Executive Functioning in School-Aged Children Who Were Born Very
Preterm or With Extremely Low Birth Weight in the 1990s
Peter J. Anderson, PhD*‡, Lex W. Doyle, MD*§, and the Victorian Infant Collaborative Study Group
ABSTRACT. Objective. To determine the frequency, nature, and severity of executive dysfunction (EDF) at 8 years of age in extremely low birth weight (ELBW)/very preterm infants who were born in the 1990s, compared with normal birth weight (NBW) control subjects.
Methods. A geographically determined cohort study was conducted in Victoria, Australia. The ELBW/very preterm cohort comprised 298 consecutive survivors at 2 years of age who had gestational ages <28 completed weeks or birth weights<1000 g and were born during 1991-1992. The NBW cohort comprised 262 randomly se-lected children of birth weight>2499 g matched on date of birth, gender, ethnicity, and health insurance status. The participation rate was 92% (275 of 298) for the ELBW/ very preterm cohort and 85% (223 of 262) for the NBW cohort. Cognitive and behavioral measures of executive functioning were administered.
Results. The ELBW/very preterm cohort exhibited significant EDF compared with their NBW peers in all areas assessed. The cognitive assessment revealed global impairment rather than deficits in specific executive do-mains. The ELBW/very preterm children also displayed more behavioral problems indicative of EDF than the NBW children. Severe impairments were exhibited in only a small minority of ELBW/very preterm children. No statistical conclusions were altered after adjustment for sociodemographic variables or when children with substantial neurosensory impairment were excluded.
Conclusions. School-aged children who were born in the 1990s and were very preterm or had ELBW are at greater risk for developing EDF and require ongoing neuropsychological review throughout middle child-hood.Pediatrics2004;114:50 –57;executive function, exec-utive dysfunction, extremely low birth weight, very pre-term, prematurity.
ABBREVIATIONS. NBW, normal birth weight; EF, executive func-tion; EDF, executive dysfuncfunc-tion; ELBW, extremely low birth weight; PVL, periventricular leukomalacia; IVH, intraventricular hemorrhage; CI, confidence interval; BRIEF, Behavior Rating In-ventory of Executive Function.
I
nfants who are born prematurely are at increased risk for cognitive and educational impairments, with group means falling approximately one half to two thirds of an SD below normal birth weight(NBW) peers.1–4Developmental delay is not the sole explanation for the neurodevelopmental deficits ex-hibited by preterm children, as learning problems persist throughout childhood and adolescence.2,5–10 For devising more effective intervention programs for preterm children, a greater understanding of their cognitive deficits is required. Identifying the nature of cognitive deficits associated with prematu-rity will also provide some indication of the neural systems compromised, which may in turn lead to medical interventions to enhance recovery from brain injury and early brain development.
Neuropsychological studies have reported im-pairments across a wide range of cognitive skills in preterm children,11–17 including executive func-tion.18,19Executive function (EF) refers to a collection of interrelated processes that are responsible for pur-poseful, goal-directed behavior and is important in a child’s cognitive functioning, behavior, emo-tional control, and social interaction.20Cognitive pro-cesses associated with EF are numerous, but the prin-cipal elements include anticipation, goal selection, planning and organization, initiation of activity, self-regulation, mental flexibility, deployment of at-tention, working memory, and utilization of feed-back.21Executive dysfunction (EDF) is not a unitary disorder20but represents a range of impairment pro-files.
Although some evidence is available indicating increased risk of EDF in preterm children, research examining this association is limited. Deficits in plan-ning ability, inhibition, and motor sequencing have been reported in a small sample of children (n⫽30) of extremely low birth weight (ELBW),18 whereas spatial working memory impairments have been found in children who were born prematurely.19 Also, problems with spatial organization and mental flexibility have been reported to escalate as birth weight decreases.16,22 As survival rates of very pre-term (⬍28 weeks) and ELBW (birth weight⬍1000 g) children have increased in the 1990s with improve-ments in perinatal care, the number of such children with EDF is likely to be greater. To the best of our knowledge, no published studies have assessed EF comprehensively in a large regional cohort of pre-term children who were born in the 1990s. This study aimed to examine the frequency, nature, and severity of EDF in a large geographically defined cohort of school-aged children who were born at⬍28 weeks or with ELBW.
From the *Royal Women’s Hospital, Melbourne, Australia; ‡Murdoch Chil-dren’s Research Institute, Melbourne, Australia; and §University of Mel-bourne, MelMel-bourne, Australia.
Received for publication May 5, 2003; accepted Nov 16, 2003.
Reprint requests to (P.J.A.) Department of Psychology, Royal Childrens Hospital, Flemington Rd, Parkville, Victoria, 3052, Australia. E-mail: [email protected]
METHODS Participants
Of 568 consecutive live births with birth weights⬍1000 g or with gestational ages⬍28 completed weeks in Victoria, Australia, between January 1991 and December 1992, 298 (52.5%) survived to 2 years of age; these survivors composed the ELBW/very preterm cohort. The participation rate was 92.3% (275 of 298), and of the 23 children who were not assessed, 8 were lost, 11 refused, and 4 were inaccessible, usually living in another country. The mean gestational age at birth for the ELBW/very preterm participants was 26.7 weeks (SD: 1.9), with 73 (27%) children born earlier than 26 weeks and 138 (50%) born at 26 or 27 weeks. Their mean birth weight was 884 g (SD: 162), with 54 (20%) weighing⬍750 g and 172 (63%) weighing 750 to 999 g. Thirty-eight (14%) were small for gestational age as defined by birth weight ⬎2 SD below that expected for gestational age and gender. Of the ELBW/very pre-term participants, 253 (92%) children were born in level III peri-natal centers, 202 (73%) received anteperi-natal steroids, 91 (33%) were administered postnatal steroids, and 108 (39%) had surfactant therapy. Bronchopulmonary dysplasia was diagnosed for 163 (59%) infants, and 71 (26%) required surgery in the newborn period. On the basis of neonatal cranial ultrasound, 16 (6%) ELBW/very preterm infants had periventricular leukomalacia (PVL), while 18 (7%) had grade III/IV intraventricular hemor-rhage (IVH). Significant neurosensory impairments were identi-fied in 34 (12%) children; 3 were blind, 4 required hearing aids, and 29 had cerebral palsy (2 of whom were also blind).
The NBW cohort, also enrolled at birth, comprised 262 survi-vors from 265 randomly selected children who had birth weight ⬎2499 g and were born in 1 of the 3 level III perinatal centers in Victoria. Each control was born on the expected date of birth for each child of birth weight⬍1000 g and was matched for gender, the mother’s country of birth (English speaking or not), and health insurance status (private health insurance or not). The participa-tion rate was 85.1% (223 of 262), and of the 39 children who were not assessed, 22 were lost, 13 refused, and 4 were inaccessible. The mean gestational age at birth for the NBW participants was 39.3 weeks (SD: 1.4), and the mean birth weight was 3407 g (SD: 443). All children in the NBW group were born in level III perinatal centers, and 3 (1%) received antenatal steroids. Only 1 child in the NBW cohort received a diagnosis of a significant neurosensory impairment, which was cerebral palsy.
Participants were assessed when aged between 8 and 9 years, although 4 children were assessed just before their 8th birthday and another 4 children were assessed a few months after their 10th birthday. Age was corrected according to the child’s expected birth date as we have previously described a small but important reduction in IQ even at 8 to 9 years of age.23
Of the children who were not assessed at 8 years of age, 48% (30 of 63) were of low social class, but this was not significantly different from the rate of 46% of low social class in those who were assessed at 8. Nonparticipants tended to have lower psychometric test scores at 2 and 5 years of age than participants at the 8-year follow-up (age 2: Mental Developmental Index on the Bayley Scales of Infant Development, mean difference,⫺4.4, 95% confi-dence interval [CI],⫺11.7 to 3.3,P⫽.27; age 5: full-scale IQ on Wechsler Preschool and Primary Scale of Intelligence–Revised, mean difference,⫺6.8, 95% CI,⫺13.6 to⫺0.1,P⫽.046).
Procedure
All children were enrolled in the newborn period in a prospec-tive longitudinal study of growth and development throughout childhood. Written informed consent was obtained from parents of NBW children, but follow-up was considered routine clinical care for the ELBW/very preterm children. The study was ap-proved by the Research and Ethics Committees of the Royal Women’s Hospital, Melbourne. Neuropsychological assessments were conducted by experienced psychologists who were unaware of children’s perinatal details. In addition to measures of EF, the Wechsler Intelligence Scale for Children–Third Edition24was ad-ministered to have an estimate of general intellectual ability. With the exception of a supplementary subtest (Mazes), the entire Wechsler Intelligence Scale for Children–Third Edition battery was administered. Social class was determined by the occupation of the main income earner in the family; low social class identified
families in which the main income earner was unskilled or unem-ployed. Twelve children in the ELBW/very preterm cohort were not assessed because of significant neurosensory impairment. Of the remaining children, some had incomplete data sets because of assessment difficulties or lack of parental compliance. Children were assessed for this component of the study between January 2000 and April 2002.
Outcome Measures
EF is a multidimensional construct that incorporates both cog-nitive and behavioral elements. The neuropsychological assess-ment included a battery of tests sensitive to specific executive processes. In addition, the parents of participants completed a questionnaire regarding behaviors associated with EDF.
Similarities
Similarities24assesses verbal conceptual reasoning, which re-fers to the ability to identify the concept/s linking words or themes. In Similarities, participants are presented with a series of word pairs (eg, wheel/ball, telephone/radio, ice/steam) for which they must identify and explain the common concept that the word pairs represent. Each response is scored (0, 1, or 2 points) accord-ing to the degree of abstraction. There are 19 word pairs, but the test is discontinued after 4 consecutive failures. Overall perfor-mance is judged according to age standardized scores that have a mean of 10 (SD: 3).
Digit Span
Digit Span24assesses verbal working memory, which refers to the capacity to store temporarily and manipulate verbal informa-tion. Digit Span has 2 parts. First, participants are presented with a series of number sequences that the participant is required to repeat verbatim. The number sequence increases from 2 digits to 9 digits, with 2 trials for each sequence length. The task is discon-tinued when participants fail both trials of a sequence length. The second part of Digit Span is similar, although participants must now repeat the sequences in the reverse order. Overall perfor-mance is judged according to age-standardized scores that have a mean of 10 (SD: 3).
Block Design
Block Design24assesses spatial conceptualization, which refers to the ability to devise spatial patterns from multiple component parts. In Block Design, participants are required to create specific 2-dimensional geometric designs using 2-colored cubes (blocks). The number of cubes increases as the geometric designs become more difficult. Block Design consists of 12 designs, but the test is discontinued after 2 consecutive failures. Each design has a time limit, and depending on the completion time, the child can earn bonus points. Overall performance is judged according to age-standardized scores that have a mean of 10 (SD: 3).
Picture Arrangement
Picture Arrangement24assesses visual reasoning, which refers to the capacity to make logical inferences on the basis of visual stimuli/information. Picture Arrangement comprises 14 items in which the participant is presented with a set of colorful pictures in a mixed-up order that requires rearrangement into a logical story sequence. Overall performance is judged according to age-stan-dardized scores that have a mean of 10 (SD: 3).
Tower of London25
Performance of participants was determined by the number of items solved correctly (maximum score of 12).
Rey Complex Figure
The Rey Complex Figure26,27assesses spatial organization and strategic decision making. Spatial organization refers to the ability to perceive and interpret complex spatial stimuli/information; strategic decision making refers to the capacity to plan ahead and devise efficient and effective strategies to attain a specific goal. In the Rey Complex Figure, participants are required to copy, as accurately as possible, a complex geometric figure consisting of a large rectangle, vertical and horizontal centerlines, 2 diagonals, and external attachments and internal sections of the large rect-angle. The accuracy scoring procedure developed by Osterri-eth28,29was used to assess spatial organization (score range: 0-36), whereas the Rey Complex Figure–Organizational Strategy Score30 was used to measure strategic decision making (1⫽poor; 2⫽ fragmented; 3⫽part-configural; 4⫽conceptual).
Behavior Rating Inventory of Executive Function
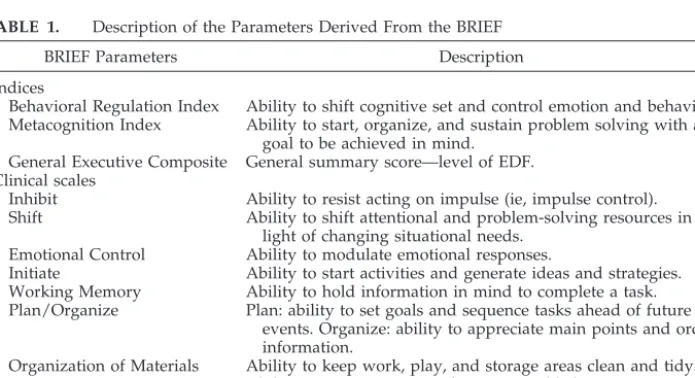
The Behavior Rating Inventory of Executive Function31 is a questionnaire that assesses behavioral manifestations of EF. In this study, the Parent version was administered. The BRIEF consists of 86 items, which provide 8 theoretically and empirically derived clinical scales (Inhibit, Shift, Emotional Control, Initiate, Working Memory, Plan/Organize, Organization of Materials, and Moni-tor), 2 indices (Metacognitive and Behavioral Regulation), and 1 composite score (Global Executive Composite). Table 1 provides a description of the BRIEF parameters. BRIEF scores are age-gender standardized with a mean of 50 (SD: 10), with higher scores reflecting greater EDF. Scoresⱖ65 (ie,ⱖ1.5 SD above the norma-tive mean) are considered to be abnormally elevated and repre-senting clinically significant behavior problems. Internal consis-tency for the parent form of the BRIEF has been found to be high, ranging from 0.80 to 0.98.31Clinical validity has been supported with a variety of diagnostic groups.31
Statistical Analyses
Between-group differences (ELBW/very preterm vs NBW) for dichotomous outcome data were analyzed by2analysis and for continuous data byttest as data were normally distributed. For the behavioral parameters with clinical cutoff scores, relative risks were calculated. For adjusting for potential confounding variables, data were also analyzed by multiple linear regression, when ap-propriate. Sociodemographic factors such as gender, ethnicity, language spoken at home, family structure, mother’s marital sta-tus, social class, and mother’s and father’s education were used as covariates in the multivariate analyzes. Furthermore, comparisons were repeated excluding children with significant neurosensory impairment (eg, cerebral palsy, blindness, deafness).
Within the ELBW/very preterm cohort, there was also interest in the contrast between the smallest (birth weight 500-749 g) and
most immature (23-25 weeks’ gestation) survivors and their slightly heavier (birth weight 750-999 g) or more mature (26-27 weeks’ gestation) counterparts. These between-group compari-sons were analyzed byttest and multiple linear regression when controlling for sociodemographic variables. The bivariate relation-ship between birth weight/gestational age and EF parameters were analyzed by Pearson correlation coefficient.
With the exception of children with missing data, the analyses included all children. With the numbers in each cohort assessed, we had 80% power of detecting differences in means between groups as small as 0.27 SD.P⬍.05 was considered statistically significant. As this study was primarily hypothesis generating rather than hypothesis proving and as each of the domains as-sessed was of individual interest, we did not reducePvalues for multiple tests.
RESULTS
The sociodemographic characteristics and gender distribution of the ELBW/very preterm and NBW cohorts were similar (see Table 2). The mean ages of the ELBW/very preterm and NBW cohorts at the time of the assessment were 8.7 years and 8.9 years, respectively. English was the only language spoken at home for the majority of families in both the ELBW/very preterm and NBW cohorts, and ethnic-ity, based on mother’s race, was comparable. Signif-icantly fewer mothers in the ELBW/very preterm cohort were married in comparison with mothers in the NBW cohort (2 ⫽ 6.7, P ⬍ .01), although the proportion of intact families was similar. Social class of the 2 cohorts did not differ; however, the propor-tions with at least 12 years of formal education were significantly greater in mothers (2 ⫽ 8.0,P ⬍ .01) and fathers (2⫽18.2,P⬍.001) in the NBW cohort. The cohorts differed significantly in terms of full-scale IQ (mean difference: ⫺9.4; 95% CI: ⫺12.1 to ⫺6.7), with the ELBW/very preterm cohort within the average range (90-109) but nearly two thirds SD below their NBW peers.
Cognitive Assessment of EF
The ELBW/very preterm cohort scored signifi-cantly lower than their NBW peers on all cognitive parameters of EF, including verbal conceptual rea-soning (Similarities: t476 ⫽ ⫺4.2, P ⬍ .001), verbal working memory (Digit Span:t473⫽ ⫺3.7,P⬍.001),
TABLE 1. Description of the Parameters Derived From the BRIEF
BRIEF Parameters Description
Indices
Behavioral Regulation Index Ability to shift cognitive set and control emotion and behavior. Metacognition Index Ability to start, organize, and sustain problem solving with a
goal to be achieved in mind. General Executive Composite General summary score—level of EDF. Clinical scales
Inhibit Ability to resist acting on impulse (ie, impulse control). Shift Ability to shift attentional and problem-solving resources in
light of changing situational needs. Emotional Control Ability to modulate emotional responses.
Initiate Ability to start activities and generate ideas and strategies. Working Memory Ability to hold information in mind to complete a task. Plan/Organize Plan: ability to set goals and sequence tasks ahead of future
events. Organize: ability to appreciate main points and order information.
Organization of Materials Ability to keep work, play, and storage areas clean and tidy. Monitor Ability to monitor own performance and behavior, to ensure
spatial conceptualization (Block Design:t474⫽ ⫺7.1,
P ⬍ .001), visual reasoning (Picture Arrangement:
t474 ⫽ ⫺5.7, P ⬍ .001), planning ability (Tower of London:t464⫽ ⫺2.6,P⬍.01), and spatial organiza-tion (Rey Complex Figure accuracy:t464⫽ ⫺6.7,P⬍ .001; Table 3). The strategic decision making (Rey Complex Figure strategy) of the ELBW/very preterm cohort was also poorer (2⫽11.2,P⬍.05), with 57% using poor strategies in comparison with 42% of the NBW children. Although the ELBW/very preterm cohort performed well below the NBW cohort across all cognitive parameters, the group means were gen-erally within the average range. Small reductions in mean differences were found when analyses were repeated adjusting for sociodemographic variables, but no statistical conclusions were affected (see Table 3). Excluding children with significant neurosensory impairment also failed to alter the statistical conclu-sions.
Within the ELBW/very preterm cohort, children with birth weights 500 to 749 g scored lower on all cognitive parameters of EF than those with birth weights 750 to 999 g, and mean differences reached significance for spatial conceptualization (Block De-sign: mean difference:⫺1.6; 95% CI: ⫺2.8 to ⫺0.4), visual reasoning (Picture Arrangement: mean differ-ence:⫺1.4; 95% CI:⫺2.6 to⫺0.2), and spatial orga-nization (Rey Complex Figure accuracy: mean differ-ence:⫺3.4; 95% CI:⫺5.9 to⫺0.9). Similarly, children with gestational ages 23 to 25 weeks scored lower on most cognitive parameters than those of gestational ages 26 to 27 weeks; however, the only mean differ-ence to reach significance was spatial organization (Rey Complex Figure accuracy; mean difference: ⫺3.0; 95% CI:⫺5.3 to⫺0.6). Controlling for sociode-mographic variables did not alter the above findings. Within the ELBW/very preterm group, gestational age and birth weight correlated weakly with the
TABLE 2. Sociodemographic Characteristics of the ELBW/Very Preterm and NBW Cohorts
ELBW/Very Preterm (n⫽275)
NBW (n⫽223)
Boys (n[%]) 128 (46.5%) 104 (46.6%)
Age at evaluation (y; mean [SD]) 8.7 (0.3) 8.9 (0.4) Ethnicity (mothers)
Born in English-speaking country (n[%]) 220/274 (80.3%) 188 (84.3%)
Aboriginal (n[%]) 4/274 (1.5%) 0 (0%)
Black (n[%]) 3/274 (1.1%) 1 (0.4%)
English only spoken at home (n[%]) 225/274 (82.1%) 192 (86.1%) Intact family structure (n[%]) 191/272 (70.2%) 170/220 (77.3%) Married mother (n[%])* 180/271 (66.4%) 169/219 (77.2%)
Low social class (n[%]) 132 (48.0%) 95/222 (42.8%)
Maternal education (ⱖ12 y of schooling;n[%])* 129/269 (48.0%) 132/217 (60.8%) Paternal education (ⱖ12 y of schooling;n[%])** 102/248 (41.1%) 125/204 (61.3%)
Full-scale IQ (mean [SD])† 95.5 (16.0) 104.9 (14.1)
*P⬍.01. †P⬍.001.
TABLE 3. Group Means and SDs of the ELBW/Very Preterm and NBW Groups on Cognitive and Behavioral Parameters of EF
ELBW/Very Preterm (Mean [SD]n)
NBW (Mean [SD]n)
Mean Difference (95% CI)
Adjusted Mean Difference*
(95% CI)
Cognitive assessment
Verbal Conceptual Reasoning (SIM)† 9.3 (3.6) 261 10.6 (3.2) 217 ⫺1.3 (⫺1.9,⫺0.7) ⫺0.9 (⫺1.5,⫺0.3) Verbal Working Memory (DS)† 8.5 (2.8) 258 9.5 (2.9) 217 ⫺1.0 (⫺1.5,⫺0.5) ⫺1.0 (⫺1.5,⫺0.4) Spatial Conceptualization (BD)† 9.7 (3.7) 259 12.0 (3.6) 217 ⫺2.4 (⫺3.0,⫺1.7) ⫺2.2 (⫺2.9,⫺1.5) Visual Reasoning (PA)† 8.9 (3.7) 259 10.8 (3.4) 217 ⫺1.9 (⫺2.5,⫺1.2) ⫺1.7 (⫺2.4,⫺1.0) Planning Ability (TOL)‡ 10.9 (1.6) 253 11.2 (1.2) 1.2 ⫺0.3 (⫺0.6,⫺0.1) ⫺0.3 (⫺0.6,⫺0.04) Spatial Organization (RCF)† 22.4 (7.6) 250 26.7 (5.7) 216 ⫺4.2 (⫺5.5,⫺3.0) ⫺4.2 (⫺5.5,⫺2.9) Behavioral assessment
Behavioral Regulation 51.8 (10.9) 245 49.9 (9.9) 205 1.9 (⫺0.1, 3.9) 1.1 (⫺1.0, 3.2) Inhibit 50.9 (10.3) 245 49.5 (10.2) 205 1.4 (⫺0.5, 3.3) 0.7 (⫺1.3, 2.6)
Shift§ 51.1 (10.6) 245 49.2 (9.8) 205 1.9 (0.0, 3.8) 1.3 (⫺0.7, 3.3)
Emotional Control 51.5 (11.1) 245 49.9 (10.1) 205 1.6 (⫺0.4, 3.6) 1.2 (⫺0.9, 3.3) Metacognition† 53.5 (9.8) 245 49.9 (9.9) 205 3.6 (1.8, 5.4) 3.2 (1.2, 5.1)
Initiate‡ 52.7 (9.7) 245 49.9 (9.2) 205 2.8 (1.0, 4.5) 2.3 (0.5, 4.1)
Working Memory† 55.5 (10.5) 245 50.6 (10.0) 205 4.9 (3.0, 6.8) 4.6 (2.6, 6.6) Planning/Organization‡ 53.3 (10.2) 245 50.0 (10.6) 205 3.3 (1.4, 5.2) 2.7 (0.6, 4.7) Organization of Materials 52.3 (10.2) 245 51.3 (10.2) 205 0.9 (⫺0.9, 2.8) 0.8 (⫺1.2, 2.8) Monitoring‡ 50.1 (10.1) 245 47.5 (9.3) 205 2.6 (0.8, 4.4) 2.0 (0.1, 3.9) Global Executive Composite‡ 52.9 (9.9) 245 49.8 (9.8) 205 3.1 (1.2, 4.9) 2.5 (0.6, 4.4)
SIM indicates Similarities; DS, Digit Span; BD, Block Design; PA, Picture Arrangement; TOL, Tower of London; RCF, Rey Complex Figure. * Adjusting for sociodemographic variables (gender, ethnicity, language spoken at home, family structure, mother’s marital status, social class, and parental education).
cognitive parameters of EF (correlation coefficient range: 0.001-0.187).
Behavioral Assessment of EF
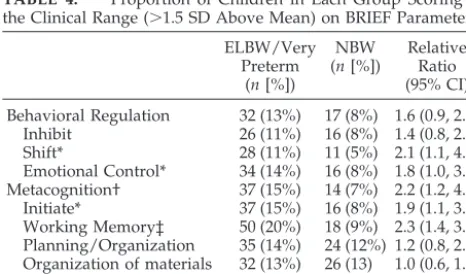
In comparison with the NBW cohort, the ELBW/ very preterm cohort scored higher across all behav-ioral parameters of EF, including the Global Execu-tive Composite (t448 ⫽ 3.3, P ⫽ .001), indicating an increased risk for EDF (Table 3). The ELBW/very preterm cohort did not differ significantly in terms of Behavioral Regulation, and of the clinical scales as-sociated with this index score, only Shift was signif-icantly elevated in the ELBW/very preterm cohort (t448⫽2.0,P⫽.048). The ELBW/very preterm cohort was significantly elevated on the Metacognition in-dex score (t448⫽3.9,P⬍ .001), as a result of higher scores on most of the associated clinical scales in-cluding Initiate (t448⫽3.1,P⫽.002), Working Mem-ory (t448⫽5.1,P⬍.001), Planning/Organization (t448 ⫽3.4,P⫽.001), and Monitoring (t448⫽2.8,P⫽.006). As shown in Table 4, children in the ELBW/very preterm cohort were at increased risk for exhibiting clinically significant behavioral problems in the Shift (P⫽.016), Emotional Control (P⫽.028), Initiate (P⫽
.012), Working Memory (P⫽ .001), and Monitoring (P⫽.008) domains. Small reductions in mean differ-ences again were observed when analyses were ad-justed for sociodemographic variables (Table 3) or when analyses were repeated excluding children with significant neurosensory impairment. Statistical conclusions were largely unaffected by these addi-tional analyses; however, the mean difference for Shift failed to reach significance when adjusting for differences in sociodemographic variables (mean dif-ference: 1.6; 95% CI:⫺0.4 to 3.5) and when children with neurosensory impairment were excluded (mean difference: 1.7; 95% CI:⫺0.3 to 3.6).
Within the ELBW/very preterm cohort, children with birth weights 500 to 749 g did not differ on any of the behavioral parameters when compared with children with birth weights 750 to 999 g. Similarly, those with gestational ages 23 to 25 weeks were not elevated on any of the behavioral parameters when compared with those with gestational ages 26 to 27
weeks; however, this latter subgroup was slightly elevated on Emotional Control (mean difference: 4.0; 95% CI: 0.6-7.3). When adjusting for sociodemo-graphic variables, the older gestational group was also found to be scoring higher on the Behavioral Regulation Index (mean difference: 3.5; 95% CI: 0.1-6.9), but no other statistical conclusions were altered. Gestational age and birth weight correlated weakly with the behavioral parameters of EF (range: 0.006-0.181).
DISCUSSION
Executive skills are important for cognitive and adaptive functioning; however, the analysis of exec-utive processes in preterm children has been largely neglected. Furthermore, the few studies that have examined EDF in preterm samples have tended to use small samples, selective samples, or inadequate outcome measures. Thus, our understanding of the frequency, nature, and severity of EDF in this popu-lation is limited. In this study, we assessed both cognitive and behavioral elements of EF in a large regional cohort of school-aged children who were born very preterm (⬍28 weeks) or with ELBW. We found that the ELBW/very preterm cohort exhibited significant deficits across all cognitive parameters assessed, whereas their behavioral impairments were restricted mainly to the Metacognition domain. Different patterns of deficits may represent EDF, and understanding the nature of the impairment in children who are born very preterm or with ELBW is crucial for remediation purposes. In our study, the cognitive assessment focused on reasoning ability, working memory, planning and organizational abil-ity, and strategic decision making. The ELBW/very preterm cohort exhibited impairments in all of these areas when compared with NBW peers. The behav-ioral assessment supported these findings, with pa-rental responses indicating that children in the ELBW/very preterm cohort have more trouble start-ing activities, generatstart-ing new ideas and strategies, holding information in mind, planning a sequence of actions in advance, and organizing information and thoughts than children in the NBW cohort. Our cog-nitive assessment did not include tasks that assess impulse control, self-regulation, and mental flexibil-ity; however, the behavioral assessment found that the ELBW/very preterm cohort experienced greater difficulties monitoring actions and shifting attention than NBW children. Children in the ELBW/very pre-term cohort were no more impulsive than their NBW peers, despite previous studies reporting higher rates of attentional problems and attention-deficit/hyper-activity disorder.32–34In summary, our ELBW/very preterm cohort born in the 1990s exhibited a global deficit in EF rather than a specific pattern of execu-tive deficits. This is consistent with previous studies with preterm children who were born before the 1990s, which report impairments across a range of executive processes including planning ability, im-pulse control, motor sequencing, spatial working memory, spatial organization, and mental flexibili-ty.16,18,19,22
TABLE 4. Proportion of Children in Each Group Scoring in the Clinical Range (⬎1.5 SD Above Mean) on BRIEF Parameters
ELBW/Very Preterm
(n[%])
NBW (n[%])
Relative Ratio (95% CI)
Behavioral Regulation 32 (13%) 17 (8%) 1.6 (0.9, 2.8) Inhibit 26 (11%) 16 (8%) 1.4 (0.8, 2.5) Shift* 28 (11%) 11 (5%) 2.1 (1.1, 4.2) Emotional Control* 34 (14%) 16 (8%) 1.8 (1.0, 3.1) Metacognition† 37 (15%) 14 (7%) 2.2 (1.2, 4.0) Initiate* 37 (15%) 16 (8%) 1.9 (1.1, 3.4) Working Memory‡ 50 (20%) 18 (9%) 2.3 (1.4, 3.9) Planning/Organization 35 (14%) 24 (12%) 1.2 (0.8, 2.0) Organization of materials 32 (13%) 26 (13) 1.0 (0.6, 1.7) Monitoring† 23 (9%) 7 (3%) 2.8 (1.2, 6.3) Global Executive Composite 32 (13%) 17 (8%) 1.6 (0.9, 2.8)
The magnitude of the mean difference between the ELBW/very preterm and NBW cohorts averaged 0.5 SD for cognitive parameters (range: 0.25-0.8) and 0.25 SD for behavioral parameters (range: 0.1-0.5), but the means for the ELBW/very preterm cohort were gen-erally within the average range. On the basis of the behavioral assessment, significantly more children in the ELBW/very preterm cohort were exhibiting clin-ically significant impairments than children in the NBW cohort. For example, children in the ELBW/ very preterm cohort were 2 to 3 times more likely to be displaying significant problems in monitoring performance, holding information in mind, initiating activities and ideas, and shifting attention. The pro-portion of ELBW/very preterm children who exhib-ited clinically relevant problems was relatively small. For instance, the highest rate of clinical problems was identified in the Working Memory domain, with 20% scoring in the clinical range, and only 13% of the ELBW/very preterm cohort were in the clinical range on the Global Executive Composite. However, it is reasonable to assume that this ELBW/very pre-term cohort was also at greater risk for “subtle” deficits, which also affect educational progress and adaptive functioning. Children who exhibit mild problems are less likely to arouse parental or teacher concerns, be referred for neuropsychological assess-ment, and receive specialist assistance.
Our overall findings were robust and were not affected when adjusting for important sociodemo-graphic factors such as gender, ethnicity, mother’s marital status, family structure, language spoken at home, social class, and parental education. Similarly, statistical conclusions were largely unaffected when children with significant neurosensory impairment were excluded from the analyses. Children who were born with birth weights of 500 to 749 g performed more poorly on cognitive parameters than the heavier survivors (750-999 g), but no differences were observed on the behavioral parameters. Chil-dren who were born before 26 weeks of gestation tended to perform slightly poorer than their more mature (26-27 weeks) counterparts on cognitive pa-rameters, but, counterintuitive, the more mature sub-group exhibited poorer behavioral regulation, espe-cially in emotional control. Our correlational analyses revealed that birth weight and gestational age correlated weakly with EF parameters (cognitive and behavioral), indicating that other factors must also mediate outcome in this cognitive domain. Un-fortunately, the numbers of children in this cohort with grade III/IV IVH (n ⫽ 18) and PVL (n ⫽ 16) were inadequate to examine the effects of these fac-tors on outcome.
It is important to note that the cognitive deficits exhibited by this ELBW/very preterm cohort were not specific to EF. When compared with the NBW cohort, we found that the ELBW/very preterm co-hort also had deficits in nonexecutive skills such as general knowledge (Information subtest24: mean dif-ference: ⫺1.4; 95% CI: ⫺1.9 to ⫺0.8), vocabulary (Vocabulary subtest24: mean difference: ⫺0.9; 95% CI:⫺1.4 to⫺0.3), and visual analysis (Picture Com-pletion24: mean difference: ⫺1.3; 95% CI: ⫺1.8 to
⫺0.8). Thus, consistent with previous neuropsycho-logical studies,11–17children in the ELBW/very pre-term cohort were at risk for impairment across a range of cognitive domains. Whether EDF in this population is a primary deficit or secondary to im-pairments in other domains is yet to be established and will be resolved only with neuroimaging stud-ies. We do not have neuroimaging data at school age in this cohort.
The cognitive and educational problems associ-ated with prematurity are thought to be relassoci-ated to brain anomalies. Periventricular white matter injury, or PVL, is the most common form of brain injury in preterm infants.35 Although the pathogenesis is not entirely clear, PVL is thought to be related to isch-emia and can result in focal or diffused lesions.36A recent report demonstrated that preterm infants with PVL had significantly less cerebral cortical gray mat-ter and brain myelin at mat-term than premat-term infants without PVL or term control subjects,35 indicating that early brain insults involving the white matter are likely to impair later myelination and develop-ment of gray matter structures. Gray matter and white matter volumes increase dramatically during the third trimester, making brain development of preterm infants vulnerable even if acute brain insults such as PVL and IVH are not present. For example Hu¨ppi et al37 found that between 29 and 41 weeks’ postconceptional age, total brain volumes increased 2.7-fold, cortical gray matter increased 4-fold, and myelinated white matter increased 5-fold (mostly after 36 weeks). Abnormalities of nutrition and met-abolic functioning as well as environmental stresses may disrupt this period of rapid brain development, especially in infants with PVL.37Neuroimaging stud-ies of preterm children in middle childhood38 and adolescence39support the view that prematurity af-fects brain development, resulting in long-term structural abnormalities. Such studies have reported disproportionately smaller volumes of the cortex, basal ganglia, amygdala, hippocampus, and corpus callosum as well as an increase in the size of the lateral ventricles in comparison with term control subjects.38,39
For EF, the prefrontal cortex is considered impor-tant. The neural systems underpinning EF are nu-merous, complex, and interrelated, involving pre-frontal connections with virtually all other brain regions including the brainstem; occipital, temporal, and parietal lobes; and limbic and subcortical re-gions.21,40EDF is not always associated with prefron-tal pathology directly but may be related to network disconnections such as white matter damage or im-pairment to subcortical or posterior brain re-gions.41,42Prefrontal neural networks are thought to be responsible for specific functions,41 and as such, the nature of impairment may assist to identify which networks are compromised. Children who are born very preterm or with ELBW seem to exhibit a general cognitive impairment including EDF, which is consistent with neuroimaging studies that report impaired myelination and reduced volumes for many subcortical and posterior structures.35,38
children who were born in the 1990s with ELBW or very preterm are at increased risk for developing EDF compared with their NBW peers. On the basis of our behavioral data, clinically significant difficulties were exhibited in a minority of ELBW/very preterm children; however, even “subtle” deficits may ad-versely affect academic achievement. As more of these children are now reaching school age, with survival rates in geographic cohorts 3 times higher in the 1990s compared with the 1970s, it is important that the nature of their cognitive deficits be under-stood by parents, teachers, and health professionals. We propose that preterm children require ongoing neuropsychological review throughout middle child-hood so that impairments, such as EDF, can be iden-tified early and intervention strategies can be imple-mented to reduce the long-term impact of their deficits. Also, additional research is needed to deter-mine the specific brain abnormalities underlying the executive deficits so that preventive strategies, espe-cially in the perinatal period, can be developed and introduced into clinical practice.
ACKNOWLEDGMENTS
This study was supported in part by a grant from Health and Community Services, Victoria, and the National Health and Med-ical Research Council, Australia.
Participants: Convenor, Lex W. Doyle, MD, FRACP (Royal Women’s Hospital and University of Melbourne). Collaborators (in alphabetical order): Peter J. Anderson, PhD (Royal Women’s Hospital and Murdoch Childrens Research Institute); Catherine Callanan, RN (Royal Women’s Hospital); Elizabeth Carse, FRACP (Monash Medical Centre); Dan Casalaz, FRACP (the Mercy Hos-pital for Women); Margaret P. Charlton, MEdPsych (Monash Medical Centre); Noni Davis, FRACP (Royal Women’s Hospital); Julianne Duff, FRACP (Royal Women’s Hospital and the Mercy Hospital for Women); Geoffrey Ford, FRACP (Royal Women’s Hospital); Simon Fraser, FRACP (the Mercy Hospital for Women); Marie Hayes, RN (Monash Medical Centre) Mary Kaimakamis, BSc (Royal Women’s Hospital); Elaine Kelly, MA (Royal Women’s Hospital and the Mercy Hospital for Women); Gillian Opie, FRACP (the Mercy Hospital for Women); Andrew Watkins, FRACP (the Mercy Hospital for Women); Heather Woods, RN (the Mercy Hospital for Women); and Victor Yu, MD, FRACP (Monash Medical Centre).
REFERENCES
1. Bhutta A, Cleves M, Casey P, Cradock M, Anand K. Cognitive and behavioral outcomes of school-aged children who were born preterm: a meta-analysis.JAMA.2002;288:728 –737
2. Saigal S. Follow-up of very low birthweight babies to adolescence.
Semin Neonatol.2000;5:107–118
3. Wolke D, Meyer R. Cognitive status, language attainment, and preread-ing skills of 6-year-old very preterm children and their peers: the Bavarian Longitudinal Study.Dev Med Child Neurol.1999;41:94 –109 4. Anderson PJ, Doyle LW, the Victorian Infant Collaborative Study
Group. Neurobehavioral outcomes of school-aged children born ex-tremely low birth weight or very preterm in the 1990s.JAMA.2003;289: 3264 –3272
5. Koller H, Lawson K, Rose S, Wallace I, McCarton C. Patterns of cogni-tive development in very low birth weight children during the first six years of life.Pediatrics.1997;99:383–389
6. McDonald M, Sigman M, Ungerer J. Intelligence and behavior problems in 5-year-olds in relation to representational abilities in the second year of life.J Dev Behav Pediatr.1989;10:86 –91
7. Rickards A, Kelly E, Doyle L, Callanan C. Cognition, academic progress, behavior and self-concept at 14 years of very low birth weight children.
J Dev Behav Pediatr.2001;22:11–18
8. Saigal S, Hoult L, Streiner D, Stoskopf B, Rosenbaum P. School difficul-ties at adolescence in a regional cohort of children who were extremely low birth weight.Pediatrics.2000;105:325–331
9. Taylor H, Klein N, Minich N, Hack M. Middle-school-age outcomes in children with very low birthweight.Child Dev.2000;71:1495–1511 10. Wolke D, Ratschinski G, Ohrt B, Riegel K. The cognitive outcome of
very preterm infants may be poorer than often reported: an empirical investigation of how methodological issues make a big difference.Eur J Pediatr.1994;153:906 –915
11. Breslau N, Chilcoat H, DeDotto J, Andreski P, Brown G. Low birth weight and neurocognitive status at six years of age.Biol Psychiatry.
1996;40:389 –397
12. de Haan M, Bauer P, Georgieff M, Nelson C. Explicit memory in low-risk infants aged 19 months born between 27 and 42 weeks of gestation.Dev Med Child Neurol.2000;42:304 –312
13. Goyen T, Lui K, Woods R. Visual-motor, visual perceptual, and fine motor outcomes in very-low-birthweight children at 5 years.Dev Med Child Neurol.1998;40:76 – 81
14. Luoma L, Herrgård E, Martikainen A, Ahonen T. Speech and language development of children born at 32 weeks’ gestation: a 5-year prospec-tive follow-up study.Dev Med Child Neurol.1998;40:380 –387 15. Rose S, Feldman J. Memory and processing speed in preterm children at
eleven years: a comparison with full-terms. Child Dev. 1996;67: 2005–2021
16. Taylor H, Hack M, Klein N. Attention deficits in children with⬍750 gm birth weight.Child Neuropsychol.1998;4:21–34
17. Taylor H, Klein N, Minich N, Hack M. Verbal memory deficits in children with less than 750 g birth weight.Child Neuropsychol.2000;6: 49 – 63
18. Harvey J, O’Callaghan M, Mohay H. Executive function of children with extremely low birthweight: a case control study.Dev Med Child Neurol.1999;41:292–297
19. Luciana M, Lindeke L, Mills M, Nelson C. Neurobehavioral evidence for working memory deficits in school-aged children with histories of prematurity.Dev Med Child Neurol.1999;41:521–533
20. Gioia G, Isquith P, Guy S. Assessment of executive functions in children with neurological impairment. In: Simeonsson R, Rosenthal S, eds.
Psychological and Developmental Assessment: Children With Disabilities and Chronic Conditions. New York, NY: The Guilford Press; 2001:317–356 21. Anderson P. Assessment and development of executive function (EF)
during childhood.Child Neuropsychol.2002;8:71– 82
22. Waber D, McCormick M. Late neuropsychological outcomes in preterm infants of normal IQ: selective vulnerability of the visual system.J Pe-diatr Psychol.1995;20:721–735
23. Rickards AL, Kitchen WH, Doyle LW, Kelly EA. Correction of devel-opmental and intelligence test scores for premature birth.Aust Paediatr J.1989;25:127–129
24. Wechsler D.Manual for the Wechsler Scale of Children’s Intelligence–3rd ed. (WISC-III). New York, NY: The Psychological Corporation; 1991 25. Shallice T. Specific impairments of planning.Philos Trans R Soc Lond B
Biol Sci.1982;298:199 –209
26. Rey A. L’examen clinique en psychologique dans les cas d’encephalopathic traumatique.Arch Psychol.1941;28:286 –340 27. Rey A. Psychological examination of traumatic encephalopathy
(trans-lation).Clin Neuropsychol.1993;7:3–21
28. Osterrieth P. Le test de copie d’une figure complexe.Arch Psychol.
1944;30:206 –256
29. Osterrieth P. The complex figure copy test (translation).Clin Neuropsy-chol.1993;7:3–21
30. Anderson P, Anderson V, Garth J. Assessment and development of organizational ability: the Rey Complex Figure Organizational Strategy Score (RCF-OSS).Clin Neuropsychol.2001;15:81–94
31. Gioia G, Isquith P, Guy S, Kenworthy L.BRIEF—Behavior Rating Inven-tory of Executive Function. Professional Manual. Odessa, FL: Psychological Assessment Resources; 2000
32. Botting N, Powls A, Cooke R, Marlow N. Attention deficit hyperactivity disorders and other psychiatric outcomes in very low birthweight chil-dren at 12 years.J Child Psychol Psychiatry.1997;38:931–941
33. Hille E, den Ouden A, Saigal S, et al. Behavioural problems in children who weigh 1000 g or less at birth in four countries.Lancet.2001;357: 1641–1643
34. Szatmari P, Saigal S, Rosenbaum P, Campbell D, King S. Psychiatric disorders at five years among children with birthweights⬍1000g: a regional perspective.Dev Med Child Neurol.1990;32:954 –962 35. Inder T, Huppi P, Warfield S, et al. Periventricular white matter injury
in the premature infant is followed by reduced cerebral cortical grey matter volume at term.Ann Neurol.1999;46:755–760
aspects, neuropathology, and pathogenesis.Semin Pediatr Neurol.1998; 5:135–151
37. Hu¨ppi P, Warfield S, Kikinis R, et al. Quantitative magnetic resonance imaging of brain development in premature and mature newborns.Ann Neurol.1998;43:224 –235
38. Peterson B, Vohr B, Staib L, et al. Regional brain volumes abnormalities and long-term cognitive outcome in preterm infants.JAMA.2000;284: 1939 –1947
39. Nosarti C, Al-Asady M, Frangou S, Stewart A, Rifkin L, Murray R.
Adolescents who were born very preterm have decreased brain vol-umes.Brain.2002;125:1616 –1623
40. Stuss D, Benson D. Neuropsychological studies of the frontal lobes.
Psychol Bull.1984;95:3–28
41. Alexander M, Stuss D. Disorders of frontal lobe functioning.Semin Neurol.2000;20:427– 437
42. Eslinger P, Grattan L. Frontal lobe and frontal-striatal substrates for different forms of human cognitive flexibility.Neuropsychologia.1993;31: 17–28
21ST INTERNATIONAL SYMPOSIUM ON NEONATAL INTENSIVE CARE
November 4 – 6, 2004 Hotel Melia`, Milan, Italy Directed by Guido Moro
Further information about faculty, topics, deadlines, and registration fees is available at: www.retecivica.milano.it/macedoniomelloni
Registration and Accommodations
M.C.A. Events srl Via Aleardo Aleardi, 17 20154 Milan, Italy
Telephone: 39 02 34934404 Fax: 39 02 34934397 E-mail: [email protected]
Scientific Information
Amiel Warm
Department of Perinatal Pathology Macedonio Melloni Maternity Hospital Via Macedonio Melloni, 52
20129 Milan, Italy
Telephone: 39 02 63633252 Fax: 39 02 745419
E-mail: [email protected]
General Secretariat
Stanley Norman c/o CSH Viale Liguria, 22 20143 Milan, Italy
DOI: 10.1542/peds.114.1.50
2004;114;50
Pediatrics
Peter J. Anderson and Lex W. Doyle
or With Extremely Low Birth Weight in the 1990s
Executive Functioning in School-Aged Children Who Were Born Very Preterm
Services
Updated Information &
http://pediatrics.aappublications.org/content/114/1/50 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/114/1/50#BIBL This article cites 39 articles, 2 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/neonatology_sub
Neonatology
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_
Fetus/Newborn Infant
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.114.1.50
2004;114;50
Pediatrics
Peter J. Anderson and Lex W. Doyle
or With Extremely Low Birth Weight in the 1990s
Executive Functioning in School-Aged Children Who Were Born Very Preterm
http://pediatrics.aappublications.org/content/114/1/50
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.