ORIGINAL ARTICLE
Vitamin D Deficiency and Osteoporosis in Rehabilitation
Inpatients
Leonid M. Shinchuk, MD, Leslie Morse, DO, Nadia Huancahuari, Seth Arum, MD, Tai C. Chen, PhD, Michael F. Holick, MD, PhD
ABSTRACT. Shinchuk LM, Morse L, Huancahuari N, Arum S, Chen TC, Holick MF. Vitamin D deficiency and osteoporosis in rehabilitation inpatients. Arch Phys Med Re-habil 2006;87:904-8.
Objective:To determine vitamin D status and bone mineral density (BMD) in patients admitted to a subacute rehabilitation facility.
Design:Cross-sectional cohort study. Setting: Subacute rehabilitation facility.
Participants: Fifty-three community-dwelling patients ad-mitted from June through February 2005.
Interventions:Not applicable.
Main Outcome Measures: BMD, 25-hydroxyvitamin D
(25[OH]D), C-telopeptide (CTX), osteocalcin, and dietary milk intake.
Results: Prevalence of vitamin D deficiency (25[OH]D ⬍20ng/mL) was 49.1%, while a total of 83% of patients were either vitamin D deficient or insufficient (25[OH]D ⬍30ng/ mL). The prevalence of osteopenia (T score, ⬍⫺1) was 52.8%; osteoporosis (T score, ⬍⫺2.5) was 17.0%. CTX (bone resorption marker) was elevated in 60.4% of patients. Osteocalcin (bone formation marker) was elevated in 13.2% of patients. Measurements of bone resorption and formation positively correlated (R2⫽.22) indicating increased bone remodeling.
Conclusions:Vitamin D deficiency and osteopenia and osteo-porosis were highly prevalent in patients admitted for rehabilita-tion. Elevated bone resorption and remodeling were evident. This could be due to vitamin D deficiency that should be corrected before antiresorptive therapy is considered. The study emphasizes the need for vigilance for vitamin D status and BMD testing in patients admitted to rehabilitation facilities.
Key Words: Bone density; Osteoporosis; Rehabilitation; Vitamin D deficiency.
©2006 by the American Congress of Rehabilitation Medi-cine and the American Academy of Physical MediMedi-cine and Rehabilitation
V
ITAMIN D IS ESSENTIAL for maintaining calcium and phosphorus homeostasis, and optimizing bone health. The active form of vitamin D, 1,25-dihydroxyvita-min D (1,25[OH]2D), acts on specific nuclear receptors to increase calcium absorption from the small intestine and to regulate bone turnover.1 Vitamin D deficiency leads to second-ary hyperparathyroidism and, if not treated, to development of osteoporosis with subsequent increase in fracture risk.2-4 Ad-ditionally, 1,25(OH)2D binds to receptors on skeletal mus-cles.5-8Recent studies9-11showed strong association between higher serum vitamin D concentrations and muscle strength, physical activity, and reduced falls in elderly.Vitamin D can be obtained from diet or synthesized in the skin under appropriate intensity and duration of ultraviolet radiation.12,13Vitamin D is biologically inert and must undergo 2 successive hydroxylations in the liver and kidney to become the biologically active 1,25(OH)2D.
1
Factors that interfere with vitamin D intake, absorption, synthesis, or metabolism result in vitamin D deficiency. Advanced age, nonwhite ethnicity, poor dietary intake, increased body mass index (BMI), in-adequate sun exposure, northern latitude, and medications that impair vitamin D activation or accelerate clearance are known risk factors for vitamin D deficiency.14 However, standard clinical risk factors are poor predictors of vitamin D status.15
The prevalence of vitamin D deficiency in community-dwelling elderly is estimated to be between 25% and 54%.16 The prevalence of vitamin D deficiency in medical inpatients was reported around 57%.15Untreated, vitamin D deficiency will lead to development of osteopenia and osteoporosis de-fined by World Health Organization (WHO) as bone mass 1 and 2.5 standard deviations (SDs) below the sex-controlled young adults, respectively. In the United States, 40% of women over the age of 50 have osteopenia and 7% suffer from osteo-porosis.17 Vitamin D deficiency is also highly prevalent in men. In the United States, 3.5 million men over the age of 65 have osteopenia and 1.5 million suffer from osteoporo-sis.18Osteoporosis is a silent disease with the first manifes-tation being development of pathologic fracture. There are approximately 1.3 million osteoporotic fractures each year in the United States with an estimated cost of $13.8 billion in 1995.19
Patients who require a subacute rehabilitation stay after an acute hospitalization possess multiple risk factors for vitamin D deficiency and are at risk of osteopenia and osteoporosis. Frequently, these patients are older, medically complex, and suffer from reduced mobility and poor nutritional status. The goal of this study was to determine vitamin D status and the prevalence of vitamin D deficiency in this vulnerable group of patients. In addition, we determined the prevalence of osteopenia and osteoporosis, ascertained factors related to vitamin D deficiency and low bone mineral density (BMD), and determined bone resorption and formation activity in these patients.
From the Departments of Physical Medicine and Rehabilitation (Shinchuk, Morse) and Medicine (Huancahuari, Arum, Chen, Holick), Boston University Medical Cen-ter, Boston, MA.
Presented to the American Academy of Physical Medicine and Rehabilitation, October 28, 2005, Philadelphia, PA.
Supported by the National Institutes of Health (grant no. M01RR 00533). No commercial party having a direct financial interest in the results of the research supporting this article has or will confer a benefit upon the authors or upon any organization with which the authors are associated.
Correspondence to Michael F. Holick, MD, PhD, Boston University School of Medicine, 715 Albany St, #M1013, Boston, MA 02118, e-mail:[email protected].
Reprints are not available from the author. 0003-9993/06/8707-10592$32.00/0 doi:10.1016/j.apmr.2006.03.009
METHODS Study Participants
From June 2004 to February 2005, we recruited a cohort of inpatients admitted to a subacute rehabilitation facility at Bos-ton Medical Center to participate in the study. Subjects were excluded if they were younger than 21 years old, pregnant, not proficient in English, or were taking vitamin D or calcium supplementation. The study was approved by the institutional review board and signed informed consent was obtained from each subject prior to enrollment.
Study Conduct
Subjects attended a single study visit at the General Clinical Research Center where demographic information, height, and weight were recorded. A dual x-ray absorptiometry (DXA) scan was performed on a QDR 4500 Hologic bone densitom-eter.aA single blood sample was collected to assess 25(OH)D, osteocalcin, and C-telopeptide (CTX). A questionnaire was administered to ascertain pertinent medical, dietary, and med-ication history.
Laboratory Studies
We determined serum 25(OH)D using a Nichols Advantage Specialty Systembwith a 6.4% to 14.5% interassay coefficient of variation (CV). The normative range for adults is 20 to 100ng/mL.
We measured CTX utilizing the Serum CrossLaps ELISAc kit. The detection limit was .01ng/mL. The intra- and interas-say CV ranges from 5.0% and 8.0%, respectively. Mean ob-served reference values for premenopausal women, postmeno-pausal women, and men are 0.32⫾0.16, 0.51⫾0.26, and 0.33⫾0.19ng/mL, respectively.
We measured osteocalcin with a Nichols Advantage system. The assay has sensitivity of 0.1ng/mL, and the intra- and interassay CV ranges from 4.6% to 5.3% and 7.3% to 9.5%, respectively. The reference values of osteocalcin for premeno-pausal women and men range from 0.5 to 7.0ng/mL and 1.1 to 7.2ng/mL, respectively.
Outcome Measures
The major outcome measures include vitamin D inadequacy, bone resorption and formation activity, prevalence of osteope-nia and osteoporosis, and milk consumption data. Various cut-points of serum 25(OH)D were used to define vitamin D inadequacy (⬍9,⬍15,⬍20,⬍25,⬍30ng/mL). An increase in bone resorption activity was defined as CTX levels above the normative range provided by the manufacturer for premeno-pausal women, postmenopremeno-pausal women, and men. An in-crease in bone formation was defined as osteocalcin levels above the normative range provided by the manufacturer for premenopausal women and men. The normative range for osteocalcin for postmenopausal women is unknown, so the value for premenopausal women was used instead, which may have led to underestimation of the results. Osteopenia and osteoporosis were defined based on the WHO classification. Inadequate milk consumption was defined as self-reported in-take of less than 1 glass of milk a day prior to hospitalization. Statistical Analysis
We calculated the distribution of serum 25(OH)D and the percentage of patients below 9, 15, 20, 25, and 30ng/mL and associated 95% confidence intervals (CIs). Prevalence of vita-min D deficiency and associated CIs by sex and race were
ascertained. The Pearson correlation coefficient was calculated to assess the relation between serum 25(OH)D, age, and BMI. We calculated the prevalence of osteopenia, osteoporosis, increased CTX and osteocalcin, and milk consumption with associated 95% CIs. The Pearson correlation coefficient was calculated to assess the relation between CTX and osteocalcin. We performed group comparisons by sex and race for serum 25(OH)D less than 20ng/mL and less than 30ng/mL, osteope-nia, osteoporosis, and inadequate milk consumption based on chi-square or Fisher exact tests as appropriate. APvalue of .05 or less was considered statistically significant.
All analyses were performed using SAS statistical software.d RESULTS
Participants
Sixty-one patients met inclusion criteria. Eight (13.1%) pa-tients were excluded from the study (3 papa-tients withdrew consent, 4 patients did not provide sufficient material for serum measurements, 1 patient was discharged prior to completion of the study). Fifty-three (86.9%) patients provided a blood sam-ple for determination of serum 25(OH)D, osteocalcin, and CTX, underwent DXA scan, and completed the questionnaire. Subjects’ mean age was 60.2⫾14.1 years and included 30 (56.6%) men, 23 (43.4%) women, 29 (54.7%) whites, 20 (37.7%) African Americans, 2 (5.7%) Hispanics, and 1 (1.9%) Asian. Forty-nine (92.5%) patients were ambulatory prior to admission, 3 (5.7%) patients were housebound, and 1 (1.9%) patient was homeless. None of the patients was a nursing home resident. Patients’ demographics are summarized intable 1.
The length of acute hospitalization prior to transfer to the transitional care unit was 7.2⫾5.3 days. Forty-three (81.1%) patients were transferred from a surgical service (23 [43.4%] patients after joint replacement, 8 [15.1%] patients after other orthopedic procedure, 12 [22.6%] patients after surgical non-orthopedic procedure). Ten (18.9%) patients were transferred from a medical service. Three (5.7%) patients were receiving therapy with glucocorticoids, 3 (5.7%) were taking anticonvul-sant agents (phenytoin, phenobarbital, or carbamazepine), 1 (1.9%) patient was receiving both glucocorticoid and anticon-vulsant agents, and none of the patients were taking rifampin.
Table 1: Demographics Characteristic Total (N⫽53) Age (y) 60.2⫾14.1 Sex Male 30 (56.6) Female 23 (43.4) Ethnicity White 29 (54.7) Black 20 (37.7) Hispanic 3 (5.7) Asian 1 (1.9) Other 0 (0.0)
Residential and functional status
Ambulatory 49 (92.5) Housebound 3 (5.7) Nursing home resident 0 (0.0) Homeless 1 (1.9) BMI (kg/m2) 29.0⫾6.5 NOTE. Values are mean⫾SD or n (%).
Prevalence of Low Serum 25(OH)D
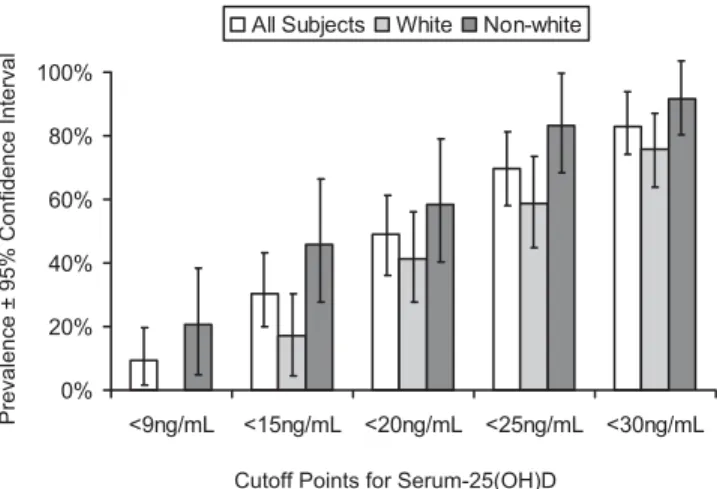
Several cutpoints were used to describe the prevalence of vitamin D inadequacy in the study population (fig 1). We found that 83.0% (95% CI, 72.9%–93.1%) of subjects had a serum 25(OH)D less than 30ng/mL and 49.1% (95% CI, 35.6%– 62.6%) had values less than 20ng/mL. Vitamin D deficiency (⬍20ng/mL) was equally present in men (46.7%) and women (52.2%). The prevalence of vitamin D deficiency was 41.4% in white patients and 58.3% in nonwhite patients (seefig 1). There was no difference in the prevalence of vitamin D deficiency during seasonal peak (June–September) and the other months (October–February), 51.7% and 45.8%, respectively. Age and BMI did not correlate with 25(OH)D (r2⫽.005 andr2⫽.097, respectively).
Prevalence of Osteopenia and Osteoporosis
Exactly 53.3% (95% CI, 35.4%–71.2%) of men and 52.2% (95% CI, 31.8%–72.6%) of women had osteopenia (T score of
⬍⫺1.0) and 20% (95% CI, 5.7%–.34.3%) of men and 13% (95% CI, 0%–26.7%) of women had osteoporosis (T score
⬍⫺2.5) (fig 2). Prevalence of osteopenia in white and non-white patients was 51.7% and 54.2%, respectively, while prev-alence of osteoporosis was 6.9% and 29.2%, respectively (see
fig 2).
Markers of Bone Resorption and Formation
In this patient population, 60.4% (95% CI, 47.2%–73.6%) of patients had an increase in bone resorption (CTX⬎.52ng/mL in men,⬎.48ng/mL in premenopausal women,⬎.77ng/mL in postmenopausal women), and 13.2% (95% CI, 4.1%–22.3%) of patients had an increase in bone formation (osteocalcin
⬎7.0ng/mL in women;⬎7.2ng/mL in men). Bone formation and resorption activity correlated weakly (r2⫽.22), indicating an increase in bone remodeling.
Milk Intake
Forty-nine percent (95% CI, 35.5%– 62.5%) of patients re-ported consuming less than 1 glass of milk a day prior to hospitalization (53.3% men, 47.8% women) while 13.2% (95% CI, 4.1%–22.3%) consumed more than 2 glasses a day (10.0% men, 17.4% women). Inadequate milk consumption was more
prevalent in African Americans (66.7%) than in whites (38.0%) (P⫽.027).
DISCUSSION
In this study of 53 patients admitted to a rehabilitation facility after an acute hospitalization, we found a high preva-lence of vitamin D deficiency in both male and female inpa-tients. There was no statistical difference in vitamin D deficiency between white and nonwhite patients; even so, there was a ten-dency for a higher prevalence of vitamin D deficiency in the nonwhite cohort. Given a relatively short duration of preceding acute hospitalization for the majority of patients, the observed prevalence of vitamin D deficiency is likely a premorbid char-acteristic of the group because the serum half-life for 25(OH)D is approximately 2 weeks.14Interestingly, neither age nor BMI correlated with 25(OH)D level (r2⫽.005 andr2⫽.097, respec-tively). One explanation might be that the younger or more overweight patients who require rehabilitation stay prior to returning home are more medically affected and therefore more likely to develop vitamin D deficiency.
Although previous studies described vitamin D deficiency in the general population and in medical inpatients, this study was aimed at evaluating a population of patients who require a subacute level rehabilitation stay after an acute hospitalization. This group of patients is at a higher risk to develop vitamin D deficiency given the reduced mobility and medical complexity that necessitated the rehabilitation stay. Clearly, little has been done to address vitamin D deficiency in these patients. As we reported previously, the prescription rate of vitamin D and/or calcium supplementation on admission to subacute rehabilita-tion was only about 12% indicating that this group remains an underdiagnosed and undertreated high-risk population for vi-tamin D deficiency.20
Osteopenia and osteoporosis were highly prevalent on the subacute rehabilitation unit. Patients of both sexes and all races were equally affected. The combined prevalence of osteopenia and osteoporosis was 69.8%. It was previously reported that 25(OH)D levels correlate positively with BMD in young and older adults.21Additionally, vitamin D plays an important role in the maintenance of proximal muscle strength and reduction of falls.22-25 Long-term vitamin D and calcium supplementa-tion was shown to reduce the risk of nonvertebral fractures by 32% to 58%.26,27Bischoff et al28demonstrated in a random-ized controlled trial that daily vitamin D and calcium
supple-0% 20% 40% 60% 80% 100% Osteopenia Osteoporosis Male Female White Non-white
T score < -2.5
Prevalence of O
s
teopenia/Os
teoporosis
T score as Defined by WHO T score < -1
Fig 2. Prevalence of osteopenia and osteoporosis in male and fe-male, white and nonwhite patients. T scores as defined by WHO (osteopenia T score<ⴚ1 SD; osteoporosis T score<ⴚ2.5 SD sex-and race-controlled young adults).
0% 20% 40% 60% 80% 100% <9ng/mL <15ng/mL <20ng/mL <25ng/mL <30ng/mL All Subjects White Non-white
Cutoff Points for Serum-25(OH)D
Prevalence ±
9
5% C
onfidence Interval
Fig 1. Prevalence of vitamin D inadequacy in all subjects, white and nonwhite patients. The percentage of subjects with serum 25(OH)D concentrations below predefined cutoffs of<9,<15,<20,<25, and <30ng/mL.
mentation improve musculoskeletal function (knee flexor and extensor strength, grip strength, and Timed Up & Go test) and reduces the risk of falls by 49% in long-term care facility patients. In a recently published meta-analysis,29 the risk of falls among ambulatory or institutionalized older subjects with stable health was reduced by more than 20% compared with placebo. Thus, the combination of established osteopenia and osteoporosis and vitamin D deficiency puts the subacute reha-bilitation inpatients in an especially high risk group of acquir-ing an osteoporotic fracture. Treatment with vitamin D and calcium supplementations will likely benefit the patients by improving their BMD and musculoskeletal function.
We evaluated bone turnover activity by measurement of CTX and osteocalcin. There was significant bone resorption activity as evident by an increased CTX in 60.4% of the patients. At least 13.2% of patients had an increase in bone formation as evidenced by an increased osteocalcin. Overall, bone formation and bone resorption markers positively corre-lated (r2⫽.22), indicating an increase in bone remodeling.
Exactly 58.5% of patients underwent an orthopedic interven-tion during the acute hospitalizainterven-tion. Similar results for mark-ers of bone resorption (CTX) and formation (osteocalcin) were obtained evaluating subgroups with and without recent ortho-pedic procedures. Markers of bone resorption and formation were elevated in 54.8% and 9.7% of patients after an orthope-dic procedure, respectively, and in 68.2% and 18.2% of pa-tients, respectively, who did not have an orthopedic interven-tion.
Bone turnover markers are much more sensitive to metabolic changes in bone than BMD.30 It is unclear if substantially increased bone resorption activity in rehabilitation inpatients is due to a preceding period of relative inactivity during an acute hospitalization or to their baseline medical status and vitamin D deficiency. Caution must be taken when interpreting these results. Nevertheless, the changes in bone turnover markers are strong predictors of reduced fracture risk.31
Casual exposure to sunlight provides most of the vitamin D requirement.1 However, elderly people have decreased ability to synthesize vitamin D. Compared with young adults, a person older than 70 years of age produces less than 30% of the amount of vitamin D3when exposed to the same amount of sunlight.
32 Cutaneous synthesis of vitamin D also depends on the exposure to appropriate ultraviolet radiation, which depends on time of the day, season, and latitude. In Boston, MA (latitude 42°N), sunlight is incapable of producing vitamin D3 in the skin between the months of November and February.33Thus, pa-tients with limited mobility and the elderly who live in the northern latitudes must rely extensively on oral intake to cover the daily vitamin D requirement. The recommended daily oral vitamin D intake in the United States is 200IU for adults up to 50 years old, 400IU for adults 51 to 70, and 600IU for men and women over 71.34
Milk is fortified with vitamin D. One glass provides approx-imately 100IU or from 17% to 50% of daily requirement depending on age.35Most dairy products, such as cheese and most yogurts, are not fortified with vitamin D. Thus, milk itself remains the main source of vitamin D. In our patient popula-tion, 49.1% of patients consumed less than 1 glass of milk a day. Dietary preferences or the higher prevalence of lactose intolerance with age, especially in the African-American pop-ulations, might explain these findings. However, it is clear that patients need to rely on other sources, either dietary or phar-macologic, to obtain adequate amounts of vitamin D.
Although the relatively small sample size and the use of a single subacute site in Boston, MA, as a referral base limit the generalization of results, the high prevalence of vitamin D
deficiency that we observed should alert physicians about hy-povitaminosis D in rehabilitation inpatients at other medical centers. The study excluded patients who were taking vitamin D or calcium supplementations. These patients were represent-ing less than 12% of all patients admitted, so excludrepresent-ing them did not significantly bias the reported prevalence of hypovita-minosis D. However, care must be taken to insure adequate vitamin D supplementation in that group as recent studies demonstrated high prevalence of vitamin D deficiency even in patients on pharmacologic therapy to treat osteoporosis and taking a multivitamin that contained vitamin D.36
CONCLUSIONS
Vitamin D deficiency and osteopenia and osteoporosis are highly prevalent in both men and women admitted for subacute rehabilitation after an acute hospitalization. Bone remodeling activity was elevated with a disproportional increase in bone resorption. This could be due to vitamin D deficiency that should be corrected before antiresorptive therapy is considered. This study emphasizes the need for vigilance for vitamin D status and BMD testing in patients admitted to rehabilitation facilities.
References
1. Holick MF. Vitamin D: photobiology, metabolism, mechanism of action, and clinical applications. In: Favus MJ, editor. Primer on the metabolic bone diseases and disorders of mineral metabolism. 5th ed. Philadelphia: Lippincott; 1999. p 92-8.
2. Kinyamu HK, Gallagher JC, Balhorn KE, Petranick KM, Rafferty KA. Serum vitamin D metabolites and calcium absorption in normal young and elderly free-living women and in women living in nursing homes. Am J Clin Nutr 1997;65:790-7.
3. Aaron JE, Gallagher JC, Anderson J, et al. Frequency of osteo-malacia and osteoporosis in fracture of the proximal femur. Lancet 1974;1:229-33.
4. Holick MF. Vitamin D: a millenium perspective. J Cell Biochem 2003;1;88:296-307.
5. Simpson RU, Thomas GA, Arnold AJ. Identification of 1,25-dihydroxyvitamin D3receptors and activities in muscle. J Biol
Chem 1985;260:8882-91.
6. Costa EM, Blau HM, Feldman D. 1,25-dihydroxyvitamin D3
receptors and hormonal responses in cloned human skeletal mus-cle cells. Endocrinology 1986;119:2214-20.
7. Haddad JG, Walgate J, Min C, Hahn TJ. Vitamin D metabolite-binding proteins in human tissue. Biochim Biophys Acta 1976; 22;444:921-5.
8. Bischoff HA, Borchers M, Gudat F, et al. In situ detection of 1,25-dihydroxyvitamin D3receptor in human skeletal muscle
tis-sue. Histochem J 2001;33:19-24.
9. Mowe M, Haug E, Bohmer T. Low serum calcidiol concentration in older adults with reduced muscular function. J Am Geriatr Soc 1999;47:220-6.
10. Dhesi JK, Bearne LM, Moniz C, et al. Neuromuscular and psy-chomotor function in elderly subjects who fall and the relationship with vitamin D status. J Bone Miner Res 2002;17:891-7. 11. Venning G. Recent developments in vitamin D deficiency and
muscle weakness among elderly people. BMJ 2005;330:524-6. 12. Holick MF, MacLaughlin JA, Clark MB, et al. Photosynthesis of
previtamin D3in human skin and the physiologic consequences.
Science 1980;210:203-5.
13. MacLaughlin JA, Anderson RR, Holick MF. Spectral character of sunlight modulates photosynthesis of previtamin D3and its
pho-toisomers in human skin. Science 1982;216:1001-3.
14. Holick MF. Sunlight and vitamin D for bone health and preven-tion of autoimmune disease, cancers, and cardiovascular disease. Am J Clin Nutr 2004;80(6 Suppl):1678S-88S.
15. Thomas MK, Lloyd-Jones DM, Thadhani RI, et al. Hypovitamin-osis D in medical inpatients. N Engl J Med 1998;338:777-83. 16. Gloth FM 3rd, Tobin JD. Vitamin D deficiency in older people.
J Am Geriatr Soc 1995;43:822-8.
17. Siris ES, Miller PD, Barrett-Connor E, et al. Identification and fracture outcomes of undiagnosed low bone mineral density in postmenopausal women: results from the National Osteoporosis Risk Assessment. JAMA 2001;286:2815-22.
18. Siddiqui NA, Shetty KR, Duthie EH Jr. Osteoporosis in older men: discovering when and how to treat it. Geriatrics 1999;54(9): 20-2, 27-8, 30.
19. Ray NF, Chan JK, Thamer M, Melton LJ 3rd. Medical expendi-tures for the treatment of osteoporotic fracexpendi-tures in the United States in 1995: report from the National Osteoporosis Foundation. J Bone Miner Res 1997;12:24-35.
20. Shinchuk LM, Huancahuari N, Ingersoll D, Holick MF. Vitamin D deficiency and osteoporosis: highly prevalent in men and women admitted to subacute rehabilitation facility in Boston, Massachusetts during summer [abstract]. Am J Phys Med Rehabil 2005;84:203.
21. Bischoff-Ferrari HA, Dietrich T, Orav EJ, Dawson-Hughes B. Positive association between 25-hydroxy vitamin D levels and bone mineral density: a population-based study of younger and older adults. Am J Med 2004;116:634-9.
22. Janssen HC, Samson MM, Verhaar HJ. Vitamin D deficiency, muscle function, and falls in elderly people. Am J Clin Nutr 2002;75:611-5.
23. Pfeifer M, Begerow B, Minne HW, et al. Vitamin D status, trunk muscle strength, body sway, falls, and fractures among 237 post-menopausal women with osteoporosis. Exp Clin Endocrinol Dia-betes 2001;109:87-92.
24. Sato Y, Inose M, Higuchi I, Higuchi F, Kondo I. Changes in the supporting muscles of the fractured hip in elderly women. Bone 2002;30:325-30.
25. Dhesi JK, Bearne LM, Moniz C, et al. Neuromuscular and psy-chomotor function in elderly subjects who fall and the relationship with vitamin D status. J Bone Miner Res 2002;17:891-7. 26. Chapuy MC, Arlot ME, Delmas PD, Meunier PJ. Effect of
cal-cium and cholecalciferol treatment for three years on hip fractures in elderly women. BMJ 1994;308:1081-2.
27. Dawson-Hughes B, Harris SS, Krall EA, Dallal GE. Effect of calcium and vitamin D supplementation on bone density in men
and women 65 years of age or older. N Engl J Med 1997;337: 670-6.
28. Bischoff HA, Stahelin HB, Dick W, et al. Effects of vitamin D and calcium supplementation on falls: a randomized controlled trial. J Bone Miner Res 2003;18:343-51.
29. Bischoff-Ferrari HA, Dawson-Hughes B, Willett WC, et al. Effect of vitamin D on falls: a meta-analysis. JAMA 2004;291:1999-2006.
30. Greenspan SL, Resnick NM, Parker RA. Early changes in bio-chemical markers of bone turnover are associated with long-term changes in bone mineral density in elderly women on alendronate, hormone replacement therapy, or combination therapy: a three-year, double-blind, placebo-controlled, randomized clinical trial. J Clin Endocrinol Metab 2005;90:2762-7.
31. Eastell R, Barton I, Hannon RA, Chines A, Garnero P, Delmas PD. Relationship of early changes in bone resorption to the reduction in fracture risk with risedronate. J Bone Miner Res 2003;18:1051-6.
32. Holick MF, Matsuoka LY, Wortsman J. Age, vitamin D, and solar ultraviolet. Lancet 1989;2:1104-5.
33. Holick MF. McCollum Award Lecture, 1994: vitamin D—new horizons for the 21st century. Am J Clin Nutr 1994;60:619-30. 34. Institute of Medicine, Food and Nutrition Board. Dietary reference
intakes: calcium, phosphorus, magnesium, vitamin D and fluoride. Washington (DC): Natl Acad Pr; 1999.
35. Dietary reference intakes: applications in dietary assessment. A Report of the Subcommittees on Interpretation and Uses of Di-etary Reference Intakes and Upper Reference Levels of Nutrients, and the Standing Committee on the Scientific Evaluation of Di-etary Reference Intakes, Food and Nutrition Board. Washington (DC): Natl Acad Pr; 2000. p 106-12.
36. Holick MF, Siris ES, Binkley N, et al. Prevalence of vitamin D inadequacy among postmenopausal North American women re-ceiving osteoporosis therapy. J Clin Endocrinol Metab 2005;90: 3215-24.
Suppliers
a. Hologic Inc, 35 Crosby Dr, Bedford, MA 01730.
b. Nichols Advantage, 1311 Calle Batido, San Clemente, CA 92673. c. Nordic Bioscience Diagnostics A/S, Herlev Hovedgade 207, 2730
Herlev, Denmark.