ARTICLE
Brain Developmental Abnormalities in Prader-Willi
Syndrome Detected by Diffusion Tensor Imaging
Kenichi Yamada, MDa, Hitoshi Matsuzawa, MD, PhDa, Makoto Uchiyama, MD, PhDb, Ingrid L. Kwee, MDc, Tsutomu Nakada, MD, PhDa,c
aCenter for Integrated Human Brain Science, Brain Research Institute, andbDivision of Pediatrics, Department of Homeostatic Regulation and Development, Graduate School of Medical and Dental Sciences, University of Niigata, Niigata, Japan;cDepartment of Neurology, University of California, Davis, California
The authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
OBJECTIVE.The purpose of this work was to detect brain developmental abnormalities
in Prader-Willi syndrome by using diffusion tensor imaging based on a high-field MRI system.
METHODS.Eight patients with Prader-Willi syndrome and 8 age- and
gender-matched normal control subjects were examined using a high-field (3.0 T) MRI system. Trace value and fractional anisotropy were assessed simultaneously in multiple representative brain regions: the deep gray matter (putamen, caudate head, and dorsomedial thalamus) and the white matter structures (frontal and parietal white matter, posterior limb of internal capsule, and corpus callosum).
RESULTS.In Prader-Willi syndrome patients, trace value was found to be significantly
higher in the left frontal white matter and the left dorsomedial thalamus, whereas fractional anisotropy was significantly reduced in the posterior limb of the internal capsule bilaterally, the right frontal white matter, and the splenium of the corpus callosum. The observed diffusivity characteristics indicate developmental abnor-malities in these areas, which are highly consistent with the clinical features of Prader-Willi syndrome.
CONCLUSIONS.The study provides the first objective evidence that Prader-Willi
syn-drome patients indeed have developmental abnormalities in specific areas of the brain, providing a new window toward understanding the pathophysiology of Prader-Willi syndrome.
www.pediatrics.org/cgi/doi/10.1542/ peds.2006-0637
doi:10.1542/peds.2006-0637
This work was presented at the 2005 annual meeting of the Society for Neuroscience; November 12–16, 2005; Washington, DC.
Key Words
Prader-Willi syndrome, brain development, diffusion tensor imaging, trace, fractional anisotropy
Abbreviations
PWS—Prader-Willi syndrome DTI— diffusion tensor imaging Tr—trace value
FA—fractional anisotropy ROI—region of interest
PLIC—posterior limb of internal capsule CC— corpus callosum
3DAC—three-dimensional anisotropy contrast
P
RADER-WILLI SYNDROME (PWS) is a genetic disorder characterized by hypotonia, intellectual disabilities, obesity, hypogonadism, short stature, and behavioral disturbance. This syndrome, first described by Prader et al1in 1956, occurs in⬃1 in every 10 000 –25 000indi-viduals, irrespective of races.1–3 Patients with PWS
typically present with several neuroendocrinological ab-normalities, such as growth hormone deficiency, hy-pogonadotropic hypogonadism, and hyperphagia, as the result of possible involvement of the hypothalamo-hy-pophyseal system.4–6 Moreover, they develop mild to
moderate intellectual disabilities and characteristic mal-adaptive behaviors (ie, irritability, lying, skin picking, and obsessions) enhanced during developmental stages from childhood to adulthood.7–9 Although cytogenetic
and molecular studies have revealed the cause of this syndrome as a failure of expression in paternally derived gene in the q11-13 region of chromosome 15,10,11 the
relationship between genotype and phenotype has not been fully elucidated.
Although maturational delay is an essential part of PWS, thus far, no systematic analysis of brain develop-ment has been reported for PWS. Several studies have focused on functional abnormalities in specific neuro-logic domains associated with maturational delay in PWS by using a recent technique of physiologic analysis. Although an event-related potential study has associated abnormal deflation of P3 components with cognitive dysfunction in oddball task, a transcranial magnetic stimulation study has suggested hypoexcitability of the motor cortical areas as the altered corticospinal tract physiology.12,13However, considering the clinical
diver-sity of developmental abnormalities in neurologic and/or behavioral domains, as shown by the profiles of psychomotor development in PWS,14 it is desirable for
the analysis of brain development to assess multiple areas of the brain simultaneously in a quantitative man-ner.
Diffusion tensor imaging (DTI) is a noninvasive im-aging technique capable of providing quantitative indi-ces of brain development.15,16 Quantitative indices
pro-vide in vivo information on trends in physiologic brain maturation17–19 and deviation as maturational delay.20,21
Although DTI provides 3 numerical values (eigenvalues) for quantitative analysis, in clinical settings 2 represen-tative index values derived from 3 eigenvalues, namely trace value (Tr) and fractional anisotropy (FA), are
fre-quently used. Although Tr gives the averaged value of diffusivity without directional consideration, FA pro-vides information of directional deviation (anisotro-pism).15,16Clinical DTI studies have so far revealed
devi-ations of FA resulting from specific conditions such as disruption, degeneration, and disturbed connectivity in white matter (ie, perinatal brain injury, adrenoleu-kodystrophy, and schizophrenia, respectively).21–23
Moreover, analyses of the brain in patients with repre-sentative developmental disorders (ie, autism, fragile X syndrome, tuberous sclerosis, and chromosome 22q11.2 deletion syndrome) by using DTI have shown the dis-ease-specific alterations in diffusivity characteristics in-dexed by Tr or FA indicative of brain developmental abnormalities.24–27Accordingly, DTI would provide
valu-able information on brain developmental abnormalities in PWS, in which specific alteration of the brain devel-opment remains unknown.
In this study, we hypothesized that there would be regional brain abnormalities in PWS associated with spe-cific developmental abnormalities in PWS. We used DTI based on a high-field (3.0 T) MRI system to detect brain developmental abnormalities in PWS.
METHODS
Subjects
Eight patients with PWS, together with 8 randomly se-lected age- and gender-matched healthy control sub-jects, were recruited for the study. The characteristics of the participants are summarized in Table 1. Studies were performed according to the human research guidelines of the Internal Review Board of the University of Ni-igata.
All of the patients satisfied the commonly used clin-ical diagnostic criteria for PWS, and the diagnosis was confirmed by fluorescence in situ hybridization analysis, showing microdeletion of chromosome 15q11-13.28The
level of adaptive functioning on behavior was assessed using the Childhood Behavior Checklist (Japanese ver-sion).29 In addition, standardized psychological tests
were administered to all of the patients by a clinical psychologist to assess global intellectual potential using intelligence quotient, calculated from values derived from the following batteries: Wechsler Intelligence Scale for Children-Third Edition or Wechsler Adult Intelli-gence Scale-Revised. Healthy subjects underwent a
com-TABLE 1 Characteristics of the Patients With PWS and the Normal Control Subjects
Disorders No. Age, ya Gender IQb,c Commentb,d
PWS 8 19 (8–29) 6 male, 2 female 43.8⫾3.3 CBCL score 74.9⫾8.3
Normal control 8 19 (8–29) 6 male, 2 female
aNumerical values represent mean (range) of age. bNumerical values represents mean⫾SD.
plete neurologic examination and interview (parents were interviewed in the case of early childhood) to ascertain that they had no developmental abnormalities and were free of any medication, illicit drugs, and alco-hol.
MRI
A Signa LX 3.0-T (GE Medical System, Waukesha, WI) imaging system was used to perform all of the studies. Diffusion-weighted images were acquired with spin echo echo-planer imaging sequences using the following pa-rameter settings: 4 axial slices; field of view: 200⫻200 mm; matrix: 128⫻128; slice thickness: 5.0 mm; inter-slice gaps: 2.5 mm; repetition time: 5 s; effective echo time: 82.7 ms; and number of excitations: 8. The b value was 500 s/mm2per each axis with the 7 combinations of
diffusion gradient vectors as follows: (0, 0, 0), (1, 0, 1) (⫺1, 0, 1), (0, 1, 1), (0, 1,⫺1), (1, 1, 0), and (⫺1, 1, 0), where (x, y, z) directions correspond with (readout, phase, slice). Parameters used for motion probing gradi-ent were: amplitude, 2.19 g/cm; ramp time, 624s;⌬ ⫽ 37.2 ms; and ␦⫽33.4 ms. The total scanning time for acquisition of the entire diffusion imaging data set was 4 minutes and 40 seconds. In all of the imaging process, adequate preparations using audiovisual aids were pro-vided for children and patients. No sedative procedure was performed.
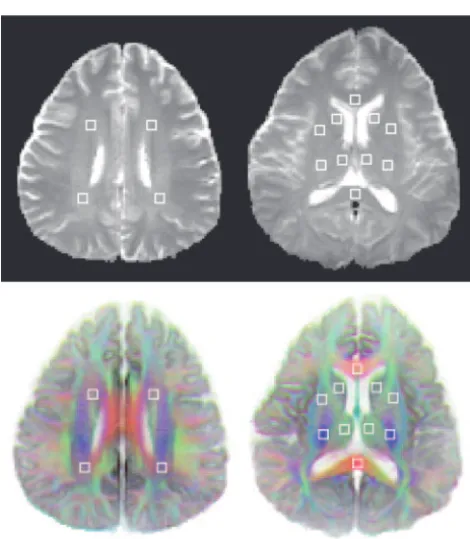
Region of Interest
Multiple regions of interest (ROIs) were set up simulta-neously in the following representative brain regions: the deep gray matter (putamen, caudate head, and dor-somedial thalamus) and the white matter structures (posterior limb of internal capsule [PLIC], frontal and parietal white matter, and genu and splenium of corpus callosum [CC]). All of the ROIs consisted of 3⫻3 pixels (4.7 mm⫻4.7 mm) placed on the following slices: (1) the slice level of the splenium of the CC: putamen, caudate head, dorsomedial thalamus, PLIC, genu, and splenium of the CC; and (2) the slice level of the upper edge of lateral ventricles: frontal and parietal white mat-ter.
For proper anatomic identification, ROI determina-tion was performed based on three-dimensional anisot-ropy contrast (3DAC) images (Fig 1). 3DAC vector con-trast imaging is known to provide exceptionally clear contrast among brain structures, especially between gray and white matter.30,313DAC images can be constructed
by processing 3 principle images of 7 images, a series obtained for eigenvalue determination. This virtually eliminates any error for placement of ROIs as demon-strated by identical identification of ROIs by 3 indepen-dent investigators in blinded fashion.
Data Analysis
Representative index values, Tr and FA, commonly used under clinical setting, were derived from 3 eigenvalues (1⬎2⬎3) by the following formula:
Tr⫽1⫹2⫹3
FA⫽
冑
共1⫺2兲2⫹共
2⫺3兲2⫹共3⫺1兲2
冑
2共12⫹22⫹32兲
(1)
Eigenvalues were determined using MATLAB version 5.3 (The MathWorks Inc, Natick, MA), and numerical data were analyzed on a Windows PC (Windows 2000, Microsoft, Redmond, WA). Data tables and illustrative figures were prepared with vector graphics software (Il-lustrator 7.0, Adobe Systems Inc, San Jose, CA).
Statistical Analysis
A 2-way repeated-measures analysis of variance was conducted on Tr and FA independently, derived from all of the ROIs simultaneously. Disorder and region were set as the between- and the within-subjects variables, respectively. After the interaction effect between disor-der and region was confirmed following the Huynh-Feldt correction in violating sphericity, tests of simple main effect on the factor of disorder were performed subsequently to contrast regional effects associated with disorder. Significant level was set atP⬍.05. All of the statistical analyses were performed by using technical statistical software (SPSS 12 and Sigma Plot 2000 for Windows version 6.0, SPSS Inc, Chicago, IL).
RESULTS
Results are summarized in Table 2 and shown pictorially in Figs 2 and 3. Significant differences in diffusivity characteristics associated with disorder were observed in a region-dependent fashion. Although there was inter-action between 2 factors (disorder and region; Tr: F10.038
⫽1.925;P⬍.05; F12.527⫽1.883;P⬍.05) following the
correction for sphericity (Huynh-Feldt’s; Tr: 0.772; FA: 0.964), tests of simple main effects subsequently showed discrete regional differences in each of the indices.
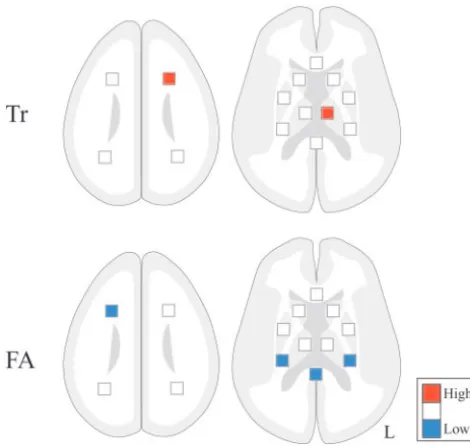
In PWS patients, Tr was found to be significantly higher in the left frontal white matter (F1132.459 ⫽
14.613; P ⬍ .05) and the left dorsomedial thalamus (F1132.459 ⫽ 5.183; P ⬍ .05), whereas FA was
signifi-cantly reduced in the PLIC bilaterally (left: F1162.322 ⫽
6.525, P ⬍ .05; right: F1162.322 ⫽ 8.400,P ⬍ .05), the
right frontal white matter (F1162.322⫽5.331;P⬍ .05),
and the splenium of the CC (F1162.322⫽5.195;P⬍.05).
There were no regions presenting either lower Tr or higher FA in PWS, compared with normal controls.
DISCUSSION
Interestingly, the observed diffusivity characteristic al-teration, which indicates developmental abnormalities in these areas, is consistent with the clinical features of PWS.
The fronto-thalamic regions, in which higher Tr were observed, have a close connection from the limbic sys-tem to the prefrontal and cingulate cortex.32It has been
suggested that abnormalities within these regions could result in psychiatric dysfunction, including personality change or bipolar disorder.33,34 Our findings may
simi-larly indicate that abnormalities within these regions may be responsible for the clinically observed behavioral phenotype, including psychiatric manifestations in PWS.9
Motor dysfunction represents a main clinical feature of PWS and is considered to be primarily because of central nervous system abnormality, not muscular in-volvement.35Previous DTI studies have shown that
re-duced FA reflects altered microstructure in PLIC and correlates with the level of motor disability in motor neuron disease.36,37Reduced FA in PLIC observed
bilat-erally in this study may indeed reflect abnormalities responsible for “central hypotonia” in PWS.
Reduced FA in frontal white matter and posterior callosal connection indicate disintegrity in these regions, important for connecting cortices responsible for cogni-tive, visual, and spatial-perceptional function.38 CC is
one of the crucial structures in developmental disorders, such as autism, in which structural difference has been reported.39,40Its disruption results in the disturbance of
executive functioning that requires effective interhemi-spheric information transfer, as a recent DTI study re-vealed in patients with alcoholism.41 Considering the
psychological profiles as the superiority in spatial-per-ceptional organization and the inferiority in short-term memory on visual-perceptional contents, observed in patients with PWS,14the difference in diffusivity
charac-teristics within posterior callosal connection may indi-cate the brain developmental abnormality of interhemi-spheric connectivity in PWS.
Either higher Tr and/or reduced FA indicate deviation from regular development in each region. Although typ-ical degenerative changes in the mature brain tend to
TABLE 2 Mean Regional Trs and FAs in Brain of Normal Control and PWS Patients
Structure Location Tr (⫻10⫺3mm2/s) FA
Control (N⫽8)
PWS (N⫽8)
Control (N⫽8)
PWS (N⫽8)
Frontal WM L 2.25⫾0.14 2.50⫾0.15a 0.32⫾0.04 0.29⫾0.09
R 2.22⫾0.17 2.34⫾0.08 0.32⫾0.08 0.25⫾0.07a
Parietal WM L 2.48⫾0.19 2.58⫾0.16 0.36⫾0.08 0.42⫾0.07
R 2.40⫾0.11 2.40⫾0.13 0.35⫾0.05 0.40⫾0.09
CC Ge 2.48⫾0.19 2.58⫾0.16 0.74⫾0.08 0.73⫾0.08
Sp 2.40⫾0.11 2.40⫾0.13 0.84⫾0.03 0.78⫾0.02a
PLIC L 2.11⫾0.05 2.16⫾0.07 0.74⫾0.05 0.66⫾0.04a
R 2.20⫾0.07 2.21⫾0.08 0.73⫾0.03 0.65⫾0.04a
Putamen L 2.16⫾0.12 2.15⫾0.09 0.10⫾0.02 0.10⫾0.02
R 2.06⫾0.10 2.13⫾0.12 0.11⫾0.04 0.12⫾0.04
Caudate head L 2.23⫾0.13 2.31⫾0.10 0.14⫾0.03 0.14⫾0.04
R 2.16⫾0.14 2.21⫾0.06 0.14⫾0.03 0.15⫾0.02 Thalamus (DM) L 2.28⫾0.07 2.42⫾0.08a 0.25⫾0.04 0.25⫾0.06 R 2.35⫾0.08 2.35⫾0.07 0.25⫾0.02 0.23⫾0.04
Numerical values represent mean⫾SD. WM indicates white matter; Ge, genu; Sp, splenium; DM, dorsomedial; L, left; R, right. aDifferent from normal control (P⬍.05).
FIGURE 1
produce Tr and FA abnormalities simultaneously, unique microstructural conditions during maturation can result in alteration in Tr or FA independently.42
Changes in eigenvalues during maturation are plausibly explained by the simultaneous occurrence of 2 indepen-dent phenomena, namely: (1) decline in unrestricted water content in extra-axonal space; and (2) increase in diffusivity within the axon. Extra-axonal free water has isotropic behavior as determined by DTI, and, hence, a decline in its relative volume results in a reduction of all eigenvalues to an identical degree. Increase in axonal diameter and/or axoplasmic flow affects anisotropic be-havior of water within the axon and affects only the largest eigenvalue opposing the aforementioned reduc-tion of the value. As a result, reducreduc-tion in values will apparently retard the largest eigenvalue.43Accordingly,
higher Tr is likely to reflect a relative higher level in
extracellular water contents because of the latent delay in the maturational process of matrix formation by glial cells,44,45whereas reduced FA is likely to reflect
matura-tional delay in axonal structure, including myelina-tion.42,44,45Nevertheless, it remains speculative, because
no systematic analysis on brain pathology has been re-ported in PWS.
CONCLUSIONS
This study provides the first objective evidence that PWS is accompanied by developmental abnormalities in spe-cific areas of the brain. Success of the study owes highly to the ROI based approach that we adopted, which is readily performed under demanding clinical settings, such as the pediatric age group. The technique is sensi-tive for identifying individual differences in brain mor-phology, providing the ROI is properly set on
function-FIGURE 2
ally significant anatomic structures. 3DAC imaging,30,31
obtainable without the necessity of any additional imag-ing procedures, virtually guarantees highly accurate ROI settings. Nevertheless, it is prudent to cautiously inter-pret our presented data because of the rather small sam-ple size studied.
ACKNOWLEDGMENTS
The study was supported by grants from the Ministry of Education, Culture, Sports, Science, and Technology (Japan).
We thank Eiko Shouji for helpful advice in commu-nicating with each patient who participated in the stud-ies.
REFERENCES
1. Prader A, Labhart A, Willi H. Ein Syndrom von Adipositas, Kleinwuchs, Kryptochismus und Oligophrenie nach Myato-nieatigem Zustand im Neugeborenenalter.Schweiz Med Wschr.
1956;86:1260 –1261
2. Akefeldt A, Gillberg C, Larsson C. Prader-Willi syndrome in a Swedish rural country: epidemiological aspects.Dev Med Child Neurol.1991;33:715–721
3. Whittington JE, Holland AJ, Webb T, Butler J, Clarke D, Boer H. Population prevalence and estimated birth incidence and mortality rate for people with Prader-Willi syndrome in 1 UK Health Region.J Med Genet.2001;38:792–798
4. Angulo M, Castro-Magana M, Mazur B, et al. Growth hormone secretion and effects or growth hormone therapy on growth velocity and weight gain in children with Prader-Willi syn-drome.J Pediatr Endocrinol Metab.1996;3:393–399
5. Bray GA et al. The Prader-Willi syndrome: a study of 40
pa-tients and a review of the literature.Medicine (Baltimore).1983; 62:59
6. Swaab DF, Purba JS, Hofman MA. Alterations in the hypotha-lamic paraventricular nucleus and its oxytocin neurons (puta-tive satiety cells) in Prader-Willi syndrome: a study of five cases.J Cli in Endocrinol Metab.1995;80:573–579
7. Curfs LG. Psychological profile and behavioral characteristics in Prader-Willi syndrome. In: Cassidy SB, ed. Prader-Willi Syn-drome and Other 15q Deletion Disorders. Berlin, Germany: Springer; 1991:430 – 434
8. Dykens EM, Kasari C. Maladaptive behavior in children with Prader-Willi syndrome, Down syndrome and non-specific mental retardation.Am J Ment Retard.1997;102:228 –237 9. Steinhausen HC, Eiholzer U, Hauffa BP, Malin Z. Behavioural
and emotional disturbances in people with Prader-Willi Syn-drome.J Intellect Disabil Res.2004;48:47–52
10. Ledbetter DH, Mascarello JT, Riccardi VM, Harper VD, Airhart SD, Strobel RJ. Deletions of chromosome 15 as a cause of the Prader-Willi syndrome.N Engl J Med.1981;304:325–329 11. Nicholls RD, Knoll JH, Butler MG, Karam S, Lalande M.
Ge-netic imprinting suggested by maternal heterodisomy in non-deletion Prader-Willi syndrome.Nature.1989;342:281–285 12. Stauder JEA, Brinkman M, Curfs L. Multi-modal P3 deflation
of event-related brain activity in Prader-Willi syndrome. Neu-rosci Lett.2002;327:99 –102
13. Civarci C, Vincentini R, Grugni G, Cantello R. Corticospinal physiology in patients with Prader-Willi syndrome: a transcra-nial magnetic stimulation study. Arch Neurol. 2004;61: 1585–1589
14. Dykens EM, Hodapp RM, Walsh K, Nash LJ. Profiles, correlates and trajectories of intelligence in individuals with Prader-Willi syndrome.J Am Acad Child Adoles Psychiat.1992;31:1125–1130 15. Basser PJ, Pierpaoli C. Microstructural and physiological fea-tures of tissues elucidated by quantitative-diffusion-tensor MRI.J Magn Reson B.1996;111:209 –219
16. Pierpaoli C, Basser PJ. Toward a quantitative assessment of diffusion anisotropy.Magn Reson Med.1997;36:893–906 17. Nomura Y, Sakuma H, Takeda K, Tagami T, Okuda Y,
Naka-gawa T. Diffusional anisotropy of the human brain assessed with diffusion-weighted MR: relation with normal brain de-velopment and aging.Am J Neuroradiol.1994;15:231–238 18. Mukherjee P, Miller JH, Shimony JS, et al. Normal brain
maturation during childhood: Developmental trends charac-terized with diffusion-tensor MR imaging.Radiology.2001;221: 349 –358
19. Schmithorst VJ, Wilke M, Dardzinski BJ, Holland SK. Correla-tion of white matter diffusivity and anisotropy with age during childhood and adolescence: a cross-sectional diffusion-tensor MR imaging study.Radiology.2002;222:212–218
20. Hu¨ppi PS, Maier SE, Peled S, et al. Microstructural develop-ment of human newborn cerebral white matter assessed in vivo by diffusion tensor magnetic resonance imaging.Pediatr Res.1998;44:584 –590
21. McKinstry RC, Miller JH, Snyder AZ, et al. A prospective, longitudinal diffusion tensor imaging study of brain injury in newborns.Neurology.2002;59:824 – 833
22. Ito R, Melhem ER, Mori S, Eichler FS, Raymond GV, Moser HW. Diffusion tensor brain MR imaging in X-linked cerebral adrenoleukodystrophy.Neurology.2001;56:544 –547
23. Kitamura H, Matsuzawa H, Shioiri T, Someya T, Kwee IL, Nakada T. Diffusion tensor analysis in chronic schizophrenia A preliminary study on a high-field (3.0T) system.Eur Arch Psy-chiatry Clin Neurosci.2005;255:313–318
24. Barnea-Goraly N, Kwon H, et al. White matter structure in
FIGURE 3
autism: preliminary evidence from diffusion tensor imaging.
Biol Psychiatry.2004;55:323–326
25. Barnea-Goraly N, Eliez S, et al. White matter tract alterations in fragile X syndrome: preliminary evidence from diffusion tensor imaging.Am J Med Genet B Neuropsychiatr Genet.2003; 118:81– 88
26. Garaci FG, Floris R, Bozzao A, et al. Increased brain apparent diffusion coefficient in tuberous sclerosis.Radiology.2004;232: 461– 465
27. Simon TJ, Ding L, Bish JP, McDonald-McGinn DM, Zackai EH, Gee J. Volmetric, connective, and morphologic changes in the brains of children with chromosome 22q11.2 deletion syndrome: an integrative study.Neuroimage.2005;25:169 –180 28. Holm VA, Cassidy SB, Butler MG, et al. Prader-Willi syndrome:
consensus diagnostic criteria.Pediatrics.1993;91:398 – 402 29. Itani T, Kanbayashi Y, Nakata Y, et al. Standardization of the
Japanese version of the Child Behavior Checklist/4 –18. Jpn J Pediatr Psychiatr Neurol.2001;41:243–252
30. Nakada T, Matsuzawa H. Three-dimensional anisotropy con-trast magnetic resonance imaging of the rat nervous system: MR axonography.Neurosci Res.1995;22:389 –398
31. Nakada T, Nakayama N, Fujii Y, Kwee IL. Clinical application of 3-dimensional anisotropy contrast magnetic resonance axonography: technical note.J Neurosurg.1999;90:791–795 32. Clark DL, Boutros NN.The Brain and Behavior: An Introduction to
Behavioral Neuroanatomy. Malden, MA: Blackwell Science; 1999:119 –129
33. Fukutake T, Akada K, Ito S, Okuda T, Ueki Y. Severe person-ality changes after unilateral left paramedian thalamic infarct.
Eur Neurol.2002;47:156 –160
34. Haznedar MM, Roversi F, Pallanti S, et al. Fronto-thalamo-striatal gray and white matter volumes and anisotropy of their connections in bipolar spectrum illnesses.Biol Psychiatry.2005; 57:733–742
35. Argov Z, Gardner-Medwin D, Johnson MA, Mastaglia FL. Pat-terns of muscle fiber-type disproportion in hypotonic infants.
Arch Neurol.1984;41:53–57
36. Graham JM, Papadakis N, Evans J, et al. Diffusion tensor imaging for the assessment of upper motor neuron integrity in ALS.Neurology.2004;63:2111–2119
37. Sach M, Winkler G, Glauche V, et al. Diffusion tensor MRI of early upper motor neuron involvement in amyotrophic lateral sclerosis.Brain2004;127:340 –350.
38. Pandya D. Two Hemispheres-One Brain. New York, NY: Allan Liss; 1986
39. Piven J, Bailey AS, Randon BJ, Arndt S. An MRI study of the corpus callosum in autism. Am J Psychiatry. 1997;154: 1051–1056
40. Chung MK, Dalton KM, Alexander AL, Davidson RJ. Less white matter concentration in autism: 2D voxel-based mor-phometry.Neuroimage.2004;23:242–251
41. Schulte T, Sullivan EV, Mu¨ller-Ochring EM, Adalsteinsson E, Pfefferbaum A. Corpus callosal microstructural integrity influ-ences interhemispheric processing: a diffusion tensor imaging study.Cereb Cortex2005;15:1384 –1392
42. Suzuki Y, Matsuzawa H, Nakada T. Feasibility study of single region lambda chart analysis for pyramidal tract physiology.
J Neurol.2003;250:1185–1189
43. Suzuki Y, Matsuzawa H, Kwee IL, Nakada T. Absolute eigen-value diffusion tensor analysis for human brain maturation.
NMR Biomed.2003;16:257–260
44. Baratti C, Barnett AS, Pierpaoli C. Comparative MR imaging study of brain maturation in kittens with T1, T2, and the trace of the diffusion tensor.Radiology.1999;210:133–142
DOI: 10.1542/peds.2006-0637
2006;118;e442
Pediatrics
Tsutomu Nakada
Kenichi Yamada, Hitoshi Matsuzawa, Makoto Uchiyama, Ingrid L. Kwee and
Diffusion Tensor Imaging
Brain Developmental Abnormalities in Prader-Willi Syndrome Detected by
Services
Updated Information &
http://pediatrics.aappublications.org/content/118/2/e442
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/118/2/e442#BIBL
This article cites 42 articles, 6 of which you can access for free at:
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2006-0637
2006;118;e442
Pediatrics
Tsutomu Nakada
Kenichi Yamada, Hitoshi Matsuzawa, Makoto Uchiyama, Ingrid L. Kwee and
Diffusion Tensor Imaging
Brain Developmental Abnormalities in Prader-Willi Syndrome Detected by
http://pediatrics.aappublications.org/content/118/2/e442
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.