Correlation of the Degree of Dyspnea With
Health-Related Quality of Life, Functional Abilities, and
Diffusing Capacity for Carbon Monoxide in Patients With
Systemic Sclerosis and Active Alveolitis
Results From the Scleroderma Lung Study
Dinesh Khanna,
1Philip J. Clements,
1Daniel E. Furst,
1Yun Chon,
1Robert Elashoff,
1Michael D. Roth,
1Mildred G. Sterz,
1Joannie Chung,
1John D. FitzGerald,
1James R. Seibold,
2John Varga,
3Arthur Theodore,
4Fredrick M. Wigley,
5Richard M. Silver,
6Virginia D. Steen,
7Maureen D. Mayes,
8M. Kari Connolly,
9Barri J. Fessler,
10Naomi F. Rothfield,
11Kamal Mubarak,
12Jerry Molitor,
13and Donald P. Tashkin,
1for the Scleroderma Lung Study Group
Objective. To determine whether baseline self-assessment measures of health status and physiologic indices of disease severity in alveolitis-positive patients
with systemic sclerosis (SSc) correlate with the severity of their dyspnea, and to quantify functional impairment in patients with scleroderma lung disease and compare it with that in patients with chronic obstructive pulmo-nary disease (COPD).
Methods. SSc patients (n ⴝ 138) with diffuse (n ⴝ 81) or limited (n ⴝ 57) cutaneous disease and active alveolitis (determined by bronchoalveolar lavage and/or high-resolution computed tomography) who par-ticipated in the National Heart, Lung, and Blood Institute–sponsored, multicenter, parallel-group, double-blind, randomized, placebo-controlled trial of oral cyclo-phosphamide for treatment of SSc-associated intersti-tial lung disease were evaluated. Pearson’s univariate correlations were determined between the Short Form 36 (SF-36) physical component summary (PCS) and mental component summary (MCS) scales, functional questionnaires, and physiologic parameters of breath-ing (forced vital capacity [FVC] and sbreath-ingle-breath dif-fusing capacity for carbon monoxide [DLCO]). Student’s
t-test was used to compare subgroups. Scores from 2 instruments for self-assessment of breathlessness, Mahler’s baseline dyspnea index (BDI) and a visual analog scale (VAS) for breathing, were divided at the median. Values for the DLCO and FVC (% predicted)
were divided based on the American Thoracic Society guidelines for mild (>70% of predicted), moderate
Supported by the USPHS (grant U01-HL-605 from the National Heart, Lung, and Blood Institute). Dr. Khanna’s work was supported by a Physician Scientist Development award from the Arthritis Foundation and the Scleroderma Foundation. Dr. Mubarak’s work was supported by grants from Actelion, Myogen, Eneysive, and United Therapeutics.
1Dinesh Khanna, MD, MS (current address: University of Cincinnati, Cincinnati, Ohio), Philip J. Clements, MD, MPH, Daniel E. Furst, MD, Yun Chon, PhD, Robert Elashoff, PhD, Michael D. Roth, MD, Mildred G. Sterz, RN, MPH, Joannie Chung, MPH, John D. FitzGerald, MD, MPH, Donald P. Tashkin, MD: David Geffen School of Medicine, University of California, Los Angeles;2James R. Seibold, MD: University of Medicine and Dentistry of New Jersey, New Brunswick;3John Varga, MD: University of Illinois, Chicago; 4Arthur Theodore, MD: Boston University, Boston, Massachusetts; 5Fredrick M. Wigley, MD: The Johns Hopkins University, Baltimore, Maryland; 6Richard M. Silver, MD: Medical University of South Carolina, Charleston;7Virginia D. Steen, MD: Georgetown University Medical Center, Washington, DC;8Maureen D. Mayes, MD, MPH: University of Texas, Houston;9M. Kari Connolly, MD: University of California, San Francisco; 10Barri J. Fessler, MD: University of Alabama at Birmingham;11Naomi F. Rothfield, MD: University of Connecticut Health Center, Farmington; 12Kamal Mubarak, MD: Wayne State University, Detroit, Michigan;13Jerry Molitor, MD, PhD: Benaroya Research Institute at Virginia Mason, Seattle, Washington. Address correspondence and reprint requests to Dinesh Khanna, MD, MS, Division of Immunology, Department of Medicine, University of Cincinnati, PO Box 670563, Cincinnati, OH 45267-0563. E-mail: [email protected].
Submitted for publication May 28, 2004; accepted in revised form October 26, 2004.
(50–70% of predicted), and severe (<50% of predicted) physiologic impairment.
Results.Scores on the BDI and VAS for breathing were highly correlated (rⴝ ⴚ0.61). The PCS and MCS were able to differentiate patients with more breathless-ness (measured by BDI and VAS for breathing) and more abnormal physiologic measures (FVC and DLCO).
In SSc patients with alveolitis, all 8 domains of the SF-36 were significantly impaired as compared with the healthy population and were similar to those reported by patients with COPD.
Conclusion. The SF-36 was able to discriminate between scleroderma lung disease patients with more severe and less severe breathlessness, the primary symptom of active alveolitis. The SF-36 complements the BDI and VAS scores for breathing in scleroderma lung disease and is variably correlated with results of pulmonary function tests, suggesting that the SF-36 should be included as an outcome measure in interven-tion trials in this populainterven-tion.
Systemic sclerosis (SSc; scleroderma) is a connec-tive tissue disease of unknown etiology characterized by microvascular injury, excessive fibrosis of the skin, and distinctive involvement of the viscera, including the heart, lung, kidney, and gastrointestinal tract (1). Lung disease is now the leading cause of morbidity and mortality in patients with SSc. About 40% of all SSc patients develop moderate to severe restrictive lung disease, with the greatest decline in pulmonary function usually occurring within the first 4 years after the onset of non–Raynaud’s phenomenon SSc symptoms (2).
Progressive decrements in lung function of pa-tients with symptomatic lung disease are likely to be accompanied by a decline in their emotional well-being and in their ability to perform day-to-day activities, that is, their health-related quality of life (HRQOL). Treat-ments for active alveolitis commonly used in clinical practice include corticosteroids and other immunosup-pressive agents. Cyclophosphamide is currently being tested against placebo in the Scleroderma Lung Study, a multicenter, parallel-group, double-blind, randomized, placebo-controlled trial in SSc patients with active alve-olitis sponsored by the National Heart, Lung, and Blood Institute. Since cyclophosphamide and other immuno-suppressive agents are associated with significant side effects and toxicity, it is important to consider HRQOL as a separate therapeutic end point in SSc.
No validated method of assessing HRQOL in this patient population is currently available. The aim of the
present study was to evaluate the impact of SSc with active alveolitis on function and HRQOL and to evalu-ate the relationship between HRQOL and measures of breathlessness, the major symptom of SSc alveolitis. A secondary aim was to quantify baseline levels of func-tional impairment and HRQOL in patients with sclero-derma lung disease compared with those in patients with another chronic lung ailment, chronic obstructive pul-monary disease (COPD) and the healthy US general population.
PATIENTS AND METHODS
Study design. The study was conducted as part of a
multicenter trial of therapy for rapidly progressive active pulmonary alveolitis associated with SSc. SSc alveolitis was defined by the presence of ground-glass opacification on high-resolution computed tomography (HRCT) of the chest and/or by the presence ofⱖ3.0% polymorphonuclear neutro-phils and/or ⱖ2.0% eosinophils on bronchoalveolar lavage (BAL).
The following 5 instruments were administered to study participants at baseline: the Medical Outcomes Short Form 36 (SF-36) health survey (3); the Scleroderma Health Assessment Questionnaire (S-HAQ), consisting of the disabil-ity index (DI) of the HAQ and 5 visual analog scales (VAS) examining vascular problems (Raynaud’s phenomenon and digital tip ulcers), gastrointestinal symptoms, lung symptoms, and overall disease severity from the perspective of the patient (4); Mahler’s baseline dyspnea index (BDI) (5); the VAS for breathing; and the patient’s global assessment (PGA). Scores on the VAS for breathing and PGA were taken from the S-HAQ assessments.
As part of the trial, each patient also underwent pulmonary function testing, consisting of spirometry (including forced vital capacity [FVC]), body plethysmographic lung volumes, maximal inspiratory and expiratory pressures, and single-breath diffusing capacity for carbon monoxide (DLCO). Data for 2 of the physiologic parameters (FVC and DLCO) are presented and analyzed as the percent of predicted values, as derived from published prediction equations (6,7). Skin changes were assessed using the modified Rodnan skin thick-ness score (MRSS) (8).
Patient selection.Patients with SSc, as defined by the
American College of Rheumatology (formerly, the American Rheumatism Association) classification criteria (9), of ⱕ7 years’ duration (onset defined as the date of the first typical non–Raynaud’s phenomenon manifestation) were included in the study. SSc patients were further grouped as those with limited cutaneous SSc and diffuse cutaneous SSc, based on the distribution of the skin thickening. Limited disease was char-acterized by thickening of the skin distal to the elbows and knees and proximal to the clavicles (including the face). Diffuse disease was characterized by thickening of the skin proximal as well as distal to the elbows and knees and including the trunk and the face (8). Other inclusion criteria included an FVC ⱕ85% of predicted, dyspnea on exertion (grade 2 or higher on the magnitude of task component of the BDI), and
alveolitis on BAL and/or HRCT (as defined above). Grade 2 dyspnea on the BDI corresponds to an inability to climb 3 flights of stairs because of significant dyspnea.
The major exclusion criteria were an FVC⬍45% of predicted or a DLCO ⬍30% of predicted; persistent unex-plained hematuria, leukopenia (⬍4,000 white blood cells) or thrombocytopenia (⬍100,000 platelets); a serum creatinine levelⱖ2.0 mg/dl; pregnancy or breast-feeding; previous use of cyclophosphamide for⬎4 weeks; severe pulmonary hyperten-sion requiring specific treatment with either bosentan, epopro-stenol, or triprostenol; uncontrolled congestive heart failure; smoking during the previous 6 months; use of prednisone at a dosage ⬎10 mg/day; or clinically significant abnormalities other than interstitial lung disease identified on chest radiog-raphy or on HRCT. Echocardiogram and right heart catheter-ization were not routinely performed as part of the study.
Questionnaires. HRQOL questionnaire. The Medical
Outcomes SF-36 is a self-administered survey that assesses general HRQOL (i.e., the concepts are not specific for any age, disease, or treatment group) (3). This allows comparisons of the relative burdens of different diseases and benefits of therapies across normal and various disease cohorts (10). The SF-36 consists of 4 physical health domains (physical function-ing [10 items], body pain [2 items], role limitations due to physical health [4 items] and general health perceptions [5 items]), 4 mental health domains (mental health [5 items], role limitations due to emotional problems [3 items], vitality [4 items], and social functioning [2 items]), and a health transition domain (1 item). Each domain is scored from 0–100, with higher scores indicating better quality of life. The 4 physical health domains can be compiled as a physical component summary (PCS) score and the 4 mental health domains as a mental component summary (MCS) score. These summary scores are standardized to responses from the general popu-lation, the mean score of which is 50 and the standard deviation is 10 (10).
Function questionnaires.The HAQ DI is a condition-specific measure of functional status (assessing activities of daily living), intended for use in arthritis (11). The standard HAQ DI is calculated as an ordinal variable, from 0 ⫽ no disability to 3⫽severe disability. The original HAQ DI was designed as a 20-item self-administered questionnaire examin-ing difficulties with the performance of activities of daily livexamin-ing in 8 dimensions (dressing and grooming, arising, eating, walk-ing, hygiene, reach, grip, and other activities). In the original HAQ DI, an additional grade of difficulty was added for patients using assistive/adaptive devices (cane, walker, etc.). In the current study, the patient responses were not modified for patient use of assistive/adaptive devices. The HAQ DI is calculated by summarizing the highest score in each of the 8 domains and dividing the sum by 8, giving a score between 0 and 3 on an ordinal scale (no disability to severe disability). The HAQ DI has been found to correlate with cutaneous and visceral involvement in SSc at baseline and with changes in physiologic parameters over time (12–16).
VAS scales measuring SSc involvement of individual organ systems were added to the HAQ DI to examine vascular problems (Raynaud’s phenomenon and digital tip ulcers), gastrointestinal symptoms, lung symptoms (VAS for breath-ing), and overall disease severity (VAS for PGA) from the
perspective of the patient (4). The addition of these 5 VAS scales to the HAQ DI constitutes the S-HAQ.
Dyspnea questionnaires.Mahler’s BDI allows patients to self-assess their level of dyspnea (5). Scores on the BDI depend on ratings for 3 different categories: functional impair-ment, magnitude of task, and magnitude of effort. Limitation of ability in each of these 3 categories of dyspnea is graded from 0 (severe) to 4 (unimpaired). The ratings for the 3 categories are summed to form the baseline score, with a range of 0 (severe) to 12 (no dyspnea).
The VAS scale for breathing is included in the S-HAQ; it allows patients to self-assess their degree of difficulty in performing daily activities due to shortness of breath. A continuous 100-mm scale (from no limitation of activity to severe limitation of activity) is used for this assessment.
Statistical analysis. Relationships between
compo-nents of the SF-36 (PCS and MCS and the 8 individual domains thereof) and the BDI, VAS for breathing, HAQ DI, PGA, MRSS, and measures of lung function were sought using parametric (Pearson’s) correlations. Clinical subsets for the BDI and the VAS for breathing were developed based on dichotomous variables by using the respective median values as the cut points.
Clinical subsets of FVC were determined according to the American Thoracic Society guidelines for mild (⬎70% of predicted), moderate (50–70% of predicted), and severe (⬍50% of predicted) physiologic impairment (17). Since there are no published classification criteria for the severity of impairment in the DLCO, we used similar cut points for the degree of severity of the DLCO(mild impairment⫽below the lower limit of the normal percent of predicted values but
⬎70% of predicted, moderate⫽ⱕ70% of predicted, moder-ately severe⫽ ⱖ50% of predicted, severe⫽ ⬍50% of pre-dicted, and very severe impairment ⫽ ⱖ34% of predicted). Nearly 48% of the study patients (n⫽66) had normal to mild impairment in the FVC, with 48% (n⫽66) having moderate impairment and 4% (n ⫽ 6) having severe impairment. In contrast, only 8 patients had a DLCOthat was⬎70% predicted, with 54 patients (39%) and 76 patients (55%), respectively, having moderate and severe impairment. Due to the low number of patients in the severe FVC group, the moderate and severe groups were combined for analysis. Similarly, the mild and moderate DLCOgroups were combined for analysis.
Student’st-test was used to compare 2 subgroups of the study population for continuous baseline characteristics, and the chi-square test was used for categorical characteristics. A number of comparisons between groups and within subsets were performed in this analysis. Because the questions ad-dressed by these comparisons are of independent interest, no adjustment for multiple comparisons was made. A Bonferroni or related correction could have been applied, but because the number of tests was large, this would have essentially elimi-nated any possibility of identifying possible clinically significant effects. The reader should recognize, however, that some part of the nominally significant findings reported here might be the result of Type I error.
To evaluate the degree of impairment of HRQOL in patients with scleroderma lung disease, the 8 domains of the SF-36 in SSc patients were compared with those in the healthy US population and with those in patients with COPD (10). The mean score in the healthy US population was age- and
sex-adjusted to match our study population by using weighted means.
The values for continuous variables are presented as the mean ⫾ SD. P values less than 0.05 were considered statistically significant, without correction for multiple compar-isons. All procedures were performed using SAS version 8.0 software (SAS Institute, Cary, NC).
RESULTS
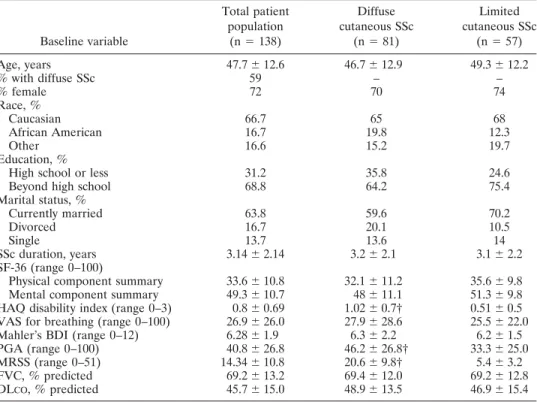
Baseline characteristics.The baseline character-istics of the SSc population are summarized in Table 1. Patients ranged in age from 19 years to 83 years, 72% were women, 66.7% were Caucasian, and 16.7% were
African American. The mean ⫾ SD duration of SSc
prior to study enrollment was 3.14⫾2.14 years from the
first non–Raynaud’s phenomenon manifestation. On average, the HAQ DI indicated only mild functional
abnormalities (mean⫾SD 0.8⫾0.69) (11,13). Patients
with diffuse cutaneous disease had a lower PCS and a higher HAQ DI, signifying greater functional disability,
compared with those with limited cutaneous disease. These findings were corroborated by the observation of a worse PGA score, along with a higher MRSS, in the patients with diffuse disease (Table 1).
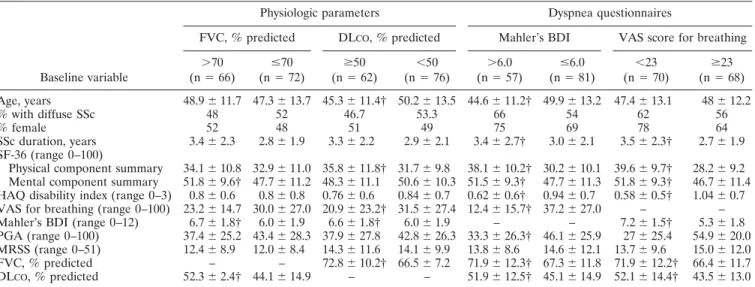
The relationship between various baseline char-acteristics of the patient population and 2 different measures of SSc pulmonary disease severity (physiologic parameters and dyspnea questionnaires) is shown in Table 2. The physiologic parameters consisted of the FVC, an objective physiologic index of restrictive
venti-latory impairment, and the DLCO, an objective
physio-logic index of impaired gas transfer (diffusion), and the dyspnea questionnaires consisted of the BDI and the VAS for breathing, both of which are subjective patient-oriented measures of dyspnea.
Table 2 further differentiates patients with values above and below the median on the dyspnea question-naires and physiologic measures (mild versus moderate and severe for the FVC; mild and moderate versus Table 1. Baseline characteristics of the patients with active alveolitis associated with systemic sclerosis*
Baseline variable Total patient population (n⫽138) Diffuse cutaneous SSc (n⫽81) Limited cutaneous SSc (n⫽57) Age, years 47.7⫾12.6 46.7⫾12.9 49.3⫾12.2 % with diffuse SSc 59 – – % female 72 70 74 Race, % Caucasian 66.7 65 68 African American 16.7 19.8 12.3 Other 16.6 15.2 19.7 Education, %
High school or less 31.2 35.8 24.6
Beyond high school 68.8 64.2 75.4
Marital status, % Currently married 63.8 59.6 70.2 Divorced 16.7 20.1 10.5 Single 13.7 13.6 14 SSc duration, years 3.14⫾2.14 3.2⫾2.1 3.1⫾2.2 SF-36 (range 0–100)
Physical component summary 33.6⫾10.8 32.1⫾11.2 35.6⫾9.8 Mental component summary 49.3⫾10.7 48⫾11.1 51.3⫾9.8 HAQ disability index (range 0–3) 0.8⫾0.69 1.02⫾0.7† 0.51⫾0.5 VAS for breathing (range 0–100) 26.9⫾26.0 27.9⫾28.6 25.5⫾22.0 Mahler’s BDI (range 0–12) 6.28⫾1.9 6.3⫾2.2 6.2⫾1.5
PGA (range 0–100) 40.8⫾26.8 46.2⫾26.8† 33.3⫾25.0
MRSS (range 0–51) 14.34⫾10.8 20.6⫾9.8† 5.4⫾3.2
FVC, % predicted 69.2⫾13.2 69.4⫾12.0 69.2⫾12.8
DLCO, % predicted 45.7⫾15.0 48.9⫾13.5 46.9⫾15.4
* Higher scores on the physical and mental component summaries of the Short Form 36 (SF-36) health survey and on Mahler’s baseline dyspnea index (BDI) indicate better status. Higher scores on the Health Assessment Questionnaire (HAQ) disability index, the visual analog scale (VAS) score for breathing, patient’s global assessment (PGA), and the modified Rodnan skin thickness score (MRSS) indicate poorer status. Except where indicated otherwise, values are the mean⫾SD. SSc⫽systemic sclerosis; FVC⫽ forced vital capacity; DLCO⫽single-breath diffusing capacity for carbon monoxide.
severe for the DLCO). Both the PCS and the MCS were
able to discriminate between patients with more severe versus less severe breathlessness as measured by the BDI
and VAS for breathing (P⬍0.05 for both the PCS and
the MCS). Importantly, the MCS was able to discrimi-nate between more versus less impairment in the FVC, and the PCS was able to discriminate between more
versus less impairment in the DLCO.
Correlations.Table 3 shows the univariate corre-lations among each of the 8 individual domains as well as the 2 summary scores of the SF-36 and the degree of dyspnea, the PGA, functional disability, and measures of lung function. The BDI and VAS for breathing were
highly correlated with each other (r⫽–0.61). The BDI,
VAS for breathing, and PGA were significantly corre-lated with all 8 domains of the SF-36. The HAQ DI was also significantly correlated with 7 of the 8 domains of the SF-36 (the exception being mental health). The FVC was only weakly correlated with the SF-36 general health and social functioning domains, and showed no
correla-tion with the BDI. The DLCOshowed a weak correlation
with the SF-36 physical functioning domain, as well as with the BDI and the VAS for breathing (Table 3).
The correlations among the various functional, HRQOL, and dyspnea questionnaires were highly sig-nificant, but the correlations were weaker between the patient assessment questionnaires and the objective
measures of pulmonary function (FVC and DLCO). A
correlation coefficient (r) of 0.40 or higher was regarded
as indicating a moderate degree of correlation. Most of the correlation coefficients among the functional,
HRQOL, and dyspnea questionnaires were ⬎0.40,
whereas the coefficient was⬍0.40 between the
question-naires and objective measures of pulmonary function. For example, the highest correlation between the patient assessment questionnaires and the FVC was only 0.24 (the social functioning domain of the SF-36) and
be-tween the questionnaires and the DLCO was –0.31 (the
VAS for breathing).
Comparison of SSc patients with the healthy US population and with COPD patients.Figure 1 presents the mean SF-36 scores in each domain. For comparison purposes, we used previously published mean SF-36 scores for the healthy US and COPD patient popula-tions (10). Patients with SSc reported impairment in multiple domains of functioning. The most severe im-pairment reported was in physical functioning, role limitations due to physical health, body pain, vitality,
and general health (P⬍ 0.0001) as compared with the
healthy US population. However, the impairment in health status of the SSc patients across the different domains of the SF-36 was similar to that reported by patients with COPD.
The mean⫾SD PCS score in the SSc population
was 34.6 ⫾ 10.8, which was ⬃1.4 SD below the mean
score in the age- and sex-adjusted healthy US population
(48.7⫾10) and was similar to the mean score in patients
with COPD (35.9 ⫾ 10.3) (Figure 1). In contrast, the
Table 2. Baseline characteristics of SSc patients, by physiologic parameters and dyspnea questionnaire scores*
Baseline variable
Physiologic parameters Dyspnea questionnaires
FVC, % predicted DLCO, % predicted Mahler’s BDI VAS score for breathing
⬎70 (n⫽66) ⱕ70 (n⫽72) ⱖ50 (n⫽62) ⬍50 (n⫽76) ⬎6.0 (n⫽57) ⱕ6.0 (n⫽81) ⬍23 (n⫽70) ⱖ23 (n⫽68) Age, years 48.9⫾11.7 47.3⫾13.7 45.3⫾11.4† 50.2⫾13.5 44.6⫾11.2† 49.9⫾13.2 47.4⫾13.1 48⫾12.2 % with diffuse SSc 48 52 46.7 53.3 66 54 62 56 % female 52 48 51 49 75 69 78 64 SSc duration, years 3.4⫾2.3 2.8⫾1.9 3.3⫾2.2 2.9⫾2.1 3.4⫾2.7† 3.0⫾2.1 3.5⫾2.3† 2.7⫾1.9 SF-36 (range 0–100)
Physical component summary 34.1⫾10.8 32.9⫾11.0 35.8⫾11.8† 31.7⫾9.8 38.1⫾10.2† 30.2⫾10.1 39.6⫾9.7† 28.2⫾9.2 Mental component summary 51.8⫾9.6† 47.7⫾11.2 48.3⫾11.1 50.6⫾10.3 51.5⫾9.3† 47.7⫾11.3 51.8⫾9.3† 46.7⫾11.4 HAQ disability index (range 0–3) 0.8⫾0.6 0.8⫾0.8 0.76⫾0.6 0.84⫾0.7 0.62⫾0.6† 0.94⫾0.7 0.58⫾0.5† 1.04⫾0.7 VAS for breathing (range 0–100) 23.2⫾14.7 30.0⫾27.0 20.9⫾23.2† 31.5⫾27.4 12.4⫾15.7† 37.2⫾27.0 – – Mahler’s BDI (range 0–12) 6.7⫾1.8† 6.0⫾1.9 6.6⫾1.8† 6.0⫾1.9 – – 7.2⫾1.5† 5.3⫾1.8 PGA (range 0–100) 37.4⫾25.2 43.4⫾28.3 37.9⫾27.8 42.8⫾26.3 33.3⫾26.3† 46.1⫾25.9 27⫾25.4 54.9⫾20.0 MRSS (range 0–51) 12.4⫾8.9 12.0⫾8.4 14.3⫾11.6 14.1⫾9.9 13.8⫾8.6 14.6⫾12.1 13.7⫾9.6 15.0⫾12.0 FVC, % predicted – – 72.8⫾10.2† 66.5⫾7.2 71.9⫾12.3† 67.3⫾11.8 71.9⫾12.2† 66.4⫾11.7 DLCO, % predicted 52.3⫾2.4† 44.1⫾14.9 – – 51.9⫾12.5† 45.1⫾14.9 52.1⫾14.4† 43.5⫾13.0 * Except where indicated otherwise, values are the mean⫾SD. SSc⫽systemic sclerosis; FVC⫽forced vital capacity; DLCO⫽single-breath diffusing capacity for carbon monoxide; BDI⫽baseline dyspnea index; VAS⫽visual analog scale; SF-36⫽Short Form 36; HAQ⫽Health Assessment Questionnaire; PGA⫽patient’s global assessment; MRSS⫽modified Rodnan skin thickness score.
Table 3. Correlation coefficients between health-related qualit y o f life instruments and measures of dyspnea and physiologic impairment* PGA Mahler’s BDI VAS for breathing HAQ DI FVC, % predicted DL CO ,% predicted MRSS Physical score SF-36 physical component summar y ⫺ 0.64† 0.51† ⫺ 0.59† ⫺ 0.69† 0.14 0.16 ⫺ 0.26‡ SF-36 physical health domains Physical functioning ⫺ 0.55† 0.56† ⫺ 0.62† ⫺ 0.70† 0.15 0.23‡ ⫺ 0.24‡ Role, physical ⫺ 0.48† 0.44† ⫺ 0.43† ⫺ 0.35† 0.05 0.09 ⫺ 0.10 Body pain ⫺ 0.59† 0.28‡ ⫺ 0.42† ⫺ 0.64† 0.10 ⫺ 0.06 ⫺ 0.35‡ General health perceptions ⫺ 0.52† 0.40† ⫺ 0.53† ⫺ 0.44† 0.23‡ 0.13 ⫺ 0.24‡ Mental score SF-36 mental component summar y ⫺ 0.31‡ 0.26‡ ⫺ 0.30‡ ⫺ 0.18 0.16 0.12 ⫺ 0.25‡ SF-36 mental health domains Vitalit y ⫺ 0.47† 0.48† ⫺ 0.50† ⫺ 0.44† 0.13 0.01 ⫺ 0.24‡ Social functioning ⫺ 0.53† 0.37† ⫺ 0.44† ⫺ 0.52† 0.24‡ ⫺ 0.12 ⫺ 0.38‡ Role, emotional ⫺ 0.31‡ 0.31‡ ⫺ 0.37† ⫺ 0.24‡ 0.16 0.02 ⫺ 0.19‡ Mental health ⫺ 0.29‡ 0.21‡ ⫺ 0.24‡ ⫺ 0.17 0.09 ⫺ 0.06 ⫺ 0.18‡ Mahler’s BDI ⫺ 0.33‡ – ⫺ 0.61† ⫺ 0.33† 0.16 0.24‡ ⫺ 0.11 VAS for breathing 0.61† ⫺ 0.61† – 0.46† ⫺ 0.19‡ ⫺ 0.31‡ 0.12 * PGA ⫽ patient’s global assessment; BDI ⫽ baseline dyspnea index; VAS ⫽ visual analog scale; HAQ ⫽ Health Assessment Questionnaire; DI ⫽ disabilit y index; FVC ⫽ forced vital capacit y; DL CO ⫽ single-breath diffusing capacit y for carbon monoxide; MRSS ⫽ modified Rodnan skin thickness score; SF-36 ⫽ Short Form 36. † P ⬍ 0.01. ‡ P ⬍ 0.05.
MCS scores were similar across the 3 groups (50.18 ⫾
10.03 in SSc patients, 50.19 ⫾ 10 in the healthy US
population, and 47.73⫾ 11.44 in COPD patients).
DISCUSSION
Although it is well known that SSc can be dis-abling, little attention has been paid to a systematic evaluation of HRQOL in patients with SSc. This may in part be due to the low prevalence of SSc and the relative scarcity of large multicenter studies in which this out-come measure could be evaluated. The Scleroderma Lung Study, therefore, provides a unique opportunity to evaluate dyspnea and its effect on HRQOL, as measured by the SF-36, in SSc patients with alveolitis participating in a longitudinal clinical trial.
When breathlessness (measured by the BDI and the VAS for breathing) was compared with the PCS and MCS, both of these HRQOL scales were able to dis-criminate between SSc patients with alveolitis who
re-ported more dyspnea (BDIⱕ6.0 or VAS for breathing
⬎23) and those who reported less dyspnea (BDI⬎6.0 or
VAS for breathingⱕ23) (P⬍0.05 for both scales). Also,
the PCS and MCS collectively were able to discriminate between patients with more abnormalities or less abnor-malities of the measures of physiologic functioning (e.g.,
between those with an FVC⬎70% predicted and those
with an FVCⱕ70% predicted as well as between those
with a DLCO ⱖ50% predicted and those with a DLCO
⬍50% predicted).
Patients with worse dyspnea, as demonstrated by
a BDIⱕ6.0 and a VAS score for breathing⬎23, had a
significantly worse score for the HAQ DI, showing the discriminative role of this arthritis-specific questionnaire (Table 2). The advantage of using the HAQ DI in the present study is its ability to quantify patient-reported disability and differentiate it from the extrapulmonary complications of their SSc. The HAQ DI showed a higher correlation with the MRSS, one of the surrogates
for severity of SSc (r⫽ 0.49,P⬍0.0001) than with the
PCS (r⫽–0.25,P⬍0.05) (data not shown). The HAQ
DI also was able to differentiate patients based on the extent of skin thickening, with a score of 0.51 in patients with limited cutaneous SSc and a score of 1.02
in those with diffuse cutaneous SSc (P ⬍ 0.001). In
contrast, the SF-36 was not able to differentiate limited versus diffuse cutaneous SSc (PCS of 35.6 in limited
cutaneous SSc versus 32.1 in diffuse cutaneous SSc;P⫽
0.06) (Table 1).
Thus, the HAQ DI complemented the SF-36 and other measures used to evaluate SSc. It was able to Figure 1. Comparison of the mean scores on the individual domains and summary scales of
the Short Form 36 (SF-36) health survey in the age- and sex-adjusted healthy US population (open bars), in patients with systemic sclerosis (SSc) and active alveolitis (gray bars), and in patients with chronic obstructive pulmonary disease (solid bars). Role physical ⫽ role limitations due to physical health; Gen health ⫽ general health; role emotion ⫽ role limitations due to emotional problems; PCS⫽physiologic component summary; MCS⫽ mental component summary.ⴱ⫽P⬍0.0001; §⫽P⫽0.002; †⫽P⫽0.004 versus the US population.
capture functional disability due to SSc more effectively than either of the SF-36 summary scales.
Evaluation of HRQOL in patients with SSc and active alveolitis at baseline revealed a marked decrease in their HRQOL, as indicated by significantly low scores in all the 8 SF-36 domains (Figure 1). This impairment is similar to that noted in patients with symptomatic COPD (18), idiopathic pulmonary fibrosis (19,20), and previously reported series of patients with early SSc (21), and it is considerably different from the age- and sex-matched healthy US population.
There are some limitations of the present study. First, it is conceivable that patients without active alve-olitis may have been included in the trial. The main objective of the Scleroderma Lung Study was to evaluate the benefits/risks of an antiinflammatory/immunosup-pressive agent (oral cyclophosphamide) versus placebo in patients with relatively early SSc with symptomatic interstitial lung disease and findings suggestive of active alveolitis (neutrophilia/eosinophilia on BAL and/or ground-glass opacification on thoracic HRCT). Since there is no perfect system for a priori identification of patients with progressive alveolitis, it is possible that the ground-glass opacification seen in a few patients with negative findings on BAL represented a process other than active alveolitis. To increase the sensitivity for the diagnosis of active alveolitis, patients were also required to have symptomatic dyspnea and abnormalities on pulmonary function testing. At the completion of the trial, with all of these parameters captured, we will be able to relate our baseline findings to clinical responses and thereby better define populations that are likely to progress.
Second, we did not include a disease-specific questionnaire for pulmonary symptoms, which would have further strengthened our study. A formal respiratory-specific validated questionnaire is not available for SSc-associated interstitial lung disease. However, Chang et al (19) tested the SF-36 and 2 respiratory-specific instru-ments (Chronic Respiratory Questionnaire and St. George’s Respiratory Questionnaire [SGRQ]) in 50 patients with idiopathic interstitial lung disease. The SGRQ had a better correlation than did the PCS of the
SF-36 with the FVC (r⫽–0.45,P⬍0.01 versus r⫽0.31,
P⬍0.05) and the DLCO(r⫽–0.55,P⬍0.01 versus r⫽
0.32, P ⬍ 0.05). The correlation coefficient for the
6-minute walk distance and the dyspnea score was
similar (r⬍0.5,P⬍0.01) for both the SF-36 PCS and
the SGRQ. The authors suggested that both the SF-36 and the SGRQ are sensitive tools for assessing HRQOL in these patients.
Third, we did not evaluate exercise tolerance in the SSc patients. Chang et al (19) found a statistically significant correlation between the SF-36 PCS and the 6-minute walk distance in patients with interstitial lung disease (19). However, due to the arthritis and contrac-tures associated with SSc, some patients in the present study would have been expected to have difficulty per-forming the 6-minute walk, even in the presence of relatively mild pulmonary disease, as a result of concom-itant arthritis. Also, the 6-minute walk distance has not yet been validated as a measure of pulmonary morbidity and mortality in patients with scleroderma interstitial lung disease, with or without arthritis.
Fourth, echocardiograms were not included as a part of the study. It is possible that patients with mild-to-moderate pulmonary hypertension not requiring specific therapy were included in the study. An isolated
decrease in the DLCO could be due to pulmonary
hypertension rather than pulmonary involvement. Last, the present study analyzed only cross-sectional data. Subsequent completion of the 2-year trial of cyclophosphamide in SSc interstitial lung disease should allow analysis of the responsiveness of the SF-36 to a therapeutic intervention. This would be key to determining whether the SF-36 or its components would be a worthwhile outcome measure in clinical studies.
In conclusion, in patients with active alveolitis associated with SSc, values for Mahler’s BDI and the VAS for breathing (both measures of breathlessness) were associated with performance on both the physical and mental component summary measures of the
SF-36 and, to a lesser degree, with the DLCO. The SF-36
was able to discriminate between patients with more severe versus less severe breathlessness, the primary symptom of active alveolitis. We have also shown the usefulness of 2 VAS scales (the VAS for breathing and the PGA VAS) in assessing patients with active alveolitis and SSc. Although physiologic variables are helpful to the clinicians, most patients are concerned about their symptoms, their ability to perform day-to-day activities, and their general well-being. As lung disease progresses in SSc, the patients invariably become severely limited in their activities and may become dependent on supplemental oxygen. The potential toxi-city of current therapy for SSc is of particular interest in this longitudinal clinical trial. Although cyclo-phosphamide therapy may result in disease stabilization or actual improvement of lung function, potentially undesirable side effects could counterbalance the effica-cious effects on HRQOL.
The overall findings from this baseline analysis of lung function, breathing problems, and various quality of life measures in participants in the Scleroderma Lung Study should be helpful to physicians. Pulmonary dis-ability is an important determinant of HRQOL in this population. When extended to include a followup assess-ment after completion of therapy in the Scleroderma Lung Study, the findings should provide us with addi-tional important information on the balance between the possible efficacy of cyclophosphamide in stabilizing or improving lung function and respiratory symptoms and its potential toxicity, both of which would be ex-pected to influence HRQOL.
ACKNOWLEDGMENTS
The following centers participated in the Scleroderma Lung Study: Boston University, Boston, MA, Georgetown University, Washington, DC, Johns Hopkins University/ University of Maryland, Baltimore, MD, Medical University of South Carolina, Charleston, University of Alabama at Bir-mingham, University of Illinois at Chicago, University of Medicine and Dentistry of New Jersey, New Brunswick, NJ, Virginia Mason Research Center, Seattle, WA, Wayne State University, Detroit, MI, University of Connecticut, Farming-ton, University of California, San Francisco, and University of Texas, Houston.
REFERENCES
1. Medsger TA Jr. Systemic sclerosis (scleroderma): clinical aspects. In: Koopman WJ, editor. Arthritis and allied conditions: a text-book of rheumatology. 13th ed. Baltimore: Williams & Wilkins; 1997. p. 1433–64.
2. Steen VD, Conte C, Owens GR, Medsger TA Jr. Severe restrictive lung disease in systemic sclerosis. Arthritis Rheum 1994;37: 1283–9.
3. Ware JE Jr, Sherbourne CD. The MOS 36-item Short-Form health survey (SF-36). I. Conceptual framework and item selec-tion. Med Care 1992;30:473–83.
4. Steen VD, Medsger TA Jr. The value of the Health Assessment Questionnaire and special patient-generated scales to demonstrate change in systemic sclerosis patients over time. Arthritis Rheum 1997;40:1984–91.
5. Mahler DA, Weinberg DH, Wells CK, Feinstein AR. The mea-surement of dyspnea: contents, interobserver agreement, and physiologic correlates of two new clinical indexes. Chest 1984;85: 751–8.
6. Crapo RO, Morris AH, Gardner RM. Reference spirometric
values using techniques and equipment that meet ATS recommen-dations. Am Rev Respir Dis 1981;123:659–64.
7. Crapo RO, Morris AH. Standardized single breath normal values for carbon monoxide diffusing capacity. Am Rev Respir Dis 1981;123:185–9.
8. Clements PJ, Hurwitz EL, Wong WK, Seibold JR, Mayes M, White B, et al. Skin thickness score as a predictor and correlate of outcome in systemic sclerosis: high-dose versus low-dose penicil-lamine trial. Arthritis Rheum 2000;43:2445–54.
9. Subcommittee for Scleroderma Criteria of the American Rheu-matism Association Diagnostic and Therapeutic Criteria Commit-tee. Preliminary criteria for the classification of systemic sclerosis (scleroderma). Arthritis Rheum 1980;23:581–90.
10. Ware JE, Kosinski M, Keller S. SF-36 physical and mental health summary scales: a user’s manual. Boston: Health Institute, New England Medical Center; 1994.
11. Fries JF, Spitz P, Kraines RG, Holman HR. Measurement of patient outcome in arthritis. Arthritis Rheum 1980;23:137–45. 12. Poole JL, Steen VD. The use of the Health Assessment
Question-naire (HAQ) to determine physical disability in systemic sclerosis. Arthritis Care Res 1991;4:27–31.
13. Clements PJ, Wong WK, Hurwitz EL, Furst DE, Mayes M, White B, et al. Correlates of the disability index of the Health Assessment Questionnaire: a measure of functional impairment in systemic sclerosis. Arthritis Rheum 1999;42:2372–80.
14. Clements PJ, Wong WK, Hurwitz EL, Furst DE, Mayes M, White B, et al. The disability index of the Health Assessment Question-naire is a predictor and correlate of outcome in the high-dose versus low-dose penicillamine in systemic sclerosis trial. Arthritis Rheum 2001;44:653–61.
15. Khanna D, Furst DE, Clements PJ, Park GS, Hays RD, Seibold JR. Responsiveness of the health related quality of life (HRQL) instruments (SF-36 and HAQ-DI) in a systemic sclerosis (SSc) clinical trial [abstract]. Arthritis Rheum 2003;48 Suppl 9:S398. 16. Merkel PA, Herlyn K, Martin RW, Anderson JJ, Mayes MD, Bell
P, et al. Measuring disease activity and functional status in patients with scleroderma and Raynaud’s phenomenon. Arthritis Rheum 2002;46:2410–20.
17. American Thoracic Society. Lung function testing: selection of reference values and interpretative strategies. Am Rev Respir Dis 1991;144:1202–18.
18. Mahler DA, Mackowiak JI. Evaluation of the Short-Form 36-item questionnaire to measure health-related quality of life in patients with COPD. Chest 1995;107:1585–9.
19. Chang JA, Curtis JR, Patrick DL, Raghu G. Assessment of health-related quality of life in patients with interstitial lung disease. Chest 1999;116:1175–82.
20. Martinez TY, Pereira CA, dos Santos ML, Ciconelli RM, Guima-raes SM, Martinez JA. Evaluation of the Short-Form 36-item questionnaire to measure health-related quality of life in patients with idiopathic pulmonary fibrosis. Chest 2000;117:1627–32. 21. Reveille JD, Fischbach M, McNearney T, Friedman AW, Aguilar
MB, Lisse J, et al. Systemic sclerosis in 3 US ethnic groups: a comparison of clinical, sociodemographic, serologic, and immuno-genetic determinants. Semin Arthritis Rheum 2001;30:332–46.