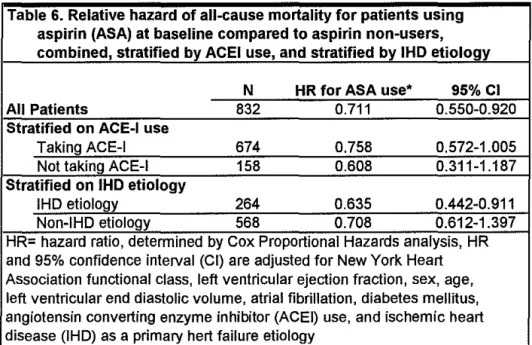
Stratified into groups based on HF etiology, the patients with known lliD
as a primary etiology of their heart failure had a 3 5% lower mortality with aspirin use (HR 0.654, 95% CI 0.455-0.939). Patients without known lliD showed no statistically significant benefit from aspirin use (HR 0.926, 95% CI 0.639-1.341). Once again, there was no statistically significant effect modification due to etiology on the relationship between aspirin use and mortality. The results of adjusted multivariate Cox proportional-hazards analysis are shown in Table 6.
Table 6. Relative hazard of all-cause mortality for patients using aspirin (ASA) at baseline compared to aspirin non-users, combined, stratified by ACEI use, and stratified by IHD etiology
N HR for ASA use• 95%CI
All Patients 832 0.711 0.550-0.920
Stratified on ACE-I use
Taking ACE-I 674 0.758 0.572-1.005
Not taking ACE-I 158 0.608 0.311-1.187
Stratified on IHD etiology
IHD etiology 264 0.635 0.442-0.911
Non-IHD etiology 568 0.708 0.612-1.397
DISCUSSION
In this study population, aspirin use is associated with a statistically significant 29% reduction in all-cause mortality using a multivariate Cox proportional hazards analysis. Although there was no detectable statistically significant interaction between aspirin use and ACEI use or lliD etiology with respect to all-cause mortality, the results of the stratified analyses are suggestive. First, there was a trend toward benefit from aspirin in those patients taking ACE inhibitors, and a trend toward larger benefit in patients not taking ACEI. The point estimates suggested a 24% reduction in the ACEI group and a 39% reduction in the non-ACEI group (full details in Table 6). Although these results must be interpreted with caution, the trend is still consistent with the hypothesis that ACEI use may lessen the benefit of aspirin use.
Second, there was a statistically significant 3 7% all-cause mortality benefit with aspirin use in patients with an lliD etiology, and a trend toward benefit from aspirin in patients with HF etiologies other than lliD. The point estimate for the non-lliD group suggested a 29% reduction in all-cause mortality. Again, these results must be interpreted with a great deal of caution due to the relatively wide confidence intervals.
m conflict, with some studies suggesting a benefit, while others suggest no benefit, or even harm. Examination of this patient population lends support to the proposition that addition of aspirin provides additional benefit over ACEI alone, although this additional benefit was unable to be demonstrated with statistical
significance at the p<0.05 level due to insufficient power.
The observed trend toward benefit with aspirin use m patients taking ACEI appears smaller than that observed in the patients not taking ACEI, consistent with the hypothesis that there is some negative interaction between ACEI use and the mortality benefit of aspirin. However, numbers in this category are relatively small, and the confidence interval is wide, so these results must be interpreted with caution. There was no statistically significant interaction term for the effect of ACEI use on the relationship between aspirin and mortality, but it is reasonable to believe that such an interaction may exist and that this study lacked sufficient power to demonstrate this effect.
Finally, the SOL VD subgroup analysis described previously suggests that the benefit of aspirin may be limited to patients with an lliD primary heart failure etiology. This current analysis of the relationship between etiology and the effect of aspirin on survival confirms a statistically significant mortality benefit with aspirin use in those patients with an lliD primary heart failure etiology, and
1 b "11 '- . 1 b fi . h . . " . HF
suggests a 1esser, ut st1 suustant1a1, ene1 t 1n t1 ose pattents w1tu a pnmary
In general, the differences between these results and those based on the SOL VD data are interesting, and do not all lend themselves to easy explanation. Certainly, this patient population was quite different from the SOL VD cohort. In addition to demographic differences, the UNC population was selected based on symptomatic HF rather than ejection fraction. In both the UNC and the SOL VD cohorts, as in all of the previously mentioned analyses, patients were not randomly assigned to aspirin, so unknown differences in baseline characteristics, might have existed and not been accounted for in the statistical analysis. In addition, patients in the UNC cohort were not randomized to ACEI. UNC patients were followed in a specialty heart failure clinic, which was not a common practice at the time of the SOL VD trials, and it is possible that we are to some extent seeing the effect of a difference in follow-up.
Additional limitations of the present study include the small sample size and non-standardized care. Furthermore, there have been substantial changes in the standard of care of HF patients over the time frame covered here, with the most obvious of these being the addition of beta-blocker therapy. The effect this may have on the observed benefit seen with aspirin use is not clear, but it is
possible that the protective effect of beta-blockade from an lliD standpoint may limit the additional benefit attributable to aspirin.
This study is retrospective and may suffer from some difficulties from
CONCLUSION
Multivariate, adjusted survival analysis indicates aspirin use at baseline was independently associated with reduced all-cause mortality in patients with symptomatic HF. The overall hazard ratio for aspirin use was 0.711 (95% CI 0.550-0.920), and the benefit of aspirin was apparently largely preserved in patients taking ACEI at baseline, where the HR for aspirin use was 0.758 (0.572-1.005). In patients with lliD as their primary HF etiology, the HR for aspirin use was 0.635 (0.442-0.911) compared to a HR of0.710 for those with a primary HF etiology other than lliD, suggesting that both groups can benefit from addition of aspirin.
The ideal follow-up study testing aspirin in heart failure and testing the potential aspirin-ACE! interaction would be a large randomized trial of aspirin vs. placebo. However, the growing body of secondary data supporting the use of aspirin in heart failure complicates the planning of further research. Not only may it be difficult ethically to randomize HF patients with lliD not to receive aspirin,
but also on a practical level, it would likely be very difficult to get physicians to agree to enroll patients.
If a large RCT of aspirin in HF is impractical, two other potential studies could be of benefit in this situation. First would be a trial of aspirin vs. clopidogrel, an antiplatelet agent acting through a different mechanism and unlikely to interact with ACEI. This trial could be performed in HF patients with
REFERENCES
1. Adams, K.F. and F. Zannad, Clinical definition of advanced heart failure. American Heart Journal, 1998. 135(6, part 2): p. S204-S215.
2. American Heart Association, 2002 Heart and Stroke Statistical Update. 2001, American Heart Association: Dallas, TX.
3. Adams, K.F., New epidemiologic perspectives concerning
mild-to-moderate heart failure. American Journal ofMedicine, 2001. 110(7A): p.
6S-12S.
4. Gheorghiade, M. and R.O. Bonow, Chronic heart failure in the United
States: a manifestation of coronary artery disease. Circulation, 1998. 97:
p. 282-289.
5. Adams, K.F., eta!., Ihe relation between gender, etiology, and survival in
patients with symptomatic heart failure. Journal of the American College
ofCardiology, 1996. 28: p. 1781-1788.
6. Bart, B.A., et al., Clinical determinants of mortality in patients with
angiographically diagnosed ischemic or nonischemic cardiomyopathy.
Journal of the American College of Cardiology, 1997. 30: p. 1002-1008. 7. Fuster, V., Badimon, and J.H. Cheseboro, Ihe pathogenesis of coronary
artery disease and the acute coronary syndromes. The New England
Journal ofMedicine, 1992. 326: p. 310-318.
9. Anti thrombotic Trialists' Collaboration, Collaborative meta-analysis of
randomised trials of antiplatelet therapy for prevention of death,
myocardial infarction, and stroke in high risk patients. British Medical
Journal, 2002. 324: p. 71-86.
10. Hayden, M., eta!., Aspirin for the primary prevention of cardiovascular
events: A summary of the evidence for the U.S. Preventive Services Task
Force. Annals oflnternal Medicine, 2002. 136(2): p. 161-172.
11. Peterson, J.G. and M.S. Lauer, Using aspirin and ACE inhibitors in
combination: Why the hullabaloo? Cleveland Clinic Journal of Medicine,
2001. 68(6): p. 569-574.
12. Peterson, J.G., eta!., Evaluation of the effects of aspirin combined with
angiotensin converting enzyme inhibitors in patients with coronary artery
disease. American Journal ofMedicine, 2000. 109: p. 371-377.
13. Stys, T., et a!., Does aspirin attenuate the beneficial effects of angiotensin
converting enzyme inhibition in heart failure? Archives oflnternal
Medicine, 2000. 160: p. 1409-1413.
14. Cleland, J.G.F., eta!. ,Is aspirin safe for patients with heart failure? British Heart Journal, 1995. 74: p. 215-219.
15. Cohn, J.N., eta!., A comparison ofenalaprilwith hydralazine-isosorbide
dinitrate in the treatment of chronic congestive heart failure. The New
16. The SOL VD Investigators, Effect of enalapril on survival in patients with
reduced left ventricular ejection fractions and congestive heart failure.
The New England Journal of Medicine, 1991. 325(5): p. 293-302. 17. The SOL VD Investigators, Effect of enalapril on mortality and the
development of heart failure in asymptomatic patients with reduced left
ventricular ejection fractions. The New England Journal of Medicine,
1992. 327(1 0): p. 685-691.
18. Yusuf, S., et al., Effect of enalapril on myocardial infarction and unstable
angina in patients with law ejection fractions. Lancet, 1992. 340(8820): p.
1173-1178.
19. Pfeffer, M.A., et al., Effect of captopril on mortality and morbidity in
patients with left ventricular dysfunction after myocardial infarction. The
New England Journal of Medicine, 1992. 327(10): p. 669-677.
20. The Acute Infarction Ramipril Efficacy (AIRE) Study Investigators, Effect
of ramipril on mortality and morbidity of survivors of acute myocardial
infarction with clinical evidence of heart failure. Lancet, 1993.342: p.
821-828.
21. Antiplatelet Trialists' Collaboration, Collaborative overview of
randomised trials of antiplatelet therapy 1: Prevention of death,
myocardial infarction, and stroke by prolonged antiplatelet therapy in
various categories of patients. British Medical Journal, 1994. 308: p.
22. ISIS-2 (Second International Study ofinfarct Survival) Collaborative Group, Randomised trial of intravenous streptokinase, oral aspirin, both,
or neither among I 7, I 87 cases of suspected acute myocardial infarction:
ISIS-2. Lancet, 1988. ii: p. 349-360.
23. Collaborative Group of the Primary Prevention Project, Low-dose aspirin
and vitamin E in people at cardiovascular risk: a randomised trial in
general practice. Lancet, 2001. 357: p. 89-95.
24. Swedberg, K., et al., Effects of the early administration of enalapril on
mortality in patients with acute myocardial infarction. The New England
Journal ofMedicine, 1992. 327(10): p. 678-683.
25. The Heart Outcomes Prevention Evaluation Study Investigators, Effects of
an angiotensin converting enzyme inhibitor, ramipril, on cardiovascular
events in high-risk patients. The New England Journal of Medicine, 2000.
342(3): p. 145-153.
26. Guazzi, M., et al., Improvement of alveolar-capillary membrane diffusing
capacity with enalapril in chronic heart failure and counteracting effect of
aspirin. Circulation, 1997. 95(7): p. 1930-1936.
27. van Wijngaarden, J., et al., Effects of acetylsalicylic acid on peripheral hemodynamics in patients with chronic heart failure treated with
angiotensin converting enzyme inhibitors. Journal of Cardiovascular
28. Aspirin Myocardial Infarction Study Research Group, A randomized,
controlled trial of aspirin in persons recovered from myocardial
infarction. JAMA, 1980. 243: p. 661-668.
29. Klimt, C.R., et al., Persantine Aspirin Reinfarction Study. Part II.
Secondary coronary prevention with persantine and aspirin. Journal of the
American College of Cardiology, 1986. 7: p. 251-269.
30. Wei!, J., et al., Prophylactic use of aspirin and risk of peptic ulcer
bleeding. British Medical Journal, 1995. 310: p. 827-830.
31. Hall, D., H. Zeitler, and W. Rudolph, Counteraction of the vasodilator
effects of enalapril by aspirin in severe heart failure. Journal of the
American College of Cardiology, 1992. 20(7): p. 1549-1555. 32. Guazzi, M., G. Pontone, and P. Agostoni, Aspirin worsens exercise
performance and pulmonary gas exchange in patients with heart failure
who are taking angiotensin-converting enzyme inhibitors. American Heart
Journal, 1999. 138(2, part 1): p. 254-260.
33. Evans, M.A., J.C. Burnett, and M.M. Redfield, Effect of low dose aspirin
on cardiorenal function and acute hemodynamic response to enalaprilat
in a canine model of severe heart failure. Journal of the American College
of Cardiology, 1995. 25(6): p. 1445-1450.
34. AJ-Khadra, A.S., et al., Antip!atelet agents and survival: A cohort analysis
from the studies of left ventricular dysfunction (SOLVD) trial. Journal of
35. Oosterga, M., eta!., Effects of aspirin on angiotensin-converting enzyme
inhibition and left ventricular dilation one year after acute myocardial
infarction. American Journal of Cardiology, 1998. 81: p. 1178-1181.
36. Lee, T.E., Nonparametric methods of estimating survival functions, in
Statistical Methods for Survival Data Analysis. 1980, Lifetime Learning
Publications: Belmont, CA. p. 75-87.
37. Cox, D.R., Regression models and life-tables. J R Stat Soc [B], 1972. 34:
L
E