0095-1137/10/$12.00
doi:10.1128/JCM.01382-10
Copyright © 2010, American Society for Microbiology. All Rights Reserved.
Changing Epidemiology of Methicillin-Resistant
Staphylococcus aureus
in Iceland from 2000 to 2008: a Challenge to Current Guidelines
䌤
†
Barbara Juliane Holzknecht,
1,2* Hjo
¨rdis Hardardottir,
3Gunnsteinn Haraldsson,
3Henrik Westh,
2Freyja Valsdottir,
3Kit Boye,
2Sigfus Karlsson,
3Karl Gustaf Kristinsson,
3,4and Olafur Gudlaugsson
1,5Department of Internal Medicine, Landspitali University Hospital, Hringbraut, IS-101 Reykjavik, Iceland
1; Department of Clinical
Microbiology, Copenhagen University Hospital, Hvidovre, Kettegaard Alle 30, DK-2650 Hvidovre, Denmark
2; Department of
Clinical Microbiology, Landspitali University Hospital, Hringbraut, IS-101 Reykjavik, Iceland
3; Faculty of Medicine,
University of Iceland, Vatnsmyrarveg 16, IS-101 Reykjavik, Iceland
4; and Department of Hospital Infection Control,
Landspitali University Hospital, Hringbraut, IS-101 Reykjavik, Iceland
5Received 7 July 2010/Returned for modification 17 August 2010/Accepted 3 September 2010
The epidemiology of methicillin-resistant
Staphylococcus aureus
(MRSA) is continuously changing. Iceland
has a low incidence of MRSA. A “search and destroy” policy (screening patients with defined risk factors and
attempting eradication in carriers) has been implemented since 1991. Clinical and microbiological data of all
MRSA patients from the years 2000 to 2008 were collected prospectively. Isolates were characterized by
pulsed-field gel electrophoresis (PFGE), sequencing of the repeat region of the
Staphylococcus
protein A gene
(
spa
typing), staphylococcal cassette chromosome
mec
(SCC
mec
) typing, and screening for the
Panton-Valen-tine leukocidin (PVL) gene. Two hundred twenty-six infected (60%) or colonized (40%) individuals were
detected (annual incidence 2.5 to 16/100,000). From 2000 to 2003, two health care-associated outbreaks
dominated (
spa
types t037 and t2802), which were successfully controlled with extensive infection control
measures. After 2004, an increasing number of community-associated (CA) cases without relation to the health
care system occurred. A great variety of clones (40 PFGE types and 49
spa
types) were found, reflecting an
influx of MRSA from abroad. The USA300 and Southwest Pacific (SWP) clones were common. SCC
mec
type
IV was most common (72%), and 38% of the isolates were PVL positive. The incidence of MRSA in Iceland has
increased since 1999 but remains low and has been stable in the last years. The search and destroy policy was
effective to control MRSA in the health care setting. However, MRSA in Iceland is now shifting into the
community, challenging the current Icelandic guidelines, which are tailored to the health care system.
The burden of methicillin-resistant
Staphylococcus aureus
(MRSA) has been rising in the past years in many parts of the
world (35, 39). MRSA accounts for substantial morbidity,
mor-tality, and socioeconomic costs (7, 11). While first known as a
health care-associated pathogen, a changing pattern in MRSA
epidemiology has been observed over the past decade. MRSA has
become a community pathogen (13, 40), and in the United States,
MRSA has become the dominant pathogen for skin and soft
tissue infections (SSTI) in outpatients (27). MRSA isolates from
community-associated (CA) cases differ from the classical health
care-associated MRSA. They are typically associated with the
staphylococcal cassette chromosome
mec
(SCC
mec
) types IV and
V, coresistance for other antibiotic classes is less common, and
they often display the Panton-Valentine leukocidin (PVL) gene
(9, 29, 37). However, the distinction between hospital-associated
(HA) and CA MRSA is not always obvious, neither from a
clin-ical nor from a microbiologclin-ical point of view (17, 25).
In Iceland, sporadic MRSA infections have been observed
through the last decades. However, since 2000 the incidence has
been increasing and clinical clusters have occurred, both in the
health care setting and in the community. A strict screening policy
and eradication of MRSA in carriers (the search and destroy
method) has been applied since 1991. This policy has been used
for many years in the Nordic countries and the Netherlands,
where a constant low MRSA incidence has been attributed to this
strategy (38). Here, we describe the changing clinical and
micro-biological features of MRSA in Iceland over the past 9 years.
(Minor parts of this work were presented as a poster
[K-1088] at the 47th Interscience Conference on Antimicrobial
Agents and Chemotherapy [ICAAC], Chicago, IL, September
2007 [14], and as a part [B. J. Holzknecht, invited speaker] of
the session “Update on MRSA in Scandinavia” at the 25th
annual meeting of the Scandinavian Society for Antimicrobial
Chemotherapy, Copenhagen, Denmark, September 2008.)
MATERIALS AND METHODS
Setting.Iceland is a 103,000-km2island in the North Atlantic, with a popula-tion of 317,630 (as of 1 January 2010). There is one university hospital (790 beds) in the capital, Reykjavik, which is the secondary care hospital for the capital region and serves as a tertiary care hospital for the whole country.
All samples, where MRSA was suspected, were handled by the reference microbiology laboratory at the university hospital.
In 1991, the search and destroy strategy was implemented, and the guidelines were revised and applied more strictly after the first cluster of health care-associated MRSA cases occurred in 2000. Defined risk groups (patients and health care workers [HCW], who in the last 6 months have worked or been treated in foreign health care institutions, previously known MRSA carriers, and their household members) were screened upon seeking hospital care. Every new MRSA patient was evaluated by an infection control nurse and/or an infectious disease specialist, and family members and close contacts were screened. MRSA
* Corresponding author. Present address: Department of Clinical
Microbiology, Copenhagen University Hospital, Herlev, Herlev
Ringvej 75, DK-2730 Herlev, Denmark. Phone: 45 4488 3850. Fax: 45
4488 3772. E-mail: [email protected].
† Supplemental material for this article may be found at http://jcm
.asm.org/.
䌤
Published ahead of print on 15 September 2010.
4221
on May 16, 2020 by guest
http://jcm.asm.org/
eradication of carriers was attempted and also offered to MRSA-negative close contacts. Standard eradication treatment consisted of skin and hair wash with chlorhexidine soap combined with mupirocin nasal ointment. Instructions for household cleaning were given. Systemic antibiotics were added in case of throat carriage or unsuccessful treatment, as appropriate. Patients were followed with surveillance cultures for 1 year. At the university hospital there is an electronic alert system for known MRSA carriers. Since May 2008, MRSA has been a notifiable disease.
Clinical data.Since 1 January 2000, clinical and epidemiological data of each MRSA patient have been collected prospectively and entered into a database, each person being registered only once. Based on clinical information, the ac-quisition mode was classified as “imported” (e.g., nonresident of Iceland or association to health care system abroad), “hospital-associated (HA)” (sample takenⱖ48 h after hospitalization, without signs of infection at hospitalization), or “community-associated (CA).” The last was subdivided into “with health care-associated risk factors” (hospital-associated, e.g., health care workers and patients having undergone invasive procedure or hospitalized overnight, or long-term care facility [LTCF]-associated) and “without health care-associated risk factors” (including risk factors for CA MRSA, such as close contact with known MRSA patient). Outbreaks were defined asⱖ10 clinically related cases with microbiologically identical isolates. Groups of fewer than 10 related cases with identical isolates were termed clusters and, according to the clinical relations, subdivided into clusters in the health care system or clusters in the community. The study design and realization were approved by the National Bioethics Com-mittee (07-035-S1) and the Data Protection Authority (2007020148).
Laboratory screening for MRSA and susceptibility testing.Screening swabs were routinely taken from the anterior nares, throat, perineum, and wounds or other skin lesions. Urine was cultured for MRSA, if a urinary catheter was present, and sputum was cultured in the case of respiratory symptoms. For admitted patients, two sets of samples were taken, with an interval of 1 to 4 h. For other persons, only one set was taken. Swabs were incubated in enrichment broth (heart infusion broth with 7% salt and 4g/ml gentamicin) for 16 to 24 h and subcultured on oxacillin resistance screening agar base (ORSAB; Oxoid) and a blood agar plate with a 30-g cefoxitin disk (1g of oxacillin prior to 1 April 2004). Suspicious colonies were tested for coagulase and, if positive, verified by a penicillin binding protein (PBP) 2 latex agglutination test (Oxoid, Cambridge, United Kingdom). In addition, the presence of themecAgene was confirmed by PCR as described before (30). Susceptibility testing for gentamicin, rifampin, trimethoprim, trimethoprim-sulfamethoxazole, tetracycline, minocycline, eryth-romycin, clindamycin, ciprofloxacin, and linezolid was done by disk diffusion (Oxoid) according to the Clinical and Laboratory Standards Institute (CLSI) guidelines, and the MICs of oxacillin, vancomycin, teicoplanin, and mupirocin were evaluated by Etest (AB bioMe´rieux, Sweden).
Typing methods.Only the first isolate of each MRSA case was submitted for further characterization. Of the 226 isolates, 215 (95%) were available for geno-typing. Pulsed-field gel electrophoresis (PFGE) typing according to the Harmony protocol (28) was performed on all isolates.Staphylococcus aureusNCTC 8325 was used as a reference standard. The international reference strains ATCC BAA-1556 (USA300) and EMRSA-15 (from the Harmony collection [6]) were also included in the analysis. The PFGE patterns were analyzed with BioNumer-ics software (Applied Maths, Sint-Martens-Latem, Belgium), using the Dice
coefficient with 1% band tolerance and 0.5% optimization settings. A similarity ofⱖ80% defined PFGE types, which were named with running numbers after appearance in the dendrogram.
Eight representative isolates from the two outbreaks and all available nonout-break isolates were subjected tospatyping (34). Designation ofspatype was conducted by using the Ridom StaphType program (Ridom GmbH, Wurzburg, Germany) (16).Spaclonal clusters (CC) were determined by the based upon repeat pattern (BURP) analysis (StaphType Software; Ridom GmbH, Wurz-burg, Germany) (26) with the default settings: exclusion ofspatypes shorter than 5 repeats and a maximum of 4 costs for clusteringspatypes into the same group. SCCmectypes were determined by an in-house multiplex PCR (5) extended withccrA1andmecIprimers (15, 31). Isolates from the first outbreak were further analyzed byccrBtyping (32) to confirm the SCCmecIII genotype, as typing by multiplex PCR had been inconclusive.
Detection of PVL gene.The PVL gene was detected by PCR as previously published (22) on 8 representative isolates from the two outbreaks and on the 169 available nonoutbreak isolates.
Statistical analysis.To compare groups by categorical data, the chi-square and Fisher’s exact tests were used. To compare groups by continuous variables, the Mann-Whitney U test was used. For processing the data, SPSS 11.0 (SPSS Inc., Chicago, IL) was used. The level of significance was set at 0.05.
RESULTS
Basic epidemiology, outbreaks, and clinical clusters.
During
the study period, MRSA was detected in 226 individuals;
106 (47%) were males. The incidence ranged from 2.5 to
16/100,000 per year. The median age was 44 years (range of
1 month to 100 years).
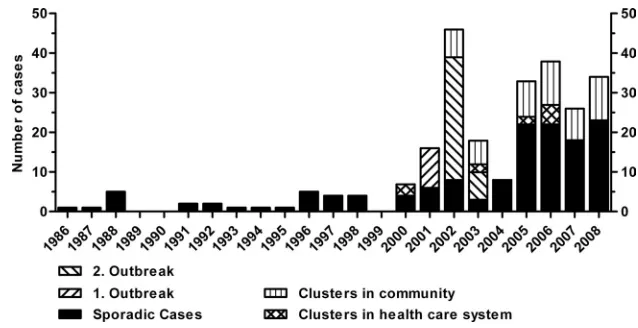
Before the year 2000, zero to five sporadic patients were
diagnosed with MRSA per year. After 2000, the incidence
increased and a growing number of epidemiologically related
cases were diagnosed (Fig. 1).
[image:2.585.130.449.66.230.2]Two health care-associated outbreaks occurred in 2001 and
from 2002 to 2003, respectively. The first outbreak (
spa
type
t037) accounted for 10 patients in a surgical ward of the
uni-versity hospital. The index patient had been transferred from a
hospital in Thailand. The second outbreak was significantly
larger, starting with an index case in a geriatric rehabilitation
ward of the university hospital. Through extensive screening
measures, another 25 patients, one family member, and 11
HCW were diagnosed over a 4-month period. The patients and
HCW were associated with four different wards in the
univer-sity hospital and three community hospitals in the capital area.
Infection control measures included screening of all contacts,
FIG. 1. MRSA in Iceland from 1986 to 2008.
on May 16, 2020 by guest
http://jcm.asm.org/
cohorting of positive patients, and MRSA eradication therapy,
as well as closure and disinfection of wards. The isolates in the
second outbreak displayed an uncommon
spa
type (t2802)
which was not detected apart from that outbreak and has so far
been described only for Iceland and Sweden (http://spaserver
.ridom.de/spa-t2802.shtml, accessed 31 August 2010). They
were susceptible to all tested antibiotics except trimethoprim,
carried SCC
mec
type IV, and were PVL negative.
Apart from the outbreaks, five clinical clusters were identified
in the health care system from 2000 to 2006, affecting 12
individ-uals. Since 2002, 21 clinical clusters occurred in the community,
involving 52 persons. The remaining 114 were sporadic cases.
Thirty-two (14%) of the 226 individuals were health care workers,
and 21 of them were associated with outbreaks and clusters.
Clinical presentation.
Of the 226 individuals, 115 (51%)
were diagnosed by screening. Of these, 40 (35%) were
screened because of previously defined risk factors, and in 75
(65%) the diagnosis was made by screening close contacts of a
newly diagnosed MRSA patient (contact tracing).
Ninety-one of the 226 cases (40%) were only colonized. The
remaining 135 cases presented with clinical infections, SSTI
being the most common (109 patients, 81%). Fifteen patients
(11%) had genitourinary tract infections, eight (6%)
respira-tory tract infections, one osteomyelitis, and two bacteremia.
Both bacteremias occurred in 2008 in young men with
com-munity-associated, recurrent SSTI. Both were imported cases
and had no other MRSA-related risk factors.
According to the National Registry, at the end of the study period
(median follow-up of 3.5 years), 36 patients (16%) had died, 20 (9%)
resided abroad, and 170 patients (75%) still lived in Iceland. None of
the deaths could be attributed to an MRSA infection.
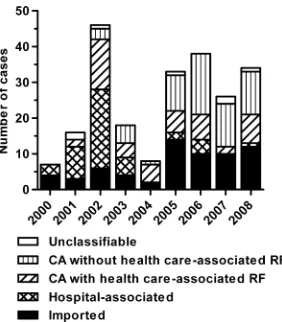
Acquisition.
MRSA was considered to be imported for 65
individuals (29%), six of whom (3%) were passengers on
trans-atlantic flights or cruise liners and admitted on an emergency
basis to an Icelandic hospital. Four patients (2%) were
short-time tourists seeking medical advice, and 13 (6%) were
pa-tients directly transferred from a foreign hospital to an
Icelan-dic hospital. Forty-six (20%) were HA, 48 (21%) CA with
health care-associated risk factors, 60 (27%) CA without
health care-associated risk factors, and 7 (3%) not classifiable
(Fig. 2).
In the first half of the study (1 January 2000 to 30 June
2004), there were nine CA MRSA cases without health
care-associated risk factors compared to 59 health care-care-associated
MRSA cases (HA and CA with health care-associated risk
factors). This changed significantly in the second half of the
study (1 July 2004 to 31 December 2008) to 51 CA MRSA
without health care-associated risk factors compared to 35
health care-associated MRSA (
P
⬍
0.001).
The median age of the health care-associated cases was 69
years (range of 12 to 100 years) and was significantly lower in
the CA cases without health care-associated risk factors (26
years; range of 0 to 82 years;
P
⬍
0.001).
Resistance pattern.
Of 226 isolates, 52 (23%) were resistant
only to beta-lactams and 67 (30%) were resistant to three or more
of the non-beta-lactam antibiotics tested. The percentage of
iso-lates resistant to three or more antibiotics was highest for
im-ported isolates (35/65; 54%), intermediate in health
care-associ-ated (HA and CA with health care-associcare-associ-ated risk factors) MRSA
cases (28/94; 30%), and lowest in isolates from CA cases without
health care-associated risk factors (4/60; 7%).
Genotyping, SCC
mec
typing, and presence of the PVL gene.
PFGE showed 40 different PFGE types, while
spa
typing
re-vealed 49 different
spa
types, which by BURP analysis were
assigned to 10 clusters and six remaining singletons. Results of
the PFGE and
spa
typing were consistent (Table 1). Also, the
two methods complemented each other; eight
spa
types
cluded more than one PFGE type, and 15 PFGE types
in-cluded more than one
spa
type. However, 12 of these PFGE
types included only
spa
types belonging to the same
spa
CC,
and the remaining three included an additional singleton. The
PFGE dendrogram, respective
spa
types,
spa
CC, SCC
mec
types, and presence of the PVL gene are available in the
supplemental material.
Comparison of the PFGE types with known reference strains
confirmed that PFGE type 1 contained the USA300 clone and
PFGE type 37 the EMRSA-15 clone.
The vast majority of the 226 isolates carried SCC
mec
type IV
(72% of 177 tested isolates, representing 74% of 215 available
isolates, when outbreaks were extrapolated). SCC
mec
type II
was the second most common type, with 24 of 177 tested
isolates (14%) (Table 1).
Of the 177 isolates tested (including the outbreak isolates and
therefore representing 215 isolates), 82 (38%) were PVL positive.
PVL was significantly less likely to be positive in isolates from
individuals related to the health care system (HA and CA with
health care-associated risk factors; 14 of 90 PVL positive) than in
CA MRSA isolates from patients without health care-associated
risk factors (42 of 58 positive,
P
⬍
0.001); this was still highly
significant (
P
⬍
0.001), when the outbreak isolates were only
counted once. PVL-positive isolates were more likely to be
asso-ciated with infections (63 of 82 isolates) than PVL-negative
iso-lates (64 of 133,
P
⬍
0.001). While 60 of the available 105 isolates
associated with SSTI were PVL positive, only three of the
avail-able 22 isolates associated with other infections were PVL
posi-tive (
P
⬍
0.001).
DISCUSSION
[image:3.585.92.233.67.228.2]Because of its small size and infrastructural characteristics and
the fact of it being an island state, Iceland provides an ideal
FIG. 2. Mode of acquisition. CA, community associated; RF, risk
factors.
on May 16, 2020 by guest
http://jcm.asm.org/
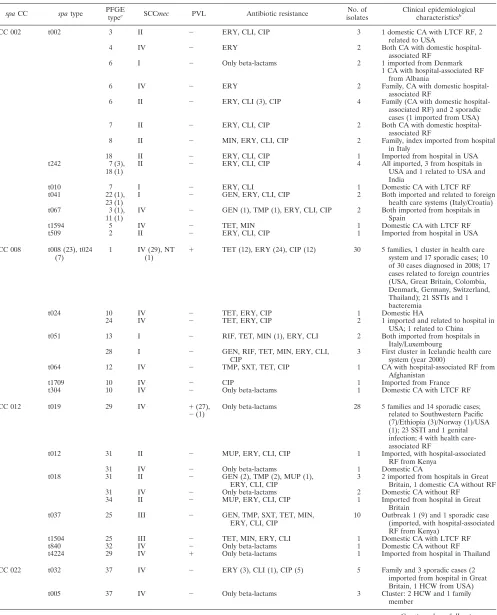
TABLE 1. Clinical and microbiological characteristics of the 226 MRSA cases
aspaCC spatype PFGE
typec SCCmec PVL Antibiotic resistance
No. of isolates
Clinical epidemiological characteristicsb
CC 002 t002 3 II ⫺ ERY, CLI, CIP 3 1 domestic CA with LTCF RF, 2
related to USA
4 IV ⫺ ERY 2 Both CA with domestic
hospital-associated RF
6 I ⫺ Only beta-lactams 2 1 imported from Denmark
1 CA with hospital-associated RF from Albania
6 IV ⫺ ERY 2 Family, CA with domestic
hospital-associated RF
6 II ⫺ ERY, CLI (3), CIP 4 Family (CA with domestic
hospital-associated RF) and 2 sporadic cases (1 imported from USA)
7 II ⫺ ERY, CLI, CIP 2 Both CA with domestic
hospital-associated RF
8 II ⫺ MIN, ERY, CLI, CIP 2 Family, index imported from hospital in Italy
18 II ⫺ ERY, CLI, CIP 1 Imported from hospital in USA
t242 7 (3),
18 (1)
II ⫺ ERY, CLI, CIP 4 All imported, 3 from hospitals in
USA and 1 related to USA and India
t010 7 I ⫺ ERY, CLI 1 Domestic CA with LTCF RF
t041 22 (1),
23 (1)
I ⫺ GEN, ERY, CLI, CIP 2 Both imported and related to foreign health care systems (Italy/Croatia)
t067 3 (1),
11 (1)
IV ⫺ GEN (1), TMP (1), ERY, CLI, CIP 2 Both imported from hospitals in Spain
t1594 5 IV ⫺ TET, MIN 1 Domestic CA with LTCF RF
t509 2 II ⫺ ERY, CLI, CIP 1 Imported from hospital in USA
CC 008 t008 (23), t024 (7)
1 IV (29), NT
(1) ⫹
TET (12), ERY (24), CIP (12) 30 5 families, 1 cluster in health care system and 17 sporadic cases; 10 of 30 cases diagnosed in 2008; 17 cases related to foreign countries (USA, Great Britain, Colombia, Denmark, Germany, Switzerland, Thailand); 21 SSTIs and 1 bacteremia
t024 10 IV ⫺ TET, ERY, CIP 1 Domestic HA
24 IV ⫺ TET, ERY, CIP 2 1 imported and related to hospital in
USA; 1 related to China t051 13 I ⫺ RIF, TET, MIN (1), ERY, CLI 2 Both imported from hospitals in
Italy/Luxembourg
28 I ⫺ GEN, RIF, TET, MIN, ERY, CLI,
CIP
3 First cluster in Icelandic health care system (year 2000)
t064 12 IV ⫺ TMP, SXT, TET, CIP 1 CA with hospital-associated RF from
Afghanistan
t1709 10 IV ⫺ CIP 1 Imported from France
t304 10 IV ⫺ Only beta-lactams 1 Domestic CA with LTCF RF
CC 012 t019 29 IV ⫹(27), Only beta-lactams 28 5 families and 14 sporadic cases;
⫺(1) related to Southwestern Pacific
(7)/Ethiopia (3)/Norway (1)/USA (1); 23 SSTI and 1 genital infection; 4 with health care-associated RF
t012 31 II ⫺ MUP, ERY, CLI, CIP 1 Imported, with hospital-associated
RF from Kenya
31 IV ⫺ Only beta-lactams 1 Domestic CA
t018 31 II ⫺ GEN (2), TMP (2), MUP (1),
ERY, CLI, CIP
3 2 imported from hospitals in Great Britain, 1 domestic CA without RF
31 IV ⫺ Only beta-lactams 2 Domestic CA without RF
34 II ⫺ MUP, ERY, CLI, CIP 1 Imported from hospital in Great
Britain
t037 25 III ⫺ GEN, TMP, SXT, TET, MIN,
ERY, CLI, CIP
10 Outbreak 1 (9) and 1 sporadic case (imported, with hospital-associated RF from Kenya)
t1504 25 III ⫺ TET, MIN, ERY, CLI 1 Domestic CA with LTCF RF
t840 32 IV ⫺ Only beta-lactams 1 Domestic CA without RF
t4224 29 IV ⫹ Only beta-lactams 1 Imported from hospital in Thailand
CC 022 t032 37 IV ⫺ ERY (3), CLI (1), CIP (5) 5 Family and 3 sporadic cases (2
imported from hospital in Great Britain, 1 HCW from USA)
t005 37 IV ⫺ Only beta-lactams 3 Cluster: 2 HCW and 1 family
member
Continued on following page
on May 16, 2020 by guest
http://jcm.asm.org/
setting for the gathering of complete epidemiological data. We
present here extensive clinical and microbiological data for all
Icelandic MRSA cases over a 9-year period.
The yearly incidence of MRSA in Iceland has become
stable over the past 4 years and is low compared to that in
other countries (4, 18) but comparable to that in the
Neth-erlands and the other Nordic countries (http://www.srga.org
/ssac/doc/2005/SSAC_MRSAreport_2004.pdf, accessed 31
August 2010).
[image:5.585.43.543.79.560.2]In the first half of the study period, MRSA was mainly a health
care-associated problem. The first outbreak was caused by an
imported, well-known multiresistant nosocomial MRSA (
spa
type
t037) carrying the SCC
mec
type III. In contrast, the second
out-break was caused by a typical “community MRSA,” resistant only
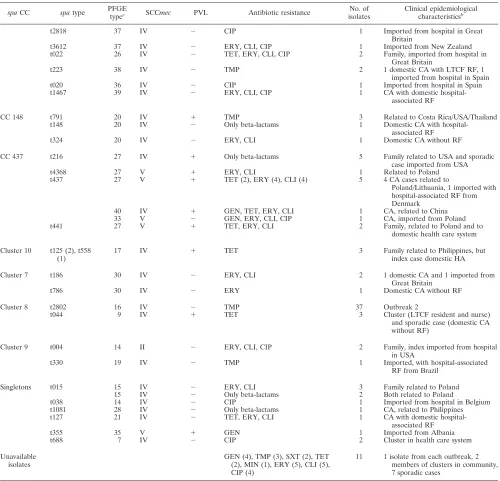
TABLE 1—
Continued
spaCC spatype PFGE
typec SCCmec PVL Antibiotic resistance
No. of isolates
Clinical epidemiological characteristicsb
t2818 37 IV ⫺ CIP 1 Imported from hospital in Great
Britain
t3612 37 IV ⫺ ERY, CLI, CIP 1 Imported from New Zealand
t022 26 IV ⫺ TET, ERY, CLI, CIP 2 Family, imported from hospital in
Great Britain
t223 38 IV ⫺ TMP 2 1 domestic CA with LTCF RF, 1
imported from hospital in Spain
t020 36 IV ⫺ CIP 1 Imported from hospital in Spain
t1467 39 IV ⫺ ERY, CLI, CIP 1 CA with domestic
hospital-associated RF
CC 148 t791 20 IV ⫹ TMP 3 Related to Costa Rica/USA/Thailand
t148 20 IV ⫺ Only beta-lactams 1 Domestic CA with
hospital-associated RF
t324 20 IV ⫺ ERY, CLI 1 Domestic CA without RF
CC 437 t216 27 IV ⫹ Only beta-lactams 5 Family related to USA and sporadic
case imported from USA
t4368 27 V ⫹ ERY, CLI 1 Related to Poland
t437 27 V ⫹ TET (2), ERY (4), CLI (4) 5 4 CA cases related to
Poland/Lithuania, 1 imported with hospital-associated RF from Denmark
40 IV ⫹ GEN, TET, ERY, CLI 1 CA, related to China
33 V ⫺ GEN, ERY, CLI, CIP 1 CA, imported from Poland
t441 27 V ⫹ TET, ERY, CLI 2 Family, related to Poland and to
domestic health care system
Cluster 10 t125 (2), t558 (1)
17 IV ⫹ TET 3 Family related to Philippines, but
index case domestic HA
Cluster 7 t186 30 IV ⫺ ERY, CLI 2 1 domestic CA and 1 imported from
Great Britain
t786 30 IV ⫺ ERY 1 Domestic CA without RF
Cluster 8 t2802 16 IV ⫺ TMP 37 Outbreak 2
t044 9 IV ⫹ TET 3 Cluster (LTCF resident and nurse)
and sporadic case (domestic CA without RF)
Cluster 9 t004 14 II ⫺ ERY, CLI, CIP 2 Family, index imported from hospital
in USA
t330 19 IV ⫺ TMP 1 Imported, with hospital-associated
RF from Brazil
Singletons t015 15 IV ⫺ ERY, CLI 3 Family related to Poland
15 IV ⫺ Only beta-lactams 2 Both related to Poland
t038 14 IV ⫺ CIP 1 Imported from hospital in Belgium
t1081 28 IV ⫺ Only beta-lactams 1 CA, related to Philippines
t127 21 IV ⫺ TET, ERY, CLI 1 CA with domestic
hospital-associated RF
t355 35 V ⫹ GEN 1 Imported from Albania
t688 7 IV ⫺ CIP 2 Cluster in health care system
Unavailable isolates
GEN (4), TMP (3), SXT (2), TET (2), MIN (1), ERY (5), CLI (5), CIP (4)
11 1 isolate from each outbreak, 2 members of clusters in community, 7 sporadic cases
a
In heterogeneous groups, numbers in parentheses indicate number of isolates matching the given result. Abbreviations: NT, nontypeable; GEN, gentamicin; TMP, trimethoprim; SXT, trimethoprim-sulfamethoxazole; RIF, rifampin; MUP, mupirocin; TET, tetracycline; MIN, minocycline; ERY, erythromycin; CLI, clindamycin; CIP, ciprofloxacin; HA, hospital-associated; CA, community-associated; LTCF, long-term care facility; RF, risk factors; HCW, health care worker; SSTI, skin and soft tissue infection.
b
If not specified otherwise, cases are sporadic cases.
c
Reference strain USA300 is PFGE type 1. Reference strain EMRSA-15 is PFGE type 37.
on May 16, 2020 by guest
http://jcm.asm.org/
to trimethoprim and carrying SCC
mec
type IV. It displayed the
rare
spa
type t2802 and was PVL negative. The search and destroy
approach implemented in 1991 was capable of keeping health
care MRSA in check; the two outbreaks were successfully
con-trolled in the years 2001 and 2003. The effectiveness of this
strat-egy in countries with a low MRSA prevalence has been
de-scribed before, and successful eradication of outbreaks in
the health care setting is well documented (19, 38).
However, we now see a shifting epidemiology of MRSA
from the health care system to the community. In many parts
of the world, the emergence of MRSA in the community has
been responsible for rapidly increasing morbidity and costs in
the past years and has been of great concern worldwide (13, 18,
27, 40). Risk factors for CA MRSA have been studied (3, 29)
but are more difficult to define than those for health
care-associated MRSA. It is therefore challenging to adapt the
“search” part of the search and destroy protocol to the
changed epidemiology. However, possible strategies for an
in-creased detection of MRSA in the community could include
the education of general practitioners and emergency room
staff about characteristics of MRSA skin infections and the
importance of obtaining specimens for culture. The
implemen-tation of a more aggressive “destroy” part of the protocol
would have to include house visits for screening of household
members and closer follow-up for MRSA carriers in the
com-munity to ensure optimal adherence to the eradication
proto-col. Focusing on locally endemic
spa
types, such as t019 and
t008/t024, could be adequate and has been shown to be feasible
and effective in similar settings (2, 36).
Genotyping by PFGE and
spa
typing showed a great
diver-sity of MRSA in Iceland. Worldwide, the molecular
epidemi-ology of MRSA varies greatly between different geographic
regions. While in some areas few clones or even one clone
clearly dominates, such as USA300 in the United States (23,
27) or the Lyon clone in France (8), heterogeneous patterns
have been found in other areas (1, 10). The MRSA clones
found in Iceland are to a great extent previously described
clones from many different geographic areas. The
spa
type t019
(Southwest Pacific [SWP] clone, multilocus sequence typing
[MLST] ST-30), which shows features of being endemic in
Iceland, has been linked to the Southwest Pacific (37) and has
recently been described as a frequently occurring clone in
Copenhagen, often in persons related to Eastern Asia (1).
However, in our study, the relationship to this region was not
very strong. Interestingly, this
spa
type did not rank among the
20 most common
spa
types of invasive MRSA infections in
Europe in a recent comprehensive study (12). Another
well-known clone that was identified was USA300. This clone has
spread rapidly in the community in the United States, is the
main causative agent for SSTI in some areas (27), and is now
occurring in hospital-associated infections (33). Recently, it
has been described with increasing frequency for the
commu-nity and hospitals in Denmark (20). Its appearance in Iceland
is worrisome, especially as one-third of the isolates (10/30)
occurred in the last study year, suggesting a rising incidence.
Interestingly, only three of the 215 isolates examined in this
study were
spa
type t044, the most common
spa
type in the
MLST ST-80 clone. This clone occurs endemically in the
com-munity in many European countries (10, 21, 37).
A recent European study has shown regional clustering of
MRSA
spa
types causing invasive infection, e.g., t067 in Spain
and t041 in the Balkans and central Italy (12). In our study,
many of the MRSA cases with these
spa
types had a travel
history matching this geographic distribution (Table 1). This
supports our hypothesis that the heterogeneous genotypic
pat-tern of MRSA in Iceland is due to repeated import of MRSA.
However, there are indications of further genetic evolution of
MRSA in Iceland. In one family with three cases, we have found
genetically closely related isolates displaying the same PFGE
type, but one patient had a
spa
type (t558) which differed from the
other two (t125) by one repeat. The 3 isolates shared the same
susceptibility pattern and were all PVL positive. This is consistent
with the evolution of a genetically closely related isolate during an
outbreak in Denmark, where two different isolates were cultured
from the same individual on the same day (1) and with the finding
of
spa
type alterations in individual MRSA patients (K. Boye and
H. Westh, submitted for publication).
Important changes occurred in the Icelandic population
dur-ing the study period, with rapidly increasdur-ing travel activity and
increasing ethnic heterogeneity of this formerly more isolated
society. The percentage of inhabitants with a foreign
citizen-ship rose from 2.6% in 2000 to 7.4% in 2008 (http://www
.statice.is, accessed 31 August 2010). The number of
passen-gers arriving at Keflavik airport, the main international airport
of Iceland, increased by 99% from 1990 to 2000 and by another
63% from 2000 to 2008 (http://www.statice.is, accessed 31
Au-gust 2010). These changes are very likely to be linked to the
increased incidence of genetically heterogeneous MRSA in
Iceland. Both travel and migration have in other studies been
associated with MRSA (3, 10, 24).
The changing epidemiology of MRSA in Iceland reflects the
changes reported worldwide and the effects of globalization.
MRSA is challenging the community and has to be fought
there to prevent the spread of community MRSA into the
health care system, as reported with the USA300 clone in the
United States and the
spa
type t2802 in the second outbreak
described in this study. Our data underline the need for
sur-veillance, typing, and constant reassessment of existing
strate-gies to control MRSA in Iceland and elsewhere.
ACKNOWLEDGMENTS
We thank Kristin Jonsdottir, Thora Rosa Gunnarsdottir, Elin Ruth
Reed, and Sigridur Sigurdardottir for their work with PFGE and
Su-sanne Mie Rohde for practical help with the SCC
mec
typing.
This study received funding from the Science Fund of Landspitali
University Hospital, Reykjavik, Iceland.
All authors have no conflicts of interest to declare.
REFERENCES
1.Bartels, M. D., K. Boye, A. Rhod Larsen, R. Skov, and H. Westh.2007. Rapid increase of genetically diverse methicillin-resistantStaphylococcus aureus, Copenhagen, Denmark. Emerg. Infect. Dis.13:1533–1540.
2.Bartels, M. D., K. Kristoffersen, K. Boye, and H. Westh.2010. Rise and subsequent decline of community-associated methicillin resistant Staphylo-coccus aureus ST30-IVc in Copenhagen, Denmark through an effective search and destroy policy. Clin. Microbiol. Infect.16:78–83.
3.Bo¨cher, S., A. Gervelmeyer, D. L. Monnet, K. Molbak, R. L. Skov, and Danish CA-MRSA Study Group.2008. Methicillin-resistantStaphylococcus aureus: risk factors associated with community-onset infections in Denmark. Clin. Microbiol. Infect.14:942–948.
4.Boyce, J. M., B. Cookson, K. Christiansen, S. Hori, J. Vuopio-Varkila, S. Kocagoz, A. Y. Oztop, C. M. Vandenbroucke-Grauls, S. Harbarth, and D. Pittet.2005. Meticillin-resistantStaphylococcus aureus. Lancet Infect. Dis.
5:653–663.
5.Boye, K., M. D. Bartels, I. S. Andersen, J. A. Moller, and H. Westh.2007. A
on May 16, 2020 by guest
http://jcm.asm.org/
new multiplex PCR for easy screening of methicillin-resistantStaphylococcus aureusSCCmectypes I-V. Clin. Microbiol. Infect.13:725–727.
6.Cookson, B. D., D. A. Robinson, A. B. Monk, S. Murchan, A. Deplano, R. de Ryck, M. J. Struelens, C. Scheel, V. Fussing, S. Salmenlinna, J. Vuopio-Varkila, C. Cuny, W. Witte, P. T. Tassios, N. J. Legakis, W. van Leeuwen, A. van Belkum, A. Vindel, J. Garaizar, S. Haeggman, B. Olsson-Liljequist, U. Ransjo, M. Muller-Premru, W. Hryniewicz, A. Rossney, B. O’Connell, B. D. Short, J. Thomas, S. O’Hanlon, and M. C. Enright.2007. Evaluation of molecular typing methods in characterizing a European collection of epi-demic methicillin-resistantStaphylococcus aureusstrains: the HARMONY collection. J. Clin. Microbiol.45:1830–1837.
7.Cosgrove, S. E., G. Sakoulas, E. N. Perencevich, M. J. Schwaber, A. W. Karchmer, and Y. Carmeli.2003. Comparison of mortality associated with methicillin-resistant and methicillin-susceptibleStaphylococcus aureus bac-teremia: a meta-analysis. Clin. Infect. Dis.36:53–59.
8.Dauwalder, O., G. Lina, G. Durand, M. Bes, H. Meugnier, V. Jarlier, B. Coignard, F. Vandenesch, J. Etienne, and F. Laurent.2008. Epidemiology of invasive methicillin-resistant Staphylococcus aureus clones collected in France in 2006 and 2007. J. Clin. Microbiol.46:3454–3458.
9.Deurenberg, R. H., and E. E. Stobberingh.2009. The molecular evolution of hospital- and community-associated methicillin-resistantStaphylococcus au-reus. Curr. Mol. Med.9:100–115.
10.Francois, P., S. Harbarth, A. Huyghe, G. Renzi, M. Bento, A. Gervaix, D. Pittet, and J. Schrenzel.2008. Methicillin-resistantStaphylococcus aureus, Geneva, Switzerland, 1993–2005. Emerg. Infect. Dis.14:304–307. 11.Gould, I. M.2006. Costs of hospital-acquired methicillin-resistant
Staphylococ-cus aureus(MRSA) and its control. Int. J. Antimicrob. Agents28:379–384. 12.Grundmann, H., D. M. Aanensen, C. C. van den Wijngaard, B. G. Spratt, D.
Harmsen, A. W. Friedrich, and European Staphylococcal Reference Labo-ratory Working Group. 2010. Geographic distribution ofStaphylococcus aureuscausing invasive infections in Europe: a molecular-epidemiological analysis. PLoS Med.7:e1000215.
13.Grundmann, H., M. Aires-de-Sousa, J. Boyce, and E. Tiemersma.2006. Emergence and resurgence of meticillin-resistantStaphylococcus aureusas a public-health threat. Lancet368:874–885.
14.Gudlaugsson, O., B. J. Holzknecht, H. Hardardottir, T. R. Gunnarsdottir, G. Haraldsson, and K. G. Kristinsson.2007. Clinical and molecular epidemi-ology of methicillin resistantStaphylococcus aureus(MRSA) in Iceland 2000 to 2006, poster K-1088. Abstr. 47th Intersci. Conf. Antimicrob. Agents Che-mother. American Society for Microbiology, Chicago, IL, September 2007. 15.Hanssen, A. M., G. Kjeldsen, and J. U. Sollid. 2004. Local variants of staphylococcal cassette chromosomemecin sporadic methicillin-resistant
Staphylococcus aureusand methicillin-resistant coagulase-negative staphylo-cocci: evidence of horizontal gene transfer? Antimicrob. Agents Chemother.
48:285–296.
16.Harmsen, D., H. Claus, W. Witte, J. Rothganger, H. Claus, D. Turnwald, and U. Vogel.2003. Typing of methicillin-resistantStaphylococcus aureusin a university hospital setting by using novel software forsparepeat determina-tion and database management. J. Clin. Microbiol.41:5442–5448. 17.Healy, C. M., K. G. Hulten, D. L. Palazzi, J. R. Campbell, and C. J. Baker.
2004. Emergence of new strains of methicillin-resistantStaphylococcus au-reusin a neonatal intensive care unit. Clin. Infect. Dis.39:1460–1466. 18.Klevens, R. M., M. A. Morrison, J. Nadle, S. Petit, K. Gershman, S. Ray,
L. H. Harrison, R. Lynfield, G. Dumyati, J. M. Townes, A. S. Craig, E. R. Zell, G. E. Fosheim, L. K. McDougal, R. B. Carey, S. K. Fridkin, and Active Bacterial Core surveillance (ABCs) MRSA Investigators.2007. Invasive methicillin-resistantStaphylococcus aureusinfections in the United States. JAMA298:1763–1771.
19.Kotilainen, P., M. Routamaa, R. Peltonen, J. Oksi, E. Rintala, O. Meurman, O. P. Lehtonen, E. Eerola, S. Salmenlinna, J. Vuopio-Varkila, and T. Rossi.
2003. Elimination of epidemic methicillin-resistant Staphylococcus aureus
from a university hospital and district institutions, Finland. Emerg. Infect. Dis.9:169–175.
20.Larsen, A. R., M. Stegger, R. V. Goering, M. Sørum, and R. Skov.2007. Emer-gence and dissemination of the methicillin resistant Staphylococcus aureus
USA300 clone in Denmark (2000–2005). Euro Surveill. 12:682. http://www .eurosurveillance.org/ViewArticle.aspx?ArticleId⫽682.
21.Larsen, A. R., M. Stegger, S. Bocher, M. Sorum, D. L. Monnet, and R. L. Skov. 2009. Emergence and characterization of community-associated methicillin-resistantStaphylococcus aureusinfections in Denmark, 1999 to 2006. J. Clin. Microbiol.47:73–78.
22.Lina, G., Y. Piemont, F. Godail-Gamot, M. Bes, M. O. Peter, V. Gauduchon, F. Vandenesch, and J. Etienne.1999. Involvement of Panton-Valentine leu-kocidin-producing Staphylococcus aureus in primary skin infections and pneumonia. Clin. Infect. Dis.29:1128–1132.
23.Liu, C., C. J. Graber, M. Karr, B. A. Diep, L. Basuino, B. S. Schwartz, M. C. Enright, S. J. O’Hanlon, J. C. Thomas, F. Perdreau-Remington, S. Gordon, H. Gunthorpe, R. Jacobs, P. Jensen, G. Leoung, J. S. Rumack, and H. F.
Chambers.2008. A population-based study of the incidence and molecular epidemiology of methicillin-resistantStaphylococcus aureusdisease in San Francisco, 2004–2005. Clin. Infect. Dis.46:1637–1646.
24.Longtin, Y., P. Sudre, P. Francois, J. Schrenzel, C. Aramburu, R. Pastore, A. Gervaix, G. Renzi, D. Pittet, and S. Harbarth.2009. Community-associated methicillin-resistantStaphylococcus aureus: risk factors for infection, and long-term follow-up. Clin. Microbiol. Infect.15:552–559.
25.Maree, C. L., R. S. Daum, S. Boyle-Vavra, K. Matayoshi, and L. G. Miller.2007. Community-associated methicillin-resistantStaphylococcus aureusisolates caus-ing healthcare-associated infections. Emerg. Infect. Dis.13:236–242. 26.Mellmann, A., T. Weniger, C. Berssenbrugge, U. Keckevoet, A. W. Friedrich,
D. Harmsen, and H. Grundmann.2008. Characterization of clonal related-ness among the natural population ofStaphylococcus aureusstrains by using
spasequence typing and the BURP (based upon repeat patterns) algorithm. J. Clin. Microbiol.46:2805–2808.
27.Moran, G. J., A. Krishnadasan, R. J. Gorwitz, G. E. Fosheim, L. K. McDou-gal, R. B. Carey, D. A. Talan, and EMERGEncy ID Net Study Group.2006. Methicillin-resistantS. aureusinfections among patients in the emergency department. N. Engl. J. Med.355:666–674.
28.Murchan, S., M. E. Kaufmann, A. Deplano, R. de Ryck, M. Struelens, C. E. Zinn, V. Fussing, S. Salmenlinna, J. Vuopio-Varkila, N. El Solh, C. Cuny, W. Witte, P. T. Tassios, N. Legakis, W. van Leeuwen, A. van Belkum, A. Vindel, I. Laconcha, J. Garaizar, S. Haeggman, B. Olsson-Liljequist, U. Ransjo, G. Coombes, and B. Cookson.2003. Harmonization of pulsed-field gel electro-phoresis protocols for epidemiological typing of strains of methicillin-resis-tantStaphylococcus aureus: a single approach developed by consensus in 10 European laboratories and its application for tracing the spread of related strains. J. Clin. Microbiol.41:1574–1585.
29.Naimi, T. S., K. H. LeDell, K. Como-Sabetti, S. M. Borchardt, D. J. Boxrud, J. Etienne, S. K. Johnson, F. Vandenesch, S. Fridkin, C. O’Boyle, R. N. Danila, and R. Lynfield.2003. Comparison of community- and health care-associated methicillin-resistantStaphylococcus aureusinfection. JAMA290:
2976–2984.
30.Oberdorfer, K., S. Pohl, M. Frey, K. Heeg, and C. Wendt.2006. Evaluation of a single-locus real-time polymerase chain reaction as a screening test for specific detection of methicillin-resistantStaphylococcus aureusin ICU pa-tients. Eur. J. Clin. Microbiol. Infect. Dis.25:657–663.
31.Oliveira, D. C., and H. de Lencastre.2002. Multiplex PCR strategy for rapid identification of structural types and variants of themecelement in meth-icillin-resistantStaphylococcus aureus. Antimicrob. Agents Chemother.46:
2155–2161.
32.Oliveira, D. C., M. Santos, C. Milheirico, J. A. Carrico, S. Vinga, A. L. Oliveira, and H. de Lencastre.2008.ccrBtyping tool: an online resource for staphylococciccrBsequence typing. J. Antimicrob. Chemother.61:959–960. 33.Seybold, U., E. V. Kourbatova, J. G. Johnson, S. J. Halvosa, Y. F. Wang, M. D. King, S. M. Ray, and H. M. Blumberg.2006. Emergence of commu-nity-associated methicillin-resistantStaphylococcus aureusUSA300 genotype as a major cause of health care-associated blood stream infections. Clin. Infect. Dis.42:647–656.
34.Shopsin, B., M. Gomez, S. O. Montgomery, D. H. Smith, M. Waddington, D. E. Dodge, D. A. Bost, M. Riehman, S. Naidich, and B. N. Kreiswirth.1999. Evaluation of protein A gene polymorphic region DNA sequencing for typing ofStaphylococcus aureusstrains. J. Clin. Microbiol.37:3556–3563. 35.Tiemersma, E. W., S. L. Bronzwaer, O. Lyytikainen, J. E. Degener, P.
Schrijnemakers, N. Bruinsma, J. Monen, W. Witte, H. Grundman, and European Antimicrobial Resistance Surveillance System Participants.2004. Methicillin-resistantStaphylococcus aureusin Europe, 1999–2002. Emerg. Infect. Dis.10:1627–1634.
36.Urth, T., G. Juul, R. Skov, and H. C. Schonheyder.2005. Spread of a methicillin-resistantStaphylococcus aureusST80-IV clone in a Danish com-munity. Infect. Control Hosp. Epidemiol.26:144–149.
37.Vandenesch, F., T. Naimi, M. C. Enright, G. Lina, G. R. Nimmo, H. Heffer-nan, N. Liassine, M. Bes, T. Greenland, M. E. Reverdy, and J. Etienne.2003. Community-acquired methicillin-resistant Staphylococcus aureus carrying Panton-Valentine leukocidin genes: worldwide emergence. Emerg. Infect. Dis.9:978–984.
38.Wertheim, H. F., M. C. Vos, H. A. Boelens, A. Voss, C. M. Vandenbroucke-Grauls, M. H. Meester, J. A. Kluytmans, P. H. van Keulen, and H. A. Verbrugh.2004. Low prevalence of methicillin-resistantStaphylococcus au-reus(MRSA) at hospital admission in the Netherlands: the value of search and destroy and restrictive antibiotic use. J. Hosp. Infect.56:321–325. 39.Wisplinghoff, H., T. Bischoff, S. M. Tallent, H. Seifert, R. P. Wenzel, and
M. B. Edmond.2004. Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study. Clin. Infect. Dis.39:309–317.
40.Zetola, N., J. S. Francis, E. L. Nuermberger, and W. R. Bishai.2005. Com-munity-acquired meticillin-resistant Staphylococcus aureus: an emerging threat. Lancet Infect. Dis.5:275–286.