Addressing Prenatal Breastfeeding Self-efficacy and Advancing the Baby Friendly Hospital Initiative
with HUG Your Baby Curriculum
By Molly Rippe
Senior Honors Thesis School of Nursing
University of North Carolina at Chapel Hill
March 22, 2019
Approved by:
Foreword
My past experience as an educator and my work as a doula inspired me to complete an honors project. One of my favorite aspects of being a doula are the prenatal appointments with clients. My first degree is in education, and yet it wasn’t until sitting in homes with families, teaching about childbirth, that I felt like the teacher in me came alive.
I was introduced to the HUG Your Baby (HYB) curriculum during my maternal-newborn nursing course in the fall. Its content and videos spoke to me because of its ease of explanation about newborn behavior and cues. I had the chance to sit down with HYB’s creator, Jan Tedder and discuss HYB’s applications and previous research with the curriculum. Jan’s enthusiasm was infectious, and I could see how important the content could be for new families wanting to know more about their newborn.
In order to do further research with HYB, I completed all of the HYB online courses for professionals, including becoming a HUG certified teacher. Furthermore, I began developing ideas for implementing its curriculum into prenatal childbirth education courses for expectant parents. Through a review of the literature, I found current recommendations in support of breastfeeding, and I knew that HYB could offer simple, straight forward education on this topic. Since NC Women’s Hospital is a Baby-Friendly designated hospital, I was curious about the extent to which breastfeeding was emphasized prenatally in its affiliated childbirth education courses.
began to consider the benefits of more focused breastfeeding education for clients giving birth at a Baby-Friendly hospital. Not only does the research demonstrate the correlation between prenatal breastfeeding education and increased rates of breastfeeding but adding this could ease the load of teaching on the busy nursing staff during postpartum recovery. I found myself wishing that these clients had the HYB DVD in their rooms to watch, and to take home with them. However, I knew that I wanted to start by introducing HYB prenatally.
Once the ideas for my research solidified, I began by applying for a scholarship to fund my research and received the Gump Family Undergraduate Research Award. I met with Jamie Conklin in the Health and Sciences Library who guided me in my literature search. I researched several breastfeeding self-efficacy scales, and contacted the creator of the one that most aligned with what I wanted to test. The author, Kristen Wells, granted me permission and sent me files of the assessment scale in its entirety. In addition to the ongoing support I received from my
advisor, I consulted with professor Maureen Baker in the School of Nursing about my research design and survey development.
In reaching out to the Women’s Health Information Center at UNC Medical Center, I gained support from the director to develop a HYB breastfeeding component that could be added to the standard childbirth preparation class. I observed instructor Chelsea Robinson’s (LCCE) 12-hour childbirth preparation training course and began talking with her about my idea for a pilot study. I also observed Jan Tedder teach a training course using HYB for childbirth
I ran the pilot study over the course of a few weeks, so that data was collected with both an intervention and control group. With each group, I introduced myself, the study, and the voluntary pre-and-post survey. For the intervention group, I taught the breastfeeding portion of the course as a HYB certified teacher. After teaching and collecting the data, I organized the results and inputted all data into excel spreadsheets. Through consultation with Chris Wiesen of the Odum Institute, I was able to implement statistical analysis of the Prenatal Breastfeeding Self-Efficacy Scale (PBSES) data. Additionally, I analyzed the intention scale and other demographic data, organizing them into tables for ease of interpretation. Lastly, I wrote the following manuscript as a draft of the pilot study for submission to the Journal of Perinatal Education, or another similar peer-reviewed journal.
Abstract
Experts recommend exclusive breastfeeding for at least the first six months of life. The World Health Organization’s (WHO) Baby-Friendly designation has significantly impacted rates of breastfeeding initiation in hospitals across the United States. However, exclusive breastfeeding rates at six months are still far below the WHO’s recommendations. Additional interventions to increase breastfeeding success are needed. A non-randomized, blinded experimental pilot study was designed to test whether participants in a standard childbirth preparation course offered at a Baby Friendly hospital differed in breastfeeding intention and self-efficacy from participants who took the same course with an added breastfeeding component from the prenatal education program called HUG Your Baby (HYB) (n=15). Breastfeeding intention and prenatal
breastfeeding self-efficacy scales were used and analyzed using a pre-and-post-test design. Results included an increased level of breastfeeding intention and self-efficacy in the
intervention group when compared to the control group. Implementing HYB curriculum may further support the Baby-Friendly Hospital Initiative and increase rates of successful
breastfeeding.
Addressing Prenatal Breastfeeding Self-efficacy and Advancing the Baby-Friendly Hospital Initiative
with HUG Your Baby Curriculum Breastfeeding Recommendations
Research describes the extensive benefits of breastfeeding to both mom and baby throughout the lifespan. The World Health Organization (WHO), United Nations International Children’s Emergency Fund (UNICEF), and American Academy of Pediatrics (AAP) all recommend and recognize the importance of exclusive breastfeeding (EBF) for at least the first six months of life (Levy & Ashley, 2018). Exclusive breastfeeding means feeding a newborn only breastmilk, and no other food or water (World Health Organization, 2018b). WHO and UNICEF created the Baby-Friendly Hospital Initiative (BFHI) to enhance breastfeeding rates around the world through supportive environments and educational services (Munn, Newman, Mueller, Phillips, & Taylor, 2016). Research shows that incorporating the Ten Steps to
Successful Breastfeeding of the BFHI has the biggest impact on increasing rates of EBF at six months after birth (Kim, Park, Oh, Kim, & Ahn, 2018). The WHO nutrition target for 2025 is to increase EBF rates in the first six months of life to 50% (World Health Organization, 2014).
The BFHI is one way in which hospitals can engage in measures to increase the nation’s rates of breastfeeding and EBF.
Baby-Friendly Hospital Initiative
The US has embraced the BFHI ethos through individual hospital designation that requires rigorous planning and implementation of structural changes. To become designated, facilities providing maternity and newborn services must initiate the Ten Steps to Successful Breastfeeding, which include policies and procedures outlining how to best support breastfeeding (World Health Organization, 2018c.) North Carolina Women’s Hospital earned the designation of Baby-Friendly in 2012 and is currently the only hospital in the triangle region with this designation. The third step in the Ten Steps to Successful Breastfeeding requires that hospitals “inform all pregnant women about the benefits and management of breastfeeding” (Baby-Friendly, 2018). Through this step, there is continual need for improvement of prenatal
breastfeeding education. Evidence demonstrates that increased education and support during the prenatal and postpartum periods is associated with increased rates of successful and exclusive breastfeeding (World Health Organization, 1998).
Interventions to Increase Breastfeeding
A review of the literature generated many studies that examine various interventions that increase rates of breastfeeding. A recent systematic review and meta-analysis of randomized controlled trials (RCTs) aimed to understand the best intervention strategies to support the WHO’s recommendations for EBF (Kim, Park, Oh, Kim, &Ahn, 2018). This study encompassed 36,051 mothers and 27 RCTs. It includes three main conclusions 1. That BFHI is the best way to support EBF; 2. there is a critical need for additional prenatal and postpartum long-term
would enhance the effectiveness of interventions (Kim, Park, Oh, Kim, &Ahn, 2018). Other findings in this meta-analysis associated interventions with the greatest impact on EBF at six months were those that liaised between the community and hospital, began prenatally and lasted after birth, used educational strategies that aimed to boost mother’s confidence and intention to breastfeed, and included breastfeeding support within the first week postpartum (Kim, Park, Oh, Kim, &Ahn, 2018). Additionally, studies showed that if the mother lacked confidence, self-efficacy, and support from partner and family, felt embarrassed or that breastfeeding was culturally unacceptable there was a reduced likelihood of breastfeeding initiation and continuation (Levy & Ashley, 2018).
Evidence suggests that higher levels of self-efficacy in women may increase the time that they exclusively breastfeed (Chan, Ip, & Choi, 2016). This research is grounded in the theoretical framework of social cognitive theory by Albert Bandura (Bandura, 1986). Social cognitive theory explains human functioning in terms of behavior, personal factors, and environmental events (Wells, Thompson, & Kloeblen-Tarver, 2006). This framework is a useful application to study breastfeeding as a health behavior because success with breastfeeding is determined by all three of these factors. Self-efficacy is part of the social cognitive theory and has been used to examine many health behaviors (Wells, Thompson, & Kloeblen-Tarver, 2006). Self-efficacy is the belief in oneself to attain something and promotes the idea that if one believes they are able to do something then one has a better chance of success in attaining it.
The WHO wrote in Evidence for the Ten Steps to Successful Breastfeeding (1998) that education during the prenatal period is most effective if it incorporates discussion of
breastfeeding myths and inhibitions, offers practical demonstration to increase skills and
type of support that facilitates the initiation of breastfeeding can be learned prenatally through confidence building and knowledge acquisition (Schreck et al., 2017). Additionally, attitudes towards the normalization and observation of breastfeeding have been shown to help increase rates of breastfeeding (Meedya, Fahy, Kable, 2010).
HUG Your Baby Curriculum
HUG Your Baby (HYB) is an acronym for “help, understanding, and guidance” for young families. It is a multicultural, evidence-based, inclusive, and Baby-Friendly educational curriculum (HUG Your Baby, 2019). The Roadmap to Breastfeeding Success program, a component of HYB, covers not only effective breastfeeding parent education, but also offers continuing education training for professionals through a certification course with HYB. This training program integrates child development theory to understand newborn behavior and cues, as well as evidence-based recommendations in lactation support, and information that supports the BFHI breastfeeding goals (Tedder, 2015).
Pilot Study Project
The purpose of this study is to determine whether teaching breastfeeding with the HYB curriculum during a prenatal childbirth class increases self-efficacy for, knowledge about, and intention to breastfeed. This pilot study measures intention and self-confidence in breastfeeding using a prenatal breastfeeding self-efficacy and intention to breastfeed scales.
Methods
Setting
Childbirth preparation classes affiliated with this project are taught at NC Women’s Hospital, a large academic teaching hospital with around 4,000 births annually situated in the southeastern United States. The childbirth education class is focused on normal physiological birth and is intended for expectant parents. Participants learn coping techniques for labor, typical interventions used in the NC Women’s Hospital setting, and knowledge about the process of labor and birth. Breastfeeding information is not considered a central part to the course. The fee for the course is $85 and it is open to the public, regardless of where one is giving birth.
Discounts are available to health center affiliated employees and students, as well as for
individuals covered by public insurance (UNC Medical Center, 2019). The training is 12-hours and takes place over the course of two sessions, typically over two weekend days. Each
instructor is a Lamaze Certified Childbirth Educator (LCCE) (UNC Medical Center, 2019).
Design
breastfeeding curriculum as a component of the childbirth course (intervention). All 16
participants voluntarily enrolled in the study, completing a survey before the course and after the 12-hour childbirth preparation course was complete. Participants had the same childbirth
instructor and format and were blind to whether or not they received the intervention on
breastfeeding teaching. All participants who completed the 12-hour class were including in this pilot study. One participant was lost from the intervention group due to not completing the childbirth preparation course.
The pre-and post-survey included a valid and reliable prenatal breastfeeding self-efficacy scale (PBSES) as well as a scale of intention to breastfeed. The PBSES is a 20-item, five-point Likert-type scale. Permission was obtained from the author of the PBSES to use the tool before implementation. Its self-efficacy measurement is comprised of four themes: “(1) confidence regarding the skills and demands required for breastfeeding or extracting breastmilk using a breast pump; (2) confidence regarding gathering information about how to breast-feed; (3) confidence regarding breast-feeding around other people and feelings of embarrassment during breastfeeding; (4) confidence regarding social pressure when breast-feeding” (Wells, Thompson, & Kloeblen-Tarver, 2006, p. 185). The intention scale came from the HUG certified teacher training modules. This scale represented numbers one through ten, where one represents ‘I do NOT want to breastfeed’, and ten represents ‘I WILL breastfeed no matter what.’ In addition to the numerical scale, participants were given a chance to write down why they chose this number on the intention scale.
Appropriate Collaborative Institutional Training Initiative (CITI) modules were
Intervention
Pregnant women in the intervention group completed the pre-survey (Appendix A) at the beginning of class and the post-survey (Appendix B) after the breastfeeding curriculum was complete. This curriculum was developed and taught by a HUG certified teacher and was based on introducing the concept of BFHI and the Roadmap to Breastfeeding Success program. As an introduction to the subject, the instructor asked for participation from the group, asking if anyone was planning on giving birth at NC Women’s Hospital because of its Baby-Friendly status. When none of the participants were familiar with BFHI, the instructor introduced the concept. The description included the significance of the designation and how BFHI designated facilities support women and families in breastfeeding.
Further participation was elicited when the instructor asked for stories participants have heard about breastfeeding. From this discussion, the class covered common breastfeeding concerns and myths including 1. pain, proper latch, seeking help at the moment of a question rather than waiting; 2. lack of milk supply and the research surrounding the rare occurrence of this, as well as the size of a newborn’s stomach using visual props, skin-to-skin and initiating breastfeeding in the first hour of life; 3. Returning to work, less missed days of work because of baby’s strong immune system, and overall health benefits of breastfeeding for mom and baby.
breast-prop. At the conclusion of the breastfeeding educational intervention, the instructor asked participants to consider if there are people in their lives who would be helpful to them during their breastfeeding experience. The class was also asked to think of others in their lives who would not be supportive of their breastfeeding. The UNC lactation service number was displayed on the screen for everyone to note. The instructor encouraged all participants to consider
someone they can call, including a lactation consultant, when they need breastfeeding support after their birth.
Following the completion of post-intervention surveys, expectant parents received gifts for participating: a HUG DVD, a printout of the Roadmap to Breastfeeding Success (see Figure 1), a HYB pamphlet called Understanding and Caring for your Newborn (see Figure 2), and a newborn sleep sack to promote safe infant sleeping.
Demographics and Data Collection
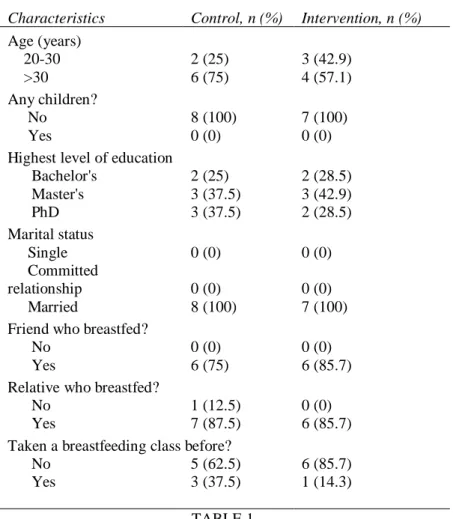
Demographic data was voluntarily collected from the participants of this study (Table 1). None of the participants had given birth previously. The women’s ages ranged from 24-38 years old, and all were married and had partners present during the class. All participants had earned at least a bachelor’s degree, with the highest level of education at a PhD level. The majority had never taken a breastfeeding course previous to this childbirth training. Participants were also asked if they had relatives or friends that breastfed.
preemptively, increases likelihood for one to continue breastfeeding (World Health Organization, 1998). At the conclusion of the survey, participants were given the option to opt-out of receiving HYB postpartum e-newsletters from the time of their estimated due date. There was a short paragraph included about the creator of HYB, and the general contents that the e-newsletter would provide.
TABLE 1. DEMOGRAPHICS OF THE SAMPLE
Characteristics Control, n (%) Intervention, n (%) Age (years)
20-30 2 (25) 3 (42.9)
>30 6 (75) 4 (57.1)
Any children?
No 8 (100) 7 (100)
Yes 0 (0) 0 (0)
Highest level of education
Bachelor's 2 (25) 2 (28.5) Master's 3 (37.5) 3 (42.9)
PhD 3 (37.5) 2 (28.5)
Marital status
Single 0 (0) 0 (0)
Committed
relationship 0 (0) 0 (0)
Married 8 (100) 7 (100)
Friend who breastfed?
No 0 (0) 0 (0)
Yes 6 (75) 6 (85.7)
Relative who breastfed?
No 1 (12.5) 0 (0)
Yes 7 (87.5) 6 (85.7)
Taken a breastfeeding class before?
No 5 (62.5) 6 (85.7)
Yes 3 (37.5) 1 (14.3)
TABLE 1. Statistical Analysis
individually and combined. Results are labeled as follows: skills and demands, gathering information, breastfeeding around others, social pressure, and total self-efficacy measured (see Tables 4-8). Numerical data from the intention to breastfeed scale and descriptive data from the explanation of chosen number were also compared in pre-and-post surveys as well.
Results
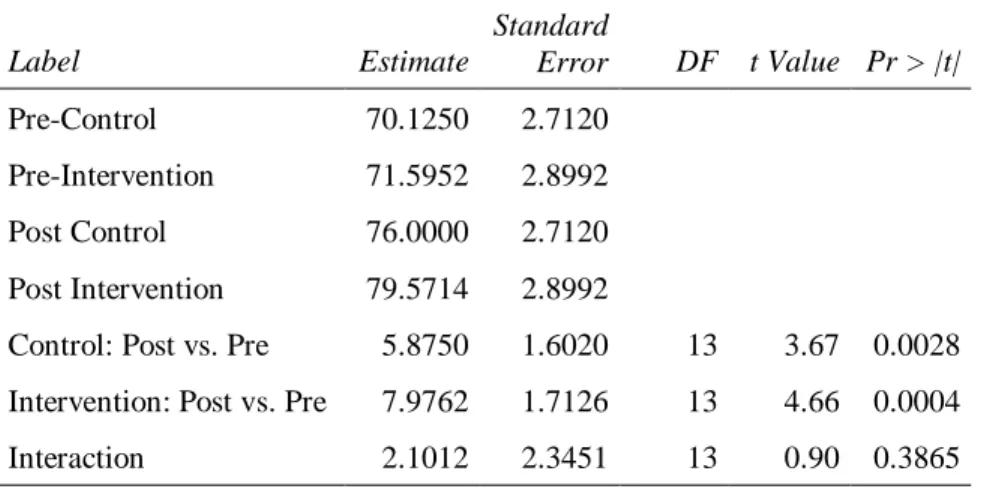
Analysis revealed a change in participants’ self-efficacy in both the control and intervention post-surveys. The two largest differences between the control and intervention groups for the factors of self-efficacy were in the skills and demands section, and the gathering information section. Furthermore, when you compare the total self-efficacy measurement between the control and intervention groups, the intervention groups had higher rates of total self-efficacy.
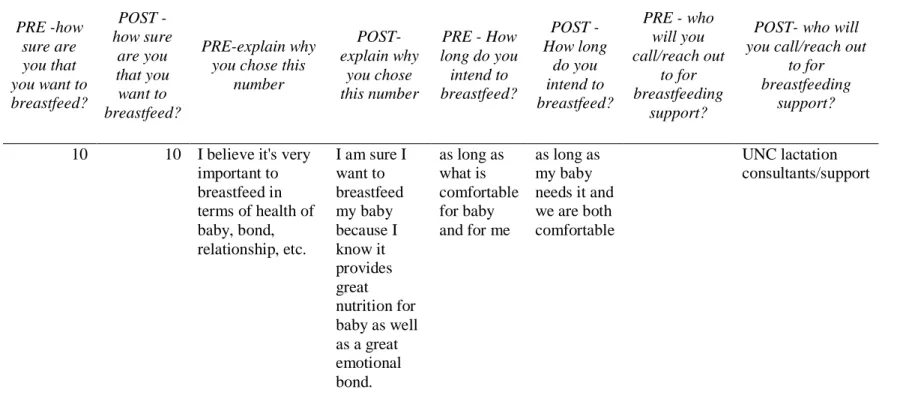
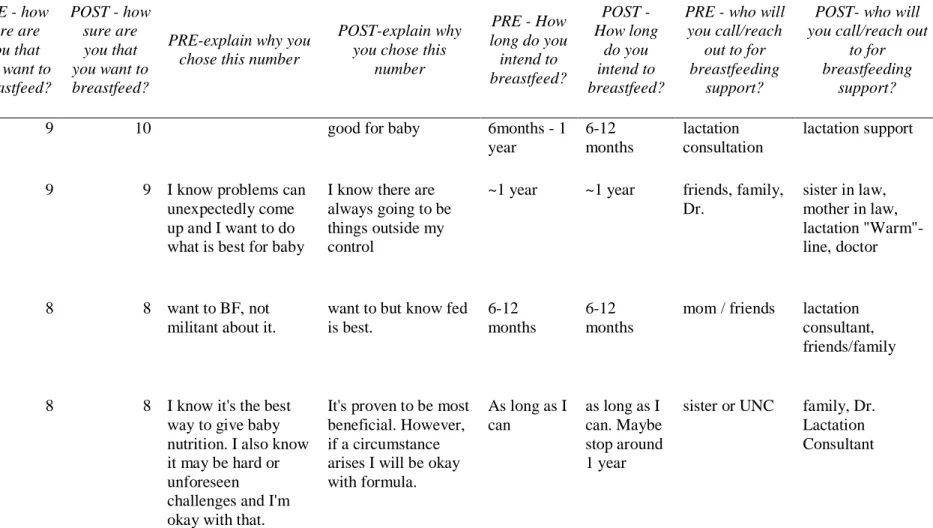
Both the intervention and control groups scored high on intentions to breastfeed. There was not a significant difference in the data before and after the childbirth course as to ‘how sure’ participants were that they would breastfeed. For example, in the control group participants’ answers ranged from seven to ten on the pre-survey intention scale, and eight to ten on the post-survey, where 63% of the answers had no change from the pre-survey to the post-survey. In the intervention group, answers ranged from eight to ten in both the pre-and-post surveys,
accounting for 71% of the participants that had no change in their intention to breastfeed scale. Details of the qualitative data collected on intention to breastfeed scale are reported in Tables 2 and 3.
TABLE 2. CONTROL GROUP DATA COLLECTION
PRE - how sure are you that you want to breastfeed? POST - how sure are you that you want to breastfeed? PRE-explain why you chose
this number
POST-explain why you chose this number
PRE - How long do you intend to breastfeed? POST - How long do you intend to breastfeed?
PRE - who will you call/reach out to for breastfeeding support? POST- who will you call/reach out to for breastfeeding support?
9 10 healthy for baby, bonding. Unless issues, I will breastfeed health benefits, bonding 6-12 months 6-12 months books, parents, friends, pediatrician, nurses probably at some point
10 9 want to try my
best to breastfeed
1 year 1 year counselor lactation consultant
9 9 I feel confident I
can make it
I don’t know
I don't know at the moment
my mother, my sister
maybe
7 9 plans are to breastfeed as long as baby responds well and grows properly
TABLE 2. (CONTINUED)
PRE -how sure are you that you want to breastfeed? POST - how sure are you that you want to breastfeed? PRE-explain why you chose this number POST-explain why you chose this number
PRE - How long do you intend to breastfeed? POST - How long do you intend to breastfeed?
PRE - who will you call/reach
out to for breastfeeding
support?
POST- who will you call/reach out
to for breastfeeding
support?
9 9 I will try my best to breastfeed but I understand there may be limitations and will not put myself or baby under unnecessary stress
I plan to breastfeed and will exhaust all support options available to me to achieve this goal. But I understand there may be
situations where supplementation is needed.
1 year 1 year lactation consultants/ support groups lactation consultant, support groups, friends, family
8 8 Won't
sacrifice my sanity in the long term if my body just is not doing it
I will go to pretty great lengths to breastfeed but if my body just proves not capable, etc. then I'm okay with formula feeding 6 months- 1year 6 months- 1year
LC lactation
consultant, online groups
9 9 knowledge that it is better for baby if possible
it is beneficial to my baby's health
TABLE 2. (CONTINUED)
PRE -how sure are you that you want to breastfeed? POST - how sure are you that you want to breastfeed? PRE-explain why you chose this
number
POST-explain why
you chose this number
PRE - How long do you intend to breastfeed? POST - How long do you intend to breastfeed?
PRE - who will you call/reach out
to for breastfeeding
support?
POST- who will you call/reach out
to for breastfeeding
support?
10 10 I believe it's very important to breastfeed in terms of health of baby, bond, relationship, etc.
I am sure I want to breastfeed my baby because I know it provides great nutrition for baby as well as a great emotional bond.
as long as what is comfortable for baby and for me
as long as my baby needs it and we are both comfortable
UNC lactation consultants/support
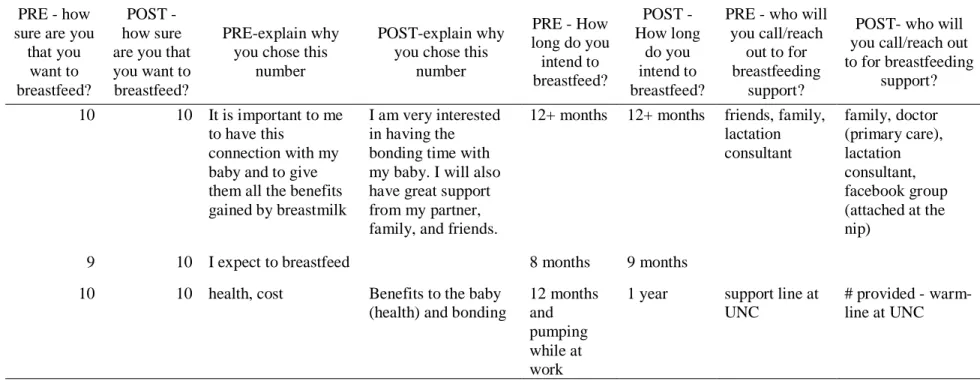
TABLE 3. INTERVENTION GROUP DATA COLLECTION
PRE - how sure are you that you want to breastfeed?
POST - how sure are you that you want to breastfeed?
PRE-explain why you chose this number
POST-explain why you chose this
number
PRE - How long do you intend to breastfeed? POST - How long do you intend to breastfeed?
PRE - who will you call/reach
out to for breastfeeding
support?
POST- who will you call/reach out
to for breastfeeding
support?
9 10 good for baby 6months - 1
year 6-12 months lactation consultation lactation support
9 9 I know problems can unexpectedly come up and I want to do what is best for baby
I know there are always going to be things outside my control
~1 year ~1 year friends, family, Dr.
sister in law, mother in law, lactation "Warm"-line, doctor
8 8 want to BF, not militant about it.
want to but know fed is best.
6-12 months
6-12 months
mom / friends lactation consultant, friends/family
8 8 I know it's the best way to give baby nutrition. I also know it may be hard or unforeseen
challenges and I'm okay with that.
It's proven to be most beneficial. However, if a circumstance arises I will be okay with formula.
As long as I can
as long as I can. Maybe stop around 1 year
TABLE 3. (CONTINUED)
PRE - how sure are you
that you want to breastfeed?
POST - how sure are you that you want to breastfeed?
PRE-explain why you chose this
number
POST-explain why you chose this
number
PRE - How long do you intend to breastfeed? POST - How long do you intend to breastfeed?
PRE - who will you call/reach
out to for breastfeeding
support?
POST- who will you call/reach out to for breastfeeding
support?
10 10 It is important to me to have this
connection with my baby and to give them all the benefits gained by breastmilk
I am very interested in having the bonding time with my baby. I will also have great support from my partner, family, and friends.
12+ months 12+ months friends, family, lactation consultant family, doctor (primary care), lactation consultant, facebook group (attached at the nip)
9 10 I expect to breastfeed 8 months 9 months
10 10 health, cost Benefits to the baby (health) and bonding
12 months and pumping while at work
1 year support line at UNC
# provided - warm-line at UNC
TABLE 4. SKILLS AND DEMANDS
Label Estimate
Standard
Error DF t Value Pr > |t|
Pre-Control 23.5000 1.5708
Pre-Intervention 25.8095 1.6793
Post Control 26.5000 1.5708
Post Intervention 29.5714 1.6793
Control: Post vs. Pre 3.0000 1.1701 13 2.56 0.0236
Intervention: Post vs. Pre 3.7619 1.2509 13 3.01 0.0101
Interaction 0.7619 1.7128 13 0.44 0.6638
TABLE 4.
TABLE 5. GATHERING INFORMATION
Label Estimate
Standard
Error DF t Value Pr > |t|
Pre-Control 20.2500 0.8097
Pre-Intervention 20.2143 0.8656
Post Control 22.2500 0.8097
Post Intervention 23.2857 0.8656
Control: Post vs. Pre 2.0000 0.5390 13 3.71 0.0026
Intervention: Post vs. Pre 3.0714 0.5762 13 5.33 0.0001
Interaction 1.0714 0.7890 13 1.36 0.1976
TABLE 5.
TABLE 6. BREASTFEEDING AROUND OTHERS
Label Estimate
Standard
Error DF t Value Pr > |t|
Pre-Control 16.5000 0.8692
Pre-Intervention 16.7143 0.9292
Post Control 17.5000 0.8692
Post Intervention 17.4286 0.9292
Control: Post vs. Pre 1.0000 0.5999 13 1.67 0.1194
Intervention: Post vs. Pre 0.7143 0.6413 13 1.11 0.2856
Interaction -0.2857 0.8782 13 -0.33 0.7501
TABLE 6.
TABLE 7. SOCIAL PRESSURE
Label Estimate
Standard
Error DF t Value Pr > |t|
Pre-Control 9.8750 0.3712
Pre-Intervention 8.8571 0.3968
Post Control 9.7500 0.3712
Post Intervention 9.2857 0.3968
Control: Post vs. Pre -0.1250 0.2101 13 -0.60 0.5620
Intervention: Post vs. Pre 0.4286 0.2246 13 1.91 0.0787
Interaction 0.5536 0.3075 13 1.80 0.0951
TABLE 8. TOTAL SELF-EFFICACY MEASURED
Label Estimate
Standard
Error DF t Value Pr > |t|
Pre-Control 70.1250 2.7120
Pre-Intervention 71.5952 2.8992
Post Control 76.0000 2.7120
Post Intervention 79.5714 2.8992
Control: Post vs. Pre 5.8750 1.6020 13 3.67 0.0028
Intervention: Post vs. Pre 7.9762 1.7126 13 4.66 0.0004
Interaction 2.1012 2.3451 13 0.90 0.3865
Discussion
The PBSES and intention scales were utilized to examine whether teaching breastfeeding with the HYB curriculum during a prenatal childbirth class was associated with an increase in self-efficacy for, knowledge about, and intention to breastfeed. High rates of self-efficacy are related to initiation and continuation of exclusive breastfeeding (Meedya, Fahy, & Kable, 2010). PBSES results revealed a positive effect on the participants’ breastfeeding self-efficacy. Rates of self-efficacy were highest in self-confidence about skills and demands of breastfeeding, as well as the ability to find information and use resources to gain support for breastfeeding when needed. In a culture that is saturated with information, knowing where to find evidence-based, reliable information can be challenging. In this way, using the HYB curriculum prenatally gives expecting and new parents information they know they can trust and rely upon, as well as resources to turn to in moments of struggle after baby arrives. In addition, providing expectant parents with this information prenatally helps to create realistic expectations of what
breastfeeding may involve.
through the built-in newsletters that arrive for the first 12 months postpartum. These e-newsletters help to support breastfeeding and reinforces information that parents learned prenatally. Content includes information on normal newborn behavior and cues, which when paired with breastfeeding support, aids in new parents’ ability to understand and communicate with their newborn. Links to YouTube videos demonstrate proper latch, hand-expressing milk, as well as other common issues in breastfeeding (Hug Your Baby, 2019). Recent systematic review and meta-analyses show that the combination of prenatal education with postpartum support is the key to increasing exclusive breastfeeding rates in the U.S. (Kim, Park, Oh, Kim, & Ahn, 2018). It is through a multi-pronged approach both in the prenatal and postpartum periods that HYB curriculum provides various interventions to help parents succeed in breastfeeding.
This study demonstrates an increase in self-efficacy in new and soon-to-be parents, offers practical demonstrations through teaching and videos, and involves the mothers’ social
supporters. Because of its multi-pronged approach, the curriculum is a well-rounded, beneficial tool that should be used. HYB curriculum may increase exclusive breastfeeding rates and should be considered when a hospital is in the process of becoming Baby-Friendly. Additionally, the HYB content and resources has the potential to reach beyond prenatal courses or Baby-Friendly hospitals. Only a small portion of expectant parents attend childbirth education classes, and the HYB resources such as the DVD, roadmap to breastfeeding success, and e-newsletters lend itself easily to settings outside the classroom. The transferability of the HYB curriculum across
settings is an asset and should be used to its fullest potential.
also only included English-speaking participants enrolling in childbirth preparation classes. Since HYB is translated into several languages, future studies should include sharing the curriculum in languages other than English.
Another aspect of this project that would be better tested in larger and more diverse groups is the intention to breastfeed scale. All the women came into this course with very high levels of intention to breastfeed, even without high levels of knowledge about and self-efficacy for breastfeeding. The intention scale did not prove to be a helpful marker in this population but would still be an important assessment tool to keep in the study for other populations.
Future studies should consider follow up with participants during the postpartum period. Self-efficacy and intentions could be compared to actual breastfeeding experiences and rates. Such findings may provide greater understanding of the impact of the multi-modal interventional approach of the HYB curriculum as it relates to exclusivity of breastfeeding at various time-markers in the postpartum period. To better understand the relationship of HYB curriculum and breastfeeding rates, this study should be replicated with more prenatal childbirth courses,
including various hospitals around the country.
Conclusion
References
Alden, K.R. (2018). A web-based module to enhance BSN students’ knowledge and confidence in teaching parents about newborn behavior. Journal of Perinatal Education 27(2), 104-114. Doi: 10.1891/1058-1243.27.2.104
Baby-Friendly USA. (2018). Ten steps to successful breastfeeding. Retrieved from: https://www.babyfriendlyusa.org/for-facilities/practice-guidelines/10-steps-and-international-code/
Bandura, A. (1986). Social foundations of thought and action: A social cognitive theory. Englewood Cliffs, New Jersey: Prentice Hall.
Center for Disease Control and Prevention. (2018). Breastfeeding report card. Atlanta, GA: US Department of Health and Human Services. Retrieved from:
https://www.cdc.gov/breastfeeding/data/reportcard.htm
Chan, M.Y., Ip, W.Y., & Choi, K. C. (2016). The effect of a self-efficacy-based educational programme on maternal breast feeding self-efficacy, breast feeding duration and
exclusive breast feeding rates: A longitudinal study. Midwifery, 36(5), 92-98. Retrieved from https://doi.org/10.1016/j.midw.2016.03.003
Demirtas Hicyilmaz, B., & Acikgoz, I. (2017). The association between breastfeeding self-efficacy, breastfeeding attitude, social-professional support and breastfeeding control. Turkiye Klinikleri Hemsirelik Bilimleri, 9(2), 133–143. Retrieved from https://doi.org/10.5336/nurses.2016-53973
de Enfermagem Do Nordeste, 19(1), 1–7. Retrieved from https://doi.org/10.15253/2175-6783.2018193175
HUG Your Baby. (2019). HUG’s mission, vision & values/history & awards. Retrieved from http://hugyourbaby.org/hug-history/
Hunter, L. M. L., Blake, S., Simmons, C., Thompson, J., & Derouin, A. (2019). Implementing a parent education program in the special care nursery. Journal of Pediatric
Healthcare, 33(2), 131–137. Retrieved from https://doi.org/10.1016/j.pedhc.2018.06.007 Kim, S. K., Park, S., Oh, J., Kim, J., & Ahn, S. (2018). Interventions promoting exclusive
breastfeeding up to six months after birth: A systematic review and meta-analysis of randomized controlled trials. International Journal of Nursing Studies, 80, 94–105. Retrieved from https://doi.org/10.1016/j.ijnurstu.2018.01.004
Levy, G., & Ashley, T. J. (2018). Breastfeeding: Factors that affect initiation and duration of breastfeeding. CINAHL Nursing Guide. Retrieved from
http://web.b.ebscohost.com/ehost/pdfviewer/pdfviewer?vid=20&sid=6e650b21-865a-4168-bced-e40e774ac569%40pdc-v-sessmgr03
McKinley, E. M., Knol, L. L., Turner, L. W., Burnham, J. J., Graettinger, K. R., Hernandez-Reif, M., & Leeper, J. D. (2019). The prenatal rating of efficacy in preparation to breastfeed scale: A new measurement instrument for prenatal breastfeeding self-efficacy. Journal of Human Lactation, 35(1), 21–31. Retrieved from
https://doi.org/10.1177/0890334418799047
Munn, A. C., Newman, S. D., Mueller, M., Phillips, S. M., & Taylor, S. N. (2016). The impact in the united states of the baby-friendly hospital initiative on early infant health and
breastfeeding outcomes. Breastfeeding Medicine, 11(5), 222–230. Retrieved from https://doi.org/10.1089/bfm.2015.0135
Parry, K. C., Tully, K. P., Moss, S. L., & Sullivan, C. S. (2017). Innovative prenatal
breastfeeding education curriculum: Ready, set, baby. Journal of Nutrition Education & Behavior, 49(7), S214–S216. Retrieved from https://doi.org/10.1016/j.jneb.2017.05.348 Schreck, P. K., Solem, K., Wright, T., Schulte, C., Ronnisch, K. J., & Szpunar, S. (2017). Both
prenatal and postnatal interventions are needed to improve breastfeeding outcomes in a low-income population. Breastfeeding Medicine, 12(3), 142–148. Retreived from https://doi.org/10.1089/bfm.2016.0131
Skouteris, H., Bailey, C., Nagle, C., Hauck, Y., Bruce, L., & Morris, H. (2017). Interventions designed to promote exclusive breastfeeding in high-income countries: A systematic review update. Breastfeeding Medicine, 12(10), 604–614. Retrieved from
https://doi.org/10.1089/bfm.2017.0065
Tedder, J. L. (2008). Give the HUG: An innovative approach to helping parents understand the language of their newborn. Journal of Perinatal Education, 17(2), 14–20. doi:
10.1624/105812408X298345
Tedder, J. L. (2012). Teaching for birth and beyond: Online program incorporated into a birthing and parenting certification. International Journal of Childbirth Education, 27(3), 65–68. Retrieved from
Tedder, J. (2015). The roadmap to breastfeeding success: Teaching child development to extend breastfeeding duration. Journal of Perinatal Education, 24(4), 239–248. doi:
10.1891/1058-1243.24.4.239
Tedder, J.L., & Quintana, E.M. (2018). Online education for WIC professionals: Teaching child development to extent breastfeeding duration. Clinical Lactation, 9(3), 108-116. doi: 10.1891/2158-0782.9.3.108
UNC Medical Center, UNC Healthcare. (2019). Women’s health information center: prepared
childbirth. Retrieved from https://reg.abcsignup.com/reg/event_page.aspx?ek=0011-0011-d31a23b2d42e47a187c67371d9f83e6f
Wells KJ, Thompson NJ, & Kloeblen-Tarver AS. (2006). Development and psychometric testing of the prenatal breast-feeding self-efficacy scale. American Journal of Health
Behavior, 30(2), 177–187. Retrieved
from http://web.b.ebscohost.com/ehost/pdfviewer/pdfviewer?vid=37&sid=4407c473-8de6-4c4f-afcf-ae7d6f58b608%40pdc-v-sessmgr06
World Health Organization. (1998). Evidence for the ten steps to successful breastfeeding.
Geneva, Switzerland: Child Health and Development, Family and Reproductive Health. Retrieved from https://www.who.int/nutrition/publications/evidence_ten_step_eng.pdf World Health Organization. (2014). Global nutrition targets 2025: Breastfeeding policy brief.
Geneva, Switzerland: Department of Nutrition for Health and Development, World Health Organization. Retrieved from
World Health Organization. (2018a). Implementation guidance: Protecting, promoting, and supporting breastfeeding in facilities providing maternity ad newborn services –the
revised baby-friendly hospital initiative (License: CC BY-NC-SA 3.0 IGO). Geneva, Switzerland: WHO Document Production Service. Retrieved from:
http://apps.who.int/iris/bitstream/handle/10665/272943/9789241513807-eng.pdf
World Health Organization. (2018b). Nutrition: Breastfeeding. Geneva, Switzerland: Department of Nutrition for Health and Development. Retrieved from
https://www.who.int/nutrition/topics/exclusive_breastfeeding/en/
World Health Organization. (2018c). Nutrition: Ten steps to successful breastfeeding. Geneva, Switzerland: Department of Nutrition for Health and Development. Retrieved from https://www.who.int/nutrition/bfhi/ten-steps/en/
Appendix A
Breastfeeding Intervention Pre-Survey
Age: _____ Previous number of births: _______ Highest level of education: ____________
Estimated Due Date: _______________________
Email address: ______________________________________________
Marital Status? (please circle one) Single Committed Relationship Married
Have you taken a breastfeeding class before? No Yes
Do you have a friend and/or relative who successfully breastfed?
Friend: No Yes Relative: No Yes
How sure are you that you want to breastfeed? (please circle a number below)
Do NOT want to breastfeed WILL breastfeed no matter what
1 2 3 4 5 6 7 8 9 10
Explain why you chose this number:
If you do plan on breastfeeding:
Who will you call/reach out to for breastfeeding support? ___________________ How long do you intend to breastfeed? _______________________
Please answer 1-4 if you have already had a baby:
1. How did you feed your newborn 0-6months? (please circle one) Formula-fed Breastfed Combination of both
2. If you breastfed, how long did you breastfeed? (please circle one)
1-2 weeks 1-3months 3-6months 6-9months 9-12months
12-15months 15-18months 18-21months 21-24months 24+months
3. How old was your baby when you gave them food for the first time?
For each of the following items, I want you to tell me how sure you are that you could do each of the things described:
Not at all sure
Slightly sure
Fairly sure
Very sure
Completely sure 1. I can find the information I need about
problems I have breastfeeding my baby. NS SS FS VS CS 2. I can find out what I need to know
about breastfeeding my baby. NS SS FS VS CS
3. I know who to ask if I have any questions about breastfeeding my baby.
NS SS FS VS CS
4. I can talk to my partner about the importance of breastfeeding my baby.
NS SS FS VS CS
5. I can talk to my health care provider about
breastfeeding my baby. NS SS FS VS CS
6. I can schedule my day around the
breastfeeding of my baby. NS SS FS VS CS
7. I can make the time to breastfeed
my baby even when I feel busy. NS SS FS VS CS
8. I can breastfeed my baby even
when I am tired. NS SS FS VS CS
9. I can breastfeed my baby even
when I am upset. NS SS FS VS CS
10. I can use a breast pump
Not at all sure
Slightly sure
Fairly sure
Very sure
Completely sure 11.
I can prepare breastmilk so
others can breastfeed my baby. NS SS FS VS CS
12. I can breastfeed my baby even
if it causes mild discomfort. NS SS FS VS CS
13. I can breastfeed my baby
without feeling embarrassed. NS SS FS VS CS
14. I can breastfeed my baby when
my partner is with me. NS SS FS VS CS
15. I can breastfeed my baby when
my family or friends are with me. NS SS FS VS CS
16. I can breastfeed my baby
around people I do not know. NS SS FS VS CS
17. I can call a lactation counselor
if I have problems breastfeeding. NS SS FS VS CS
18. I can choose to breastfeed my baby even
if my partner does not want me to. NS SS FS VS CS
19. I can choose to breastfeed my baby even
if my family does not want me to. NS SS FS VS CS
20. I can breastfeed my baby for one year.
Appendix B
Breastfeeding Intervention Post-Survey
Email address: _______________________________
For each of the following items, I want you to tell me how sure you are that you could do each of the things described:
Not at all sure
Slightly sure
Fairly sure
Very sure
Completely sure 1.
I can prepare breastmilk so
others can breastfeed my baby. NS SS FS VS CS
2. I can breastfeed my baby even
if it causes mild discomfort. NS SS FS VS CS
3. I can breastfeed my baby
without feeling embarrassed. NS SS FS VS CS
4. I can breastfeed my baby when
my partner is with me. NS SS FS VS CS
5. I can breastfeed my baby when
my family or friends are with me. NS SS FS VS CS
6. I can breastfeed my baby
around people I do not know. NS SS FS VS CS
7. I can call a lactation counselor
if I have problems breastfeeding. NS SS FS VS CS
8. I can choose to breastfeed my baby even if my partner does not want
me to.
NS SS FS VS CS
9. I can choose to breastfeed my baby even
if my family does not want me to. NS SS FS VS CS
10 I can breastfeed my baby for one year.
Not at all sure
Slightly sure
Fairly sure
Very sure
Completely sure 11. I can find the information I need about
problems I have breastfeeding my baby. NS SS FS VS CS
12. I can find out what I need to know
about breastfeeding my baby. NS SS FS VS CS
13. I know who to ask if I have any questions about breastfeeding my baby.
NS SS FS VS CS
14. I can talk to my partner about the importance of breastfeeding my baby.
NS SS FS VS CS
15. I can talk to my health care provider about
breastfeeding my baby. NS SS FS VS CS
16. I can schedule my day around the
breastfeeding of my baby. NS SS FS VS CS
17. I can make the time to breastfeed
my baby even when I feel busy. NS SS FS VS CS
18. I can breastfeed my baby even
when I am tired. NS SS FS VS CS
19. I can breastfeed my baby even
when I am upset. NS SS FS VS CS
20. I can use a breast pump
to obtain milk. NS SS FS VS CS
How sure are you that you want to breastfeed? (please circle one)
Do NOT want to breastfeed WILL breastfeed no matter what
0 1 2 3 4 5 6 7 8 9 10