Clinical Ophthalmology
Dove
press
R e v i e w
open access to scientific and medical research
Open Access Full Text Article
Spotlight on reticular pseudodrusen
Alessandro Rabiolo1
Riccardo Sacconi1,2
Maria vittoria Cicinelli1
Lea Querques1,3
Francesco Bandello1
Giuseppe Querques1
1Department of Ophthalmology,
University vita-Salute, iRCCS San Raffaele, Milan, 2eye Clinic,
Department of Neurological and Movement Sciences, University of verona, verona, 3G. B. Bietti
Foundation-iRCCS, Rome, italy
Abstract: Age-related macular degeneration (AMD) is a leading cause of vision loss in patients .50 years old. The hallmark of the disease is represented by the accumulation of extracellular material between retinal pigment epithelium and the inner collagenous layer of Bruch’s membrane, called drusen. Although identified almost 30 years ago, reticular pseudod-rusen (RPD) have been recently recognized as a distinctive phenotype. Unlike dpseudod-rusen, they are located in the subretinal space. RPD are strongly associated with late AMD, especially geographic atrophy, type 2 and 3 choroidal neovascularization, which, in turn, are less common in typical AMD. RPD identification is not straightforward at fundus examination, and their identification should employ at least 2 different imaging modalities. In this narrative review, we embrace all aspects of RPD, including history, epidemiology, histology, imaging, functional test, natural history and therapy.
Keywords: age-related macular degeneration, choroidal neovascularization, geographic atrophy, reticular macular degeneration, reticular drusen, reticular macular disease, reticular pseudodrusen, subretinal drusenoid deposit
Introduction
Age-related macular degeneration (AMD) is a chronic, progressive degenerative retinal disease characterized by loss of central vision and represents one of the leading causes of blindness in subjects .50 years old.1 Being a distinctive feature of AMD, drusen
appear on fundus examination as focal yellowish dots clustered at the posterior pole and are constituted by extracellular material accumulation between retinal pigment epithelium (RPE) and the inner collagenous layer of Bruch’s membrane (BM).1
In recent times, a distinctive phenotype, called reticular pseudodrusen (RPD), has been in the spotlight.
Here, we aim to provide the reader a comprehensive narrative review embracing all aspects of RPD.
Literature search
A PubMed engine search was carried out using the terms “reticular pseudodrusen”, “reticular drusen”, “subretinal drusenoid deposits”, and “reticular macular disease”. All studies published in English up to July 2017, irrespective of their publication status, were reviewed and relevant publications were included in this review.
History
Mimoun et al2 described for the first time “pseudodrusen visible en lumière bleue” in
1990 to define retinal lesions with a variable diameter of about 100 μm that did not appear hyperfluorescent on fluorescein angiography (FA), but with enhanced visibility in blue light. In 1991, RPD were incorporated into the Wisconsin AMD grading system
Correspondence: Giuseppe Querques Department of Ophthalmology, University vita-Salute, iRCCS San Raffaele, via Olgettina 60, Milan, 20132, italy
Tel +39 022 643 2648 Fax +39 022 643 3643
email [email protected]
Journal name: Clinical Ophthalmology Article Designation: Review Year: 2017
Volume: 11
Running head verso: Rabiolo et al Running head recto: Spotlight on RPD DOI: http://dx.doi.org/10.2147/OPTH.S130165
Clinical Ophthalmology downloaded from https://www.dovepress.com/ by 118.70.13.36 on 21-Aug-2020
For personal use only.
Number of times this article has been viewed
This article was published in the following Dove Press journal: Clinical Ophthalmology
Dovepress
Rabiolo et al
as “ill-defined networks of broad interlacing ribbons” on color fundus photography and were named reticular soft drusen.3
In 1995, Arnold et al4 further characterized RPD as “yellow
interlacing network 125–250 μm wide appearing first in the superior outer macula and then extending circumferentially and beyond” and coined the terminology RPD. Since then, the nomenclature RPD spread in the current literature, although other terms (ie, subretinal drusenoid deposits, reticular macu-lar disease, reticumacu-lar drusen) have been used.
epidemiology
Prevalence
Prevalence of RPD varies in relation to the modality of evalu-ation and the cohort of patients enrolled. Prevalence of RPD in general elder population was assessed by large, long-term follow-up prospective studies, namely, Beaver Dam Eye, Blue Mountains Eye and Melbourne Collaborative Cohort studies.5–7 In those studies, the prevalence of RPD turned to
be 0.41%–1.95% and 3.0%–4.0% at baseline and 15 years, respectively.5–7 However, the sensitivity of color fundus
pho-tography is very low. Conversely, novel imaging modalities (ie, spectral-domain optical coherence tomography [SD-OCT], infrared [IR] reflectivity and multicolor) exhibited excellent sensitivity/specificity, and, therefore, studies employing these modalities disclosed higher prevalence of RPD.8 In the Rotterdam Eye Study, RPD were detected in
about 5% of participants using color fundus photograph (CFP) and near-infrared reflectance (NIR).9 Prevalence of RPD was
even higher ranging from 13.4% to 32% when multimodal imaging was employed.10,11 Interestingly, RPD seem to be
less frequent in Asiatic compared with White populations.12
RPD are bilateral in 50%–84% of cases.6,13–15
Independently from the macular status, the presence of RPD in older population increased 3.4-fold the chance to suffer from AMD in general elder population.11 Prevalence
of RPD in patients with AMD is obviously higher than that in general population, ranging from 16.8% to 79%, depending on the imaging modality used, stage and type of AMD.8,11,16–20 Surprisingly, RPD prevalence was even higher
(85%) in postmortem histological samples of patients with AMD.21 Although their overall presence in neovascular AMD
ranges between 22% and 36%, RPD are more easily found in eyes with type 3 choroidal neovascularization (CNV) (68.4%–83%). Conversely, they are less commonly seen in eyes with typical neovascular AMD (type 1 and 2) or polypoi-dal choroipolypoi-dal vasculopathy with a prevalence of 9%–13.9% and 2%–3.4%, respectively.17,19,22,23 In eyes with geographic
atrophy, the prevalence of RPD ranges between 29% and
50%.14,17 An association between RPD and acquired
vitelli-form detachment has been reported, suggesting RPE dysfunc-tion and impairment to outer segments turnover.24,25
Although RPD are commonly found in AMD, they have also been associated with other retinal affections, including early-onset drusen,26 pseudoxanthoma elasticum,27,28 Sorsby
macular dystrophy29 and adult-onset foveomacular
vitel-liform dystrophy.30 RPD have been anecdotally reported in
late-onset macular degeneration,31 vitamin A deficiency32
and IgA nephropathy.33
Risk factors
RPD occur in the setting of AMD, and, therefore, phenotypic features of AMD are associated with higher risk of RPD presence. Patients with late AMD have the highest odds of having RPD, and the risk is greater in the geographic atrophy (GA) over the CNV phenotype, followed by intermediate and early stages.4,5,34,35 Large drusen and focal pigmentary
changes are additional risk factors for RPD presence.5 AMD
and RPD share several non-ocular risk factors, including older age,5–7,36 female sex,5,7,19,36 current smoking6,7 and high
body mass index.6 Other reported risk factors for RPD include
less education,7 B-vitamin complex use,7 history of steroid
eye drop use7 and glaucoma.7 As for AMD, the prevalence
of RPD is lower in patients with diabetes.7,37 In the Beaver
Dam Eye Study,7 RPD were an independent risk factor for
mortality, and Cymerman et al38 have recently reported higher
prevalence of RPD in patients with coronary artery disease. Compared with AMD without RPD, patients with RPD dem-onstrated higher rates of systemic hypertension, angina and mortality.39 However, this association is still under debate,
and other studies did not confirm association between RPD and cardiovascular risk factors.40,41 Decreased renal function
represents another vascular association; interestingly, both choroid and kidney share a lobular, end-arterial vascular system, and this could account for this connection.42
With the advent of the enhanced depth imaging (EDI)- and swept-source (SS)-OCT, several studies focused on the choroidal imaging. A reduction of the subfoveal choroidal thickness has been extensively demonstrated in patients with RPD when compared not only with healthy subjects but also with AMD without RPD.43–46 Also, choroidal
thin-ning involves all the macula area and even areas outside the macula, such as in the peripapillary region, suggesting a widespread choroidal involvement.47–50 Employing
chor-oidal binarization, Corvi et al51 showed that stromal area is
more represented in patients suffering from AMD with RPD compared with those without RPD, suggesting a choroidal
Clinical Ophthalmology downloaded from https://www.dovepress.com/ by 118.70.13.36 on 21-Aug-2020
Dovepress Spotlight on RPD
vascular depletion and fibrotic replacement. Zheng et al52
illustrated choroidal vessel density reduction in eyes with RPD, suggesting that RPD may be a sign of choroidal vascu-lopathy. Interestingly, areas of lowest vessel density did not correspond to the location of thinnest choroid, and, therefore, RPD may be related to a global choroidal dysfunction lead-ing to choriocapillaris hypoperfusion, possibly indicatlead-ing an ocular sign of systemic vascular deficiency.52,53
Little is known regarding genetic susceptibility and RPD. Two major AMD risks alleles, namely, complement factor H (CHF, rs1061170) 402H on chromosome 1q32 and the age-related maculopathy susceptibility 2 (ARMS2, rs10490924) 69S on chromosome 10q26, have been pointed out by large studies.54–57 Data regarding RPD are
controver-sial. The Beaver Eye Study7 and the Blue Mountain Eye
Study6 revealed a linkage between RPD and both ARMS2
and CFH Y402H. Smith et al58 found ARMS2 and CHF
402H variant as a risk and protective factor, respectively. In the Melbourne Collaborative Cohort Study,5 the ARMS2
single-nucleotide polymorphism (SNP) rs10490924, HTRA1 SNPs rs11200638 and rs3793917, and CFH SNPs rs393955, rs1061170 and rs2274700 were linked to higher prevalence of RPD. Association between RPD and ARMS2 allele was also confirmed in Japanese population.17 Buitendijk et al9 found
CFH, C2/FB and ARMS2 to be associated with both RPD and soft drusen, whereas C3 was linked only to RPD.
Conversely, Puche et al40 did not find any genotypic
difference between AMD patients with and without RPD. Similarly, Boddu et al36 did not find any association between
RPD and both ARMS2 and CHF alleles.
Histology
Different from drusen, which are made of lipids gathering in the BM (basal deposits), RPD are histologically character-ized by the accumulation of material in the subretinal space extending up to the outer segment and even in the outer nuclear layers.59,60 Neighboring structures are affected by the
presence of RPD, which is associated with RPE polymegath-ism, photoreceptor disruption and reactive gliosis.60
Although RPD have some similarities with drusen in their composition (ie, neutral lipid, cholesterol, amyloid, comple-ment factor, and membranous debris), they have significant differences in their components, and, therefore, RPD are not just drusen material located above the RPE.60–63 RPD have
higher concentration of unesterified cholesterol, vitronectin, include opsins, peanut agglutinin, and photoreceptor pigments (including precursors of A2E/lipofuscin).60–63 Since RPD and
drusen lipids did not stain with the same dye, differences
in lipid composition have been postulated.60 Moreover,
RPD are rich in immune cells, predominantly immune-reactive microglia and macrophages, confirming the role of inflammation.60 However, precise composition of RPD is
yet to be determined.
imaging
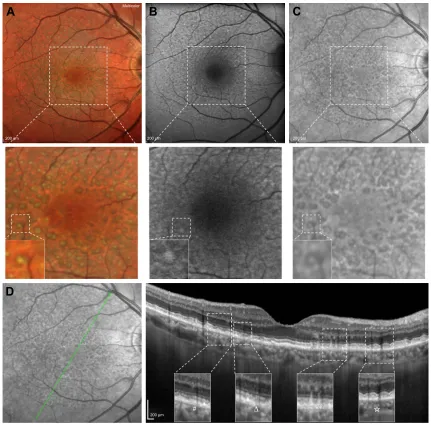
Different imaging modalities alone or in combination have been used to investigate RPD, including CFP, IR, short wave-length (SW)- and NIR-fundus autofluorescence (FAF), multicolor, OCT, en face OCT, OCT angiography (OCT-A), FA, indocyanine green angiography (ICGA) and adaptive optics.63 Figure 1 shows multimodal imaging of an eye
with RPD. Written informed consent was received from all patients for publication of images in this review.
Multimodal imaging studies revealed that IR, FAF, SD-OCT and widefield en face SS-OCT have the highest sensitivity in detecting RPD, whereas late phases of ICGA, blue channel of CFP and confocal blue reflectance (CBR) have almost perfect specificity.14,18,64 However, there is no real
gold standard for PRD detection, and use of at least 2 imaging modalities has been advocated.65 It has been suggested to use a
high sensible modality (ie, SD-OCT, IR) as a screening test and a high specific one (ie, ICGA, CFP, CBR) as confirmation.18
Color fundus photograph
CFP reveals RPD as yellowish, ill-defined network of broad, interlacing ribbons preferentially located in the superior aspect of the macular area, which tends to become more punctate as they become closer to the fovea.59,66 The blue
channel of CFP allows better contrast of RPD since the SW of blue light is highly reflected by the RPD, but preferentially absorbed by melanin contained in the RPE surrounding the RPD, creating contrast.18 Although some milestone studies5–7
employed CFP to individuate RPD, the diagnostic ability of this technique is unsatisfactory, due to the low sensitivity.18
On the contrary, its specificity is extremely high, virtually reaching 100%, and, therefore, it could be a powerful confirmatory test.18
Fundus autofluorescence
SW-FAF (excitation λ=488 nm; emission λ.500 nm) reveals RPD as hypofluorescent.23,35,67–69 The reason why RPD appear
as hypofluorescent is still uncertain.18,70 One possible
explana-tion is that the reflecexplana-tion and blockage of the blue excitaexplana-tion light prevent it from reaching the RPE.
On the other hand, most RPD deposits/subretinal materials may have an isofluorescent core conferring to these lesions a
Clinical Ophthalmology downloaded from https://www.dovepress.com/ by 118.70.13.36 on 21-Aug-2020
Dovepress
Rabiolo et al
“target aspect”.24 This peculiar aspect could derive from the
accumulation in the RPD core of lipofuscin-like material, probably representing unphagocytized photoreceptor outer segments; alternatively, it could be related to the interruption of ellipsoid zone (EZ).24 The absence of the target aspect in
some RPD could be ascribed to heterogeneity in RPD compo-sition or confocal selective laser ophthalmoscopy properties.24
Interestingly, a small subset of patients may have intense hyperfluorescent RPD, which have been initially reported
as less associated with late AMD,71 even though it was not
confirmed by later analysis.71,72 It has been speculated that
hyperfluorescent RPD could be a transient form of pseudod-rusen or small foci of acquired vitelliform material.71 RPD
extent increases over time, and it has been estimated to have a mean growth rate of 4.4 mm2/year.73 Using quantitative
FAF (qFAF), it has been observed that eyes with RPD have lower qFAF values compared with patients with soft drusen, cuticular drusen and controls even in unaffected retina areas.74
Figure 1 Multicolor imaging, FAF, iR and SD-OCT of a patient affected by RPD.
Notes: (A) Multicolor imaging showing a yellowish–green reticular pattern and some RPD with a target appearance characterized by a more intense yellowish/greenish core surrounded by a decreased intensity. (B) Blue FAF showing RPD as hypoautofluorescent dots surrounded by a faint hyperautofluorescent halo. Several RPD have a isoautofluorescent core, conferring a target aspect. (C) IR showing RPD as small lesions clustered in a reticular pattern and a variable target aspect, with an isoreflective core surrounded by hyporeflective halo. (D) Combined IR and structural SD-OCT B-scan passing through the fovea showing RPD as discrete accumulation of hyperreflective material above the RPE in the subretinal space. Green arrow shows the position of the scan lines used to generate the cross-sectional SD-OCT images. Magnifications showing an example of four different stages of RPD: 1) diffuse accumulation of granular hyperreflective material between RPE and EZ (hash); 2) mounds of material bowing and distorting EZ profile (star); 3) conical accumulations with focal interruption of EZ (asterisk); 4) drusenoid material reabsorption and migration in inner retinal layers (triangle).
Abbreviations: FAF, fundus autofluorescence; IR, infrared reflectivity; SD-OCT, spectral-domain optical coherence tomography; RPD, reticular pseudodrusen; RPE, retinal pigment epithelium; EZ, ellipsoid zone.
$
P P P
P ¨
'
%
&
0XOWLFRORU
Clinical Ophthalmology downloaded from https://www.dovepress.com/ by 118.70.13.36 on 21-Aug-2020
Dovepress Spotlight on RPD
Reduced qFAF values could reflect reduction in (intracellular but not extracellular) lipofuscin accumulation due to dysfunc-tion in choroid-BM-RPE complex, slowing in visual cycle, reduced cone and rode densities and different composition of lipofuscin.74 Since it is rapid, noninvasive, highly reliable,
accurate (sensitivity: 86%, specificity: 92%–95%), SW-FAF is a valuable imaging modality to identify RPD.18,68,75
Conversely, NIR-FAF (excitation λ=787 nm; emission
λ.800 nm) has not good diagnostic abilities.18
iR and multicolor
RPD appearance at IR imaging parallels FAF showing a hypo-reflective reticular pattern and a variable target aspect, with an isoreflective core surrounded by hyporeflective halo.24,35,73,76
Using multimodal imaging (including CFP, IR and OCT), Suzuki et al66 subclassified RPD in 3 different subtypes:
dot, ribbon and midperipheral. In the first type, IR reveals perifoveal hyporeflective dots often showing a target aspect; the second type is characterized by perifoveal faint hypore-flective ribbons; and the third subtype is featured by mid-peripheral hyperreflective spots.66 Different RPD subtypes
may have distinct components and may confer differing risk of disease progression.66 Since it is noninvasive, fast, high
sensible and reliable, IR imaging has been advocated as a screening test to identify RPD.18
MultiColor (Spectralis SD-OCT; Heidelberg Engineering, Heidelberg, Germany) merges 3 different laser channels (ie, IR: λ=820 nm; green reflectance: λ=515 nm; blue reflectance at λ=488 nm) into a single pseudocolor image. RPD have a peculiar yellowish-green reticular pattern and are more evident at green and IR than at blue reflectance.77
Similar to IR, RPD may have a target appearance with a more intense yellowish/greenish core surrounded by a decreased intensity.75,77 MultiColor demonstrated equal identification
rates of FAF and IR and higher individuation of target aspect.75,78 The green–blue enhanced mode, which stresses
blue and green channels, reveals RPD as green/gray lesions, but has lower detection rates than standard MultiColor, con-firming the value of the IR component.75
OCT, en face OCT and OCT-A
SD-OCT shows RPD as discrete accumulation of hyper-reflective material above the RPE in the subretinal space.79,80
Although contradicted by some studies, it is widely accepted that that hyperreflective subretinal drusenoid material seen at SD-OCT corresponds to RPD seen at other imaging modalities.15,76,80,81 Zweifel et al80 cataloged RPD in 3 different
stages: 1) diffuse accumulation of granular hyperreflective
material between RPE and EZ, 2) mounds of material bowing and distorting EZ profile and 3) conical amassing with focal interruption of EZ. Subsequently, Querques et al79 elucidated
that RPD are dynamic structures characterized by agglomera-tion of subretinal material; moreover, they illustrated that the drusenoid material eventually reabsorbs and migrates into the inner retinal layers, and this was referred to as stage 4. Auge et al82 confirmed the dynamism of RPD and emphasized the
importance of dense scan protocols and exact registration of B-scans in the follow-up. Advanced stages of pseudodrusen life cycle are associated with sublesional RPE degeneration and shortening of photoreceptors.83 Small series reported
that RPD can completely disappear during the time, and this phenomenon may be unilateral and asymmetric.84 RPD
disappearance may leave outer retinal atrophy and focal reduction in choroidal thickness, and this could represent a novel phenotype of late AMD not included in the current classification systems.85 It has been speculated that outer
retinal atrophy following RPD regression may eventually involve RPE and choriocapillaris, leading to GA.86
As previously discussed, several studies using EDI- and SS-OCT demonstrated that eyes with RPD are characterized by choroidal vascular depletion and fibrotic replacement, resulting in a widespread reduction in choroidal thickness even in comparison with other AMD phenotypes.43–52 Mrejen
and Spaide87 observed that RPD have low prevalence in
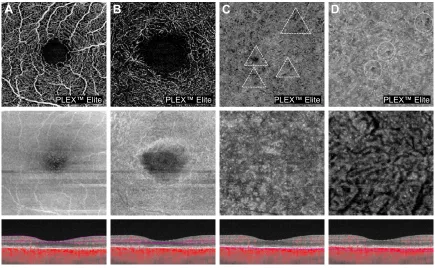
eyes with very thin choroid (ie, pathologic myopia), and, therefore, they argued that RPD accumulation is unlikely to be related to a primary dysfunction at the choroidal level, but rather explained by other factors (eg, RPE dysfunction). However, this argument fails to consider that the thin choroid in high myopia can be functionally and structurally healthy, compatible with normal visual function. Interestingly, high prevalence of RPD has been reported in eyes suffering from age-related choroidal atrophy, which is an entity recently described characterized by choroidal thickness reduction, pigmentary changes and scarcity of visible choroidal ves-sels, reflecting a disease of small vessels involving the chor-oid.88 Using OCT-A (Figure 2), eyes with RPD exhibited a
reduction in choriocapillary vessel density more extensive than in those with drusen and no RPD and which has been associated with poor visual acuity.89–91
SD-OCT has excellent diagnostic properties and reliabil-ity in identification of RPD.18 Schaal et al64,92 demonstrated
that en face OCT can image RPD, and this methodology alone has similar diagnostic abilities of conventional multi-modal imaging (ie, CFP, IR and FAF). Polarization-sensitive (PS)-OCT is able to provide more contrast for structures,
Clinical Ophthalmology downloaded from https://www.dovepress.com/ by 118.70.13.36 on 21-Aug-2020
Dovepress
Rabiolo et al
such as RPE, that are able to alter the polarization state of the light.93 PS-OCT can identify RPD, which preserve
polariza-tion, and distinguish them from drusen, which, conversely, alter polarization.94 However, PS-OCT has not broken into
the clinical practice, and its diagnostic properties are still unknown.
In addition to RPD identification, some authors have tried to determine whether OCT could provide information on the natural history of the disease. RPD thickness was a robust biomarker of future areas of GA growth.95–97 Moreover, EZ
disruption pattern has been related to GA progression over time.98 Identification of biomarkers and anatomic surrogates
predicting future vision loss could be beneficial for clinical trials concerning early or intermediate AMD.99
FA and iCGA
FA may reveal RPD as a filling defect in the choriocapillaris in early frames; however, due to its low sensitivity and inva-sive nature, it is seldom performed.63
RPD are seen as hypofluorescent dots at mid and late phases of ICGA, which co-localize with dots seen at IR and FAF, suggesting a pathology internal to RPE.14,100 Using IR
and ICGA, Querques et al44 showed that RPD co-localize
with choroidal intervascular stroma with sparing of areas above large choroidal vessels, suggesting impaired choroidal filling. Similarly, Alten et al101 observed that RPD are located
in areas of choroidal watershed, reinforcing the pathogenic role of choroidal hypoxia. However, further study did not find concordance between RPD and large choroidal blood vessels.102 Although it owns good diagnostic abilities
(sensi-tivity: 73%, specificity: 100%), ICGA is not the first choice test because of its invasive nature.18 As shown in Figure 3,
FA and ICGA have a pivotal role in diagnosing CNV associ-ated with RPD.
Adaptive optics
By improving the transverse resolution to 2 μm, adaptive optics visualize cone photoreceptors in vivo. Adaptive optics illustrate RPD as isoreflective lesions surrounded by a con-tinuous/discontinuous hyporeflective halo, with the hyper-reflective core ascribed to the drusenoid material itself and the hyporeflective halo related to absent or degenerated pho-toreceptors correspondent to EZ disruption.103 Photo receptors
mosaic is perturbed by RPD according to lesion stage; spe-cifically, stages 1 and 2 are characterized by a reduction in photoreceptor density, whereas only stage 3 has an annular
$
%
3/(;(OLWH 3/(;(OLWH 3/(;(OLWH
3/(;(OLWH
&
'
Figure 2 OCT-A of a patient affected by RPD.
Notes: (A, B) Superficial and deep capillary plexuses (A and B, respectively), corresponding en-face OCT and B-scan with flow showing no significant alterations. (C, D) Choriocapillaris and choroidal segmentation (C and D, respectively) showing choriocapillaris and choroidal impairment of the vessel density (dashed triangles and circles, respectively). Measurement: 3×3 mm OCT-A.
Abbreviations: OCT-A, optical coherence tomography angiography; RPD, reticular pseudodrusen; OCT, optical coherence tomography.
Clinical Ophthalmology downloaded from https://www.dovepress.com/ by 118.70.13.36 on 21-Aug-2020
Dovepress Spotlight on RPD
P
0XOWLFRORU
P P
P P
P
P
P
$
%
&
)
(
'
*
+
Figure 3 Multicolor imaging, FA, fundus autofluorescence, ICGA and structural SD-OCT of a patient affected by RPD and a type 1 CNV.
Notes: (A, D) Multicolor imaging (A) and fundus autofluorescence (D) showing RPD, a large hemorrhage around the central lesion. FA (B, C) and iCGA (E, F) revealing the presence of a type 1 CNV with a typical hyperfluorescent plaque in the late phase of ICGA (F). (G, H) Combined iCGA and structural horizontal and vertical SD-OCT B-scans passing through the fovea revealing the presence of RPD and an active type 1 CNv. Green arrows show the position of the scan lines used to generate the cross-sectional SD-OCT images.
Abbreviations: FA, fluorescein angiography; ICGA, indocyanine green angiography; SD-OCT, spectral-domain optical coherence tomography; RPD, reticular pseudodrusen; CNv, choroidal neovascularization.
Clinical Ophthalmology downloaded from https://www.dovepress.com/ by 118.70.13.36 on 21-Aug-2020
Dovepress
Rabiolo et al
configuration.104,105 As shown by OCT studies, dynamism of
RPD was further confirmed using adaptive optics.106
Mrejen et al107 showed that cone density over and around
RPD is lower than drusen and healthy controls, suggesting that RPD could affect retinal function even in the absence of CNV or GA. On the contrary, Querques et al103 found that
cone density similarly decreased in drusen and RPD.
Functional tests
AMD is characterized by abnormal retinal function even in early or intermediate stage. Impairment in dark adaption and low-luminance visual acuity have been demonstrated in AMD, and these parameters are more severely affected by the presence of RPD potentially reflecting impairment in rod function.68,108,109
In agreement with this hypothesis, Steinberg et al110 illustrated
a more pronounced deterioration of mean threshold sensitivity at scotopic than at photopic microperimetry. A recent study comparing eyes in normal macular health with and without RPD illustrated no significant difference regarding photopic acuity, mesopic acuity, low-luminance acuity, photopic con-trast sensitivity and photopic light sensitivity.111 In the same
study, eyes with RPD exhibited delayed dark adaptation, although significant differences in age between the 2 groups could be imputable for such a difference.111
Eyes with RPD have reduction in microperimetric retinal sensitivity despite preserved visual acuity.112 Compared with
drusen, RPD are associated with a more pronounced impair-ment in macular sensitivity.113 Whether the extent of RPD is
related to macular sensitivity is still unclear and contrasting results have been published.114,115
By recording local electroretinographic responses from the central 40°–50° of the macula, multifocal electroretino-graphy (mfERG) allows assessing retinal function in a topo-graphic way. Studies involving mfERG reported contrasting results.115–117 Alten et al116,117 did not find any significant
differ-ence between patients with RPD and healthy controls. Com-paring areas with and without pseudodrusen, they observed no significant differences at baseline; conversely, reduction in amplitude was seen in affected areas during the follow-up, suggesting a progressive decline in retinal function over time, which did not correlate with structural data.116,117 Wu et al115
reported conflicting results, showing that RPD presence and extent in intermediate AMD are independently linked to worse mfERG implicit time, but not to amplitude.
Natural history
As illustrated in the aforementioned paragraphs, RPD are dynamic structures evolving and even reabsorbing with time. RPD confer a higher risk of developing AMD during
follow-up. In elder population with an otherwise healthy macula, RPD were found in the 25% of subjects conferring a 2-fold risk to develop early AMD.118 In addition, the presence
of RPD increase is significantly associated with higher odds to progress to late AMD.6,119 In fellow eyes of patients with
unilateral CNV, the presence of AMD conferred extra odds to progress to late AMD.34 RPD are linked to the development
of GA, especially with multilobular type, and higher progres-sion rates.96,97,120 RPD are a strong risk factor for developing
type 3 CNV, and, moreover, they are associated with higher earlier onset and bilateral disease.121,122 Eyes affected by
type 3 CNV have higher odds to have also RPD, and, for this reason, RPD have been advocated as a diagnostic sign to distinguish type 3 CNV from other forms.123,124 Eyes with
exclusively RPD have been associated with type 2 CNV.125
In case of CNV development, RPD fade nearby the CNV itself, but they may still be observed more peripherally.14,69
RPD are a risk factor to develop atrophy following intra-vitreal anti-vascular endothelial growth factor (VEGF).126–128
However, presence of RPD did not interfere with the response to intravitreal anti-VEGF, at least in the short term.129
Therapy
No specific therapy is available for RPD. Since RPD are in the spectrum of AMD, they can benefit from vitamin supple-mentation (ie, AREDS and AREDS2 formula) in case of early and intermediate diseases.130 Beyond reducing the risk of late
AMD development, supplementation with macular pigment component (ie, lutein, zeaxanthin and meso-zeaxanthin) may increase the macular pigment optical density primarily, if not only, in the RPD phenotype.131 Presence of RPD in the setting
of late AMD has no impact on the therapeutic strategy.
Conclusions
RPD represent a specific component of AMD, although they may be found even in other ocular diseases. They differ from drusen not only for their location (ie, subretinal space) but also for their components. Their presence should always be sought in patients suffering from AMD, since they are strongly associated with late stages of disease. RPD identifi-cation should employ at least 2 different imaging modalities, since their recognition may not be straightforward with one technique only. Future clinical trials and epidemiological studies should take into account RPD phenotype employing imaging modalities suitable for their identification.
Disclosure
GQ is a consultant for Alimera Sciences (Alpharetta, Georgia, USA), Allergan Inc. (Irvine, California, USA), Bayer
Clinical Ophthalmology downloaded from https://www.dovepress.com/ by 118.70.13.36 on 21-Aug-2020
Dovepress Spotlight on RPD
Schering-Pharma (Berlin, Germany), Heidelberg (Germany), Novartis (Basel, Switzerland), Sandoz (Berlin, Germany), Zeiss (Dublin, OH, USA). FB has the following disclosures: Allergan (s), Alimera (s), Bayer (s), Farmila-Thea (s), Scher-ing Pharma (s), Sanofi-Aventis (s), Novagali (s), Pharma (s), Hoffmann-La Roche (s), Genentech (s) and Novartis (s). The other authors report no conflicts of interest in this work.
References
1. Lim LS, Mitchell P, Seddon JM, Holz FG, Wong TY. Age-related macular degeneration. Lancet. 2012;379(9827):1728–1738.
2. Mimoun G, Soubrane G, Coscas G. Les drusen maculaires. [Macular drusen]. J Fr Ophtalmol. 1990;13(10):511–530. French.
3. Klein R, Davis MD, Magli YL, Segal P, Klein BE, Hubbard L. The Wisconsin age-related maculopathy grading system. Ophthalmology. 1991;98(7):1128–1134.
4. Arnold JJ, Sarks SH, Killingsworth MC, Sarks JP. Reticular pseudod-rusen. A risk factor in age-related maculopathy. Retina. 1995;15(3): 183–191.
5. Finger RP, Chong E, McGuinness MB, et al. Reticular Pseudodrusen and Their Association with Age-Related Macular Degeneration: The Melbourne Collaborative Cohort Study. Ophthalmology. 2016; 123(3):599–608.
6. Joachim N, Mitchell P, Rochtchina E, Tan AG, Wang JJ. Incidence and progression of reticular drusen in age-related macular degenera-tion: findings from an older Australian cohort. Ophthalmology. 2014; 121(4):917–925.
7. Klein R, Meuer SM, Knudtson MD, Iyengar SK, Klein BE. The epi-demiology of retinal reticular drusen. Am J Ophthalmol. 2008;145(2): 317–326.
8. De Bats F, Mathis T, Mauget-Faysse M, Joubert F, Denis P, Kodjikian L. Prevalence of reticular pseudodrusen in age-related macular degenera-tion using multimodal imaging. Retina. 2016;36(1):46–52.
9. Buitendijk GH, Hooghart AJ, Brussee C, et al. Epidemiology of reticular pseudodrusen in age-related macular degeneration: the Rotterdam study.
Invest Ophthalmol Vis Sci. 2016;57(13):5593–5601.
10. Chan H, Cougnard-Gregoire A, Delyfer MN, et al. Multimodal imag-ing of reticular pseudodrusen in a population-based settimag-ing: the alienor study. Invest Ophthalmol Vis Sci. 2016;57(7):3058–3065.
11. Zarubina AV, Neely DC, Clark ME, et al. Prevalence of subretinal druse-noid deposits in older persons with and without age-related macular degeneration, by multimodal imaging. Ophthalmology. 2016;123(5): 1090–1100.
12. Joachim N, Mitchell P, Younan C, et al. Ethnic variation in early age-related macular degeneration lesions between white Australians and Sin-gaporean Asians. Invest Ophthalmol Vis Sci. 2014;55(7):4421–4429. 13. Alten F, Clemens CR, Milojcic C, Eter N. Subretinal drusenoid deposits
associated with pigment epithelium detachment in age-related macular degeneration. Retina. 2012;32(9):1727–1732.
14. Smith RT, Sohrab MA, Busuioc M, Barile G. Reticular macular disease.
Am J Ophthalmol. 2009;148(5):733–743.e2.
15. Sohrab MA, Smith RT, Salehi-Had H, Sadda SR, Fawzi AA. Image registration and multimodal imaging of reticular pseudodrusen. Invest
Ophthalmol Vis Sci. 2011;52(8):5743–5748.
16. Cohen SY, Dubois L, Tadayoni R, Delahaye-Mazza C, Debibie C, Quentel G. Prevalence of reticular pseudodrusen in age-related macular degeneration with newly diagnosed choroidal neovascularisation.
Br J Ophthalmol. 2007;91(3):354–359.
17. Ueda-Arakawa N, Ooto S, Nakata I, et al. Prevalence and genomic association of reticular pseudodrusen in age-related macular degenera-tion. Am J Ophthalmol. 2013;155(2):260–269.e262.
18. Ueda-Arakawa N, Ooto S, Tsujikawa A, Yamashiro K, Oishi A, Yoshimura N. Sensitivity and specificity of detecting reticular pseudod-rusen in multimodal imaging in Japanese patients. Retina. 2013;33(3): 490–497.
19. Wilde C, Patel M, Lakshmanan A, Morales MA, Dhar-Munshi S, Amoaku WM. Prevalence of reticular pseudodrusen in eyes with newly presenting neovascular age-related macular degeneration.
Eur J Ophthalmol. 2016;26(2):128–134.
20. Wu Z, Ayton LN, Luu CD, Baird PN, Guymer RH. Reticular pseudod-rusen in intermediate age-related macular degeneration: prevalence, detection, clinical, environmental, and genetic associations. Invest
Ophthalmol Vis Sci. 2016;57(3):1310–1316.
21. Curcio CA, Messinger JD, Sloan KR, McGwin G, Medeiros NE, Spaide RF. Subretinal drusenoid deposits in non-neovascular age-related macular degeneration: morphology, prevalence, topography, and biogenesis model. Retina. 2013;33(2):265–276.
22. Kim JH, Chang YS, Kim JW, Lee TG, Kim CG. Prevalence of subtypes of reticular pseudodrusen in newly diagnosed exudative age-related macular degeneration and polypoidal choroidal vasculopathy in Korean patients. Retina. 2015;35(12):2604–2612.
23. Smith RT, Chan JK, Busuoic M, Sivagnanavel V, Bird AC, Chong NV. Autofluorescence characteristics of early, atrophic, and high-risk fellow eyes in age-related macular degeneration. Invest Ophthalmol Vis Sci. 2006;47(12):5495–5504.
24. Querques G, Querques L, Martinelli D, et al. Pathologic insights from integrated imaging of reticular pseudodrusen in age-related macular degeneration. Retina. 2011;31(3):518–526.
25. Zweifel SA, Spaide RF, Yannuzzi LA. Acquired vitelliform detachment in patients with subretinal drusenoid deposits (reticular pseudodrusen).
Retina. 2011;31(2):229–234.
26. De Bats F, Wolff B, Mauget-Faysse M, Meunier I, Denis P, Kodjikian L. Association of reticular pseudodrusen and early onset drusen. ISRN
Ophthalmol. 2013;2013:273085.
27. Gliem M, Muller PL, Birtel J, Hendig D, Holz FG, Charbel Issa P. Frequency, phenotypic characteristics and progression of atrophy associated with a diseased bruch’s membrane in pseudoxanthoma elasticum. Invest Ophthalmol Vis Sci. 2016;57(7):3323–3330. 28. Zweifel SA, Imamura Y, Freund KB, Spaide RF. Multimodal fundus
imaging of pseudoxanthoma elasticum. Retina. 2011;31(3):482–491. 29. Gliem M, Muller PL, Mangold E, et al. Reticular pseudodrusen in sorsby
fundus dystrophy. Ophthalmology. 2015;122(8):1555–1562. 30. Wilde C, Lakshmanan A, Patel M, Morales MU, Dhar-Munshi S,
Amoaku WM. Prevalence of reticular pseudodrusen in newly pre-senting adult onset foveomacular vitelliform dystrophy. Eye (Lond). 2016;30(6):817–824.
31. Cukras C, Flamendorf J, Wong WT, Ayyagari R, Cunningham D, Sieving PA. Longitudinal structural changes in late-onset retinal degeneration. Retina. 2016;36(12):2348–2356.
32. Aleman TS, Garrity ST, Brucker AJ. Retinal structure in vitamin A deficiency as explored with multimodal imaging. Doc Ophthalmol. 2013;127(3):239–243.
33. Lally DR, Baumal C. Subretinal drusenoid deposits associated with complement-mediated IgA nephropathy. JAMA Ophthalmol. 2014; 132(6):775–777.
34. Pumariega NM, Smith RT, Sohrab MA, Letien V, Souied EH. A prospec-tive study of reticular macular disease. Ophthalmology. 2011;118(8): 1619–1625.
35. Schmitz-Valckenberg S, Alten F, Steinberg JS, et al; Geographic Atrophy Progression (GAP) Study Group. Reticular drusen associated with geographic atrophy in age-related macular degeneration. Invest
Ophthalmol Vis Sci. 2011;52(9):5009–5015.
36. Boddu S, Lee MD, Marsiglia M, Marmor M, Freund KB, Smith RT. Risk factors associated with reticular pseudodrusen versus large soft drusen. Am J Ophthalmol. 2014;157(5):985–993.e2.
37. Cho BJ, Heo JW, Shin JP, Ahn J, Kim TW, Chung H. Epidemiological association between systemic diseases and age-related macular degen-eration: the Korea National Health and Nutrition Examination Survey 2008–2011. Invest Ophthalmol Vis Sci. 2014;55(7):4430–4437. 38. Cymerman RM, Skolnick AH, Cole WJ, Nabati C, Curcio CA, Smith RT.
Coronary artery disease and reticular macular disease, a subphenotype of early age-related macular degeneration. Curr Eye Res. 2016;41(11): 1482–1488.
Clinical Ophthalmology downloaded from https://www.dovepress.com/ by 118.70.13.36 on 21-Aug-2020
Dovepress
Rabiolo et al
39. Rastogi N, Smith RT. Association of age-related macular degenera-tion and reticular macular disease with cardiovascular disease. Surv
Ophthalmol. 2016;61(4):422–433.
40. Puche N, Blanco-Garavito R, Richard F, et al. Genetic and environ-mental factors associated with reticular pseudodrusen in age-related macular degeneration. Retina. 2013;33(5):998–1004.
41. McCarter RV, McKay GJ, Quinn NB, et al. Evaluation of coronary artery disease as a risk factor for reticular pseudodrusen. Br J Ophthalmol. Epub 2017 Aug 19.
42. Leisy HB, Ahmad M, Marmor M, Smith RT. Association between decreased renal function and reticular macular disease in age-related macular degeneration. Ophthalmology Retina. 2017;1(1):42–48. 43. Garg A, Oll M, Yzer S, et al. Reticular pseudodrusen in early age-related
macular degeneration are associated with choroidal thinning. Invest
Ophthalmol Vis Sci. 2013;54(10):7075–7081.
44. Querques G, Querques L, Forte R, Massamba N, Coscas F, Souied EH. Choroidal changes associated with reticular pseudodrusen. Invest
Ophthalmol Vis Sci. 2012;53(3):1258–1263.
45. Thorell MR, Goldhardt R, Nunes RP, et al. Association between sub-foveal choroidal thickness, reticular pseudodrusen, and geographic atrophy in age-related macular degeneration. Ophthalmic Surg Lasers
Imaging Retina. 2015;46(5):513–521.
46. Switzer DW Jr, Mendonca LS, Saito M, Zweifel SA, Spaide RF. Segregation of ophthalmoscopic characteristics according to choroidal thickness in patients with early age-related macular degeneration.
Retina. 2012;32(7):1265–1271.
47. Yun C, Oh J, Ahn SE, Hwang SY, Kim SW, Huh K. Peripapillary choroidal thickness in patients with early age-related macular degenera-tion and reticular pseudodrusen. Graefes Arch Clin Exp Ophthalmol. 2016;254(3):427–435.
48. Haas P, Esmaeelpour M, Ansari-Shahrezaei S, Drexler W, Binder S. Choroidal thickness in patients with reticular pseudodrusen using 3D 1060-nm OCT maps. Invest Ophthalmol Vis Sci. 2014;55(4): 2674–2681.
49. Ueda-Arakawa N, Ooto S, Ellabban AA, et al. Macular choroidal thickness and volume of eyes with reticular pseudodrusen using swept-source optical coherence tomography. Am J Ophthalmol. 2014;157(5): 994–1004.
50. Capuano V, Souied EH, Miere A, Jung C, Costanzo E, Querques G. Choroidal maps in non-exudative age-related macular degeneration.
Br J Ophthalmol. 2016;100(5):677–682.
51. Corvi F, Souied EH, Capuano V, et al. Choroidal structure in eyes with drusen and reticular pseudodrusen determined by binarisation of optical coherence tomographic images. Br J Ophthalmol. 2017;101:348–352. 52. Zheng F, Gregori G, Schaal KB, et al. Choroidal thickness and chor-oidal vessel density in nonexudative age-related macular degeneration using swept-source optical coherence tomography imaging. Invest
Ophthalmol Vis Sci. 2016;57(14):6256–6264.
53. A Martillo M, Marsiglia M, D Lee M, Pumariega N, Bearelly S, Smith RT. Is reticular macular disease a choriocapillaris perfusion prob-lem? Med Hypothesis Discov Innov Ophthalmol. 2012;1(2):37–41. 54. Edwards AO, Ritter R 3rd, Abel KJ, Manning A, Panhuysen C,
Farrer LA. Complement factor H polymorphism and age-related macular degeneration. Science. 2005;308(5720):421–424.
55. Jakobsdottir J, Conley YP, Weeks DE, Mah TS, Ferrell RE, Gorin MB. Susceptibility genes for age-related maculopathy on chromosome 10q26. Am J Hum Genet. 2005;77(3):389–407.
56. Klein RJ, Zeiss C, Chew EY, et al. Complement factor H polymor-phism in age-related macular degeneration. Science. 2005;308(5720): 385–389.
57. Rivera A, Fisher SA, Fritsche LG, et al. Hypothetical LOC387715 is a second major susceptibility gene for age-related macular degeneration, contributing independently of complement factor H to disease risk.
Hum Mol Genet. 2005;14(21):3227–3236.
58. Smith RT, Merriam JE, Sohrab MA, et al. Complement factor H 402H variant and reticular macular disease. Arch Ophthalmol. 2011;129(8): 1061–1066.
59. Khan KN, Mahroo OA, Khan RS, et al. Differentiating drusen: Drusen and drusen-like appearances associated with ageing, age-related macular degeneration, inherited eye disease and other pathological processes.
Prog Retin Eye Res. 2016;53:70–106.
60. Greferath U, Guymer RH, Vessey KA, Brassington K, Fletcher EL. Correlation of histologic features with in vivo imaging of reticular pseudodrusen. Ophthalmology. 2016;123(6):1320–1331.
61. Curcio CA, Presley JB, Millican CL, Medeiros NE. Basal deposits and drusen in eyes with age-related maculopathy: evidence for solid lipid particles. Exp Eye Res. 2005;80(6):761–775.
62. Johnson LV, Leitner WP, Staples MK, Anderson DH. Complement activation and inflammatory processes in Drusen formation and age related macular degeneration. Exp Eye Res. 2001;73(6):887–896. 63. Sivaprasad S, Bird A, Nitiahpapand R, et al. Perspectives on reticular
pseudodrusen in age-related macular degeneration. Surv Ophthalmol. 2016;61(5):521–537.
64. Schaal KB, Legarreta AD, Feuer WJ, et al. Comparison between wide-field en face swept-source OCT and conventional multimodal imaging for the detection of reticular pseudodrusen. Ophthalmology. 2017; 124(2):205–214.
65. Alten F, Eter N. Current knowledge on reticular pseudodrusen in age-related macular degeneration. Br J Ophthalmol. 2015;99(6):717–722. 66. Suzuki M, Sato T, Spaide RF. Pseudodrusen subtypes as delineated
by multimodal imaging of the fundus. Am J Ophthalmol. 2014;157(5): 1005–1012.
67. Bindewald A, Bird AC, Dandekar SS, et al. Classification of fundus autofluorescence patterns in early age-related macular disease. Invest
Ophthalmol Vis Sci. 2005;46(9):3309–3314.
68. Hogg RE, Silva R, Staurenghi G, et al. Clinical characteristics of reticular pseudodrusen in the fellow eye of patients with unilateral neovascular age-related macular degeneration. Ophthalmology. 2014;121(9): 1748–1755.
69. Sarks J, Arnold J, Ho IV, Sarks S, Killingsworth M. Evolution of reticular pseudodrusen. Br J Ophthalmol. 2011;95(7):979–985. 70. Lois N, Owens SL, Coco R, Hopkins J, Fitzke FW, Bird AC. Fundus
autofluorescence in patients with age-related macular degeneration and high risk of visual loss. Am J Ophthalmol. 2002;133(3):341–349. 71. Lee MY, Ham DI. Subretinal drusenoid deposits with increased
autofluorescence in eyes with reticular pseudodrusen. Retina. 2014; 34(1):69–76.
72. Querques G, Souied EH. Correspondence. Retina. 2015;35(1):e4–e6. 73. Steinberg JS, Auge J, Jaffe GJ, Fleckenstein M, Holz FG, Schmitz-Valckenberg S; GAP Study Group. Longitudinal analysis of reticular drusen associated with geographic atrophy in age-related macular degeneration. Invest Ophthalmol Vis Sci. 2013;54(6):4054–4060. 74. Gliem M, Muller PL, Finger RP, McGuinness MB, Holz FG,
Charbel Issa P. Quantitative fundus autofluorescence in early and inter-mediate age-related macular degeneration. JAMA Ophthalmol. 2016; 134(7):817–824.
75. Alten F, Clemens CR, Heiduschka P, Eter N. Characterisation of reticular pseudodrusen and their central target aspect in multi-spectral, confocal scanning laser ophthalmoscopy. Graefes Arch Clin Exp
Ophthalmol. 2014;252(5):715–721.
76. Spaide RF. Colocalization of pseudodrusen and subretinal drusenoid deposits using high-density en face spectral domain optical coherence tomography. Retina. 2014;34(12):2336–2345.
77. Querques G, Srour M, Massamba N, Puche N, Souied EH. Reticular pseudodrusen. Ophthalmology. 2013;120(4):872.
78. Badal J, Biarnes M, Mones J. Performance characteristics of multicolor versus blue light and infrared imaging in the identification of reticular pseudodrusen. Int Ophthalmol. Epub 2017 Jan 21.
79. Querques G, Canoui-Poitrine F, Coscas F, et al. Analysis of progres-sion of reticular pseudodrusen by spectral domain-optical coherence tomography. Invest Ophthalmol Vis Sci. 2012;53(3):1264–1270. 80. Zweifel SA, Spaide RF, Curcio CA, Malek G, Imamura Y. Reticular
pseudodrusen are subretinal drusenoid deposits. Ophthalmology. 2010; 117(2):303–312. e1.
Clinical Ophthalmology downloaded from https://www.dovepress.com/ by 118.70.13.36 on 21-Aug-2020
Dovepress Spotlight on RPD
81. Heiferman MJ, Fernandes JK, Munk M, Mirza RG, Jampol LM, Fawzi AA. Reticular pseudodrusen on infrared imaging are topographi-cally distinct from subretinal drusenoid deposits on en face optical coherence tomography. Retina. 2015;35(12):2593–2603.
82. Auge J, Steinberg JS, Fleckenstein M, Holz FG, Schmitz-Valckenberg S. Retikuläre Drusen über die Zeit mittels SD-OCT. [Reticular drusen over time with SD-OCT]. Ophthalmologe. 2014;111(8):765–771. German. 83. Xu X, Liu X, Wang X, et al. Retinal pigment epithelium degeneration
associated with subretinal drusenoid deposits in age-related macular degeneration. Am J Ophthalmol. 2017;175:87–98.
84. Schick T, Ersoy L, Kirchhof B, Liakopoulos S. Asymmetrical behaviour of disappearance of reticular pseudodrusen in both eyes during long-term follow-up with spectral domain optical coherence tomography. GMS Ophthalmol Cases. 2014;4:Doc06.
85. Spaide RF. Outer retinal atrophy after regression of subretinal druse-noid deposits as a newly recognized form of late age-related macular degeneration. Retina. 2013;33(9):1800–1808.
86. Spaide RF. Improving the age-related macular degeneration construct: a new classification system. Retina. Epub 2017 May 26.
87. Mrejen S, Spaide RF. The relationship between pseudodrusen and choroidal thickness. Retina. 2014;34(8):1560–1566.
88. Spaide RF. Age-related choroidal atrophy. Am J Ophthalmol. 2009; 147(5):801–810.
89. Alten F, Heiduschka P, Clemens CR, Eter N. Exploring choriocapil-laris under reticular pseudodrusen using OCT-angiography. Graefes
Arch Clin Exp Ophthalmol. 2016;254(11):2165–2173.
90. Cicinelli MV, Rabiolo A, Marchese A, et al. Choroid morphometric analysis in non-neovascular age-related macular degeneration by means of optical coherence tomography angiography. Br J Ophthalmol. 2017;101(9):1193–1200.
91. Nesper PL, Soetikno BT, Fawzi AA. Choriocapillaris nonperfusion is associated with poor visual acuity in eyes with reticular pseudodrusen.
Am J Ophthalmol. 2017;174:42–55.
92. Schaal KB, Legarreta AD, Gregori G, et al. Widefield en face optical coherence tomography imaging of subretinal drusenoid deposits.
Ophthalmic Surg Lasers Imaging Retina. 2015;46(5):550–559.
93. Pircher M, Hitzenberger CK, Schmidt-Erfurth U. Polarization sensitive optical coherence tomography in the human eye. Prog Retin Eye Res. 2011;30(6):431–451.
94. Roberts PK, Baumann B, Schlanitz FG, et al. Retinal pigment epithelial features indicative of neovascular progression in age-related macular degeneration. Br J Ophthalmol. Epub 2017 Mar 7.
95. Niu S, de Sisternes L, Chen Q, Rubin DL, Leng T. Fully automated prediction of geographic atrophy growth using quantitative spectral-domain optical coherence tomography biomarkers. Ophthalmology. 2016;123(8):1737–1750.
96. Marsiglia M, Boddu S, Bearelly S, et al. Association between geo-graphic atrophy progression and reticular pseudodrusen in eyes with dry age-related macular degeneration. Invest Ophthalmol Vis Sci. 2013; 54(12):7362–7369.
97. Xu L, Blonska AM, Pumariega NM, et al. Reticular macular disease is associated with multilobular geographic atrophy in age-related macular degeneration. Retina. 2013;33(9):1850–1862.
98. Giocanti-Auregan A, Tadayoni R, Fajnkuchen F, Dourmad P, Magazzeni S, Cohen SY. Predictive value of outer retina en face OCT imaging for geographic atrophy progression. Invest Ophthalmol Vis
Sci. 2015;56(13):8325–8330.
99. Schaal KB, Rosenfeld PJ, Gregori G, Yehoshua Z, Feuer WJ. Ana-tomic clinical trial endpoints for nonexudative age-related macular degeneration. Ophthalmology. 2016;123(5):1060–1079.
100. Arnold JJ, Quaranta M, Soubrane G, Sarks SH, Coscas G. Indocya-nine green angiography of drusen. Am J Ophthalmol. 1997;124(3): 344–356.
101. Alten F, Clemens CR, Heiduschka P, Eter N. Localized reticular pseudodrusen and their topographic relation to choroidal watershed zones and changes in choroidal volumes. Invest Ophthalmol Vis Sci. 2013;54(5):3250–3257.
102. Vongkulsiri S, Ooto S, Mrejen S, Suzuki M, Spaide RF. The lack of concordance between subretinal drusenoid deposits and large choroidal blood vessels. Am J Ophthalmol. 2014;158(4):710–715.
103. Querques G, Kamami-Levy C, Blanco-Garavito R, et al. Appearance of medium-large drusen and reticular pseudodrusen on adaptive optics in age-related macular degeneration. Br J Ophthalmol. 2014; 98(11):1522–1527.
104. Zhang Y, Wang X, Rivero EB, et al. Photoreceptor perturbation around subretinal drusenoid deposits as revealed by adaptive optics scanning laser ophthalmoscopy. Am J Ophthalmol. 2014;158(3): 584–596.e1.
105. Meadway A, Wang X, Curcio CA, Zhang Y. Microstructure of subreti-nal drusenoid deposits revealed by adaptive optics imaging. Biomed
Opt Express. 2014;5(3):713–727.
106. Zhang Y, Wang X, Godara P, et al. Dynamism of dot subretinal drusenoid deposits in age-related macular degeneration demonstrated with adaptive optics imaging. Retina. Epub 2017 Feb 10.
107. Mrejen S, Sato T, Curcio CA, Spaide RF. Assessing the cone photore-ceptor mosaic in eyes with pseudodrusen and soft Drusen in vivo using adaptive optics imaging. Ophthalmology. 2014;121(2):545–551. 108. Flamendorf J, Agron E, Wong WT, et al. Impairments in dark
adaptation are associated with age-related macular degeneration severity and reticular pseudodrusen. Ophthalmology. 2015;122(10): 2053–2062.
109. Sevilla MB, McGwin G Jr, Lad EM, et al. Relating retinal morphology and function in aging and early to intermediate age-related macular degeneration subjects. Am J Ophthalmol. 2016;165:65–77. 110. Steinberg JS, Fitzke FW, Fimmers R, Fleckenstein M, Holz FG,
Schmitz-Valckenberg S. Scotopic and photopic microperimetry in patients with reticular drusen and age-related macular degeneration.
JAMA Ophthalmol. 2015;133(6):690–697.
111. Neely D, Zarubina AV, Clark ME, et al. Association between visual function and subretinal drusenoid deposits in normal and early age-related macular degeneration eyes. Retina. 2017;37(7):1329–1336. 112. Forte R, Cennamo G, de Crecchio G, Cennamo G. Microperimetry of
subretinal drusenoid deposits. Ophthalmic Res. 2014;51(1):32–36. 113. Querques G, Massamba N, Srour M, Boulanger E, Georges A,
Souied EH. Impact of reticular pseudodrusen on macular function.
Retina. 2014;34(2):321–329.
114. Ooto S, Ellabban AA, Ueda-Arakawa N, et al. Reduction of retinal sen-sitivity in eyes with reticular pseudodrusen. Am J Ophthalmol. 2013; 156(6):1184–1191.e2.
115. Wu Z, Ayton LN, Makeyeva G, Guymer RH, Luu CD. Impact of reticular pseudodrusen on microperimetry and multifocal electroretin-ography in intermediate age-related macular degeneration. Invest
Ophthalmol Vis Sci. 2015;56(3):2100–2106.
116. Alten F, Heiduschka P, Clemens CR, Eter N. Multifocal electroretinog-raphy in eyes with reticular pseudodrusen. Invest Ophthalmol Vis Sci. 2012;53(10):6263–6270.
117. Alten F, Heiduschka P, Clemens CR, Eter N. Longitudinal structure/ function analysis in reticular pseudodrusen. Invest Ophthalmol Vis Sci. 2014;55(9):6073–6081.
118. Huisingh C, McGwin G Jr, Neely D, et al. The association between subretinal drusenoid deposits in older adults in normal macular health and incident age-related macular degeneration. Invest Ophthalmol
Vis Sci. 2016;57(2):739–745.
119. Gil JQ, Marques JP, Hogg R, et al. Clinical features and long-term progression of reticular pseudodrusen in age-related macular degen-eration: findings from a multicenter cohort. Eye (Lond). 2017;31(3): 364–371.
120. Finger RP, Wu Z, Luu CD, et al. Reticular pseudodrusen: a risk factor for geographic atrophy in fellow eyes of individuals with uni-lateral choroidal neovascularization. Ophthalmology. 2014;121(6): 1252–1256.
121. Chang YS, Kim JH, Yoo SJ, Lew YJ, Kim J. Fellow-eye neovascu-larization in unilateral retinal angiomatous proliferation in a Korean population. Acta Ophthalmol. 2016;94(1):e49–e53.
Clinical Ophthalmology downloaded from https://www.dovepress.com/ by 118.70.13.36 on 21-Aug-2020
Clinical Ophthalmology
Publish your work in this journal
Submit your manuscript here: http://www.dovepress.com/clinical-ophthalmology-journal
Clinical Ophthalmology is an international, peer-reviewed journal covering all subspecialties within ophthalmology. Key topics include: Optometry; Visual science; Pharmacology and drug therapy in eye diseases; Basic Sciences; Primary and Secondary eye care; Patient Safety and Quality of Care Improvements. This journal is indexed on
PubMed Central and CAS, and is the official journal of The Society of Clinical Ophthalmology (SCO). The manuscript management system is completely online and includes a very quick and fair peer-review system, which is all easy to use. Visit http://www.dovepress.com/ testimonials.php to read real quotes from published authors.
Dovepress
Dove
press
Rabiolo et al
122. Sawa M, Ueno C, Gomi F, Nishida K. Incidence and characteristics of neovascularization in fellow eyes of Japanese patients with unilateral retinal angiomatous proliferation. Retina. 2014;34(4):761–767. 123. Ravera V, Bottoni F, Giani A, Cigada M, Staurenghi G. Retinal
angiomatous proliferation diagnosis: a multiimaging approach. Retina. 2016;36(12):2274–2281.
124. Marsiglia M, Boddu S, Chen CY, et al. Correlation between neovas-cular lesion type and clinical characteristics of nonneovasneovas-cular fel-low eyes in patients with unilateral, neovascular age-related macular degeneration. Retina. 2015;35(5):966–974.
125. Naysan J, Jung JJ, Dansingani KK, Balaratnasingam C, Freund KB. Type 2 (Subretinal) neovascularization in age-related macular degen-eration associated with pure reticular pseudodrusen phenotype. Retina. 2016;36(3):449–457.
126. Cho HJ, Yoo SG, Kim HS, et al. Risk factors for geographic atrophy after intravitreal ranibizumab injections for retinal angiomatous pro-liferation. Am J Ophthalmol. 2015;159(2):285–292.e1.
127. Munk MR, Ceklic L, Ebneter A, Huf W, Wolf S, Zinkernagel MS. Macular atrophy in patients with long-term anti-VEGF treatment for neovascular age-related macular degeneration. Acta Ophthalmol. 2016; 94(8):e757–e764.
128. Saito M, Iida T, Kano M, Itagaki K. Two-year results of combined intravitreal ranibizumab and photodynamic therapy for retinal angiomatous proliferation. Jpn J Ophthalmol. 2016;60(1):42–50. 129. Nghiem-Buffet S, Giocanti-Auregan A, Jung C, et al. Reticular
pseudodrusen are not a predictive factor for the 1-year response to intravitreal ranibizumab in neovascular age-related macular degenera-tion. Retina. 2017;37(1):53–59.
130. Bandello F, Sacconi R, Querques L, Corbelli E, Cicinelli MV, Querques G. Recent advances in the management of dry age-related macular degeneration: a review. F1000Res. 2017;6:245.
131. Corvi F, Souied EH, Falfoul Y, et al. Pilot evaluation of short-term changes in macular pigment and retinal sensitivity in different phe-notypes of early age-related macular degeneration after carotenoid supplementation. Br J Ophthalmol. 2017;101(6):770–773.
Clinical Ophthalmology downloaded from https://www.dovepress.com/ by 118.70.13.36 on 21-Aug-2020