Review Article
Comparison of the peri- and postoperative
parameters between artery-only and artery-vein
clamping techniques in partial nephrectomy:
a systematic review and meta-analysis
Wei Liu1*, Fang Wang2*, Hui Ding1, Xingchen Liu1, Jinhui Tian3, Yuwen Gong1, Diyin Li1, Hanzhang Wang4,
Dharam Kaushik4, Ronald Rodriguez4, Zhiping Wang1
1Institute of Urology, Lanzhou University Second Hospital, Key Laboratory of Gansu Province for Urological
Diseases, Gansu Nephro-Urological Clinical Center, Lanzhou 730030, Gansu Province, P.R. China; 2Reproductive
Medicine Center, Lanzhou University Second Hospital, Lanzhou 730030, P.R. China; 3Evidence-based Medicine
Center of Lanzhou University, Key Laboratory of Evidence-based Medicine and Knowledge Translation of Gansu Province, Lanzhou 730000, P.R. China; 4Department of Urology, University of Texas Health Science Center at San
Antonio, 7703 Floyd Curl Drive, San Antonio, Texas 78229-3900, USA. *Equal contributors.
Received September 19, 2017; Accepted January 23, 2018; Epub March 15, 2018; Published March 30, 2018
Abstract: Renal artery-only (AO) and renal artery-vein (AV) clamping are known as the conventional hilar clamping techniques in partial nephrectomy (PN), but there is a paucity of data comprehensively comparing the two tech-niques. This meta-analysis aimed to compare the peri- and postoperative outcomes between AO and AV clamping techniques in PN. Electronic databases including Pubmed, Embase, Web of Science, and the Cochrane Library were searched. Randomized controlled trials (RCTs) and observational comparative studies, providing data of pa-tient baseline variables, and peri- and postoperative outcomes of the two clamping techniques were included. Two reviewers independently screened literature, extracted data, and appraised the quality of the included studies. A meta-analysis was performed for the outcomes of interest. A total of five studies and 549 patients were included. The meta-analysis showed that AV clamping PN had a shorter operative time (P = 0.003) when compared with AO clamping PN. No significant differences were detected between the two groups in estimated blood loss (EBL) (P = 0.15), blood transfusion rate (P = 0.71), urine leakage rate (P = 0.36), postoperative complication rate (P = 1.00), and positive margin rate (P = 0.81). A descriptive analysis showed that AV clamping could get comparable re-sults for renal function after surgery when compared with AO clamping technique. In conclusion, this meta-analysis shows that AV clamping is comparable with AO clamping technique with regard to peri- and postoperative outcomes. Considering the inherent limitations of the included studies, the result should be carefully applied based on appro-priate patient selection. Thus well-designed randomized future clinical trials are needed.
Keywords: Partial nephrectomy, renal artery, meta-analysis
Introduction
Partial nephrectomy (PN) has been widely used in localized renal tumors. As European Associa- tion of Urology (EAU) guidelines recommended, radical nephrectomy (RN) should not be per-formed in patients with T1 tumors for whom PN is indicated [1]. Compared with RN, PN confers a survival advantage and a lower risk of severe chronic kidney disease after surgery for local-ized renal tumors [2].
Irrespective of the surgical technique, clamping
clinical trials [4, 7-10] compared peri- and post-operative parameters during PN with AV and AO clamping. However, there is paucity of data comprehensively comparing the two clamping techniques which impacts on surgical tech-nique, estimated blood loss (EBL), postopera-tive renal function, and other peri- and postop-erative outcomes. Therefore, we sought to per-form a systematic review and meta-analysis.
Material and methods
Literature acquisition
This systematic review was performed following the Meta-analysis of Observational Studies in Epidemiology (MOOSE) guidelines [11]. To iden-tify relevant studies, electronic databases in- cluding Pubmed, Embase, Web of Science, and the Cochrane Library were searched with no time and language restrictions. The search terms were ‘(artery OR hilar OR hilum) [Title/ Abstract] AND (clamp OR occlusion) [Title/ Abstract] AND (partial nephrectomy OR neph-ron sparing) [Title/Abstract]’. The references of retrieved articles were searched to identify re- lated articles. The initial search was conducted on March 18, 2017, and an updating search was finished on June 25, 2017 and there was no extra studies appropriate for inclusion. The searching was finished including a team mem-ber with dedicated expertise in literature sear- ches (J. T.).
Inclusion and exclusion criteria
Studies were included by the following criteria: (i) randomized controlled trials (RCTs) and ob- servational comparative studies, providing da- ta of patient baseline variables, perioperative parameters and postoperative outcomes dur-ing PN, (ii) surgical technique was restricted to PN, (iii) direct comparisons between clamping techniques must include AO versus AV clamp-ing, (iv) the sample size of each group ≥10. Studies were excluded by the following criteria: (i) the inclusion criteria were not met, (ii) stud-ies were animal experiments, case reports, re- views and letters to editors, (iii) surgical tech-nique used cryoablation or radiofrequency ab- lation, (iv) the data was unavailable for statisti-cal analysis even after contacting authors to supply the missing information in published articles.
Literature screening and data extraction
Two reviewers independently identified studies for inclusion and used a standard data-extrac-tion form to collect data of included studies. Disagreements between reviewers were resol- ved by discussion or submitted to a third party for decision. The original data extracted were first author, year of publication, surgical tech-nique, number of patients and means of group allocation. The following outcomes of interest were important data to be extracted: (i) base-line variables of each group: age, sex ratio, bo- dy mass index (BMI), functional status, comor-bidities, tumor size, tumor location, R.E.N.A.L. nephrometry score, preoperative serum creati-nine (Pre-sCr) level, preoperative estimated glo-merular filtration rate (Pre-eGFR) and follow-up time. (ii) the primary outcomes were warm isch-emia time (WIT), changes in renal function, blood transfusion rate, urine leakage rate, con-versions rate, intra- and postoperative compli-cations, positive margin rate. (iii) the second- ary outcomes were operative time, estimated blood loss (EBL), and length of hospital stay. Methodological quality assessment
The Newcastle-Ottawa Scale (NOS) was used to assess the methodological quality of obser-vational studies [12]. The quality of included studies was judged by patient selection, com-parability on the basis of design or analysis, and ascertainment of either the exposure or outcome of interest. Scores measured with zero to nine stars were allocated to each study. Statistical analysis
heterogeneity and the I2 was used to evaluate
the quantity of heterogeneity between the included studies. A random-effects model was applied if heterogeneity existed. Otherwise, a fixed effects model was used. Meta-analysis was performed using the RevMan v.5.3 (The Cochrane Collaboration, Oxford, UK).
Results
We acquired 1929 studies after searching the four databases. Of the 1929 studies, 452 with repetitive contents were excluded and 1465 were excluded due to non-relevance based on the titles and abstracts. Full text of 12 studies were appraised, of which five studies [4, 7-10] were eventually included in the systematic review. The detailed process of literature selec-tion is shown in Figure 1.
Literature characteristics
The characteristics of included studies are sho- wn in Table 1. All of the included literature were
rate, hypertension rate, tumor in right side rate, preoperative eGFR, preoperative sCr and tumor size.
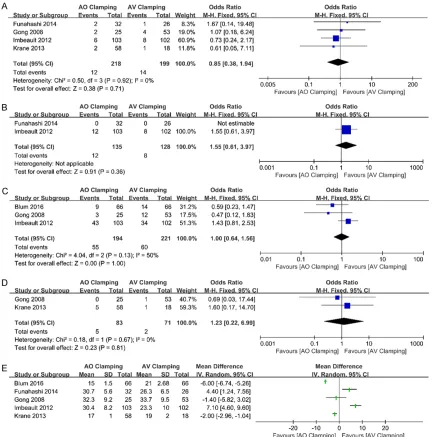
In terms of primary outcomes (Figure 2), there were no statistically significant differences in blood transfusion rate (OR: 0.85, 95% CI: 0.38 to 1.94, P = 0.71) and postoperative complica-tion rate (OR: 1.00, 95% CI: 0.64 to 1.56, P = 1.00). Only two studies [4, 8] reported urine leakage rate, and no significant difference was detected between AO and AV clamping group for meta-analysis. The same situation was seen for positive margin rate. Intraoperative compli-cation rate and open conversion rate was re- ported in only one study [7], respectively, and no statistical differences were reported bet- ween the two clamping techniques. Due to the contrasting results of included studies of WIT, a merge analysis has not yet been conducted. Changes of renal function in the AO and AV clamping groups were not suitable for quantita-tive synthesis, owing to different follow-up dura-Figure 1. Flowchart
depict-ing the process of literature selection.
cohort observational stud-ies with no randomization, and were published from the year of 2008 to 2016. Of the five included studies, three studies [4, 7, 8] com-pared AO with AV clamping during LPN, one study [10] conducted a comparison among AO clamping, AV clamping and unclamping techniques during RPN and another study [9] compared AO with AV clamping during RPN. Using the NOS to eval-uate the quality of included studies, four studies [4, 7- 9] scored seven stars and one study [10] scored five stars.
Meta-analysis results
[image:3.612.90.386.72.443.2]tions and different measuring variables. How- ever, a descriptive analysis was conducted and the results of it are shown in Table 3.
With regard to secondary outcomes (Figure 3), the meta-analysis of three studies [4, 7, 10] showed that operative time was significantly longer in AO clamping group than AV clamping group (MD: 6.63, 95% CI: 2.32 to 10.94, P = 0.003). Pooled data from five studies [4, 7-10] reported estimated blood loss (EBL) and sho- wed that EBL was less in the AO group (MD: -11.57, 95% CI: -15.47 to -7.68, P < 0.00001), but sensitivity analysis showed no significant difference between the two groups (MD: -6.98, 95% CI: -16.48 to 2.53, P = 0.15). Only one study [4] reported length of hospital stay, and found no significant difference between the AO and AV clamping group (4.5 days vs 3.9 days, P = 0.1218).
Discussion
This meta-analysis included five studies, which consisted of three LPNs and two RPNs. With regard to the primary and secondary outcomes,
operative time was significantly shorter in the AV clamping group, while, no statistically signifi-cant differences were detected for blood trans-fusion rate, urine leakage rate, postoperative complication rate, positive margin rate, and estimated blood loss in the AO and AV clamping groups.
Known as the critical step of PN, clamping of renal hilum has been studied by many research-ers. As a conventional technique, AV clamping has been favored despite the unnecessary indi-vidual dissection of the renal artery and vein [4]. It can provide a bloodless operative field for precise tumor excision and parenchymal clo-sure [14]. Our meta-analysis showed that the AV clamping technique does have a shorter operative time, which might be largely attribute to less extensive dissection of the renal vessels and better visualization than AO clamping. In contrast to the supposed superiority of AV clamping, meta-analysis of estimated blood loss showed that less bleeding was seen in AO clamping during PN. Seeing the forest plot in
[image:4.612.92.524.86.174.2]Figure 3, this meta-analysis result was largely determined by the study of “Blum 2016” [9].
Table 1. Characteristics and quality of included studies
First author,
year approachSurgical No. of pts: AO/AV Group allocation Clinical stage Follow-up duration: AO/AV NOS score
Funahashi, 2014 LPN 32/26 Prospective cohort NA 1 wk and 6 mos ☆☆☆☆☆☆☆
Gong, 2008 LPN 25/53 Matched retrospectively NA 21.9±11.8/10.1±9.9 mos ☆☆☆☆☆☆☆
Imbeault, 2012 LPN 103/102 Matched retrospectively Surgically eligible 44 (29-65)/15 (2-28) mos ☆☆☆☆☆☆☆
Krane, 2013 RPN 58/18 Prospective cohort (based
on Surgeon preference) NA At discharge and at last follow-up
☆☆☆☆☆
Blum, 2016 RPN 66/66 Matched retrospectively T1 9.5 (6.7-13.2)/8.1 (6.4-12.2) mos ☆☆☆☆☆☆☆
[image:4.612.91.528.224.372.2]Abbreviations: LPN, laparoscopic partial nephrectomy; RPN, robot-assisted partial nephrectomy; AO, artery-only (clamping); AV, artery-vein (clamping); No. of pts, number of patients; NA, not available; wk, week; mos, months.
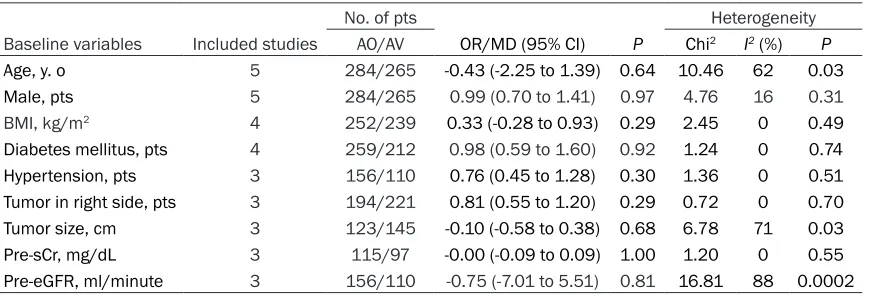
Table 2. Meta-analysis of baseline variables
No. of pts Heterogeneity
Baseline variables Included studies AO/AV OR/MD (95% CI) P Chi2 I2 (%) P
Age, y. o 5 284/265 -0.43 (-2.25 to 1.39) 0.64 10.46 62 0.03
Male, pts 5 284/265 0.99 (0.70 to 1.41) 0.97 4.76 16 0.31
BMI, kg/m2 4 252/239 0.33 (-0.28 to 0.93) 0.29 2.45 0 0.49
Diabetes mellitus, pts 4 259/212 0.98 (0.59 to 1.60) 0.92 1.24 0 0.74
Hypertension, pts 3 156/110 0.76 (0.45 to 1.28) 0.30 1.36 0 0.51
Tumor in right side, pts 3 194/221 0.81 (0.55 to 1.20) 0.29 0.72 0 0.70
Tumor size, cm 3 123/145 -0.10 (-0.58 to 0.38) 0.68 6.78 71 0.03
Pre-sCr, mg/dL 3 115/97 -0.00 (-0.09 to 0.09) 1.00 1.20 0 0.55
Pre-eGFR, ml/minute 3 156/110 -0.75 (-7.01 to 5.51) 0.81 16.81 88 0.0002
Blum and colleagues subjectively estimated blood loss and thus the minimal changes on the field are difficult to calculate [9]. Moreover, the original data of EBL in their study was reported as median (range). We estimated the mean (SD) from median (range), thus, and the bias of a pooled effect should be taken into account. Considering these influencing factors, we conducted a sensitivity analysis of EBL, and the result showed that no significant differ-ence was detected between the two clamping groups. Blood transfusion rate is known to be closely related to blood loss. In line with the
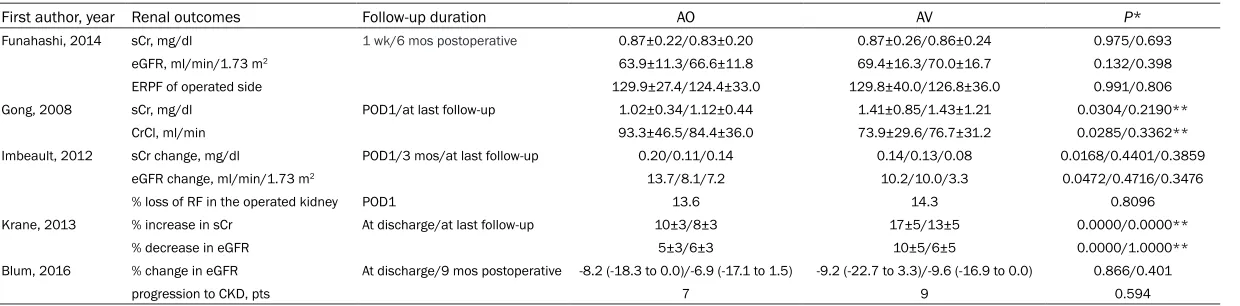
[image:5.612.90.522.71.508.2]Table 3. Renal function after PN between AO and AV clamping group with different follow-up durations
First author, year Renal outcomes Follow-up duration AO AV P*
Funahashi, 2014 sCr, mg/dl 1 wk/6 mos postoperative 0.87±0.22/0.83±0.20 0.87±0.26/0.86±0.24 0.975/0.693 eGFR, ml/min/1.73 m2 63.9±11.3/66.6±11.8 69.4±16.3/70.0±16.7 0.132/0.398
ERPF of operated side 129.9±27.4/124.4±33.0 129.8±40.0/126.8±36.0 0.991/0.806 Gong, 2008 sCr, mg/dl POD1/at last follow-up 1.02±0.34/1.12±0.44 1.41±0.85/1.43±1.21 0.0304/0.2190**
CrCl, ml/min 93.3±46.5/84.4±36.0 73.9±29.6/76.7±31.2 0.0285/0.3362** Imbeault, 2012 sCr change, mg/dl POD1/3 mos/at last follow-up 0.20/0.11/0.14 0.14/0.13/0.08 0.0168/0.4401/0.3859
eGFR change, ml/min/1.73 m2 13.7/8.1/7.2 10.2/10.0/3.3 0.0472/0.4716/0.3476
% loss of RF in the operated kidney POD1 13.6 14.3 0.8096 Krane, 2013 % increase in sCr At discharge/at last follow-up 10±3/8±3 17±5/13±5 0.0000/0.0000**
% decrease in eGFR 5±3/6±3 10±5/6±5 0.0000/1.0000** Blum, 2016 % change in eGFR At discharge/9 mos postoperative -8.2 (-18.3 to 0.0)/-6.9 (-17.1 to 1.5) -9.2 (-22.7 to 3.3)/-9.6 (-16.9 to 0.0) 0.866/0.401
progression to CKD, pts 7 9 0.594
extracted at length. Unfortunately, the collect-ed data could not be uscollect-ed for meta-analysis due to different follow-up durations and differ-ent measuring variables. Although limited by this, a summary table (Table 3) describes anal-ysis of renal function after PN, by comparing the two clamping techniques. Gong et al. [7] compared postoperative sCr and creatinine clearance (CrCl) with preoperative values in AO and AV clamping separately, and significant dif-ferences were detected in AV group. However, these cross-references could not confirm that AV clamping impairs renal function, considering the detection bias, other factors that affect renal function, and no direct comparison with AO clamping. Thus, we compared the postop-erative sCr and CrCl values, separately, using the original data, and the results showed that significant differences were detected in renal function on postoperative day one (POD1) be- tween the two clamping techniques. Imbeault et al. [4] assessed postoperative renal function by sCr and eGFR change in different follow-up durations, and the only significant difference was also detected on POD1. Krane et al. [10] detected significant differences in sCr and eGFR change between AO and AV clamping, and AV clamping showed compromise in renal function when the patients were discharged.
While in longer follow-up durations, most stud-ies detected no statistical differences of renal function between the AO and AV groups, mea-sured by sCr or eGFR. These phenomena sug-gest that renal function varies from different durations after surgery. However, we could not distinguish which clamping technique was ben-eficial for renal function preservation, based on currently available evidence. Animal experi-ments show that AO clamping can ensure bet-ter renal function by retrograde perfusion of the kidney through the renal vein [5, 16]. But this benefit was supposed to be negated by pneu-moperitoneum, which caused partial occlusion of the renal vein in endoscopic surgery [17]. With regard to AV clamping, Imbeault et al. [4] reported that AV clamping improved visualiza-tion during tumorectomy and reduced WIT. In addition, AV clamping could create a relatively bloodless field, which minimized the removing amount of normal renal parenchyma, an impor-tant factor known to be closely related to post-operative renal function [18]. Given the incon-sistent standpoints of the impacts of the two clamping techniques on renal function, further studies are urgently needed.
[image:7.612.93.521.71.328.2]tion after PN [19, 20]. We had initially extracted the data of WIT of included studies, but it was not suitable for merge analysis and for drawing a definitive conclusion, due to a limited number of studies and the values comparing the two clamping techniques not being evenly matched. Therefore, further studies are needed to draw a rigorous conclusion.
As reported in many literature [21-26], urinary leaks, intraoperative complications, open con-versions, positive surgical margins, and length of hospital stay are all important variables to assess safety and efficacy of PN. The original studies or our meta-analysis results found no significant differences between AO and AV clamping groups, which indicate that AV clamp-ing is comparable with AO clampclamp-ing for these primary and secondary outcomes. While, limit-ed by the number of studies and available data, only individual studies reported the variables above, and sufficient evidence remains to be found.
Certain limitations of this study should be no- ted. First, in spite of widely searching for poten-tial literature from four databases, only five studies were included for this meta-analysis. None of the included studies were randomized controlled trials and only two of them used a prospective cohort for group allocation. Alth- ough one study [10] reported a prospective co- hort, it was based on the surgeon’s preference for patient grouping, and the selection biases from this must be noted. Second, with regard to baseline variables, the clinical stages and R.E.N.A.L. nephrometry score of renal masses are considered critical concerns of PN. But these data were not available in our included studies. Although the meta-analysis of tumor size and the rate of the presence of tumors in the unilateral side showed no significant differ-ences. The location and growth pattern of renal masses could not be compared due to insuffi-cient original data, which might be of significant heterogeneity between the AO and AV group, and the impact on primary and (or) secondary outcomes due to that remains unknown. Third, the follow-up durations varied among the in- cluded studies, thus, we could not conduct a meta-analysis of renal function based on post-operative eGFR or sCr change. Fourth, consid-ering that the operations were performed by different surgeons and the experience of
sur-geons was not identical, performance biases from this could not be ruled out.
In spite of these limitations, we think the pres-ent study is still significant to give a compre-hensive comparison of AO and AV clamping te- chniques during PN. Considering the advantag-es of AV clamping, it is associated with shorter operative time and optimal visualization for tu- mor excision, and these advantages may facili-tate the hilar or complex tumorectomy [27, 28]. While, for other primary and secondary out-comes, our study showed that AV clamping was comparable with the AO clamping technique. However, these results should be applied care-fully due to the limited available evidence. In conclusion, the present meta-analysis shows that the AV clamping technique in PN is associ-ated with a shorter operative time, equal esti-mated blood loss, blood transfusion rate, urine leakage rate, postoperative complication rate, and positive margin rate when compared with AO clamping. In terms of renal function, a des- criptive analysis showed that AV clamping can give comparable results. Considering the inher-ent limitations of included studies, the result should be applied based on careful patient se- lection. To draw sufficient evidence-based con-clusions, well-designed randomized clinical tri-als are needed.
Acknowledgements
This study was funded by National Natural Sci- ence Foundation of China (Grant No. 8137- 2733/H1619).
Disclosure of conflict of interest
None.
Address correspondence to: Dr. Zhiping Wang, Ins- titute of Urology, Lanzhou University Second Hos- pital, No. 82 Cuiyingmen, Lanzhou 730030, Gansu Province, P.R. China. Tel: (86) 0931-8943714; E-mail: [email protected]
References
http://uroweb.org/guideline/renal-cell-carci-noma/#2.
[2] Kim SP, Murad MH, Thompson RH, Boorjian SA, Weight CJ, Han LC, Erwin PJ, Costello BA, Chow GK and Leibovich BC. Comparative ef-fectiveness for survival and renal function of partial and radical nephrectomy for localized renal tumors: a systematic review and meta-analysis. J Urol 2012; 188: 51-57.
[3] Azhar RA, Metcalfe C and Gill IS. Anatomic par-tial nephrectomy: technique evolution. Curr Opin Urol 2015; 25: 95-99.
[4] Imbeault A, Pouliot F, Finley DS, Shuch B and Dujardin T. Prospective study comparing two techniques of renal clamping in laparoscopic partial nephrectomy: impact on perioperative parameters. J Endourol 2012; 26: 509-514. [5] Neely WA and Turner MD. The effect of arterial,
venous, and arteriovenous occlusion on renal blood flow. Surg Gynecol Obstet 1959; 108: 669-672.
[6] Colli JL, Wang Z, Johnsen N, Grossman L and Lee BR. Clamping renal artery alone produces less ischemic damage compared to clamping renal artery and vein together in two animal models: near-infrared tissue oximetry and quantitation of 8-isoprostane levels. Int Urol Nephrol 2013; 45: 421-428.
[7] Gong EM, Zorn KC, Orvieto MA, Lucioni A, Mse-zane LP and Shalhav AL. Artery-only occlusion may provide superior renal preservation during laparoscopic partial nephrectomy. Urology 2008; 72: 843-846.
[8] Funahashi Y, Kato M, Yoshino Y, Fujita T, Sassa N and Gotoh M. Comparison of renal ischemic damage during laparoscopic partial nephrec-tomy with arteryevein and arteryeonly clamp-ing. J Urol 2014; 191: e437.
[9] Blum KA, Paulucci DJ, Abaza R, Eun DD, Bhan-dari A, Delto JC, Krane LS, Hemal AK and Badani KK. Main renal artery clamping with or without renal vein clamping during robotic par-tial nephrectomy for clinical T1 renal masses: perioperative and long-term functional out-comes. Urology 2016; 97: 118-123.
[10] Krane LS, Mufarrij PW, Manny TB and Hemal AK. Comparison of clamping technique in ro-botic partial nephrectomy: does unclamped partial nephrectomy improve perioperative outcomes and renal function? Can J Urol 2013; 20: 6662-6667.
[11] Stroup DF, Berlin JA, Morton SC, Olkin I, Wil-liamson GD, Rennie D, Moher D, Becker BJ, Sipe TA and Thacker SB. Meta-analysis of ob-servational studies in epidemiology: a propos-al for reporting. Meta-anpropos-alysis of observationpropos-al studies in epidemiology (MOOSE) group. JAMA 2000; 283: 2008-2012.
[12] Wells G, Shea B, O’Connell D and Peterson J. The Newcastle-Ottawa scale (NOS) for assess-ing the quality of nonrandomised studies in meta-analyses. Available from: URL: http:// www.ohri.ca/programs/clinical_epidemiology/ oxford.asp.
[13] Hozo SP, Djulbegovic B and Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol 2005; 5: 13.
[14] Haber GP and Gill IS. Laparoscopic partial ne-phrectomy: contemporary technique and out-comes. Eur Urol 2006; 49: 660-665.
[15] Hung AJ, Cai J, Simmons MN and Gill IS. “Tri-fecta” in partial nephrectomy. J Urol 2013; 189: 36-42.
[16] Birkeland S, Vogt A, Krog J and Semb C. Renal circulatory occlusion and local cooling. J Appl Physiol 1959; 14: 227-232.
[17] Orvieto MA, Zorn KC, Mendiola F, Lyon MB, Mikhail AA, Gofrit ON and Shalhav AL. Recov-ery of renal function after complete renal hilar versus artery alone clamping during open and laparoscopic surgery. J Urol 2007; 177: 2371-2374.
[18] Rod X, Peyronnet B, Seisen T, Pradere B, Go-mez FD, Verhoest G, Vaessen C, De La Taille A, Bensalah K and Roupret M. Impact of isch-aemia time on renal function after partial ne-phrectomy: a systematic review. BJU Int 2016; 118: 692-705.
[19] Thompson RH, Lane BR, Lohse CM, Leibovich BC, Fergany A, Frank I, Gill IS, Blute ML and Campbell SC. Renal function after partial ne-phrectomy: effect of warm ischemia relative to quantity and quality of preserved kidney. Urol-ogy 2012; 79: 356-360.
[20] Becker F, Van Poppel H, Hakenberg OW, Stief C, Gill I, Guazzoni G, Montorsi F, Russo P and Stockle M. Assessing the impact of ischaemia time during partial nephrectomy. Eur Urol 2009; 56: 625-634.
[21] Choi JE, You JH, Kim DK, Rha KH and Lee SH. Comparison of perioperative outcomes be-tween robotic and laparoscopic partial ne-phrectomy: a systematic review and meta-analysis. Eur Urol 2015; 67: 891-901.
[22] Aboumarzouk OM, Stein RJ, Eyraud R, Haber GP, Chlosta PL, Somani BK and Kaouk JH. Ro-botic versus laparoscopic partial nephrectomy: a systematic review and meta-analysis. Eur Urol 2012; 62: 1023-1033.
[24] Liu W, Li Y, Chen M, Gu L, Tong S, Lei Y and Qi L. Off-clamp versus complete hilar control par-tial nephrectomy for renal cell carcinoma: a systematic review and meta-analysis. J Endou-rol 2014; 28: 567-576.
[25] Trehan A. Comparison of off-clamp partial ne-phrectomy and on-clamp partial nene-phrectomy: a systematic review and meta-analysis. Urol Int 2014; 93: 125-134.
[26] Zhou L, Wei X, Sun WJ, Liu Q, Jian ZY, Li H and Wang KJ. Selective versus hilar clamping dur-ing minimally invasive partial nephrectomy: a systematic review and meta-analysis. J Endou-rol 2015; 29: 855-863.
[27] Reisiger K, Venkatesh R, Figenshau RS, Bae KT and Landman J. Complex laparoscopic par-tial nephrectomy for renal hilar tumors. Urology 2005; 65: 888-891.