Serum
Immunoreactive
Pancreatic
Lipase
and
Cationic Trypsinogen
for the Assessment
of
Exocrine
Pancreatic
Function
in Older
Patients
With Cystic
Fibrosis
Geoffrey
Cleghorn,
MBBS,
FRACP,
Lynne
Benjamin,
BSc,
Mary
Corey,
MSc,
Gordon
Forstner,
MD, FRCP(C),
Francesco
Dati,
PhD,
and
Peter
Dune,
MD, FRCP(C)
From the Division of Qastroenterology, Departments of Pediatrics, and the Research Institute, The Hospital for Sick Children, University of Toronto, Toronto, Canada, and Behringwerke AG, Marburg, FederalRepublic of Germany
ABSTRACT.
Indirect and qualitative tests of pancreaticfunction are commonly used to screen patients with cystic
fibrosis for pancreatic insufficiency. In an attempt to
develop a more quantitative assessment, we compared
the usefulness of measuring serum pancreatic lipase using
a newly developed enzyme-linked immunosorbent
im-munoassay with that of cationic trypsinogen using a
radioimmunoassay in the assessment of exocrine
pan-creatic function in patients with cystic fibrosis.
Previ-ously, we have shown neither lipase nor trypsinogen to
be of use in assessing pancreatic function prior to 5 years of age because the majority ofpatients with cystic fibrosis in early infancy have elevated serum levels regardless of
pancreatic function. Therefore, we studied 77 patients
with cystic fibrosis older than 5 years of age, 41 with steatorrhea and 36 without steatorrhea. In addition, 28 of 77 patients consented to undergo a quantitative pan-creatic stimulation test. There was a significant differ-ence between the steatorrheic and nonsteatorrheic pa-tients with the steatorrheic group having lower lipase and
trypsinogen values than the nonsteatorrheic group (P <
.001). Sensitivities and specificities in detecting
steator-rhea were 95% and 86%, respectively, for lipase and 93% and 92%, respectively, for trypsinogen. No correlations were found between the serum levels of lipase and
tryp-sinogen and their respective duodenal concentrations because of abnormally high serum levels of both enzymes
found in some nonsteatorrheic patients. We conclude from this study that both serum lipase and trypsinogen
levels accurately detect steatorrhea in patients with cystic
fibrosis who are older than 5 years but are imprecise
Received for publication Jan 8, 1985; accepted May 2, 1985. Presented, in part, at the combined American Pediatric Society/ Society for Pediatric Research meeting in San Francisco, May
1983.
Reprint requests to (P.R.D.) Division of Gastroenterology, The Hospital for Sick Children, 555 University Aye, Toronto, On-tario, Canada, M5G 1X8.
PEDIATRICS (ISSN 0031 4005). Copyright © 1986 by the
American Academy of Pediatrics.
indicators of specific pancreatic exocrine function above
the level needed for normal fat absorption. Pediatrics
1986;77:301-306; pancreatic lipase, cationic trypsinogen, pancreas function, cystic fibrosis, steatorrhea.
Quantitative pancreatic function tests in patients
with cystic fibrosis have shown that approximately 10% to 15% of patients with cystic fibrosis possess
variable, but sufficient, exocrine pancreatic
func-tion to have normal fat absorption.’ Also, we have
shown that, as a group, those patients with cystic fibrosis who do not have steatorrhea maintain bet-ter pulmonary function and seemingly have a better prognosis than their counterparts with fat malab-sorption.2 Thus, routine pancreatic enzyme replace-ment may not be required in all patients with cystic fibrosis, and because therapy is both unnecessary and may have potential complications, patients
with normal fat absorption should be identified. At present, the quantitative pancreatic stimula-tion test is the most specific and accurate method for estimating exocrine pancreatic function. How-ever, this invasive, direct pancreatic function test is time consuming, expensive, and often beyond the scope of many nonspecialized hospital units. As an alternative to pancreatic stimulation testing, mdi-rect tests ofpancreatic function, such as fat balance studies, the bentiromide test, and 14C02 breath tests, are used to screen for pancreatic
insuffi-ciency.3
test of pancreatic function. In recent years, it has become possible to detect, using different assay techniques, a variety of pancreatic enzymes, such
as immunoreactive trypsinogen, lipase, and
isoam-ylase
in plasma or serum of both normal individualsand patients with a variety of conditions affecting
the exocrine pancreas. With the ability to quanti-tate the levels of these circulating enzymes, our
group and others4#{176} have been investigating the
usefulness of their measurement in the assessment
of exocrine pancreatic function in patients with cystic fibrosis.
In a separate study7 of infants and children
younger than 10 years of age with cystic fibrosis,
with and
without steatorrhea, we have shown thatboth
serum lipase and trypsinogen values aresig-nificantly elevated in infants younger than 1 year and decline throughout the first few years of life. Prior to 5 to
7
years of age, there was no correlation between either serum enzyme and the presence or absence of steatorrhea, but in a small number of patients older than 5 years, there was a suggestionthat both lipase and trypsinogen
values were of use
in distinguishing cystic fibrosis children with pan-creatic insufficiency from cystic fibrosis children
with
normal fat absorption. The purpose of the present study, therefore, was to examine and com-pare the usefulness of serum lipase with immuno-reactive trypsinogen for the assessment of exocrine pancreatic function in a larger number of patients older than 5 years, both with and without steator-rhea, who were known to have cystic fibrosis.METHODS
We studied
77 patients
(mean
age 17.7 years,
range 5 to 41; 37 males and 40 females), older than
5 years,
who
were known to have cystic .fibrosisbased upon typical clinical features and at least two elevated sweat chloride determinations (>60 mEciJ L). All patients included in this study were being treated at the cystic fibrosis clinic, the Hospital for Sick Children, Toronto. This study was ap-proved by the Ethics and Human Experimentation Committee of the Hospital for Sick Children.
Assessment
of Pancreatic
Function
Fecal fat output was estimated in three-day stool collections by the method of van der Kamer et a!.8
In any patient receiving medium chain triglyceride
supplements, fecal fat output was estimated using the methods of Jeejeebhoy et al.9 Fecal fat output was expressed as a percentage of fat intake as
determined by dietary recording and weighing and
with reference to standard food content tables.
Pa-tients with cystic fibrosis were considered to have
pancreatic insufficiency if they had fecal fat outputs
>7%
of intake on previous fat balance studies.Cystic fibrosis patients with fecal fat outputs
s7%
of intake were
considered
to have pancreatic suffi-ciency. The term pancreatic sufficiency has beencoined
for cystic fibrosis patients with probablepancreatic pathology and variable loss of function but who have sufficient residual pancreatic activity for normal fat absorption.’#{176} Thirty-six patients (mean age 19.0 ± 1.5 years, range 6.5 to 36.7 years) were considered to have pancreatic sufficiency by these criteria and 41 patients (mean age 15.9 ± 1.5 years, range 5 to 41 years) were considered to have pancreatic insufficiency.
Pancreatic
Stimulation
Test
Twenty-eight of the
77
patients with cysticfibro-sis included in the study consented to undergo a
simultaneous, quantitative pancreatic stimulation
test. This involved intubation of the duodenum
with
a double-lumen tube so that one lumen openedproximally near the ampulla of Vater and the other,
which
contained several ports, was positioneddis-tally at the ligament of Treitz. A nonabsorbable
marker
solution
was infused through the proximalopening at a constant rate, and pancreatic juice
mixed with marker solution was aspirated through the distal port during an initial collection period of 20 minutes without stimulation and then during 1
hour with continuous intravenous infusion of
secre-tin and pancreozymin. Gastric juice was aspirated
through
a separate nasogastric tube to preventcon-tamination of duodenal contents. Duodenal
aspi-rates were
analyzed
for colipase, total lipase, andtrypsin content by titermetric techniques.11”2 En-zyme output was corrected for distal losses and expressed in units per kilogram of body weight per
hour. All individuals with fat malabsorption had
extremely low enzyme output values consistent with data previously reported from our laboratory. The range of enzyme output in the patients with
cystic fibrosis
without
steatorrhea
was extremelywide
from values marginally above the threshold for developing steatorrhea to outputs well within the normal control range.”On the basis of the stimulation test and previous experience from our laboratory,4”13”4 the 28 pa-tients with cystic fibrosis were divided into two groups: low and adequate enzyme output groups. These groups represented the range of pancreatic function seen in cystic fibrosis, with the low enzyme output group corresponding to patients at or below the threshold for developing steatorrhea and the adequate output group corresponding to patients
without
steatorrhea
but with pancreatic160
140
120
100
80
60
40
20
0 :‘ #{149}. #{149}#{149}.
:,
‘. .: , . . , . J .5 9 13 17 21 25 29 31 33 37
AGE YEARS
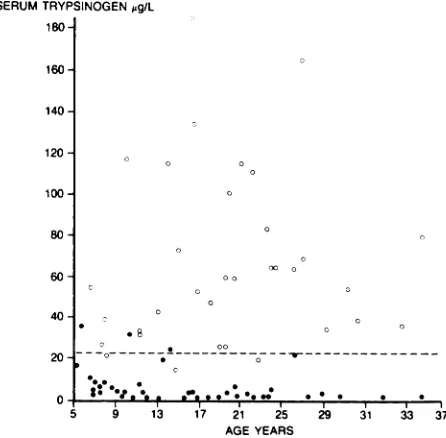
Fig 1.
Serum trypsinogen plotted against age in patients with cystic fibrosis older than 5 years. 0, Patients with pancreatic sufficiency;#{149},
patients with pancreatic insuf-ficiency; horizontal interrupted line, 97.5th percentile of standard error of estimate for cystic fibrosis patients with pancreatic insufficiency. No correlation existed betweenserum trypsinogen and age for either pancreatic
insuffi-cient (r = .1) or sufficient (r = .12) patients.
SERUM LIPASE g/L
2201 0
180
160
140
120
100#{149}
80
60
40
20 #{176}#{176}#{176}
_
_o___oA .4.:’#{149}
#{149}
#{149}. #{149}#{149}.#{149}#{149} #{149} . #{149}j
#{149} - SAGE YEARS
Fig 2.
Serum pancreatic lipase plotted against age in patients with cystic fibrosis older than 5 years. 0,Pa-tients with pancreatic sufficiency;
#{149},
patients withpan-creatic insufficiency; horizontal interrupted line, 97.5th percentile of standard error of estimate for cystic fibrosis
patients with pancreatic insufficiency. No correlation
existed between serum lipase and age for either pan-creatic insufficient (r = .17) or sufficient (r = .01) pa-tients.
for noncystic fibrosis controls.4”3”4 Thus, serum trypsinogen was compared with pancreatic trypsin output: low trypsin output (50 U/kg/h, n = 6),
adequate trypsin output (>50 U/kg/h, n = 22), and serum lipase was compared with total pancreatic
lipase
output: low lipase output (250 U/kg/h, n =8) and adequate
lipase
output (>250 U/kg/h, n =20). Although the duodenal output of pancreatic trypsin and lipase was highly correlated (r =
.73,
P< .01), some individual patients exhibited a degree of nonparallel loss for trypsin and lipase output
and, thus, the patient groups were not identical.
Assay
of Serum
Pancreatic
Enzymes
A random blood sample was obtained from each patient, centrifuged, and the serum stored at -70#{176}C until analyzed. Serum lipase was measured using
an enzyme-linked immunosorbent immunoassay
(ELISA) double-antibody sandwich technique as
described by Grenner
et al.’5 In brief, the method-ology entailed the addition of serum (200 tL) toplastic tubes coated
with specific antibodies toli-pase raised in sheep. After incubation (two hours at
25#{176}C),
the test tubes were washed andperoxi-dase-conjugated
antibodies
to
human lipase added.After further incubation (two hours at 25#{176}C),a
second washing step
was performed. Boundperox-idase activity was determined in a reaction using
hydrogen
peroxide
as substrate ando-phenylene-diamine as chromogen. The reaction was stopped
using
sulfuric acid and the lipase concentration measured photometrically at 492 nm. Cationictryp-sinogen
was measured in each serum sample usingthe double-antibody radioimmunoassay technique
of Geokas
et al’6 which
has previously
been
de-scribed
in detail.’7DATA
ANALYSIS
Geometric means were calculated because of the
unequal distribution of the results. Comparisons were made with age, trypsinogen, and lipase, and the standard error of the estimate was calculated.’8 Serum trypsinogen and lipase values were com-pared using regression analysis, single factor anal-ysis of variance by ranks, and also with the
duo-denal outputs of trypsin and total lipase values obtained from the quantitative stimulation tests.
RESULTS
The individual data points ofboth serum trypsin-ogen and lipase, respectively, were plotted against age for all of the patients with cystic fibrosis studied (Figs 1 and 2). The interrupted horizontal lines in
each figure represents the 97.5th percentile of the
standard
error of the estimate for trypsinogen andSERUM TRYPSINOGEN ,g/L
180
175#{149}
150
125
100
80
70
60
50
40
30
20
10
#{149}1#{149}#{149}#{149} #{149}
TABLE.
Sensitivities and Specificities of SerumPan-creatic Lipase and Cationic Trypsinogen in Detecting
Steatorrhea in Patients With Cystic Fibrosis Older Than
5 Years*
Sensitivity 95% (39/41) 93% (38/41) 88% (36/41)
Specificity 86% (31/36) 92% (33/36) 94% (34/36)
* Results are percentages of patients with (sensitivity)
and without (specificity) steatorrhea. Numbers of
pa-tients are in parentheses.
lipase for the patients with pancreatic insufficiency. SERUM TRYPSINOGEN ng/mI
The open circles represent the trypsinogen and
lipase values
for the patients with cysticfibrosis
without steatorrhea, and the closed circles
repre-sent
those patients with pancreatic insufficiency.Unlike
our previous data in children with cysticfibrosis
younger than 5 years,7 no age-related trends were apparent for either trypsinogen or lipase.Serum trypsinogen clearly distinguished between
the cystic fibrosis patients with and without
stea-torrhea. Ninety-three percent (38/41) of the cystic
fibrosis patients with pancreatic insufficiency had
serum trypsinogen values below the 97.5th
percent-ile for the standard error of the estimate for pan-creatic insufficiency. Only three of 36 (8%) patients with pancreatic sufficiency had trypsinogen values
below
this point (Fig 1). Serum lipase was equallyuseful
in screening for pancreatic insufficiencybe-cause 95% (39/41) of the cystic fibrosis patients
with pancreatic insufficiency had serum lipase
val-ues
below
the 97.5th percentile for the standarderror
of the estimate for pancreatic insufficiencyand only five (14%) of the 36 patients with
pan-creatic sufficiency had lipase values below this point (Fig 2).
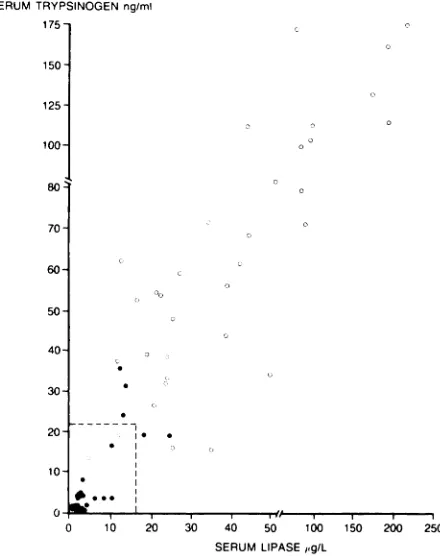
We assessed the usefulness of the combined
mea-surements
of
trypsinogen and lipase in screeningfor pancreatic insufficiency in these patients.
En-zyme measurements for each patient were
com-pared with one another (Fig 3). The intersecting
horizontal
and vertical lines in Fig 3 represent the97.5th percentile for the standard error of the
esti-mate for pancreatic insufficiency for trypsinogen
and lipase, respectively. Serum trypsinogen and
lipase levels were highly correlated in both the
pancreatic insufficient (r =
.77,
P
< .001) and pancreatic sufficient (r=
.90, P < .001) groups. In88%
(36/41)
of the
cystic
fibrosis
patients
with
pancreatic
insufficiency, the combinedmeasure-ment of trypsinogen and lipase were below the 97.5th percentile limits, whereas only two of 36 (6%) of the pancreatic sufficient patients had com-bined measurements below this point. The
sensitiv-ities
and specificities of the individual enzymesalone and for the combined measurements of
tryp-sinogen and lipase
in detecting pancreaticinsuffi-ciency are shown in the Table. Both enzymes are
highly specific and sensitive when measured
mdi-vidually;
however, there is no improvement whentrypsinogen and lipase values are combined.
As previously mentioned, the quantitative
pan-creatic
stimulation test is the most specific andaccurate method of measuring the entire range of pancreatic exocrine function. The serum
trypsino-gen and lipase values for the “low” and “adequate” pancreatic function groups are shown in Fig 4. The
0 10 20 30 40 50 100 150 200 250
SERUM LIPASE gIL
Fig 3.
Serum trypsinogen compared with serumpan-creatic lipase in patients with cystic fibrosis older than 5
years.
0,
Patients without steatorrhea;#{149},
patients withsteatorrhea; intersecting horizontal and vertical lines,
97.5th percentile for standard error of estimate for cystic
fibrosis patients with steatorrhea for trypsinogen and
lipase, respectively. Significant correlations existed for
both pancreatic insufficient (r = .77,
P
< .001) andsufficient (r = .90, P < .001) patients.
Lipase Trypsinogen Lipase -I’
Trypsinogen
horizontal lines represent the two standard
devia-tions of the normal age-related range for serum trypsinogen (16 to 46 tg/L) and lipase (10 to 40.5 tg/L). In the low trypsin output group, the geomet-rid mean serum trypsinogen value was 6.1 tg/mL, and for the adequate trypsin output group, it was 48.2 tg/L. The geometric mean serum lipase values were 4.6 tg/L and 32.3 g/L for the low and ade-quate total lipase output groups, respectively. There was, however, great variability in the serum
tryp-sinogen and lipase levels within the adequate
220 200 -180 120 100-#{163} -J DI
z
w 0 0z
C,)>-a:
w U) s-s. 60 LOW ADEQUATETOTAL LIPASE OUTPUT
[#{174}JL
LOW ADEQUATE
DUODENAL TRYPSIN OUTPUT
Fig 4. Comparison between serum pancreatic trypsino-gen, lipase, and pancreatic function as determined by
quantitative stimulation testing. Low = duodenal trypsin output 50 U/kg/h, duodenal lipase output 250 U/kg/ h. Adequate = duodenal trypsin output > 50 U/kg/h,
duodenal lipase output > 250 U/kg/h.
between serum trypsinogen and duodenal trypsin output and pancreatic lipase and total lipase output revealed a gross separation into very low output and adequate output groups. There was, however, no overall correlation between the serum and duo-denal enzyme levels (trypsinogen v duodenal
tryp-sin, r
=
.10, not significant; pancreatic lipase v total lipase, r=
.01, not significant) because ofabnor-mally elevated serum levels of both enzymes in
many pancreatic sufficient patients.
DISCUSSION
This study has shown that either serum cationic trypsinogen or lipase measurements will detect in excess of 90% of patients with cystic fibrosis older than 5 years who have steatorrhea. Although each enzyme appears to be equally as efficient in detect-ing steatorrhea, the specificity is not significantly increased by the combined measurement of both
enzymes simultaneously.
In a previous publication involving a limited number of patients,’9 we suggested that serum cat-ionic trypsinogen levels were possibly as effective
as duodenal trypsin output levels in determining
subtle changes in pancreatic function in older
pa-tients with cystic fibrosis. From the present study, based on a larger number of patients, it is apparent that this is not the case. Because many of the
pancreatic sufficient patients with cystic fibrosis
had diminished exocrine pancreatic function, as
shown by quantitative pancreatic stimulation
test-ing, one would expect similarly diminished levels of circulating trypsinogen and lipase. In fact, many of
these patients had normal or even elevated circu-lating enzyme levels. This suggests that there may be an element of pancreatic ductular obstruction with resultant reflux of trypsinogen and lipase into the circulation. Recently, we showed that patients with cystic fibrosis at all levels of pancreatic
func-tion secrete significantly less water than controls
without cystic fibrosis with equivalent pancreatic exocrine function.2#{176} It is possible that this defect in
pancreatic water secretion could cause increased
viscosity of secretions and obstruction in the pan-creatic ductules of patients with cystic fibrosis,
which, in turn, could lead to increased reflux of
pancreatic enzymes into the circulation. These
con-cepts will be the subject of further communications
from our laboratory.
We
conclude from this study that serum lipaseand trypsinogen values are equally effective in
de-tecting pancreatic insufficiency, manifest clinically
as steatorrhea, in patients with cystic fibrosis who
are older than 5 years, but neither appear to be
precise indicators of the exact level of exocrine pancreatic function. However, the ELISA method
used for detecting serum pancreatic lipase in this
study does not involve the use of radioisotopes and is much quicker, and, hence, preferable for routine
clinical studies, than the radioimmunoassay tech-nique for cationic trypsinogen. Clinically, the de-termination of pancreatic function in patients with
cystic fibrosis is vital at the time of diagnosis, which in the majority of patients is in the first few years
of life. Unfortunately, neither serum lipase nor trypsinogen are of use in assessing pancreatic
func-tion in this age group and some other method of
testing pancreatic functions such as the serum
p-aminobenzoic acid test may be useful.’#{176}’2’We
spec-ulate, however, that patients with cystic fibrosis
older than 5 years who have elevated levels of serum
trypsinogen or lipase are at risk for failing exocrine pancreatic function and that it may be possible to monitor the pancreatic function of these patients
using either serum trypsinogen or lipase
determi-nations. However, only a long-term, longitudinal, comparative study between serum lipase and
tryp-sinogen and quantitative pancreatic stimulation
data will
resolve this question.ACKNOWLEDGMENTS
This work was supported by a grant from the Canadian
Cystic Fibrosis Foundation. Dr Cleghorn was a recipient
of a research fellowship from the Canadian Cystic Fibro-sis Foundation.
The ELISA kits for serum lipase were donated by
Behringwerke AG, Marburg, Federal Republic of
REFERENCES
1. Shwachman H, Dooley RR, Guilmette F, et al: Cystic fibrosis
of the pancreas with varying degrees of pancreatic
insuffi-ciency. Am J Dis Child 1956;92:347-368
2. Gaskin K, Gurwitz D, Dune P, et al: Improved respiratory prognosis in patients with cystic fibrosis with normal fat absorption. J Pediatr 1982;100:857-862
3. Lankisch PG, Lembcke B: Indirect pancreatic function tests:
Chemical and radioisotope methods. Clin Gastroenterol
1984;13:717-737
4. Dune PR, Largman C, Brodrick JW, et al: Plasma
immu-noreactive pancreatic cationic trypsinogen in cystic fibrosis:
A sensitive indication of exocrine pancreatic dysfunction.
Pediatr Res 1981;15:1351-1355
5. Gillard BK, Cox KL, Pollack PA, et al: Cystic fibrosis serum
pancreatic amylase. Am JDis Child 1984;138:577-580
6. Junglee D, Penketh A, Katrak A, et al: Serum pancreatic
lipase in cystic fibrosis. Br Med J 1983;286:1693-1694
7. Cleghorn G, Benjamin L, Corey M, et al: Age related
alter-ations of immunoreactive pancreatic lipase and cationic trypsinogen in young children with cystic fibrosis. J Pediatr
1985;107:377-381
8. van der Kamer JH, ten Bokkel Huinink H, Weyers HA:
Rapid method for the determination of fat in feces. J Biol Chem 1949;177:347-355
9. Jeejeebhoy KN, Ahmod 5, Kozak G: Determination of fecal
fats containing both medium and long chain triglycerides and fatty acids. Clin Biochem 1970;3:157-163
10. Dune PR, Gaskin KJ, Corey M, et al: Pancreatic function testing in cystic fibrosis. J Pediatr Gastroenterol Nutr
1984;3(suppl):S89-598
1 1. Gaskin KJ, Dune PR, Hill RE, et al: Colipase and maximally
activated pancreatic lipase in normal subjects and patients
with steatorrhea. J Clin Invest 1982;69:427-434
12. Dyck WP: Titermetric measurements of fecal trypsin and
chymotrypsin in cystic fibrosis with pancreatic exocrine
insufficiency. Am J Dig Dis 1967;12:310-317
13. Gaskin KJ, Dune PR, Lee L, et al: Colipase and lipase
secretion in childhood-onset pancreatic insufficiency:
Delin-eation of patients with steatorrhea secondary to relative co-lipase deficiency. Gastroenterology 1984;86:1-7
14. Gaskin K, Dune P, Corey M, et a!: Evidence for a primary
defect of pancreatic HCOi secretion in cystic fibrosis. Pe-diatr Res 1982;16:554-557
15. Grenner G, Deutsch G, Schmidtberger R, et al: A highly sensitive enzyme immunoassay for the determination of
pancreatic lipase. J Clin Chem Clin Biochem
1982;20:515-519
16. Geokas MC, Largman C, Brodrick JW, et al: Determination of human pancreatic cationic trypsinogen in serum by
ra-dioimmunoassay. Am J Physiol 1979;236:E77-E83
17. Largman C, Brodrick JW, Geokas MC: Radioimmunoassay
determination of circulating pancreatic endopeptidases.
Methods Enzymol. 1981;74:272-290
18. Zar JH: Biostatistical Analysis. Englewood Cliffs, NJ,
Pren-tice-Hall Inc, 1974
19. Dune PR, Largman C, Brodrick JW, et al: Plasma
immu-noreactive pancreatic cationic trypsinogen in cystic fibrosis: A sensitive indicator of exocrine pancreatic dysfunction.
Pediatr Res 1981;15:1351-1355
20. Kopelman H, Dune P, Gaskin G, et al: Pancreatic fluid
secetion and protein hyperconcentration in cystic fibrosis. N EngI J Med 1985;312:329-334
21. Dockter G, Nacu I, Kohlberger E: Determination of
pro-tease-cleaved p-aminobenzoic acid (PABA) in serum after
oral administration of N-benzoyl-L-tyrosyl-p-aminobenzoic
acid (PABA-peptide) in children. Eur J Pediatr 1981;
135:277-279